
Higher Iron Intake Is Independently Associated with Obesity in Younger Japanese Type-2 Diabetes Mellitus Patients

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Dietary and Physical Assessment
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
3.1. Characteristics of the Study Participants
3.2. Correlations between Intake of Iron and Food Groups
3.3. Multivariate Analysis of Associations between Iron Intake and Obesity Adjusted by Nutrient Intake
3.4. Correlations between Intake of Fiber and Food Groups
3.5. Multivariate Analysis of Associations between Iron Intake and Obesity Adjusted by Food Group
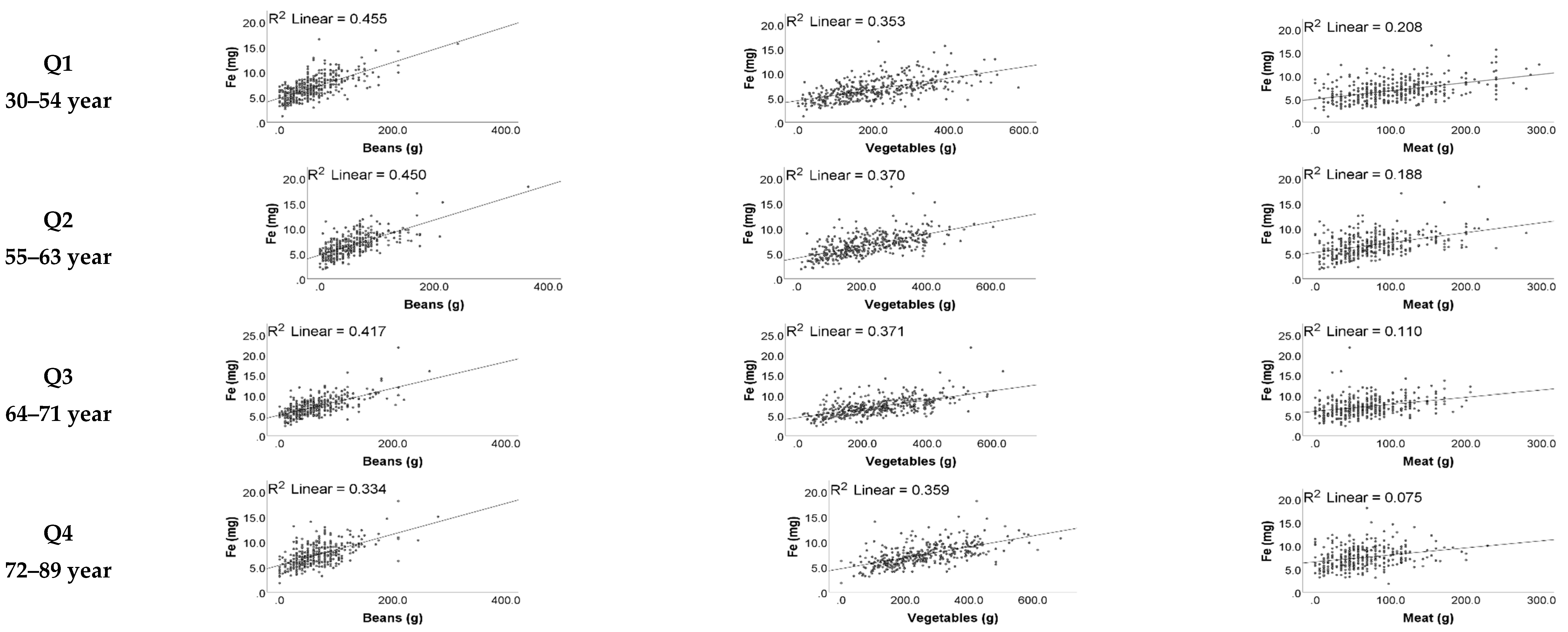
3.6. Relationships between Intake of Iron and Food Groups
3.7. Multivariate Analysis of Associations between Meat Intake and Obesity
3.8. Stratified Multivariate Analysis of Associations between Iron Intake and Obesity Adjusted by Nutrient Intake
3.9. Multivariate Analysis of Associations between Iron Intake and Overweight and Obesity According to World Health Organization (WHO) Definitions Adjusted by Nutrient Intake
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Apovian, C.M.; Okemah, J.; O’Neil, P.M. Body Weight Considerations in the Management of Type 2 Diabetes. Adv. Ther. 2018, 36, 44–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García, O.P.; Long, K.Z.; Rosado, J.L. Impact of micronutrient deficiencies on obesity. Nutr. Rev. 2009, 67, 559–572. [Google Scholar] [CrossRef]
- Zhao, L.; Zhang, X.; Shen, Y.; Fang, X.; Wang, Y.; Wang, F. Obesity and iron deficiency: A quantitative meta-analysis. Obes. Rev. 2015, 16, 1081–1093. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos Vieira, D.A.; Sales, C.H.; Cesar, C.L.G.; Marchioni, D.M.; Fisberg, R.M. Influence of Haem, Non-Haem, and Total Iron Intake on Metabolic Syndrome and Its Components: A Population-Based Study. Nutrients 2018, 10, 314. [Google Scholar] [CrossRef] [Green Version]
- de Oliveira Otto, M.C.; Alonso, A.; Lee, D.-H.; Delclos, G.L.; Bertoni, A.G.; Jiang, R.; Lima, J.A.; Symanski, E.; Jacobs, D.R.; Nettleton, J.A. Dietary Intakes of Zinc and Heme Iron from Red Meat, but Not from Other Sources, Are Associated with Greater Risk of Metabolic Syndrome and Cardiovascular Disease. J. Nutr. 2012, 142, 526–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, Z.; Wu, F.; Lu, Y.; Wu, C.; Wang, Z.; Zang, J.; Guo, C.; Jia, X.; Yao, J.; Peng, H.; et al. Total and Nonheme Dietary Iron Intake Is Associated with Metabolic Syndrome and Its Components in Chinese Men and Women. Nutrients 2018, 10, 1663. [Google Scholar] [CrossRef] [Green Version]
- Esfandiar, Z.; Hosseini-Esfahani, F.; Mirmiran, P.; Habibi-Moeini, A.-S.; Azizi, F. Red meat and dietary iron intakes are associated with some components of metabolic syndrome: Tehran Lipid and Glucose Study. J. Transl. Med. 2019, 17, 313. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Ma, X.; Li, M.; Yan, S.; Zhao, H.; Pan, Y.; Wang, C.; Yao, Y.; Jin, L.; Li, B. Association between dietary mineral nutrient intake, body mass index, and waist circumference in U.S. adults using quantile regression analysis NHANES 2007–2014. PeerJ 2020, 8, e9127. [Google Scholar] [CrossRef]
- Liu, J.; Zhu, X.; Fulda, K.G.; Chen, S.; Tao, M.-H. Comparison of Dietary Micronutrient Intakes by Body Weight Status among Mexican-American and Non-Hispanic Black Women Aged 19–39 Years: An Analysis of NHANES 2003–2014. Nutrients 2019, 11, 2846. [Google Scholar] [CrossRef] [Green Version]
- Głąbska, D.; Włodarek, D.; Kołota, A.; Czekajło, A.; Drozdzowska, B.; Pluskiewicz, W. Assessment of mineral intake in the diets of Polish postmenopausal women in relation to their BMI—The RAC-OST-POL study. J. Health Popul. Nutr. 2016, 35, 23. [Google Scholar] [CrossRef] [Green Version]
- Ozato, N.; Saito, S.; Yamaguchi, T.; Katashima, M.; Tokuda, I.; Sawada, K.; Katsuragi, Y.; Imoto, S.; Ihara, K.; Nakaji, S. Association between Nutrients and Visceral Fat in Healthy Japanese Adults: A 2-Year Longitudinal Study Brief Title: Micronutrients Associated with Visceral Fat Accumulation. Nutrients 2019, 11, 2698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKay, J.; Ho, S.; Jane, M.; Pal, S. Overweight & obese Australian adults and micronutrient deficiency. BMC Nutr. 2020, 6, 12. [Google Scholar] [CrossRef]
- Kobayashi, M.; Yamazaki, K.; Hirao, K.; Oishi, M.; Kanatsuka, A.; Yamauchi, M.; Takagi, H.; Kawai, K. The status of diabetes control and antidiabetic drug therapy in Japan—A cross-sectional survey of 17,000 patients with diabetes mellitus (JDDM 1). Diabetes Res. Clin. Pract. 2006, 73, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Yoshimura, Y.; Kaimoto, T.; Kunii, D.; Komatsu, T.; Yamamoto, S. Validation of a Food Frequency Questionnaire Based on Food Groups for Estimating Individual Nutrient Intake. Jpn. J. Nutr. Diet. 2001, 59, 221–232. [Google Scholar] [CrossRef]
- Horikawa, C.; Yoshimura, Y.; Kamada, C.; Tanaka, S.; Tanaka, S.; Hanyu, O.; Araki, A.; Ito, H.; Tanaka, A.; Ohashi, Y.; et al. Dietary Sodium Intake and Incidence of Diabetes Complications in Japanese Patients with Type 2 Diabetes: Analysis of the Japan Diabetes Complications Study (JDCS). J. Clin. Endocrinol. Metab. 2014, 99, 3635–3643. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Murase, N. Validity and reliability of Japanese version of International Physical Activity Questionnaire. J. Health Welf. Stat. 2002, 49, 1–9. Available online: https://ci.nii.ac.jp/naid/10030213124/ (accessed on 28 June 2021).
- Yuji, M. New Criteria for “Obesity Disease” in Japan: The Examination Committee of Criteria for ‘Obesity Disease’ in Japan, Japan Society for the Study of Obesity. New Criteria for ‘Obesity Disease’ in Japan. Circ. J. 2002, 66, 987–992. [Google Scholar] [CrossRef] [Green Version]
- Jih, J.; Mukherjea, A.; Vittinghoff, E.; Nguyen, T.T.; Tsoh, J.; Fukuoka, Y.; Bender, M.S.; Tseng, W.; Kanaya, A.M. Using appropriate body mass index cut points for overweight and obesity among Asian Americans. Prev. Med. 2014, 65, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Felipe, A.; Guadalupe, E.; Druso, P.; Carlos, M.; Pablo, S.; Oscar, C.; Luis, V.; Diego, M.; Jaime, R.; Inés, U.; et al. Serum Ferritin Is Associated with Metabolic Syndrome and Red Meat Consumption. Oxid. Med. Cell. Longev. 2015, 2015, 769739. [Google Scholar] [CrossRef] [Green Version]
- Eshak, E.S.; Iso, H.; Maruyama, K.; Muraki, I.; Tamakoshi, A. Associations between dietary intakes of iron, copper and zinc with risk of type 2 diabetes mellitus: A large population-based prospective cohort study. Clin. Nutr. 2017, 37, 667–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagata, C.; Wada, K.; Tamura, T.; Konishi, K.; Goto, Y.; Koda, S.; Kawachi, T.; Tsuji, M.; Nakamura, K. Dietary soy and natto intake and cardiovascular disease mortality in Japanese adults: The Takayama study. Am. J. Clin. Nutr. 2016, 105, 426–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messina, M. Soy and Health Update: Evaluation of the Clinical and Epidemiologic Literature. Nutrients 2016, 8, 754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scrimshaw, N.S. Iron Deficiency. Sci. Am. 1991, 265, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Hallberg, L.; Hulthén, L. Prediction of dietary iron absorption: An algorithm for calculating absorption and bioavailability of dietary iron. Am. J. Clin. Nutr. 2000, 71, 1147–1160. [Google Scholar] [CrossRef]
- Cepeda-Lopez, A.C.; Melse-Boonstra, A.; Zimmermann, M.B.; Herter-Aeberli, I. In overweight and obese women, dietary iron absorption is reduced and the enhancement of iron absorption by ascorbic acid is one-half that in normal-weight women. Am. J. Clin. Nutr. 2015, 102, 1389–1397. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| All Participants n = 1567 | 30–54 Year n = 401 | 55–63 Year n = 396 | 64–71 Year n = 405 | 72–89 Year n = 365 | p Trend | |
|---|---|---|---|---|---|---|
| Age (years) | 62.3 (11.6) | 46.9 (5.5) | 59.3 (2.6) | 67.01 (2.2) | 77.20 (4.0) | 0.000 |
| Sex (Men, %) | 988 (63.1%) | 291 (72.6%) | 252 (63.6%) | 249 (61.5%) | 196 (53.7%) | <0.001 |
| BMI (kg/m2) | 25.8 (4.6) | 28.3 (5.2) | 25.9 (4.6) | 24.7 (3.8) | 24.4 (3.5) | 0.000 |
| Diabetes duration (years) | 11.8 (7.8) | 8.3 (6.1) | 10.5 (6.5) | 13.2 (7.6) | 15.4 (8.8) | <0.001 |
| METs (hour/week) | 29.2 (39.6) | 25.3 (39.4) | 28.9 (39.8) | 32.6 (39.6) | 30.0 (39.3) | 0.001 |
| Current smoking (%) | 303 (19.3%) | 126 (31.4%) | 90 (22.7%) | 53 (13.1%) | 34 (9.3%) | <0.001 |
| Current drinking (%) | 732 (46.7%) | 203 (50.6%) | 193 (48.7%) | 201 (49.6%) | 135 (37%) | <0.001 |
| Current insulin treatment (%) | 451 (28.8%) | 98 (24.4%) | 106 (26.8%) | 105 (25.9%) | 142 (38.9%) | <0.001 |
| Current OHA and/or GLP treatment (%) | 1279 (81.6%) | 328 (81.8%) | 328 (82.8%) | 342 (84.4%) | 281 (77%) | 0.051 |
| Energy (kcal/day) | 1764.1 (439.1) | 1807.5 (453.5) | 1744.7 (456.5) | 1735.2 (416.4) | 1769.7 (425.8) | 0.276 |
| Protein (g/day) | 65.1 (18.6) | 65.3 (19.5) | 63.2 (19.5) | 65.0 (18.2) | 67.1 (17.0) | 0.036 |
| Fat (g/day) | 58.3 (19.7) | 64.3 (21.9) | 57.1 (19.9) | 54.8 (17.4) | 56.8 (17.7) | <0.001 |
| Saturated fat (g/day) | 17.9 (6.6) | 19.8 (7.5) | 17.4 (6.5) | 16.9 (6.1) | 17.4 (5.9) | 0.823 |
| Carbohydrate (g/day) | 229.2 (59.4) | 225.3 (60.6) | 226.9 (60.9) | 229.5 (54.9) | 235.7 (61.1) | 0.006 |
| Fe intake (mg/day) | 7.0 (2.1) | 6.7 (2.2) | 6.6 (2.1) | 7.1 (2.1) | 7.4 (2.1) | <0.001 |
| Na intake (mg/day) | 3387.0 (1252.2) | 3080.8 (1147.0) | 3246.6 (1154.1) | 3471.7 (1212.6) | 3781.5 (1390.8) | <0.001 |
| Soluble fiber (g/day) | 2.9 (1.0) | 2.6 (0.9) | 2.8 (0.9) | 3.0 (0.9) | 3.1 (1.0) | <0.001 |
| Insoluble fiber (g/day) | 9.0 (2.9) | 8.2 (2.7) | 8.6 (2.8) | 9.5 (2.9) | 9.9 (3.1) | 0.000 |
| Beans (g/day) | 60.4 (42.1) | 55.3 (42.1) | 56.8 (41.9) | 62.5 (42.6) | 67.5 (40.7) | <0.001 |
| Vegetables (g/day) | 230.5 (118.2) | 204.9 (114.3) | 218.6 (111.2) | 245.5 (121.4) | 255.0 (119.4) | <0.001 |
| Fruits (g/day) | 84.1 (71.3) | 49.6 (57.3) | 78.22 (67.6) | 101.7 (73.4) | 108.7 (71.1) | 0.000 |
| Meat (g/day) | 75.9 (49.6) | 101.7 (56.9) | 74.6 (47.8) | 64.8 (41.4) | 61.1 (39.2) | 0.000 |
| Seafood (g/day) | 72.8 (45.3) | 59.6 (42.8) | 68.8 (44.3) | 80.0 (44.9) | 83.7 (45.4) | 0.000 |
| Age Group | Fe Intake (Quartile) | Model 1 | Model 2 | Model 3 |
|---|---|---|---|---|
| OR (CI) | OR (CI) | OR (CI) | ||
| All participants | Q1 (low) | Reference | Reference | Reference |
| Q2 | 0.788 (0.593–1.047) | 0.643 (0.485–0.992) | 0.828 (0.570–1.205) | |
| Q3 | 0.909 (0.681–1.214) | 0.782 (0.518–1.180) | 1.080 (0.685–1.704) | |
| Q4 (high) | 0.805 (0.606–1.071) | 0.726 (0.432–1.219) | 1.270 (0.681–2.366) | |
| p trend | 0.315 | 0.259 | 0.233 | |
| 30–54 years | Q1 (low) | Reference | Reference | Reference |
| Q2 | 0.607 (0.347–1.063) | 0.597 (0.310–1.151) | 0.813 (0.405–1.631) | |
| Q3 | 1.090 (0.573–2.076) | 1.279 (0.557–2.936) | 2.277 (0.888–5.840) | |
| Q4 (high) | 1.194 (0.632–2.258) | 1.482 (0.514–4.272) | 3.641 (1.020–12.990) | |
| p trend | 0.124 | 0.060 | 0.011 | |
| 55–63 years | Q1 (low) | Reference | Reference | Reference |
| Q2 | 0.916 (0.529–1.586) | 0.788 (0.411–1.512) | 0.904 (0.456–1.790) | |
| Q3 | 0.901 (0.527–1.514) | 0.623 (0.300–1.294) | 0.790 (0.354–1.764) | |
| Q4 (high) | 0.718 (0.414–1.245) | 0.429 (0.164–1.124) | 0.620 (0.207–1.854) | |
| p trend | 0.703 | 0.377 | 0.847 | |
| 64–71 years | Q1 (low) | Reference | Reference | Reference |
| Q2 | 0.656 (0.378–1.139) | 0.523 (0.278–0.981) | 0.605 (0.308–1.190) | |
| Q3 | 0.827 (0.468–1.462) | 0.524 (0.248–1.107) | 0.685 (0.299–1.566) | |
| Q4 (high) | 0.778 (0.447–1.355) | 0.493 (0.195–1.244) | 0.801 (0.261–2.457) | |
| p trend | 0.515 | 0.218 | 0.408 | |
| 72–89 years | Q1 (low) | Reference | Reference | Reference |
| Q2 | 1.174 (0.629–2.194) | 1.080 (0.535–2.182) | 1.281 (0.617–2.662) | |
| Q3 | 0.918 (0.503–1.675) | 0.823 (0.383–1.766) | 1.141 (0.487–2.673) | |
| Q4 (high) | 0.710 (0.390–1.291) | 0.615 (0.233–1.625) | 1.121 (0.348–3.614) | |
| p trend | 0.406 | 0.574 | 0.913 |
| Age Group | Fe Intake (Quartile) | Model 1 | Model 2 | Model 3 | Model 4 |
|---|---|---|---|---|---|
| OR (CI) | OR (CI) | OR (CI) | OR (CI) | ||
| All participants | Q1 (low) | Reference | Reference | Reference | Reference |
| Q2 | 0.613 (0.450–0.834) | 0.742 (0.537–1.025) | 0.638 (0.465–0.874) | 0.776 (0.558–1.079) | |
| Q3 | 0.602 (0.428–0.847) | 0.837 (0.574–1.220) | 0.654 (0.454–0.941) | 0.916 (0.615–1.365) | |
| Q4 (high) | 0.453 (0.300–0.684) | 0.751 (0.467–1.209) | 0.531 (0.330–0.854) | 0.892 (0.522–1.524) | |
| p trend | 0.001 | 0.337 | 0.024 | 0.428 | |
| 30–54 years | Q1 (low) | Reference | Reference | Reference | Reference |
| Q2 | 0.489 (0.262–0.913) | 0.577 (0.300–1.109) | 0.583 (0.306–1.110) | 0.679 (0.348–1.327) | |
| Q3 | 0.830 (0.391–1.762) | 1.152 (0.496–2.676) | 1.224 (0.533–2.809) | 1.651 (0.669–4.075) | |
| Q4 (high) | 0.809 (0.336–1.946) | 1.246 (0.454–3.420) | 1.686 (0.560–5.074) | 2.528 (0.755–8.463) | |
| p trend | 0.104 | 0.088 | 0.042 | 0.023 | |
| 55–63 years | Q1 (low) | Reference | Reference | Reference | Reference |
| Q2 | 0.781 (0.424–1.438) | 1.030 (0.537–1.978) | 0.765 (0.411–1.424) | 1.018 (0.524–1.977) | |
| Q3 | 0.577 (0.294–1.133) | 0.867 (0.411–1.830) | 0.552 (0.270–1.131) | 0.846 (0.384–1.864) | |
| Q4 (high) | 0.357 (0.156–0.817) | 0.648 (0.251–1.674) | 0.329 (0.128–0.844) | 0.618 (0.213–1.795) | |
| p trend | 0.102 | 0.722 | 0.137 | 0.736 | |
| 64–71 years | Q1 (low) | Reference | Reference | Reference | Reference |
| Q2 | 0.519 (0.281–0.956) | 0.659 (0.346–1.258) | 0.557 (0.300–1.034) | 0.722 (0.374–1.395) | |
| Q3 | 0.491 (0.244–0.989) | 0.707 (0.328–1.522) | 0.593 (0.283–1.245) | 0.886 (0.391–2.008) | |
| Q4 (high) | 0.437 (0.194–0.986) | 0.837 (0.315–2.220) | 0.630 (0.246–1.612) | 1.286 (0.423–3.907) | |
| p trend | 0.132 | 0.532 | 0.294 | 0.384 | |
| 72–89 years | Q1 (low) | Reference | Reference | Reference | Reference |
| Q2 | 0.938 (0.473–1.862) | 1.054 (0.522–2.127) | 0.977 (0.484–1.975) | 1.099 (0.535–2.257) | |
| Q3 | 0.619 (0.303–1.266) | 0.789 (0.364–1.712) | 0.657 (0.310–1.392) | 0.838 (0.374–1.879) | |
| Q4 (high) | 0.423 (0.174–1.030) | 0.613 (0.226–1.659) | 0.476 (0.175–1.290) | 0.689 (0.232–2.051) | |
| p trend | 0.162 | 0.615 | 0.328 | 0.743 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferreira, E.d.; Hatta, M.; Takeda, Y.; Horikawa, C.; Takeuchi, M.; Kato, N.; Yokoyama, H.; Kurihara, Y.; Iwasaki, K.; Fujihara, K.; et al. Higher Iron Intake Is Independently Associated with Obesity in Younger Japanese Type-2 Diabetes Mellitus Patients. Nutrients 2022, 14, 211. https://doi.org/10.3390/nu14010211
Ferreira Ed, Hatta M, Takeda Y, Horikawa C, Takeuchi M, Kato N, Yokoyama H, Kurihara Y, Iwasaki K, Fujihara K, et al. Higher Iron Intake Is Independently Associated with Obesity in Younger Japanese Type-2 Diabetes Mellitus Patients. Nutrients. 2022; 14(1):211. https://doi.org/10.3390/nu14010211
Chicago/Turabian StyleFerreira, Efrem d’Ávila, Mariko Hatta, Yasunaga Takeda, Chika Horikawa, Mizuki Takeuchi, Noriko Kato, Hiroki Yokoyama, Yoshio Kurihara, Koichi Iwasaki, Kazuya Fujihara, and et al. 2022. "Higher Iron Intake Is Independently Associated with Obesity in Younger Japanese Type-2 Diabetes Mellitus Patients" Nutrients 14, no. 1: 211. https://doi.org/10.3390/nu14010211
APA StyleFerreira, E. d., Hatta, M., Takeda, Y., Horikawa, C., Takeuchi, M., Kato, N., Yokoyama, H., Kurihara, Y., Iwasaki, K., Fujihara, K., Maegawa, H., & Sone, H. (2022). Higher Iron Intake Is Independently Associated with Obesity in Younger Japanese Type-2 Diabetes Mellitus Patients. Nutrients, 14(1), 211. https://doi.org/10.3390/nu14010211