
The Health Effects of Chocolate and Cocoa: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Review Objective
2.2. Inclusion and Exclusion Criteria
2.2.1. Type of Study
2.2.2. Type of Participants
2.2.3. Type of Intervention
- Any studies using only isolated cocoa constituents as intervention.
- Any studies on co-intervention in combination with chocolate or cocoa products.
2.2.4. Type of Outcomes
- i.
- Effects on skin
- Photoprotection
- Photoaging
- ii.
- Cardiovascular clinical outcomes
- Risk of myocardial infarction
- Risk of stroke
- Incidence of death due to cardiovascular event
- iii.
- Cardiovascular parameters
- (a)
- Changes in blood pressure
- Systolic blood pressure
- Diastolic blood pressure
- (b)
- Changes in lipid profile
- Total cholesterol level
- HDL level
- LDL level
- Triglyceride level
- (c)
- Blood glucose parameters
- Fasting blood glucose
- (d)
- Anthropometric parameters
- Weight
- BMI
- Other potentially relevant quantifiable outcomes including waist circumference and body fat percentage
- (a)
- Cognitive outcomes in any validated measure
- Overall cognitive functioning
- Specific cognitive subdomain
- Memory
- Reaction time
- Execution
- (b)
- Psychological outcomes in any validated measure
- Mood
- Depression
- Anxiety
- (c)
- Effects on immunity
- (d)
- Anti-cancer effects
- (e)
- Quality of life
- (f)
- Adverse event (e.g., cravings, headache, allergy)
2.3. Search Strategy
2.4. Study Selection
2.5. Data Extraction & Management
2.6. Data Analysis
2.6.1. Risk of Bias Assessment
2.6.2. Treatment Effect for Primary and Secondary Outcomes
2.6.3. Missing Data
2.6.4. Assessment of Heterogeneity
- Characteristics of the participants (e.g., age, gender, occupation).
- Settings of the studies (e.g., community or institution).
- Interventions (type of chocolate substance given, dosage and length of intervention (dosage: weekly or less frequent vs. twice weekly or more frequent)).
- Risk of bias, in particular, risks of selection and attrition bias (as detailed in the assessment of risk of bias in included studies section).
2.7. Reporting Bias
2.8. Data Synthesis
2.9. Subgroup Analysis and Investigation of Heterogeneity
2.10. Sensitivity Analysis
2.11. Rating Certainty-of-Evidence
3. Results
3.1. Description of Studies
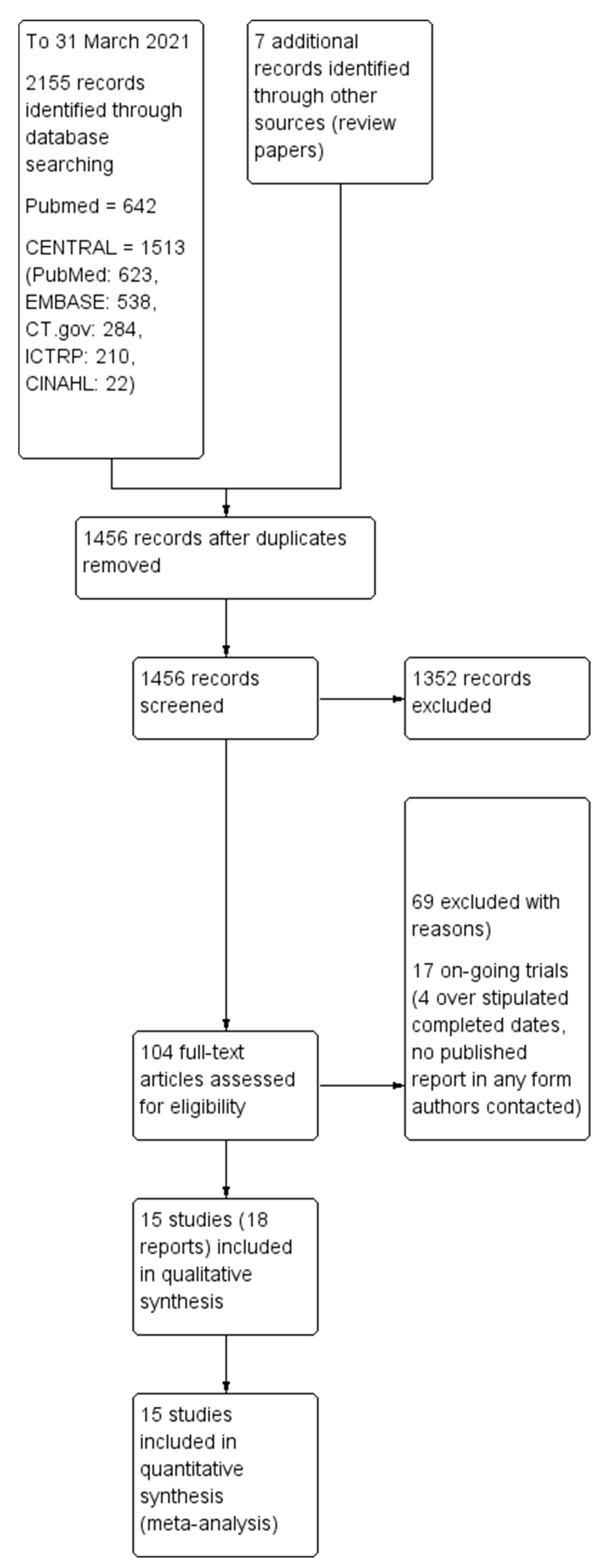
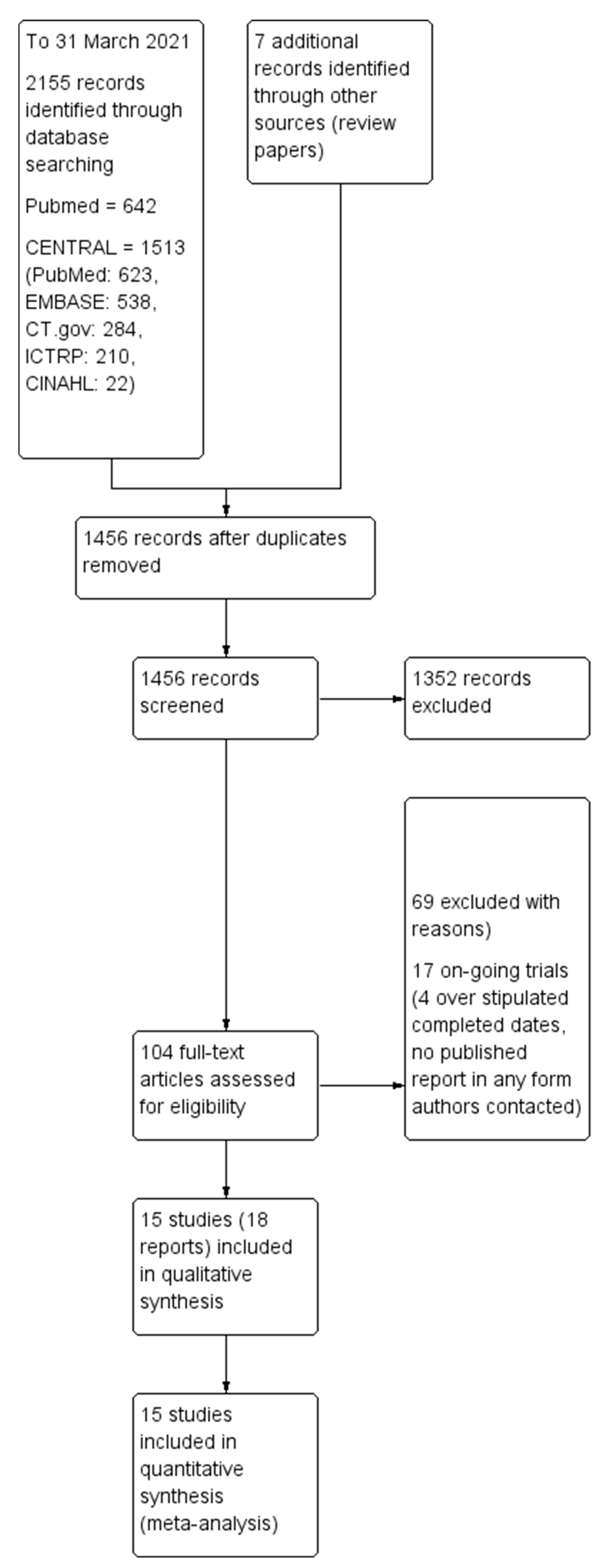
3.1.1. Results of the Search
3.1.2. Included Studies
3.1.3. Outcomes
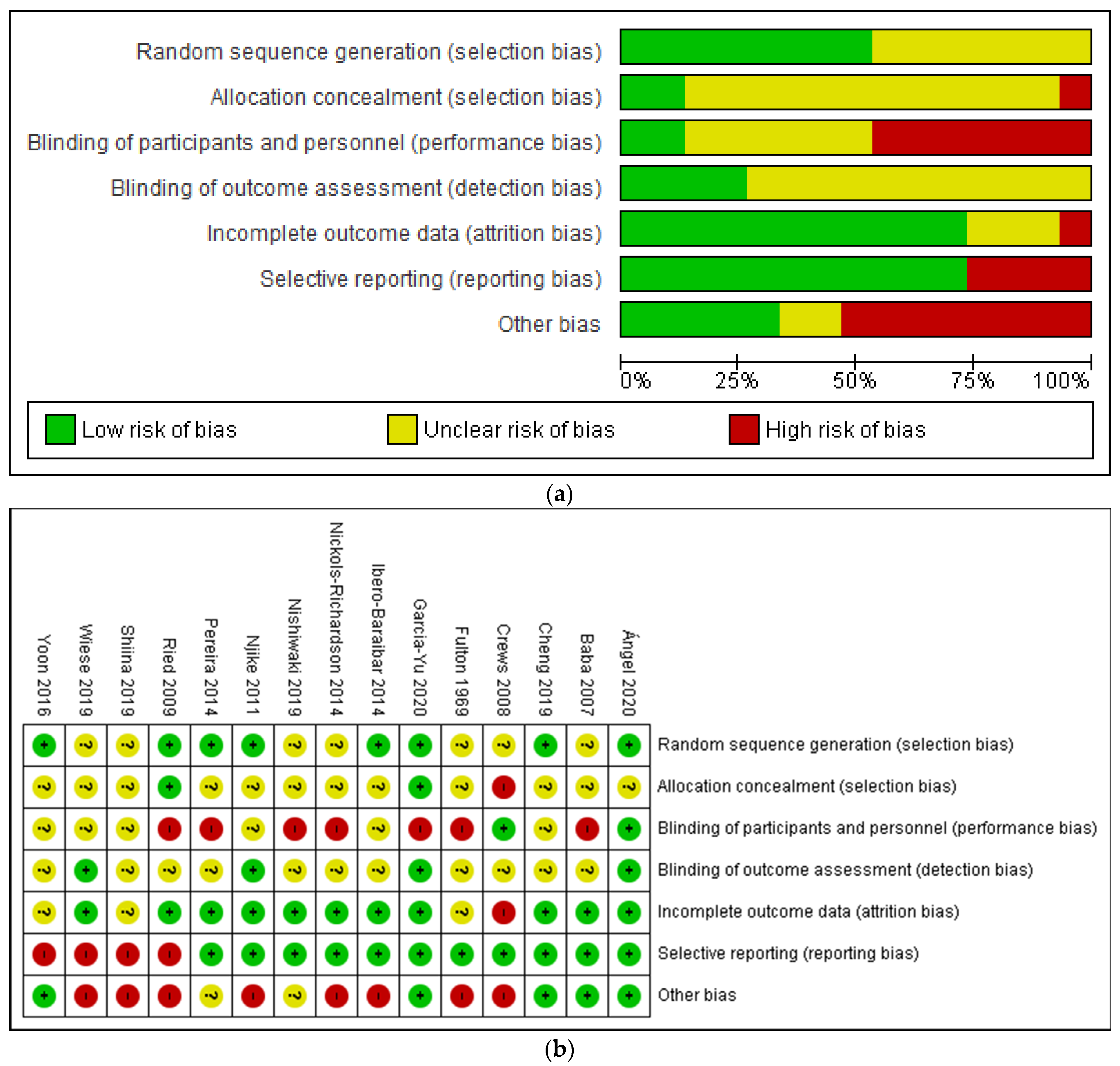
3.2. Risk of Bias Assessment
3.3. Effects of Intervention
3.3.1. Skin Condition
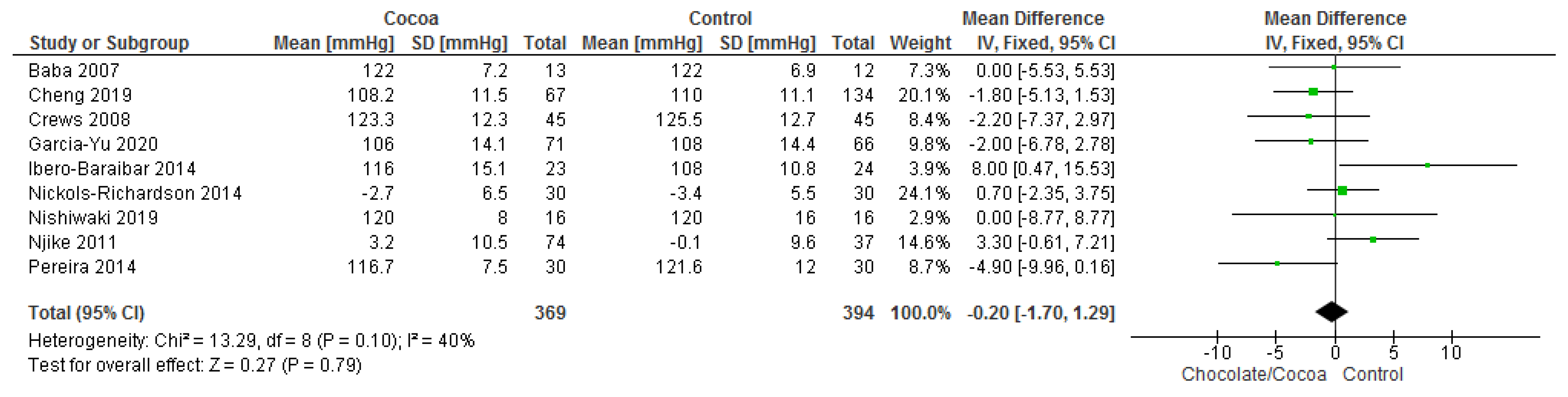
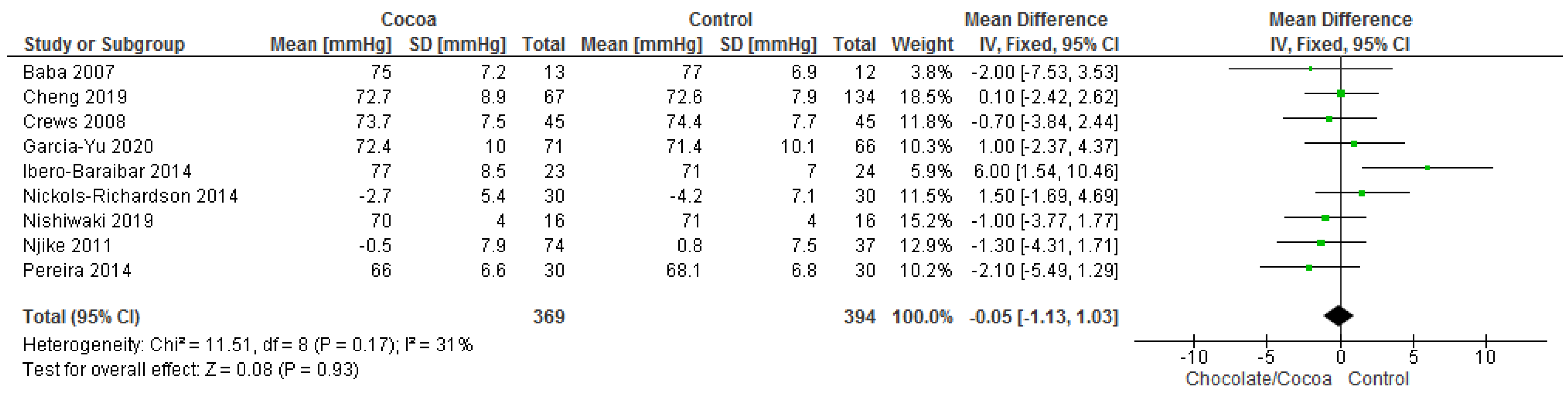
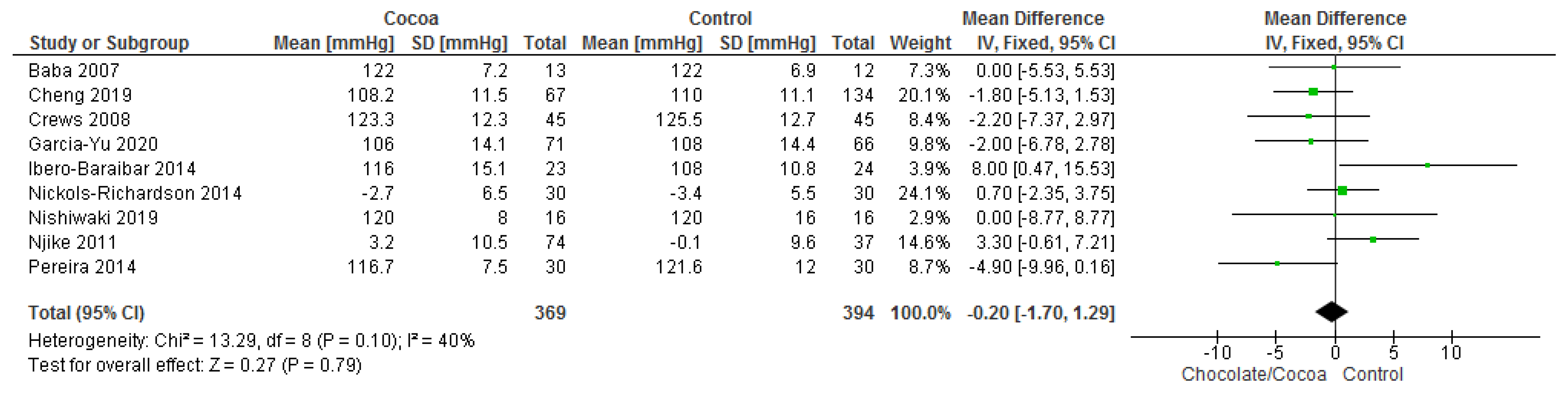
3.3.2. Blood Pressure
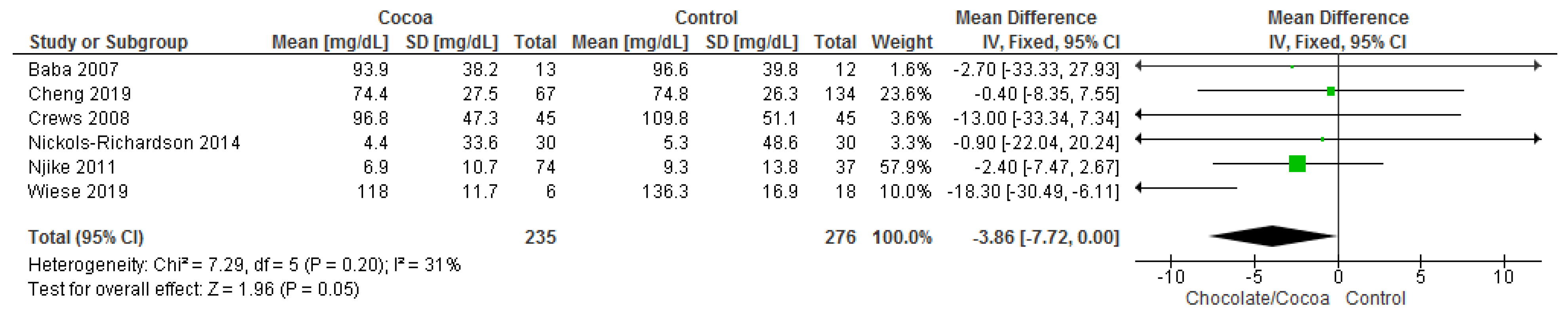
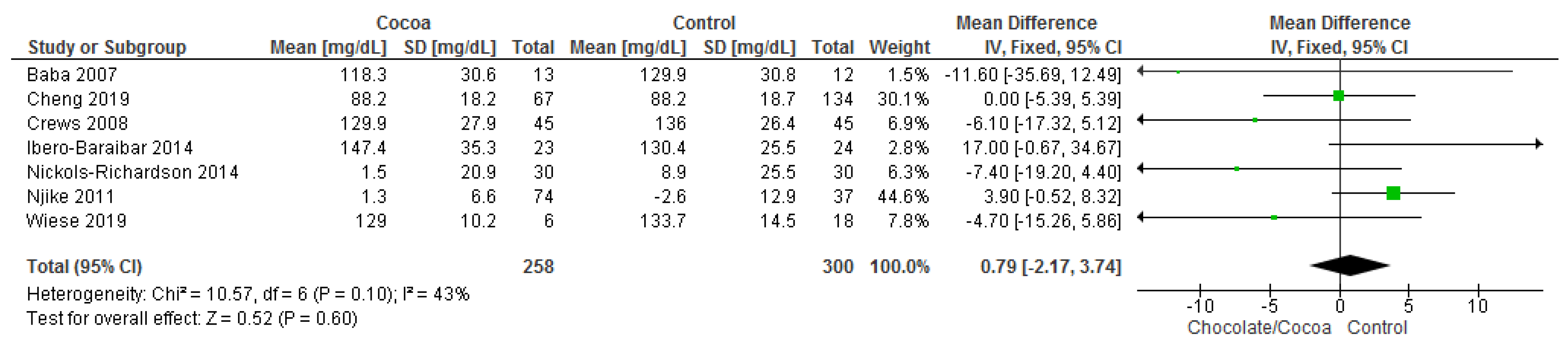
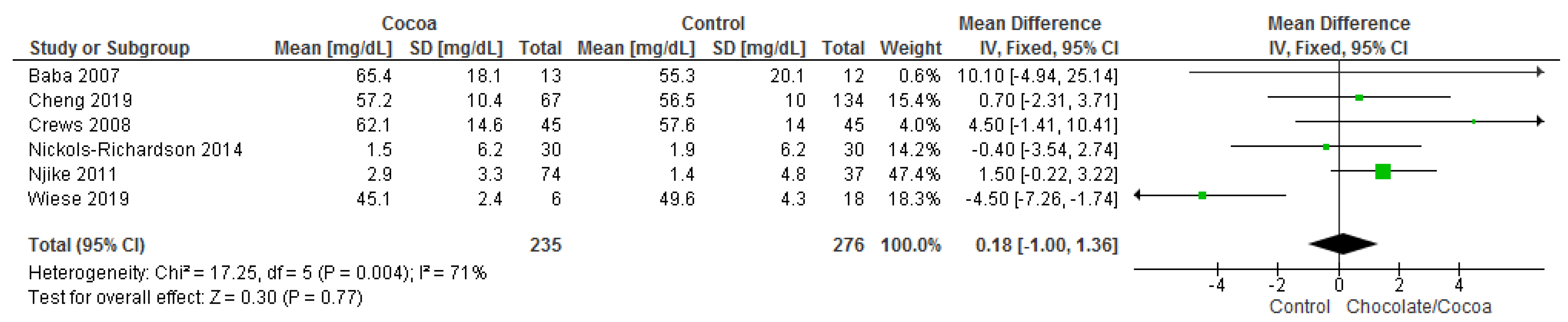
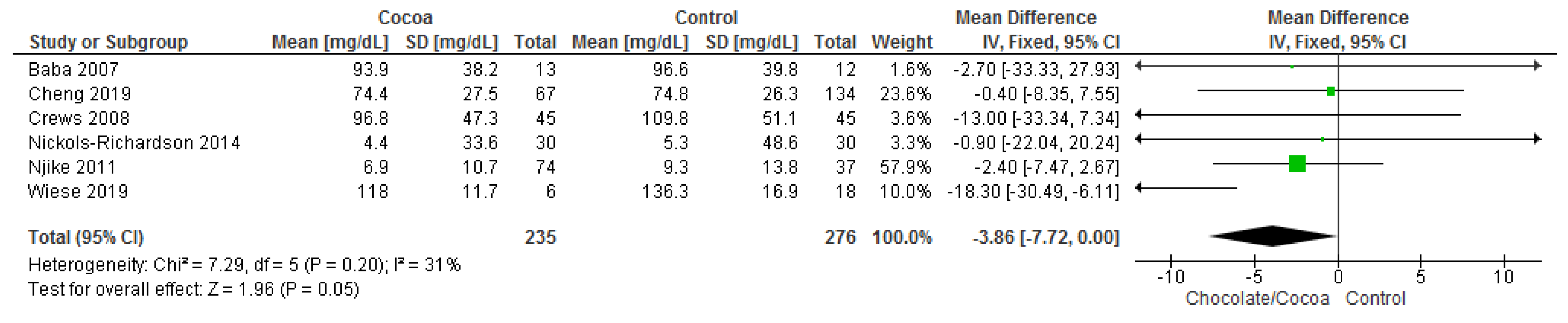
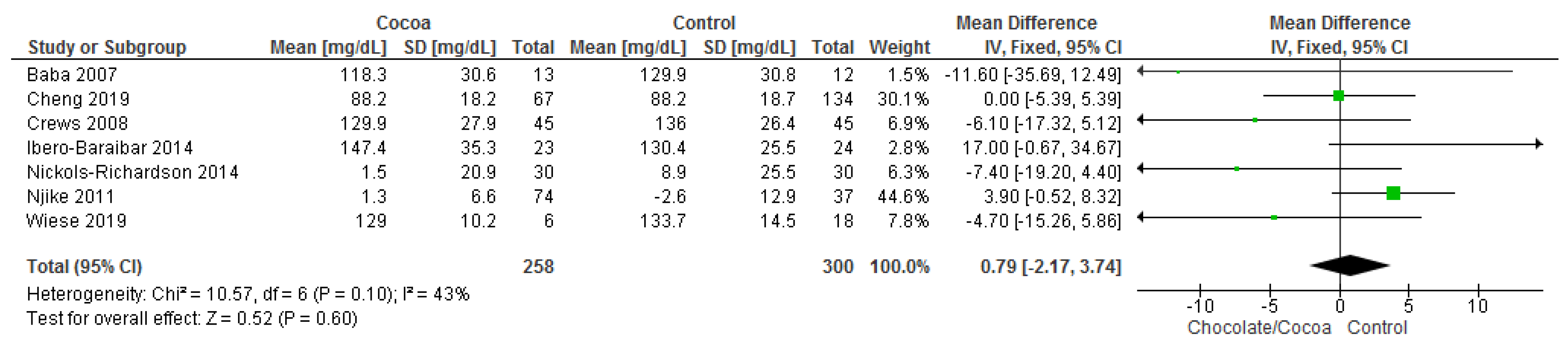
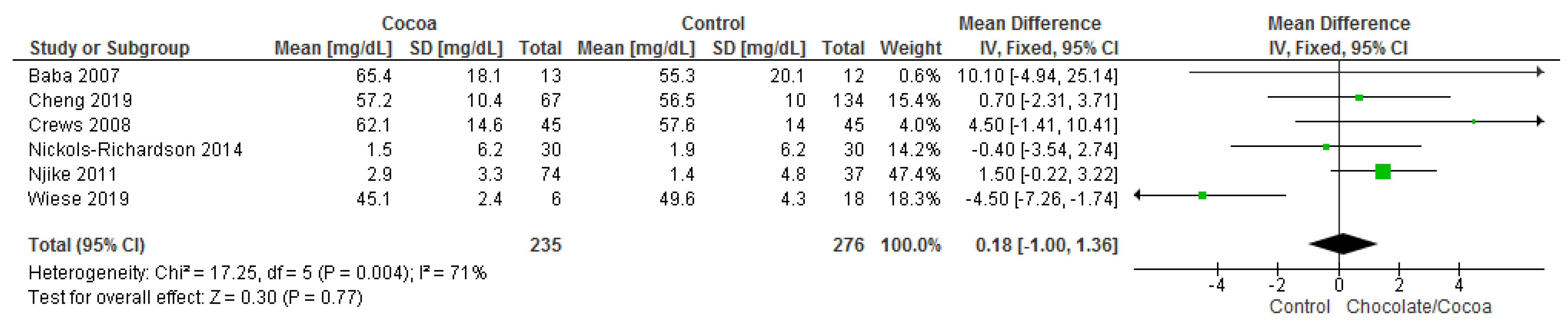
3.3.3. Lipid Profile
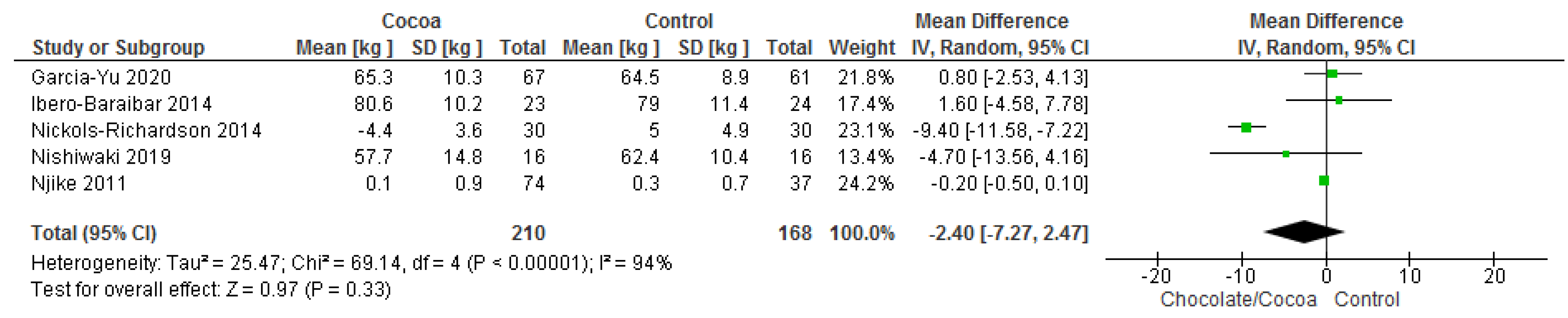
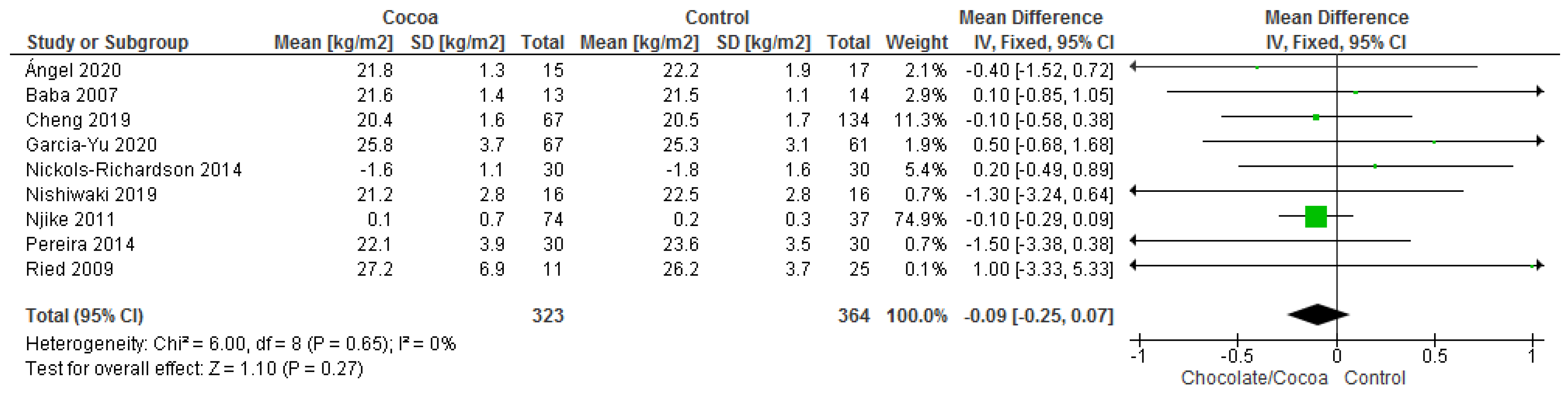
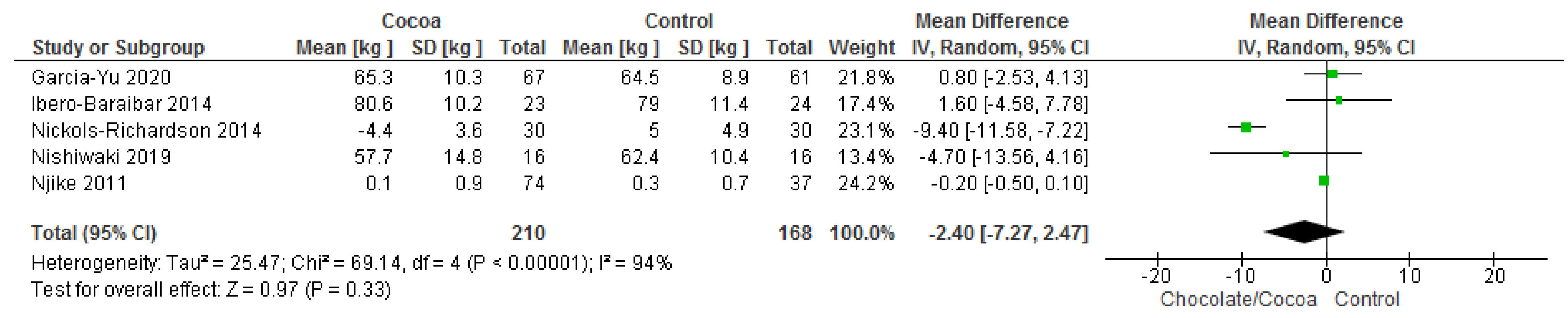
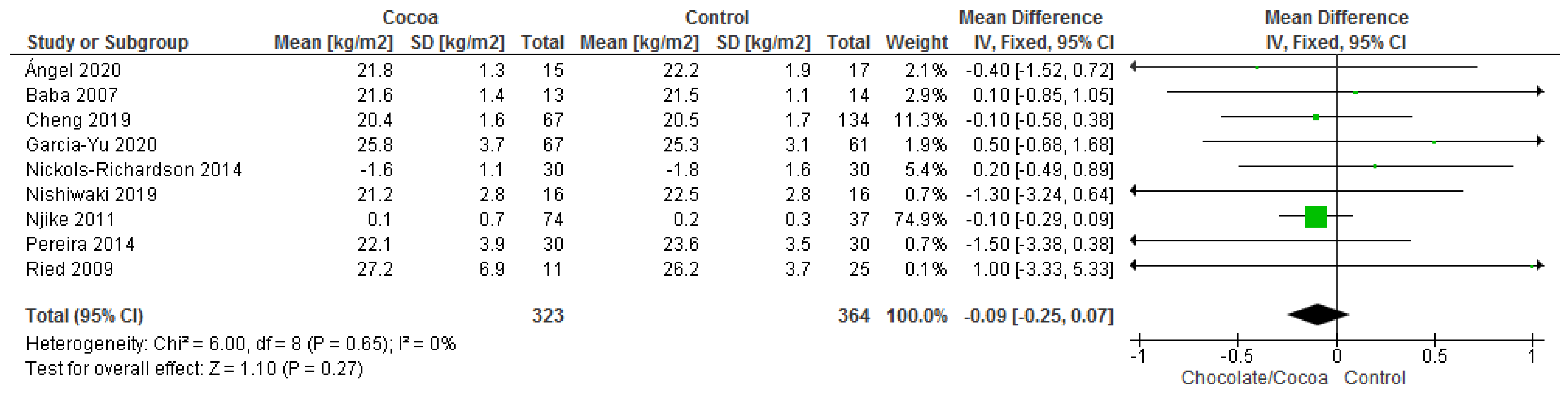
3.3.4. Anthropometric Parameters
3.3.5. Blood Glucose
3.3.6. Cognitive Function
3.3.7. Quality of Life
3.4. Safety Assessment
4. Discussion
4.1. Summary of Main Findings
4.2. Assessment of the Overall Certainty-of-Evidence (GRADE Approach)
4.3. Limitation and Strength of This Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Verna, R. The history and science of chocolate. Malays. J. Pathol. 2013, 35, 111–121. [Google Scholar]
- Di Mattia, C.D.; Sacchetti, G.; Mastrocola, D.; Serafini, M. From Cocoa to Chocolate: The Impact of Processing on In Vitro Antioxidant Activity and the Effects of Chocolate on Antioxidant Markers In Vivo. Front. Immunol. 2017, 8, 1207. [Google Scholar] [CrossRef] [Green Version]
- Żyżelewicz, D.; Budryn, G.; Oracz, J.; Antolak, H.; Kręgiel, D.; Kaczmarska, M. The effect on bioactive components and characteristics of chocolate by functionalization with raw cocoa beans. Food Res. Int. 2018, 113, 234–244. [Google Scholar] [CrossRef]
- Montagna, M.T.; Diella, G.; Triggiano, F.; Caponio, G.R.; Giglio, O.D.; Caggiano, G.; Ciaula, A.D.; Portincasa, P. Chocolate, “Food of the Gods”: History, science, and human health. Int. J. Environ. Res. Public Health 2019, 16, 4960. [Google Scholar] [CrossRef] [Green Version]
- Moramarco, S.N. Nutritional and Health Effects of Chocolate. In The Economics of Chocolate, 1st ed.; Squicciarini, M.P., Swinner, J., Eds.; Oxford University Press: New York, NY, USA, 2016. [Google Scholar]
- Talbot, G. Chocolate and cocoa butter-Structure and composition. In Cocoa Butter and Related Compounds; Academic Press: Cambridge, MA, USA, 2012; pp. 1–33. [Google Scholar]
- Urbanska, B.; Kowalska, J. Comparison of the Total Polyphenol Content and Antioxidant Activity of Chocolate Obtained from Roasted and Unroasted Cocoa Beans from Different Regions of the World. Antioxidants 2019, 8, 283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García, L.C.; Hernández, A.N.M. Beneficial effects of cocoa and dark chocolate polyphenols on health. Faseb J. 2020, 34. [Google Scholar] [CrossRef]
- Larsson, S.C.; Akesson, A.; Gigante, B.; Wolk, A. Chocolate consumption and risk of myocardial infarction: A prospective study and meta-analysis. Heart 2016, 102, 1017–1022. [Google Scholar] [CrossRef]
- Yuan, S.; Li, X.; Jin, Y.; Lu, J. Chocolate consumption and risk of coronary heart disease, stroke, and diabetes: A meta-analysis of prospective studies. Nutrients 2017, 9, 688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiina, Y.; Funabashi, N.; Lee, K.; Murayama, T.; Nakamura, K.; Wakatsuki, Y.; Daimon, M.; Komuro, I. Acute effect of oral flavonoid-rich dark chocolate intake on coronary circulation, as compared with non-flavonoid white chocolate, by transthoracic Doppler echocardiography in healthy adults. Int. J. Cardiol. 2009, 131, 424–429. [Google Scholar] [CrossRef]
- Lamport, D.J.; Christodoulou, E.; Achilleos, C. Beneficial Effects of Dark Chocolate for Episodic Memory in Healthy Young Adults: A Parallel-Groups Acute Intervention with a White Chocolate Control. Nutrients 2020, 12, 483. [Google Scholar] [CrossRef] [Green Version]
- Bisson, J.-F.; Nejdi, A.; Rozan, P.; Hidalgo, S.; Lalonde, R.; Messaoudi, M. Effects of long-term administration of a cocoa polyphenolic extract (Acticoa powder) on cognitive performances in aged rats. Br. J. Nutr. 2008, 100, 94–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rozan, P.; Hidalgo, S.; Nejdi, A.; Bisson, J.-F.; Lalonde, R.; Messaoudi, M. Preventive antioxidant effects of cocoa polyphenolic extract on free radical production and cognitive performances after heat exposure in Wistar rats. J. Food Sci. 2006, 72, S203–S206. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.A.; Goya, L.; de Pascual-Teresa, S. Effect of Cocoa and Cocoa Products on Cognitive Performance in Young Adults. Nutrients 2020, 12, 3691. [Google Scholar] [CrossRef] [PubMed]
- Chalyk, N.; Klochkov, V.; Sommereux, L.; Bandaletova, T.; Kyle, N.; Petyaev, I. Continuous Dark Chocolate Consumption Affects Human Facial Skin Surface by Stimulating Corneocyte Desquamation and Promoting Bacterial Colonization. J. Clin. Aesthet. Dermatol. 2018, 11, 37–41. [Google Scholar]
- Maskarinec, G. Cancer protective properties of cocoa: A review of the epidemiologic evidence. Nutr. Cancer 2009, 61, 573–579. [Google Scholar] [CrossRef]
- Lakshmi, A.; Vishnurekha, C.; Baghkomeh, P.N. Baghkomeh Effect of theobromine in antimicrobial activity: An in vitro study. Dent. Res. J. 2019, 16, 76–80. [Google Scholar] [CrossRef]
- Hirao, C.; Nishimura, E.; Kamei, M.; Ohshima, T.; Maeda, N. Antibacterial effects of cocoa on periodontal pathogenic bacteria. J. Oral Biosci. 2010, 52, 283–291. [Google Scholar] [CrossRef]
- Septianti, E.; Langkong, J. Profile of bioactive compounds, antioxidant and aromatic component from several clones of cocoa beans during fermentation. In IOP Conference Series: Earth and Environmental Science; IOP Publishing: Bristol, UK, 2020; Volume 575, p. 012009. [Google Scholar]
- Ministry of Foreign Affairs, The Netherlands. What is the Demand for Cocoa on the European Market? Center for the Promotion of Imports. Available online: https://www.cbi.eu/market-information/cocoa/trade-statistics (accessed on 23 May 2021).
- Ackar, D.; Lendić, K.V.; Valek, M.; Šubarić, D.; Miličević, B.; Babić, J.; Nedić, I. Cocoa polyphenols: Can we consider cocoa and chocolate as potential functional food? J. Chem. 2013. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Sterne, J.A.C. Chapter 8—Assessing Risk of Bias in Included Studies. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 2011. Available online: https://handbook-5-1.cochrane.org/chapter_8/8_assessing_risk_of_bias_in_included_studies.htm (accessed on 14 June 2021).
- Higgins, J.P.S.; Page, M.J.; Elbers, R.G.; Sterne, J.A. Chapter 8: Assessing Risk of Bias in a Randomised Trial. Cochrane Handbook for Systematic Reviews of Interventions Version 6.0 2019. Available online: https://training.cochrane.org/handbook/current/chapter-08 (accessed on 14 June 2021).
- Higgins, J.P.A.; Sterne, J.A. Chapter 11: Presenting Results and “Summary of Findings” Table. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 2011. Available online: https://handbook-5-1.cochrane.org/chapter_11/11_presenting_results_and_summary_of_findings_tables.htm (accessed on 14 June 2021).
- Review Manager 5 (RevMan 5) [Computer Program]; Version 5.4; Nordic Cochrane Centre: Copenhagen, Denmark, 2014.
- Schünemann, H.J.; Oxman, A.D.; Vist, G.E.; Higgins, J.P.T.; Deeks, J.J.; Glasziou, P.; Guyatt, G.H. Chapter 12: Interpreting Results and Drawing Conclusions. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 2011. Available online: https://handbook-5-1.cochrane.org/chapter_12/12_interpreting_results_and_drawing_conclusions.htm (accessed on 14 June 2021).
- GRADEpro GDT; Developed by Evidence Prime; McMaster University: Hamilton, ON, Canada, 2015.
- Garcia-Yu, I.A.; Garcia-Ortiz, L.; Gomez-Marcos, M.A.; Rodriguez-Sanchez, E.; Agudo-Conde, C.; Gonzalez-Sanchez, J.; Maderuelo-Fernandez, J.A.; Recio-Rodriguez, J.I. Effects of Cocoa-Rich Chocolate on Blood Pressure, Cardiovascular Risk Factors, and Arterial Stiffness in Postmenopausal Women: A Randomized Clinical Trial. Nutrients 2020, 12, 1758. [Google Scholar] [CrossRef]
- Wiese, M.; Bashmakov, Y.; Chalyk, N.; Nielsen, D.S.; Krych, Ł.; Kot, W.; Klochkov, V.; Pristensky, D.; Bandaletova, T.; Chernyshova, M. Prebiotic Effect of Lycopene and Dark Chocolate on Gut Microbiome with Systemic Changes in Liver Metabolism, Skeletal Muscles and Skin in Moderately Obese Persons. Biomed. Res. Int. 2019, 2019, 4625279. [Google Scholar] [CrossRef]
- Ried, K.; Frank, O.R.; Stocks, N.P. Dark chocolate or tomato extract for prehypertension: A randomised controlled trial. BMC Complement. Altern. Med. 2009, 9, 22. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.; Wang, D.; Xia, H.; Wang, F.; Yang, X.; Pan, D.; Wang, S.; Yang, L.; Lu, H.; Shu, G.; et al. A comparative study of the effects of palm olein, cocoa butter and extra virgin olive oil on lipid profile, including low-density lipoprotein subfractions in young healthy Chinese people. Int. J. Food Sci. Nutr. 2019, 70, 355–366. [Google Scholar] [CrossRef]
- Fulton, J.E., Jr.; Plewig, G.; Kligman, A.M. Effect of chocolate on acne vulgaris. JAMA 1969, 210, 2071–2074. [Google Scholar] [CrossRef]
- Njike, V.Y.; Faridi, Z.; Shuval, K.; Dutta, S.; Kay, C.D.; West, S.G.; Kris-Etherton, P.M.; Katz, D.L. Effects of sugar-sweetened and sugar-free cocoa on endothelial function in overweight adults. Int. J. Cardiol. 2011, 149, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Shiina, K.; Tomiyama, H.; Matsumoto, C.; Komatsu, S.; Natsume, M.; Oba, C.; Ohshiba, Y.; Yamaji, T.; Chikamori, T.; Yamashina, A. Gender difference in the effects of cacao polyphenols on blood pressure and glucose/lipid metabolism in prediabetic subjects: A double-blinded, randomized, placebo-controlled crossover trial. Hypertens. Res. 2019, 42, 1083–1085. [Google Scholar] [CrossRef] [PubMed]
- Nickols-Richardson, S.M.; Piehowski, K.E.; Metzgar, C.J.; Miller, D.L.; Preston, A.G. Changes in body weight, blood pressure and selected metabolic biomarkers with an energy-restricted diet including twice daily sweet snacks and once daily sugar-free beverage. Nutr. Res. Pract. 2014, 8, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Crews, W.D., Jr.; Harrison, D.W.; Wright, J.W. A double-blind, placebo-controlled, randomized trial of the effects of dark chocolate and cocoa on variables associated with neuropsychological functioning and cardiovascular health: Clinical findings from a sample of healthy, cognitively intact older adults. Am. J. Clin. Nutr. 2008, 87, 872–880. [Google Scholar] [PubMed] [Green Version]
- Nishiwaki, M.; Nakano, Y.; Matsumoto, N. Effects of regular high-cocoa chocolate intake on arterial stiffness and metabolic characteristics during exercise. Nutrition 2019, 60, 53–58. [Google Scholar] [CrossRef]
- Baba, S.; Osakabe, N.; Kato, Y.; Natsume, M.; Yasuda, A.; Kido, T.; Fukuda, K.; Muto, Y.; Kondo, K. Continuous intake of polyphenolic compounds containing cocoa powder reduces LDL oxidative susceptibility and has beneficial effects on plasma HDL-cholesterol concentrations in humans. Am. J. Clin. Nutr. 2007, 85, 709–717. [Google Scholar] [CrossRef] [Green Version]
- Angel Garcia-Merino, J.; Moreno-Perezde, D.; Lucas, B.; Montalvo-Lominchar, M.G.; Munoz, E.; Sanchez, L.; Naclerio, F.; Herrera-Rocha, K.M.; Moreno-Jimenez, M.R.; Rocha-Guzman, N.E.; et al. Chronic flavanol-rich cocoa powder supplementation reduces body fat mass in endurance athletes by modifying the follistatin/myostatin ratio and leptin levels. Food Funct. 2020, 11, 3441–3450. [Google Scholar] [CrossRef]
- Ibero-Baraibar, I.; Abete, I.; Navas-Carretero, S.; Massis-Zaid, A.; Martinez, J.A.; Zulet, M.A. Oxidised LDL levels decreases after the consumption of ready-to-eat meals supplemented with cocoa extract within a hypocaloric diet. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 416–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, H.S.; Kim, J.R.; Park, G.Y.; Kim, J.E.; Lee, D.H.; Lee, K.W.; Chung, J.H. Cocoa Flavanol Supplementation Influences Skin Conditions of Photo-Aged Women: A 24-Week Double-Blind, Randomized, Controlled Trial. J. Nutr. 2016, 146, 46–50. [Google Scholar]
- Pereira, T.; Maldonado, J.; Laranjeiro, M.; Coutinho, R.; Cardoso, E.; Andrade, I.; Conde, J. Central arterial hemodynamic effects of dark chocolate ingestion in young healthy people: A randomized and controlled trial. Cardiol. Res. Pract. 2014, 2014, 945951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, E.L.; Hutfless, S.M.; Ding, X.; Girotra, S. Chocolate and prevention of cardiovascular disease: A systematic review. Nutr. Metab. 2006, 3, 2. [Google Scholar] [CrossRef] [Green Version]
- Gianfredi, V.; Salvatori, T.; Nucci, D.; Villarini, M.; Moretti, M. Can. chocolate consumption reduce cardio-cerebrovascular risk? A systematic review and meta-analysis. Nutrition 2018, 46, 103–114. [Google Scholar] [CrossRef]
- Hooper, L.; Kay, C.; Abdelhamid, A.; Kroon, P.A.; Cohn, J.S.; Rimm, E.B.; Cassidy, A. Effects of chocolate, cocoa, and flavan-3-ols on cardiovascular health: A systematic review and meta-analysis of randomized trials. Am. J. Clin. Nutr. 2012, 95, 740–751. [Google Scholar] [CrossRef] [PubMed]
- Khawaja, O.; Gaziano, J.M.; Djousse, L. Chocolate and coronary heart disease: A systematic review. Curr. Atheroscler. Rep. 2011, 13, 447–452. [Google Scholar] [CrossRef]
- Krittanawong, C.; Narasimhan, B.; Wang, Z.; Hahn, J.; Virk, H.U.H.; Farrell, A.M.; Zhang, H.J.; Tang, W.W. Association between chocolate consumption and risk of coronary artery disease: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2020. [Google Scholar] [CrossRef]
- Buitrago, A.; Sanderson, J.; Johnson, L.; Warnakula, S.; Wood, A.; Angelantonio, E.; Franco, O. Chocolate consumption and cardiometabolic disorders: Systematic review and meta-analysis. BMJ 2011, 343, d4488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, L.; Caris-Veyrat, C.; Lowe, G.; Böhm, V. Lycopene and Its Antioxidant Role in the Prevention of Cardiovascular Diseases-A Critical Review. Crit. Rev. Food Sci. Nutr. 2016, 56, 1868–1879. [Google Scholar] [CrossRef] [PubMed]
- Story, E.N.; Kopec, R.E.; Schwartz, S.J.; Harris, G.K. An update on the health effects of tomato lycopene. Annu. Rev. Food Sci. Technol. 2010, 1, 189–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senkus, K.E.; Tan, L.; Crowe-White, K.M. Lycopene and Metabolic Syndrome: A Systematic Review of the Literature. Adv. Nutr. 2019, 10, 19–29. [Google Scholar] [CrossRef] [Green Version]
- Kord-Varkaneh, H.; Ghaedi, E.; Nazary-Vanani, A.; Mohammadi, H.; Shab-Bidar, S. Does cocoa/dark chocolate supplementation have favorable effect on body weight, body mass index and waist circumference? A systematic review, meta-analysis and dose-response of randomized clinical trials. Crit. Rev. Food Sci. Nutr. 2019, 59, 2349–2362. [Google Scholar] [CrossRef]
- Scholey, A.; Owen, L. Effects of chocolate on cognitive function and mood: A systematic review. Nutr. Rev. 2013, 71, 665–681. [Google Scholar] [CrossRef]
- Gratton, G.; Weaver, S.R.; Burley, C.V.; Low, K.A.; Maclin, E.L.; Johns, P.W.; Pham, Q.S.; Lucas, S.J.E.; Fabiani, M.; Rendeiro, C. Dietary flavanols improve cerebral cortical oxygenation and cognition in healthy adults. Sci. Rep. 2020, 10, 19409. [Google Scholar] [CrossRef] [PubMed]
- Mogollon, J.A.; Boivin, C.; Lemieux, S.; Blanchet, C.; Claveau, J.; Dodin, S. Chocolate flavanols and skin photoprotection: A parallel, double-blind, randomized clinical trial. Nutr. J. 2014, 13, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vongraviopap, S.; Asawanonda, P. Dark chocolate exacerbates acne. Int. J. Dermatol. 2016, 55, 587–591. [Google Scholar] [CrossRef] [PubMed]
- Grassi, D.; Desideri, G.; Necozione, S.; di Giosia, P.; Barnabei, R.; Allegaert, L.; Bernaert, H.; Ferri, C. Cocoa consumption dose-dependently improves flow-mediated dilation and arterial stiffness decreasing blood pressure in healthy individuals. J. Hypertens. 2015, 33, 294–303. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Country, Year | Clinical Trial Design | Population | Sex | Sample Size Chocolate/Placebo | Duration/Outcome | Intervention Group | |
|---|---|---|---|---|---|---|---|
| Intervention Group | Placebo Group | ||||||
| Ángel García-Merino, Spain, 2020 | Randomised, parallel-group placebo-controlled trial | Male endurance cross-country athletes | Male | 15/17 | 10 weeks | 5 g of fat-reduced cocoa containing 425 mg of flavanols | 5 g of maltodextrin |
| Fulton, USA, 1969 | Crossover, single-blind | Subjects with mild to moderate acne | Both | 65 | 2 months | 114 g of bittersweet chocolate bar | 112 g of 28% vegetable fat to mimic the lipids contained in chocolate liquor and cocoa butter bar |
| Cheng, China, 2018 | Randomised crossover 33 Latin-square design | Male or female aged 20–40 years | Both | 67 | 4 weeks | Cocoa butter | (1) Palm olein (2) extra virgin olive oil |
| Garcia-Yu, Spain, 2020 | Controlled randomised trial with two parallel groups | Women aged between 50 and 64 years and in the period of post-menopause | Female | 69/63 | 6 months | Chocolate (99% cocoa) 10 g as supplement | No intervention |
| Nishiwaki, Japan, 2019 | Randomised, controlled, parallel-group intervention study | Healthy Japanese college student | Both | 16/16 | 4 weeks | 20 g/day (508 mg of cacao polyphenol) of high-cocoa chocolate | No intervention |
| Wiese, Russia, 2019 | Randomised, parallel-five group placebo-controlled trial | Moderately obese volunteers | Both | 6 people per group | 4 weeks | 10 g of dark chocolate | (1) 7 mg GA lycopene (GAL) formulated with medium saturated fatty acids (GAL-MUFA) (2) 30 mg GAL-MUFA (3) 30 mg GAL-PUFA |
| Yoon, Korea, 2015 | Randomised, parallel-group placebo-controlled trial | Healthy female volunteers | Female | 31/31 | 24 weeks | Beverage containing 4 g cocoa powder to yield 320 mg total cocoa flavanols | Nutrient-matched cocoa-flavored beverage without cocoa flavanols |
| Shiina, Japan, 2019 | Randomised, placebo-controlled doubleblind crossover trial | Pre-diabetic volunteers | Both | 11/11 | 4 weeks | Cacao procyanidin supplement (83.3 ± 2.7 mg/day) which contain 13.9 ± 2.7 mg procyanidins | 240 mg dextrin |
| Baba, Japan, 2007 | Randomised controlled trial | Healthy Japanese male subjects | Male | 25 | 12 weeks | Cocoa powder and sugar | Sugar |
| Ibero-Baraibar, Spain, 2014 | Randomised, parallel and double-blind study | Healthy Caucasian adult | Both | 50 | 4 weeks | Cocoa extract | Placebo |
| Nickols-Richardson, USA, 2014 | Randomised controlled trial | Overweight otherwise healthy women age 25–45 years (premenopausal) | Female | 60 | 18 weeks | Cocoa beverage with dark chocolate | Cocoa free beverage with non- chocolate snacks |
| Njike, USA, 2011 | Randomised, controlled, crossover trial | Overweight, but otherwise healthy, men and women | Both | 44 | 6 weeks | Unsweetened or sweetened cocoa beverage | Non-cocoa beverage |
| Prereira, Portugal, 2014 | Randomised controlled trial | Clinically healthy individuals of Portuguese nationality, all undergraduate students at the Superior Polytechnic Institute of Coimbra, under the age of 25 years | Both | 60 | 4 weeks | Dark chocolate | Placebo |
| Ried, Australia, 2009 | Randomised controlled trial (2 phases) | Prehypertensive otherwise healthy adults | Both | 36 | 8 weeks | Dark chocolate bar | (1) Placebo (2) Tomato extract |
| Crews, USA, 2008 | Double-blind, placebo-controlled, randomised trial | Healthy older male and female adults 60 years and above | Both | 101 | 6 weeks | Dark chocolate bar | Placebo |
| Author, Year | Findings |
|---|---|
| Angel García-Merino, 2020 | Not reported |
| Fulton, 1969 | Not specifically reported; but caused gastrointestinal disturbances in one case leading to defaulting intervention |
| Cheng, 2018 | Not reported |
| Garcia-Yu 2020 | Not specifically reported; but did not change body composition |
| Nishiwaki, 2019 | Slight increase in resting glucose levels (especially in the intervention group with normal diets +20 g/day of high-cocoa chocolate) |
| Wiese, 2019 | Not specifically reported; but did not cause significant changes in glucose and liver enzymes AST and ALT |
| Yoon, 2015 | Well tolerated, no subjective adverse events reported. No significant changes in serum biochemistry and haematologic indices (AST, ALT, glucose, blood urea nitrogen, creatinine, hemoglobin, hematocrits) |
| Shiina, 2019 | Not reported |
| Baba, 2007 | All biochemical and urinalysis within normal range at baseline and at 12 weeks (including plasma total protein, albumin, glucose, uric acid, urea nitrogen, creatinine, free fatty acids, phospholipids, total bilirubin, AST, ALT, GGT, alkaline phosphatase, lactate dehydrogenase, sodium, potassium, chloride, proteinuria, glucosuria, urobilinogen, and occult blood). |
| Ibero-Baraibar, 2014 | Not reported |
| Nickols-Richardson, 2014 | Not reported |
| Njike, 2011 | Cocoa products (sweetened and unsweetened) does not adversely affect body weight during short term consumption |
| Prereira, 2014 | Not reported |
| Ried, 2009 | Dark chocolate: unpalatable (n = 2)-withdrew;Tomato extract: gastrointestinal upset (n = 1)-withdrew |
| Crews, 2008 | 13 adverse events reported in treatment group compared to 10 in control group. Most are mild to moderate including gastrointestinal disturbances and cold symptoms. One severe adverse event atrial arrythmia (type unknown) was reported in the treatment group and was hospitalised. This event was thought to be not related to the treatment |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, T.Y.C.; Lim, X.Y.; Yeo, J.H.H.; Lee, S.W.H.; Lai, N.M. The Health Effects of Chocolate and Cocoa: A Systematic Review. Nutrients 2021, 13, 2909. https://doi.org/10.3390/nu13092909
Tan TYC, Lim XY, Yeo JHH, Lee SWH, Lai NM. The Health Effects of Chocolate and Cocoa: A Systematic Review. Nutrients. 2021; 13(9):2909. https://doi.org/10.3390/nu13092909
Chicago/Turabian StyleTan, Terence Yew Chin, Xin Yi Lim, Julie Hsiao Hui Yeo, Shaun Wen Huey Lee, and Nai Ming Lai. 2021. "The Health Effects of Chocolate and Cocoa: A Systematic Review" Nutrients 13, no. 9: 2909. https://doi.org/10.3390/nu13092909
APA StyleTan, T. Y. C., Lim, X. Y., Yeo, J. H. H., Lee, S. W. H., & Lai, N. M. (2021). The Health Effects of Chocolate and Cocoa: A Systematic Review. Nutrients, 13(9), 2909. https://doi.org/10.3390/nu13092909