
Postoperative Dietary Intake Achievement: A Secondary Analysis of a Randomized Controlled Trial

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
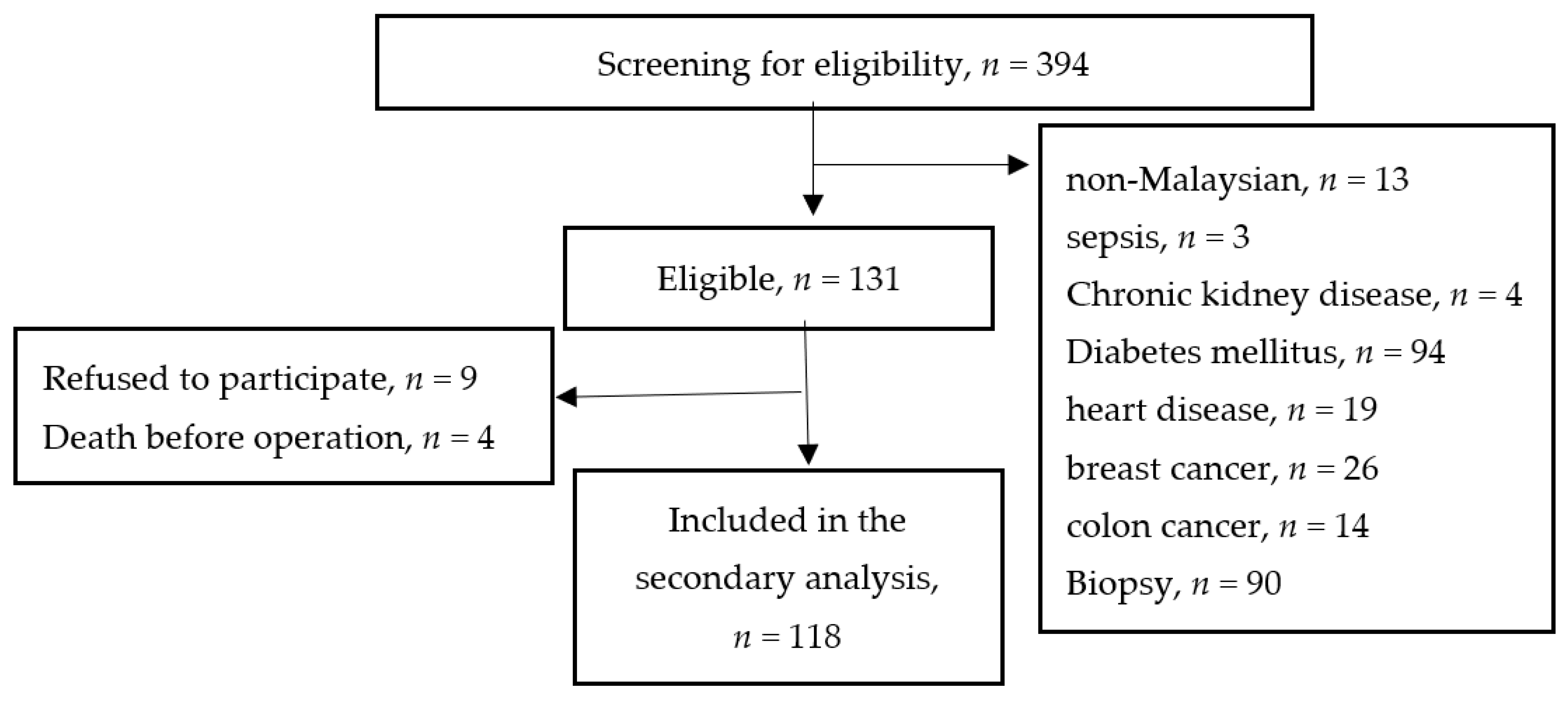
2.2. Participants
2.3. Outcomes Measurement
Participant Group and Study Endpoint
2.4. Sociodemographic and Clinical Characteristics
2.5. Nutritional and Functional Status
2.6. Biochemical Profile (Serum albumin)
2.7. Pre-Admission and Postoperative Dietary Intake
2.8. Postoperative Outcomes
2.9. Ethical Approval
2.10. Statistical Analysis
3. Results
4. Discussion
Strength and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wilmore, D.W. Metabolic Response to Severe Surgical Illness: Overview. World J. Surg. 2000, 24, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. Espen Guidelines on Nutrition in Cancer Patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arved, W.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.; et al. Espen Guideline: Clinical Nutrition in Surgery. Clin. Nutr. 2017, 36, 623–650. [Google Scholar]
- Yi, H.C.; Ibrahim, Z.; Zaid, Z.A.; Daud, Z.M.; Yusop, N.B.M.; Omar, J.; Abas, M.N.M.; Rahman, Z.A.; Jamhuri, N. Impact of Enhanced Recovery after Surgery with Preoperative Whey Protein-Infused Carbohydrate Loading and Postoperative Early Oral Feeding among Surgical Gynecologic Cancer Patients: An Open-Labelled Randomized Controlled Trial. Nutrients 2020, 12, 264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahan, L.; Kathleen, J.; Raymond, L. Krause and Mahan’s Food & the Nutrition Care Process, 15th ed.; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Megan, R.; Marshall, A.; Desbrow, B.; Roberts, S. Feeding Practices and Nutrition Intakes among Non-Critically Ill, Postoperative Adult Patients: An Observational Study. Nutr. Clin. Pract. 2018, 34, 371–380. [Google Scholar]
- Charlotte, M.; Rasmussen, T.; Jakobsen, D.H.; Ottosen, C.; Lundvall, L.; Ottesen, B.; Callesen, T.; Kehlet, H. The Effect of Accelerated Rehabilitation on Recovery after Surgery for Ovarian Malignancy. Acta Obstet. Gynecol. Scand. 2006, 85, 488–492. [Google Scholar]
- Henriksen, M.G.; Hessov, I.; Dela, F.; Hansen, H.V.; Haraldsted, V.; Rodt, S.Å. Effects of Preoperative Oral Carbohydrates and Peptides on Postoperative Endocrine Response, Mobilization, Nutrition and Muscle Function in Abdominal Surgery. Acta Anaesthesiol. Scand. 2003, 47, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Yi, H.C.; Ibrahim, Z.; Yu, N.B.M.; Zaid, Z.A.; Daud, Z.M. Fast Track Recovery Surgery with a Whey Protein Infused Carbohydrate Loading Drink Pre-Operatively and Early Oral Feeding Post-Operatively among Surgical Gynaecologic Cancer Patients: Study Protocol of an Open Labelled Randomised Controlled Trial. Trials 2020, 21, 533. [Google Scholar]
- Daniels, L.A. Good Nutrition for Good Surgery: Clinical and Quality of Life Outcomes. Australia 2003, 26, 136–140. [Google Scholar] [CrossRef] [Green Version]
- Peterson, S.J.; Tsai, A.A.; Scala, C.M.; Sowa, D.C.; Sheean, P.M.; Braunschweig, C.L. Adequacy of Oral Intake in Critically Ill Patients 1 Week after Extubation. J. Am. Diet. Assoc. 2010, 110, 427–433. [Google Scholar] [CrossRef]
- Gibson, R.S. Principles of Nutritional Assessment; Oxford University Press: New York, NY, USA, 2005. [Google Scholar]
- Zahara, A.M.; Shahar, S.; Safii, N.S.; Haron, H. Atlas of Food Exchanges & Portion Sizes; MDC Publishers: Kuala Lumpur, Malaysia, 2015. [Google Scholar]
- First Data Bank. Nutritionist Pro Nutrition Analysis Software; Version 2.4; First Data Bank: San Bruno, CA, USA, 2005. [Google Scholar]
- Brenda, L.; Cleghorn, G.; Janda, M.; Obermair, A. Comparison of Different Nutritional Assessments and Body-Composition Measurements in Detecting Malnutrition among Gynecologic Cancer Patients. Am. J. Clin. Nutr. 2008, 87, 1678–1685. [Google Scholar]
- Laky, B.; Janda, M.; Bauer, J.; Vavra, C.; Cleghorn, G.; Obermair, A. Malnutrition among Gynaecological Cancer Patients. Eur. J. Clin. Nutr. 2006, 61, 642–646. [Google Scholar] [CrossRef] [PubMed]
- Ju-Hee, N.; Kim, S.R.; Kwon, Y.S. Depression and Appetite: Predictors of Malnutrition in Gynecologic Cancer. Support. Care Cancer 2014, 22, 3081–3088. [Google Scholar]
- Ho, C.Y.; Ibrahim, Z.; Zaid, Z.A.; Daud, Z.M.; Yusop, N.B.M. Clinical Malnutrition Predictive Model among Gynecologic Cancer Patients Prior to Elective Operation: A Cross-Sectional Study. Clin. Nutr. 2021, 40, 4373–4379. [Google Scholar] [CrossRef]
- Ram, E.; Raban, O.; Tsoref, D.; Jakobson-Setton, A.; Sabah, G.; Salman, L.; Yeoshua, E.; Ben-Haroush, A. Malignant Ascites: Validation of a Novel Ascites Symptom Mini-Scale for Use in Patients with Ovarian Cancer. Int. J. Gynecol. Cancer 2018, 28, 1162–1166. [Google Scholar]
- Kehlet, H. Enhanced Recovery after Surgery (Eras): Good for Now, but What about the Future? Can. J. Anesth./J. Can. D’anesthésie 2015, 62, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Nermina, R.; Adam, V.N.; Čaušević, S.; Dervišević, S.; Delibegović, S. A Randomised Controlled Study of Preoperative Oral Carbohydrate Loading versus Fasting in Patients Undergoing Colorectal Surgery. Int. J. Colorectal Dis. 2019, 34, 1551–1561. [Google Scholar]
- Yeung, S.E.; Hilkewich, L.; Gillis, C.; Heine, J.A.; Fenton, T.R. Protein Intakes Are Associated with Reduced Length of Stay: A Comparison between Enhanced Recovery after Surgery (Eras) and Conventional Care after Elective Colorectal Surgery. Am. J. Clin. Nutr. 2017, 106, 44–51. [Google Scholar] [PubMed]
- Phuong, N.; Ramakrishnan, U.; Katz, B.; Gonzalez-Casanova, I.; Lowe, A.E.; Nguyen, H.; Pham, H.; Truong, T.; Nguyen, S.; Martorell, R. Mid-Upper-Arm and Calf Circumferences Are Useful Predictors of Underweight in Women of Reproductive Age in Northern Vietnam. Food Nutr. Bull. 2014, 35, 301–311. [Google Scholar]
- Gustafsson, U.O.; Scott, M.J.; Schwenk, W.; Demartines, N.; Roulin, D.; Francis, N.; McNaught, C.E.; MacFie, J.; Liberman, A.S.; Soop, M.; et al. Guidelines for Perioperative Care in Elective Colonic Surgery: Enhanced Recovery after Surgery (Eras®) Society Recommendations. World J. Surg. 2013, 37, 259–284. [Google Scholar] [CrossRef]
- Steven, B.; Nelson, G.; Altman, A. Impact of Nutrition on Enhanced Recovery after Surgery (Eras) in Gynecologic Oncology. Nutrients 2019, 11, 1088. [Google Scholar]
- de Ana Carolina Martins, O.; de Lima Friche, A.A.; Salomão, M.S.; Bougo, G.C.; Vicente, L.C.C. Predictive Factors for Oropharyngeal Dysphagia after Prolonged Orotracheal Intubation. Braz. J. Otorhinolaryngol. 2018, 84, 722–728. [Google Scholar]
- David, G.; Bidd, H.; Rashid, H. Multimodal Intraoperative Monitoring: An Observational Case Series in High Risk Patients Undergoing Major Peripheral Vascular Surgery. Int. J. Surg. 2014, 12, 231–236. [Google Scholar]
- Oyama, Y.; Iwasaka, H.; Shiihara, K.; Hagiwara, S.; Kubo, N.; Fujitomi, Y.; Noguchi, T. Effects of Preoperative Oral Carbohydrates and Trace Elements on Perioperative Nutritional Status in Elective Surgery Patients. Middle East J. Anaesthesiol. 2011, 21, 375–383. [Google Scholar] [PubMed]
- Beattie, A.H.; Prach, A.T.; Baxter, J.P.; Pennington, C.R. A Randomised Controlled Trial Evaluating the Use of Enteral Nutritional Supplements Postoperatively in Malnourished Surgical Patients. Gut 2000, 46, 813–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, S.C.; Koh, A.J.H. Nutrition and the Elderly Surgical Patients. MOJ Surg. 2017, 4, 00088. [Google Scholar]
- Jeong, O.; Ryu, S.Y.; Park, Y.K. Postoperative Functional Recovery after Gastrectomy in Patients Undergoing Enhanced Recovery after Surgery: A Prospective Assessment Using Standard Discharge Criteria. Medicine 2016, 95, e3140. [Google Scholar] [CrossRef]
- Mc Loughlin, S.; Terrasa, S.A.; Ljungqvist, O.; Sanchez, G.; Fornari, G.G.; Alvarez, A.O. Nausea and Vomiting in a Colorectal Eras Program: Impact on Nutritional Recovery and the Length of Hospital Stay. Clin. Nutr. ESPEN 2019, 34, 73–80. [Google Scholar] [CrossRef]
- Francesco, L.; Calvani, R.; Tosato, M.; Martone, A.M.; Ortolani, E.; Savera, G.; D’Angelo, E.; Sisto, A.; Marzetti, E. Protein Intake and Muscle Health in Old Age: From Biological Plausibility to Clinical Evidence. Nutrients 2016, 8, 295. [Google Scholar]
- Dock-Nascimento, D.B.; de Aguilar-Nascimento, J.E.; Faria, M.S.M.; Caporossi, C.; Slhessarenko, N.; Waitzberg, D.L. Evaluation of the Effects of a Preoperative 2-Hour Fast with Maltodextrine and Glutamine on Insulin Resistance, Acute-Phase Response, Nitrogen Balance, and Serum Glutathione after Laparoscopic Cholecystectomy. J. Parenter. Enter. Nutr. 2012, 36, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Lyell, N.J.; Kitano, M.; Smith, B.; Gleisner, A.L.; Backes, F.J.; Cheng, G.; McCarter, M.D.; Abdel-Misih, S.; Jones, E.L. The Effect of Preoperative Nutritional Status on Postoperative Complications and Overall Survival in Patients Undergoing Pelvic Exenteration: A Multi-Disciplinary, Multi-Institutional Cohort Study. Am. J. Surg. 2019, 218, 275–280. [Google Scholar] [CrossRef]
- Ogawa, M.; Izawa, K.P.; Satomi-Kobayashi, S.; Tsuboi, Y.; Komaki, K.; Gotake, Y.; Yoshida, N.; Wakida, K.; Uchida, J.; Sakai, Y.; et al. Effects of Postoperative Dietary Intake on Functional Recovery of Patients Undergoing Cardiac Surgery. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Marie-Claude, R.; Bélanger, L.; Lachapelle, P.; Grégoire, J.; Sebastianelli, A.; Plante, M. Effectiveness of an Enhanced Recovery after Surgery Program in Gynaecology Oncologic Surgery: A Single-Centre Prospective Cohort Study. J. Obstet. Gynaecol. Can. 2019, 41, 436–442. [Google Scholar]
- Yeung, S.E.; Fenton, T.R. Colorectal Surgery Patients Prefer Simple Solid Foods to Clear Fluids as the First Postoperative Meal. Dis. Colon Rectum 2014, 52, 1616–1623. [Google Scholar] [CrossRef]
- Henrik, K.; Wilmore, D.W. Multimodal Strategies to Improve Surgical Outcome. Am. J. Surg. 2002, 183, 630–641. [Google Scholar]
- Yamada, S.; Shimada, M.; Utsunomiya, T. Surgical Results of Pancreatoduodenectomy in Elderly Patients. Surg. Today 2012, 42, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Tsaousi, G.; Kokkota, S.; Papakostas, P.; Stavrou, G.; Doumaki, E.; Kotzampassi, K. Body Composition Analysis for Discrimination of Prolonged Hospital Stay in Colorectal Cancer Surgery Patients. Eur. J. Cancer Care 2017, 26, e12491. [Google Scholar] [CrossRef] [PubMed]
- Ilana, F.; German, L.; Castel, H.; Harman-Boehm, I.; Shahar, D.R. Individualized Nutritional Intervention During and after Hospitalization: The Nutrition Intervention Study Clinical Trial. J. Am. Geriatr. Soc. 2011, 59, 10–17. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Parameters | EDIA (n = 46) | DDIA (n = 72) | p-Value |
|---|---|---|---|
| Age (years) (mean ± SD) | 47.5 ± 11.9 | 52.1 ± 11.8 | b 0.039 * |
| Primary diagnosis (n, %) | |||
| Ovarian cancer | 18 (39) | 32 (44) | |
| Endometrial cancer | 18 (39) | 22 (31) | |
| Cervical cancer | 8 (17) | 13 (18) | |
| Uterine cancer | 2 (5) | 5 (7) | |
| Stage of cancer (n, %) | |||
| 1 | 42 (91) | 64 (89) | |
| 2 | 1 (2) | 2 (3) | |
| 3 | 1 (2) | 0 (0) | |
| Advanced | 2(4) | 6 (8) | |
| Comorbidities (n, %) | a 0.021 * | ||
| Hypertension | 13 (28) | 35 (49) | |
| Hypertension and dyslipidemia | 1 (2) | 12 (17) | |
| None | 32 (70) | 25 (34) | |
| ASA classification score (n, %) | a 0.034 * | ||
| 1 | 26 (57) | 16 (22) | |
| 2 & 3 | 20 (43) | 56 (78) | |
| Preoperative nutritional status (mean ± SD) | |||
| Weight (kg) | 63.7 ± 12.7 | 65.9 ± 16.4 | b 0.419 |
| BMI (kg/m2) | 35.6 ± 6.1 | 37.1 ± 6.2 | b 0.193 |
| Muscle mass (kg) | 37.1 ± 4.0 | 37.3 ± 4.7 | b 0.808 |
| Percentage weight loss within 1-month (%) | −3.3 ± 5.8 | −5.9 ± 7.4 | b 0.041 * |
| Total daily energy intake (kcal/day) | 1490 ± 247 | 1319 ± 355 | b 0.005 ** |
| Total daily protein intake (g/day) | 61.9 ± 15.8 | 53.3 ± 16.4 | b 0.006 ** |
| Serum albumin level (g/L) | 39.4 ± 4.4 | 37.4 ± 6.5 | b 0.053 |
| Functional status (mean ± SD) | |||
| Handgrip strength | 17.0 ± 6.3 | 15.2 ± 6.0 | b 0.121 |
| Parameters | EDIA (n = 46) | DDIA (n = 72) | p-Value |
|---|---|---|---|
| Surgical outcomes | |||
| Preoperative whey protein CHO loading (n, %) | a <0.001 ** | ||
| Yes | 45 (98) | 17 (24) | |
| No | 1 (2) | 55 (76) | |
| Method of operation (n, %) | a 0.072 | ||
| Laparoscopic | 27 (59) | 54 (75) | |
| Laparotomy | 19 (41) | 18 (25) | |
| ICU admission (n, %) | a 0.001 ** | ||
| Yes | 1 (2) | 17 (24) | |
| No | 45 (98) | 55 (76) | |
| Postoperative nausea and vomiting (n, %) | a <0.001 ** | ||
| Yes | 7 (15) | 53 (74) | |
| No | 39 (85) | 19 (26) | |
| Postoperative infection (n, %) | 0.402 | ||
| Yes | 1 (2) | 5 (7) | |
| No | 45 (98) | 67 (93) | |
| Operation time (mean ± SD) | 2.3 ± 1.1 | 2.7 ± 1.2 | 0.031 * |
| Postoperative serum albumin (g/L) (mean ± SD) | 32.5 ± 6.1 | 28.5 ± 6.0 | b <0.001 ** |
| Time to start clear fluid (hours) (mean ± SD) | 9.7 ± 2.9 | 19.7 ± 9.0 | b <0.001 ** |
| Time to tolerate solid diet (hours) (mean ± SD) | 21.3 ± 11.6 | 46.6 ± 19.6 | b <0.001** |
| Duration of hospital stays (hours) (mean ± SD) | 114.6 ± 38.4 | 150.0 ± 30.1 | b <0.001 ** |
| Nutritional outcomes | |||
| Weight (kg) | −0.3 ± 2.5 | −1.7 ± 2.3 | b 0.002 ** |
| Muscle mass (kg) | 0.4 ± 1.8 | −0.5 ± 2.4 | b 0.018 * |
| Functional outcomes | |||
| Handgrip strength (kg) | 0.7 ± 4.0 | −1.4 ± 4.8 | b 0.010 * |
| Postoperative Dietary Intake on Postoperative Day-Two Summary Measure | Beta | 95% CI | p-Value |
|---|---|---|---|
| Preoperative whey protein-CHO loading | 0.552 | 407.532–693.712 | <0.001 ** |
| PONV | −0.210 | −330.754–−87.173 | 0.001 ** |
| Age | −0.127 | −9.506–−0.993 | 0.010 ** |
| Time to start clear fluid | −0.182 | −18.347–−2.533 | 0.016 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, C.Y.; Ibrahim, Z.; Abu Zaid, Z.; Mat Daud, Z.A.; Mohd Yusop, N.B.; Mohd Abas, M.N.; Omar, J. Postoperative Dietary Intake Achievement: A Secondary Analysis of a Randomized Controlled Trial. Nutrients 2022, 14, 222. https://doi.org/10.3390/nu14010222
Ho CY, Ibrahim Z, Abu Zaid Z, Mat Daud ZA, Mohd Yusop NB, Mohd Abas MN, Omar J. Postoperative Dietary Intake Achievement: A Secondary Analysis of a Randomized Controlled Trial. Nutrients. 2022; 14(1):222. https://doi.org/10.3390/nu14010222
Chicago/Turabian StyleHo, Chiou Yi, Zuriati Ibrahim, Zalina Abu Zaid, Zulfitri Azuan Mat Daud, Nor Baizura Mohd Yusop, Mohd Norazam Mohd Abas, and Jamil Omar. 2022. "Postoperative Dietary Intake Achievement: A Secondary Analysis of a Randomized Controlled Trial" Nutrients 14, no. 1: 222. https://doi.org/10.3390/nu14010222
APA StyleHo, C. Y., Ibrahim, Z., Abu Zaid, Z., Mat Daud, Z. A., Mohd Yusop, N. B., Mohd Abas, M. N., & Omar, J. (2022). Postoperative Dietary Intake Achievement: A Secondary Analysis of a Randomized Controlled Trial. Nutrients, 14(1), 222. https://doi.org/10.3390/nu14010222