
Acceptability of Plant-Based Diets for People with Chronic Kidney Disease: Perspectives of Renal Dietitians

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample and Recruitment
2.2. Hypothetical Plant-Based Dietary Prescription
2.3. Data Collection and Analysis
3. Results
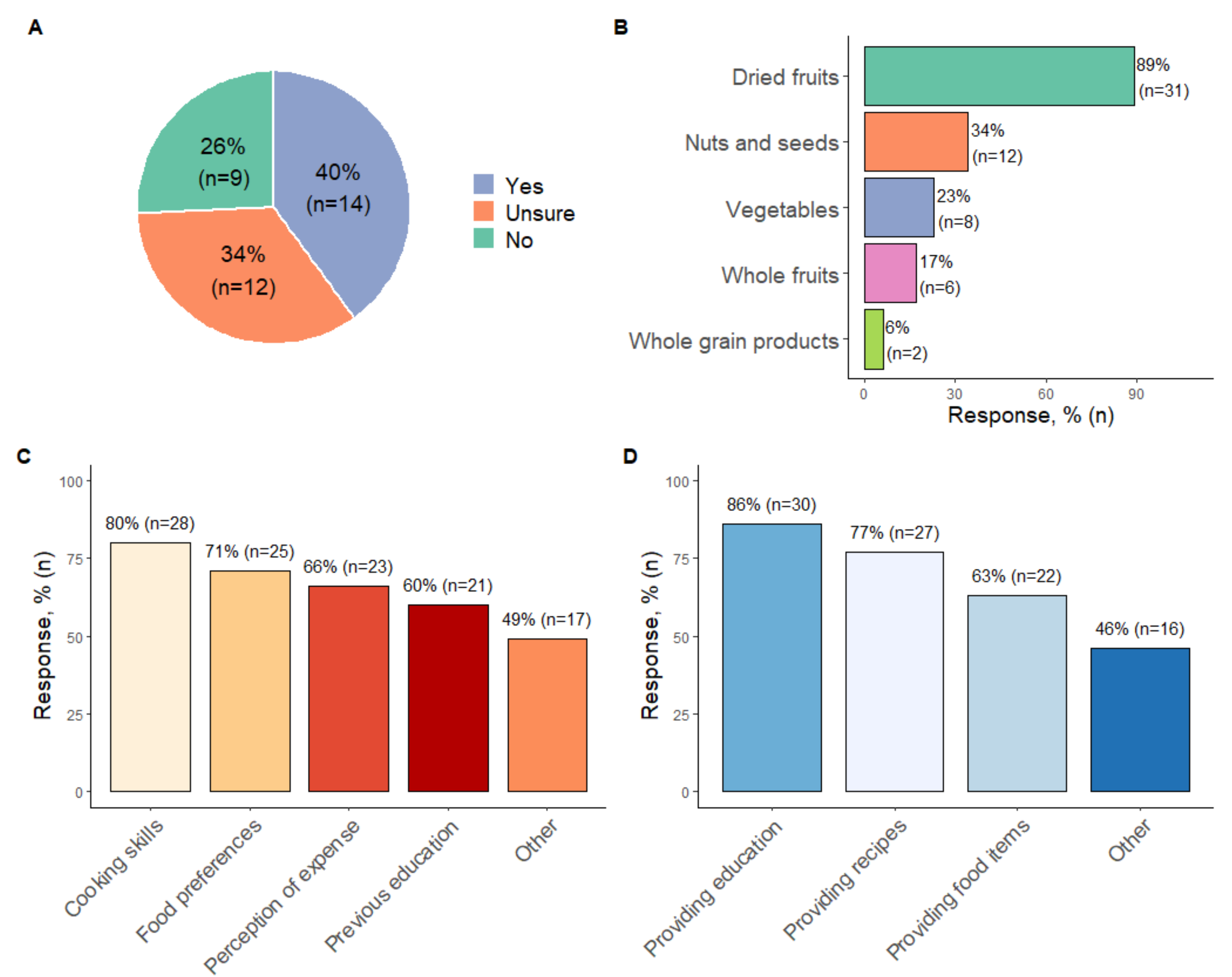
3.1. Online Survey
3.2. In-Depth Interviews
3.2.1. Value of Plant-Based Diets and Strengths of the Hypothetical Dietary Prescription
Addresses Multiple Clinical Concerns
“…so if they are eating this way…glycemic control will be better, hypertension control will be better, proteinuria is likely to be better, …all of the things that you would be worried about.. a plant-based diet is going to help with that”(Dietitian 11)
Shifts Focus from Nutrients to Whole Foods
“We’re very focused on guidelines and millimoles of potassium, but I get concerned … when I provide my education…that people are not able to put that into practice or they get the message wrong and then end up cutting out things unnecessarily because they think it’s bad for them…It [the hypothetical dietary prescription] focuses on making healthy food choices because I think people are misunderstanding the information about potassium and phosphate and see it as cutting out fruit and vegetables…and that is a very big concern…When in fact you want to maintain a healthy diet overall and variety… it [the hypothetical dietary prescription] allows for flexibility, and it allows people to transition from receiving some abstract information about food into this is what I’m going to eat today.”(Dietitian 10)
A Need for Practical Complementary Resources
“The recipes are a great suggestion because there is no point giving this if people don’t have the skills or the knowledge of how to incorporate those foods to make it into a meal… demonstrating it is achievable.”(Dietitian 5)
“I like the variety… they have this list of foods that they can swap, like each meal, each fruit serve out with, so that really helps.”(Dietitian 5)
3.2.2. Barriers and Enablers to Implementation
Organisational Norms and System Inadequacies Are Barriers
“I think it would be crucial about our follow up … in our pre-dialysis clinic, we do not see patients for like another two to three months, just because of our wait times…”(Dietitian 7)
“Generally, dietitians do not have the time to do these sorts of detailed meal plans.”(Dietitian 3)
“...you would need to spend a fair bit of time making sure that the patients understand and checking it.”(Dietitian 2)
Differing Nutrition Philosophies and Perceptions about Diet Are Barriers
“On this sort of diet [high plant-based diet] … that perception, that they have to restrict them because of the potassium, and doctors or people, other people who might also have that perception and not, who do not sort of understand the difference in bioavailability.”(Dietitian 8)
“Depending on the medication they’re on, they can be more susceptible to hyperkalaemia regardless of what they’re eating...”(Dietitian 11)
“You have a patient who is very compliant with previous dietary recommendations; they often do not like to go against that.”(Dietitian 4)
“Trying to move towards [a plant-based diet]…which will undoubtedly include some of the foods that a lot of them just will not touch. It has been entrenched in them … I cannot eat that sort of food…”(Dietitian 7)
Supportive Multidisciplinary Networks Facilitates Implementation
“[Implementation] would [need] convincing other health staff about the research because many others other than dietitians provide dietary education...you have got doctors…or nurses. So making sure they are aware of the evidence …because …if a patient hears something from their doctor, they [the patient] will listen to them over what we [dietitians] recommend so, I think making sure that the message is consistent.”(Dietitian 4)
Timing of Implementation
“[if] they are preparing for dialysis… patients can be quite overwhelmed …, so I think [managing] the complexity of the diet you are trying to prescribe, but also managing their cognitive and emotional states as well can be quite challenging.”(Dietitian 11)
“… they’re unlikely to have seen a dietitian at CKD stage 3, so you know they don’t have all those restrictions placed on them…they typically are more motivated as they don’t want dialysis and are more likely to benefit from using nutrition as a preventative to delay disease progression…I think if you can get them early, then I think that’s wonderful.”(Dietitian 1)
‘Marketing’ the Plant-Based Approach
“I think if we are very clear on the outcomes we are looking at, we could sell this to patients…what outcomes can we expect because if people know that it might actually maintain their kidney function for another two years, or three years, or five years, that could be a very big motivator for them. But if we are just talking about general health, they already feel okay, especially when they are in the earlier stages.”(Dietitian 11)
“… a starting point of …I am having x amount of plant-based foods… over the next two weeks can I increase it by an extra 5 or 10 foods a week…so it can be a little bit more of a step guided approach ... that could be another strategy to help them with goal setting.”.(Dietitian 11)
“Having it … mapped out …how many meals they like to have over the day and being able to fit it in that way… some people might find it a little bit easier to …actually to see how it fits into … breakfast, lunch and dinner, or how many meals a day.”(Dietitian 11)
“I think it’s good how you have under free vegetables you say one serve is one cup or half a cup cooked. I think its nice to have a standard serve for as many of the foods within a category.”(Dietitian 10)
“Pictures…. I think pictures are really important …particularly with literacy and also non-English speaking patients.”(Dietitian 7)
4. Discussion
5. Relevance to Practice
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chan, M.; Kelly, J.; Tapsell, L. Dietary Modeling of Foods for Advanced CKD Based on General Healthy Eating Guidelines: What Should Be on the Plate? Am. J. Kidney Dis. 2017, 69, 436–450. [Google Scholar] [CrossRef]
- Lambert, K.; Mansfield, K.; Mullan, J. How do patients and carers make sense of renal dietary advice? A qualitative exploration. J. Ren. Care 2018, 44, 238–250. [Google Scholar] [CrossRef]
- Naismith, D.J.; Braschi, A. An investigation into the bioaccessibility of potassium in unprocessed fruits and vegetables. Int. J. Food Sci. Nutr. 2008, 59, 438–450. [Google Scholar] [CrossRef] [PubMed]
- Picard, K. Potassium Additives and Bioavailability: Are We Missing Something in Hyperkalemia Management? J. Ren. Nutr. 2019, 29, 350–353. [Google Scholar] [CrossRef] [PubMed]
- Bernier-Jean, A.; Wong, G.; Saglimbene, V.; Ruospo, M.; Palmer, S.C.; Natale, P.; Garcia-Larsen, V.; Johnson, D.W.; Tonelli, M.; Hegbrant, J.; et al. Dietary Potassium Intake and All-Cause Mortality in Adults Treated with Hemodialysis. Clin. J. Am. Soc. Nephrol. 2021, 16, 1851–1861. [Google Scholar] [CrossRef]
- Kelly, J.T.; Palmer, S.C.; Wai, S.N.; Ruospo, M.; Carrero, J.J.; Campbell, K.L.; Strippoli, G.F. Healthy Dietary Patterns and Risk of Mortality and ESRD in CKD: A Meta-Analysis of Cohort Studies. Clin. J. Am. Soc. Nephrol. 2017, 12, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, T.; Liu, Y.; Crews, D.C. Dietary Patterns and CKD Progression. Blood Purif 2016, 41, 117–122. [Google Scholar] [CrossRef]
- Guldris, S.C.; Parra, E.G.; Amenós, A.C. Gut microbiota in chronic kidney disease. Nefrología 2017, 37, 9–19. [Google Scholar] [CrossRef]
- Koppe, L.; Fouque, D.; Soulage, C.O. The Role of Gut Microbiota and Diet on Uremic Retention Solutes Production in the Context of Chronic Kidney Disease. Toxins 2018, 10, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossi, M.; Johnson, D.W.; Xu, H.; Carrero, J.J.; Pascoe, E.; French, C.; Campbell, K.L. Dietary protein-fiber ratio associates with circulating levels of indoxyl sulfate and p-cresyl sulfate in chronic kidney disease patients. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.-Y.; Tarng, D.-C. Diet, gut microbiome and indoxyl sulphate in chronic kidney disease patients. Nephrology 2018, 23, 16–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Alessandro, C.; Piccoli, G.B.; Cupisti, A. The “phosphorus pyramid”: A visual tool for dietary phosphate management in dialysis and CKD patients. BMC Nephrol. 2015, 16, 9. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G. Improving the Quality of Web Surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jager, J.; Putnick, D.L.; Bornstein, M.H. More than just convenient: The scientific merits of homogeneous convenience samples. Monogr. Soc. Res. Child. Dev. 2017, 82, 13–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, D.; Hyde, E.; Debelius, J.W.; Morton, J.T.; Gonzalez, A.; Ackermann, G.; Aksenov, A.A.; Behsaz, B.; Brennan, C.; Chen, Y.; et al. American Gut: An Open Platform for Citizen Science Microbiome Research. mSystems 2018, 3, e00031-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Health and Medical Research Council. Australian Dietary Guidelines. 2013. Available online: https://www.nhmrc.gov.au/_files_nhmrc/file/publications/n55_australian_dietary_guidelines1.pdf (accessed on 4 January 2022).
- Ash, S.; Campbell, K.; MacLaughlin, H.; McCoy, E.; Chan, M.; Anderson, K.; Corke, K.; Dumont, R.; Lloyd, L.; Meade, A.; et al. Evidence based practice guidelines for the nutritional management of chronic kidney disease. Nutr. Diet. 2006, 63, S33–S45. [Google Scholar] [CrossRef] [Green Version]
- Ash, S.; Campbell, K.L.; Bogard, J.; Millichamp, A. Nutrition prescription to achieve positive outcomes in chronic kidney disease: A systematic review. Nutrients 2014, 6, 416–451. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Elo, S.; Kyngas, H. The qualitative content analysis process. J. Adv. Nurs 2008, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Dedoose Version 8.3.17, w.a.f.m., Analyzing, and Presenting Qualitative and Mixed Method Research Data; SocioCultural Research Consultants, LLC: Los Angeles, CA, USA, 2020.
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Joshi, S.; Shah, S.; Kalantar-Zadeh, K. Adequacy of Plant-Based Proteins in Chronic Kidney Disease. J. Ren. Nutr. 2019, 29, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Khor, B.-H.; Tallman, D.A.; Karupaiah, T.; Khosla, P.; Chan, M.; Kopple, J.D. Nutritional Adequacy of Animal-Based and Plant-Based Asian Diets for Chronic Kidney Disease Patients: A Modeling Study. Nutrients 2021, 13, 3341. [Google Scholar] [CrossRef] [PubMed]
- Hand, R.K. Workforce needs and estimated costs/savings for nutrition care in chronic kidney disease–stage 3 through maintenance dialysis. In Seminars in Dialisis; Wiley-Blackwell Publishing Ltd: Hoboken, NJ, USA, 2021; pp. 1–9. [Google Scholar] [CrossRef]
- Vergili, J.M.; Wolf, R.L. Nutrition practices of renal dietitians in hemodialysis centers throughout the United States: A descriptive study. J. Ren. Nutr. 2010, 20, e1–e8. [Google Scholar] [CrossRef]
- Trudel, T.; McCune, A.; Donahue, K.; Zuberbuhler, L.; Farmer, A.; Mager, D. Variables influencing adoption of practice-based guidelines in Canadian renal dietetic practice. J. Ren. Nutr. 2010, 20, 235–242. [Google Scholar] [CrossRef]
- Hall-McMahon, E.J.; Campbell, K.L. Have renal dietitians successfully implemented evidence-based guidelines into practice? A survey of dietitians across Australia and New Zealand. J. Ren. Nutr. 2012, 22, 584–591. [Google Scholar] [CrossRef] [PubMed]
- British Renal Society, A Multi-Professional Renal Workforce Plan for Adults and Children with Kidney Disease. 2020. Available online: https://britishrenal.org/wp-content/uploads/2020/10/FINAL-WFP-OCT-2020.pdf (accessed on 15 December 2021).
- Notaras, S.; Galea, L.; Lee, P.; Mak, M.; Lambert, K.; Makris, A. The association between dietetic consultation and time to dialysis for patients attending a pre-dialysis clinic: A retrospective cohort study. Nephrology 2020, 25, 390–397. [Google Scholar] [CrossRef]
- Goldstein, M.; Yassa, T.; Dacouris, N.; McFarlane, P. Multidisciplinary predialysis care and morbidity and mortality of patients on dialysis. Am. J. Kidney Dis. 2004, 44, 706–714. [Google Scholar] [CrossRef]
- Lee, W.-C.; Lee, Y.-T.; Li, L.-C.; Ng, H.-Y.; Kuo, W.-H.; Lin, P.-T.; Liao, Y.-C.; Chiou, T.T.-Y.; Lee, C.-T. The Number of Comorbidities Predicts Renal Outcomes in Patients with Stage 3-5 Chronic Kidney Disease. J. Clin. Med. 2018, 7, 493. [Google Scholar] [CrossRef] [Green Version]
- Sladdin, I.; Chaboyer, W.; Ball, L. Patients’ perceptions and experiences of patient-centred care in dietetic consultations. J. Hum. Nutr. Diet. 2018, 31, 188–196. [Google Scholar] [CrossRef]
- Taylor, D.M.; Fraser, S.; Dudley, C.; Oniscu, G.C.; Tomson, C.; Ravanan, R.; Roderick, P.; the ATTOM Investigators. Health literacy and patient outcomes in chronic kidney disease: A systematic review. Nephrol. Dial. Transplant. 2017, 33, 1545–1558. [Google Scholar] [CrossRef] [Green Version]
- Lambert, K.; Mullan, J.; Mansfield, K.; Lonergan, M. Comparison of the extent and pattern of cognitive impairment among predialysis, dialysis and transplant patients: A cross-sectional study from Australia. Nephrology 2017, 22, 899–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morony, S.; Flynn, M.; McCaffery, K.J.; Jansen, J.; Webster, A.C. Readability of Written Materials for CKD Patients: A Systematic Review. Am. J. Kidney Dis. 2015, 65, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Beto, J.A.; Schury, K.A.; Bansal, V.K. Strategies to promote adherence to nutritional advice in patients with chronic kidney disease: A narrative review and commentary. Int. J. Nephrol. Renov. Dis. 2016, 9, 21–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, R.; James, H.; Burns, A. Adhering to behaviour change in older pre-dialysis populations-what do patients think? A qualitative study. J. Ren. Care 2012, 38, 34–42. [Google Scholar] [CrossRef]
- Rinaldi, S.; Campbell, E.E.; Fournier, J.; O’Connor, C.; Madill, J. A Comprehensive Review of the Literature Supporting Recommendations From the Canadian Diabetes Association for the Use of a Plant-Based Diet for Management of Type 2 Diabetes. Can. J. Diabetes 2016, 40, 471–477. [Google Scholar] [CrossRef]
- Asher, K.E.; Doucet, S.; Luke, A. Registered dietitians’ perceptions and use of the plant-based recommendations in the 2019 Canada’s Food Guide. J. Hum. Nutr. Diet. 2021, 34, 715–723. [Google Scholar] [CrossRef]
- Janse Van Rensburg, L.M.; Wiles, N.L. The opinion of KwaZulu-Natal dietitians regarding the use of a whole-foods plant-based diet in the management of non-communicable diseases. S. Afr. J. Clin. Nutr. 2021, 34, 60–64. [Google Scholar] [CrossRef] [Green Version]
- Betz, M.V.; Nemec, K.B.; Zisman, A.L. Plant-based Diets in Kidney Disease: Nephrology Professionals’ Perspective. J. Ren. Nutr. 2021; in press. [Google Scholar] [CrossRef]

{kind=link}
| Characteristics | Interview (n = 11) | Survey (n = 35) |
|---|---|---|
| Gender (female, %) | 11 (100%) | - |
| Age (range) | 25–64 | - |
| Years actively working as a renal dietitian (median-IQR) | 9.17 (3.67–27.50) | 7 (3–12.25) |
| Current employment status (Full time equivalent: median, IQR) | 0.6 (0.3–1.0) | - |
| Practice setting | ||
| Community settings | 1 (9%) | - |
| Private practice | 1 (9%) | - |
| Public health/hospitals | 10 (91%) | - |
| Area of practice | ||
| Early CKD | 2 (18.2%) | 11 (31.4%) |
| Pre-dialysis | 7 (63.6%) | 23 (65.7%) |
| Haemodialysis | 8 (72.7%) | 31 (88.6%) |
| Peritoneal dialysis | 5 (45.5%) | 20 (57.1%) |
| Renal transplant | 4 (36.4%) | 12 (34.3%) |
| Renal supportive care/palliative care | 5 (45.5%) | 13 (37.1%) |
| Other | 0 (0%) | 3 (8.6%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stanford, J.; Zuck, M.; Stefoska-Needham, A.; Charlton, K.; Lambert, K. Acceptability of Plant-Based Diets for People with Chronic Kidney Disease: Perspectives of Renal Dietitians. Nutrients 2022, 14, 216. https://doi.org/10.3390/nu14010216
Stanford J, Zuck M, Stefoska-Needham A, Charlton K, Lambert K. Acceptability of Plant-Based Diets for People with Chronic Kidney Disease: Perspectives of Renal Dietitians. Nutrients. 2022; 14(1):216. https://doi.org/10.3390/nu14010216
Chicago/Turabian StyleStanford, Jordan, Mikaela Zuck, Anita Stefoska-Needham, Karen Charlton, and Kelly Lambert. 2022. "Acceptability of Plant-Based Diets for People with Chronic Kidney Disease: Perspectives of Renal Dietitians" Nutrients 14, no. 1: 216. https://doi.org/10.3390/nu14010216
APA StyleStanford, J., Zuck, M., Stefoska-Needham, A., Charlton, K., & Lambert, K. (2022). Acceptability of Plant-Based Diets for People with Chronic Kidney Disease: Perspectives of Renal Dietitians. Nutrients, 14(1), 216. https://doi.org/10.3390/nu14010216