Towards an In-Depth Understanding of Physical Activity and Eating Behaviours during COVID-19 Social Confinement: A Combined Approach from a Portuguese National Survey

 ,
,  ,
,  , ,
, ,  ,
, 
Abstract
:1. Introduction
1.1. Social Confinement and Eating Behaviours
1.2. Social Confinement and Physical Activity
1.3. The Need for Adequate, Local, and Integrated Monitoring—A Step for Effective Public Health Policies
2. Methods
2.1. Study Design and Participants
2.2. The Survey
2.2.1. Eating Behaviours
2.2.2. Physical Activity and Sedentary Behaviour
2.3. Statistical Analyses
3. Results
3.1. Participants’ Characteristics
3.2. Physical Activity and Sedentary Behaviour
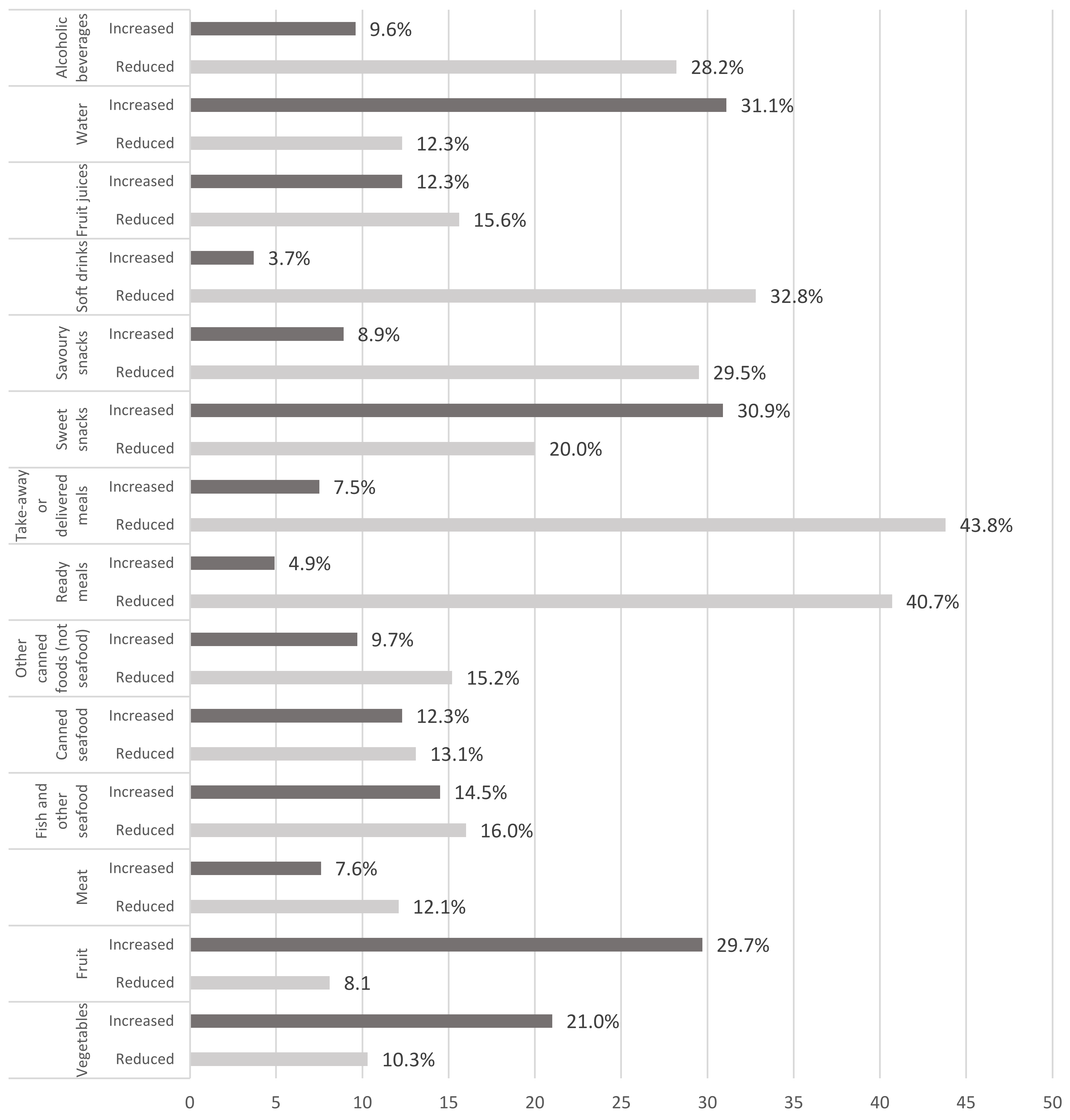
3.3. Eating Habits
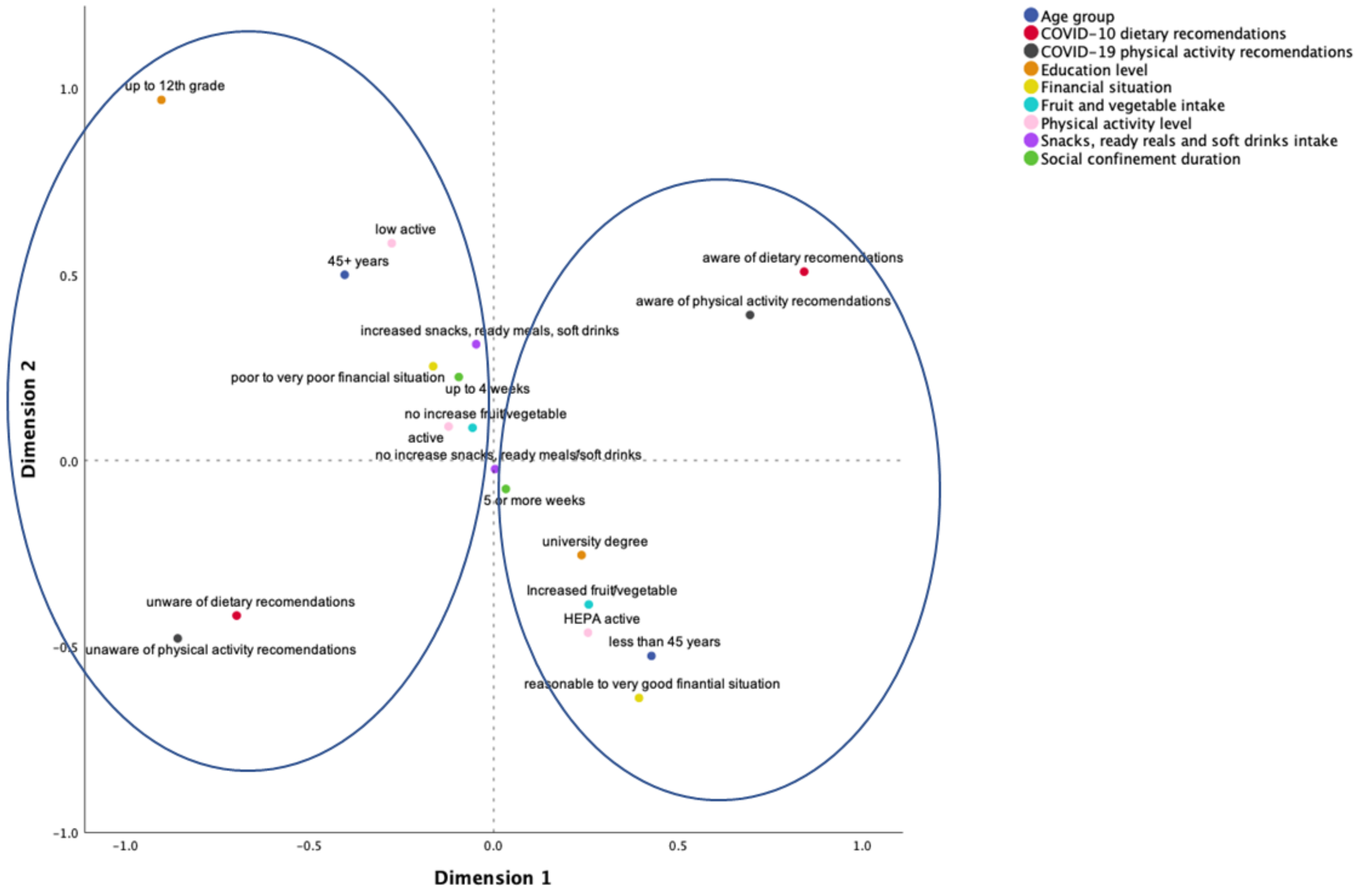
3.4. Combined Approach: Health and Risk Patterns
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kluge, H.H.P.; Wickramasinghe, K.; Rippin, H.L.; Mendes, R.; Peters, D.H.; Kontsevaya, A.; Breda, J. Prevention and control of non-communicable diseases in the COVID-19 response. Lancet 2020, 395, 1678–1680. [Google Scholar] [CrossRef]
- Bas, D.; Martin, M.; Pollack, C.; Venne, R. The Impact of COVID-19 on Sport, Physical Activity and Well-Being and Its Effects on Social Development-Policy Brief No. 73; United Nations Department of Economic and Social Affairs: New York, NY, USA, 2020. [Google Scholar]
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. World Health Organization. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 3 August 2020).
- World Health Organization. COVID-19 Strategy Update-14 April 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Ainsworth, B.A.; Li, F. Physical activity during the coronavirus disease-19 global pandemic. J. Sport Health Sci. 2020, 9, 291–292. [Google Scholar] [CrossRef]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 home confinement on eating behaviour and physical activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Woods, J.A.; Hutchinson, N.T.; Powers, S.K.; Roberts, W.O.; CarmenGomez-Cabrera, M.; Radak, Z.; Berkes, I.; Boros, A.; Boldogh, I.; Leeuwenburg, C.; et al. The COVID-19 pandemic and physical activity. Sports Med. Health Sci. 2020, 2, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Mao, L.; Nassis, G.P.; Harmer, P.; Ainsworth, B.E.; Li, F. Coronavirus disease (COVID-19): The need to maintain regular physical activity while taking precautions. J. Sport Health Sci. 2020, 9, 103–104. [Google Scholar] [CrossRef] [PubMed]
- Hall, G.; Laddu, D.R.; Phillips, S.A.; Lavie, C.J.; Arena, R. A tale of two pandemics: How will COVID-19 and global trends in physical inactivity and sedentary behavior affect one another? Prog. Cardiovasc. Dis. 2021, 64, 108–110. [Google Scholar] [CrossRef]
- Gakidou, E.; Afshin, A.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulle, A.M.; Abera, S.F.; Aboyans, V.; et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar]
- Lippi, L.G.; Henry, B.M.; Sanchis-Gomar, F. Physical inactivity and cardiovascular disease at the time of coronavirus disease 2019 (COVID-19). Eur. J. Prev. Cardiol. 2020, 27, 906–908. [Google Scholar] [CrossRef] [PubMed]
- Jakobsson, J.; Malm, C.; Furberg, M.; Ekelund, U.; Svensson, M. Physical activity during the coronavirus (COVID-19) pandemic: Prevention of a decline in metabolic and immunological functions. Front. Sports Act. Living 2020, 2, 57. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Ferran, M.; de la Guía-Galipienso, F.; Sanchis-Gomar, F.; Pareja-Galeano, H. Metabolic impacts of confinement during the COVID-19 pandemic due to modified diet and physical activity habits. Nutrients 2020, 12, 1549. [Google Scholar] [CrossRef]
- Mattioli, A.V.; Sciomer, S.; Cocchi, C.; Maffei, S.; Gallina, S. Quarantine during COVID-19 outbreak: Changes in diet and physical activity increase the risk of cardiovascular disease. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1409–1417. [Google Scholar] [CrossRef]
- Banerjee, S.; Burkholder, G.; Sana, B.; Szirony, G.M. Social Isolation as a predictor for mortality: Implications for COVID-19 prog-nosis. MedRxiv 2020. (preprint). [Google Scholar]
- Elovainio, M.; Hakulinen, C.; Pulkki-Råback, L.; Virtanen, M.; Josefsson, K.; Jokela, M.; Vahtera, J.; Kivimäki, M. Contribution of risk factors to excess mortality in isolated and lonely individuals: An analysis of data from the UK Biobank cohort study. Lancet Public Health 2017, 2, e260–e266. [Google Scholar] [CrossRef] [Green Version]
- Sahle, B.W.; Chen, W.; Melaku, Y.A.; Akombi, B.J.; Rawal, L.B.; Renzaho, A.M.N. Association of psychosocial factors with risk of chronic diseases: A nationwide longitudinal study. Am. J. Prev. Med. 2020, 58, e39–e50. [Google Scholar] [CrossRef] [PubMed]
- Peçanha, T.; Goessler, K.F.; Roschel, H.; Gualano, B. Social isolation during the COVID-19 pandemic can increase physical inactivity and the global burden of cardiovascular disease. Am. J. Physiol. Heart Circ. Physiol. 2020, 318, H1441–H1446. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, N.R. A review of social isolation: An important but underassessed condition in older adults. J. Prim. Prev. 2012, 33, 137–152. [Google Scholar] [CrossRef] [PubMed]
- Arora, T.; Grey, I. Health behaviour changes during COVID-19 and the potential consequences: A mini-review. J. Health Psychol. 2020, 25, 1155–1163. [Google Scholar] [CrossRef]
- Betsch, C.; Wieler, L.H.; Habersaat, K. Monitoring behavioural insights related to COVID-19. Lancet 2020, 395, 1255–1256. [Google Scholar] [CrossRef]
- Balanzá-Martínez, V.; Atienza-Carbonell, B.; Kapczinski, F.; de Boni, R.B. Lifestyle behaviours during the COVID-19-time to connect. Acta Psychiatr. Scand. 2020, 141, 399–400. [Google Scholar] [CrossRef]
- British Dietetic Association. Eating Well during Coronavirus/COVID-19. British Dietetic Association. Available online: https://www.bda.uk.com/resource/eating-well-during-coronavirus-covid-19.html (accessed on 3 August 2020).
- World Health Organization. Food and Nutrition during Self-Quarantine: What to Choose and How to Eat Healthily. Geneva, Switzerland: World Health Organization. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/news/news/2020/3/food-and-nutrition-during-self-quarantine-what-to-choose-and-how-to-eat-healthily (accessed on 3 August 2020).
- World Health Organization Regional Office for Europe. Food and Nutrition Tips during Self-Quarantine. World Health Organization. Available online: http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/novel-coronavirus-2019-ncov-technical-guidance/food-and-nutrition-tips-during-self-quarantine (accessed on 4 August 2020).
- Barazzoni, R.; Bischoff, S.C.; Breda, J.; Wickramasinghe, K.; Krznaric, Z.; Nitzan, D.; Pirlich, M.; Singer, P. ESPEN expert statements and practical guidance for nutritional management of individuals with SARS-CoV-2 infection. Clin. Nutr. 2020, 39, 1631–1638. [Google Scholar] [CrossRef]
- Hill, J.O.; Wyatt, H.R.; Peters, J.C. Energy balance and obesity. Circulation 2012, 126, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Siordia, J.A. Epidemiology and clinical features of COVID-19: A review of current literature. J. Clin. Virol. 2020, 127, 104357. [Google Scholar] [CrossRef]
- Walsh, N.P.; Gleeson, M.; Shephard, R.J.; Gleeson, M.; Woods, J.A.; Bishop, N.C.; Fleshner, M.; Green, C.; Pedersen, B.K.; Hoffman-Goetz, L.; et al. Position statement. Part one: Immune function and exercise. Exerc. Immunol. Rev. 2011, 17, 6–63. [Google Scholar]
- Martin, S.A.; Pence, B.D.; Woods, J.A. Exercise and respiratory tract viral infections. Exerc. Sport Sci. Rev. 2009, 37, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Da Silveira, M.P.; da Silva Fagundes, K.K.; Bizuti, M.R.; Starck, É.; Rossi, R.C.; de Resende e Silva, D.T. Physical exercise as a tool to help the immune system against COVID-19: An integrative review of the current literature. Clin. Exp. Med. 2021, 21, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Nieman, D.C. Coronavirus disease-2019: A tocsin to our aging, unfit, corpulent, and immunodeficient society. J. Sport Health Sci. 2020, 9, 293–301. [Google Scholar] [CrossRef]
- Nieman, D.C.; Wentz, L.M. The compelling link between physical activity and the body’s defense system. J. Sport Health Sci. 2019, 8, 201–217. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd ed.; Department of Health and Human Services: Washington, DC, USA, 2018.
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Füzéki, E.; Groneberg, D.A.; Banzer, W. Physical activity during COVID-19 induced lockdown: Recommendations. J. Occup. Med. Toxicol. 2020, 15, 25. [Google Scholar] [CrossRef]
- Sallis, J.F.; Adlakha, D.; Oyeyemi, A.; Salvo, D. An international physical activity and public health research agenda to inform coronavirus disease-19 policies and practices. J. Sport Health Sci. 2020, 9, 328–334. [Google Scholar] [CrossRef]
- Sallis, R.; Young, D.R.; Tartof, S.Y.; Sallis, J.F.; Sall, J.; Li, Q.; Smith, G.N.; Cohen, D.A. Physical inactivity is associated with a higher risk for severe COVID-19 outcomes: A study in 48 440 adult patients. Br. J. Sports Med. 2021, 1–8. [Google Scholar]
- Son, J.S.; Nimrod, G.; West, S.T.; Janke, M.C.; Liechty, T.; Naar, J.J. Promoting older adults’ physical activity and social well-being during COVID-19. Leis. Sci. 2021, 43, 287–294. [Google Scholar] [CrossRef]
- Dwyer, M.J.; Pasini, M.; De Dominicis, S.; Righi, E. Physical activity: Benefits and challenges during the COVID-19 pandemic. Scand. J. Med. Sci. Sports 2020, 30, 1291. [Google Scholar] [CrossRef] [PubMed]
- Deschasaux-Tanguy, M.; Druesne-Pecollo, N.; Esseddik, Y.; de Edelenyi, F.S.; Allès, B.; Andreeva, V.A.; Baudry, J.; Charreire, H.; Deschamps, V.; Egnell, M. Diet and physical activity during the coronavirus disease 2019 (COVID-19) lockdown (March-May 2020): Results from the French NutriNet-Santé cohort study. Am. J. Clin. Nutr. 2021, 113, 924–938. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, E.W.; Beyl, R.A.; Fearnbach, S.N.; Altazan, A.D.; Martin, C.K.; Redman, L.M. The impact of COVID-19 stay-at-home orders on health behaviors in adults. Obesity 2021, 29, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.M.; Sultana, A.; Purohit, N. Mental health outcomes of quarantine and isolation for infection prevention: A systematic umbrella review of the global evidence. Epidemiol. Health 2020, 42, e2020038. [Google Scholar] [CrossRef] [PubMed]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef] [PubMed]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical activity change during COVID-19 con-finement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef]
- McCarthy, H.; Potts, H.W.W.; Fisher, A. Physical activity behavior before, during, and after COVID-19 restrictions: Longitudinal smartphone-tracking study of adults in the United Kingdom. J. Med. Internet Res. 2021, 23, e23701. [Google Scholar] [CrossRef]
- Lesser, I.A.; Nienhuis, C.P. The impact of COVID-19 on physical activity behavior and well-being of Canadians. Int. J. Environ. Res. Public Health 2020, 17, 3899. [Google Scholar] [CrossRef] [PubMed]
- Spence, J.C.; Rhodes, R.E.; McCurdy, A.; Mangan, A.; Hopkins, D.; Mummery, W.K. Determinants of physical activity among adults in the United Kingdom during the COVID-19 pandemic: The DUK-COVID study. Br. J. Health Psychol. 2021, 26, 588–605. [Google Scholar] [CrossRef]
- Faulkner, J.; O’Brien, W.J.; McGrane, B.; Wadsworth, D.; Batten, J.; Askew, C.D.; Badenhorst, C.; Byrd, E.; Coulter, M.; Draper, N.; et al. Physical activity, mental health and well-being of adults during initial COVID-19 containment strategies: A multi-country cross-sectional analysis. J. Sci. Med. Sport 2021, 24, 320–326. [Google Scholar] [CrossRef]
- Smith, L.; Jacob, L.; Butler, L.; Schuch, F.; Barnett, Y.; Grabovac, I.; Veronese, N.; Caperchione, C.; Lopez-Sanchez, G.F.; Meyer, J.; et al. Prevalence and correlates of physical activity in a sample of UK adults observing social distancing during the COVID-19 pandemic. BMJ Open Sport Exerc. Med. 2020, 6, e000850. [Google Scholar] [CrossRef] [PubMed]
- Tison, G.H.; Avram, R.; Kuhar, P.; Abreau, S.; Marcus, G.M.; Pletcher, M.J.; Olgin, J.E. Worldwide effect of COVID-19 on physical activity: A descriptive study. Ann. Intern. Med. 2020, 173, 767–770. [Google Scholar] [CrossRef]
- Maertl, T.; de Bock, F.; Huebl, L.; Oberhauser, C.; Coenen, M.; Jung-Sievers, C.; on behalf of the COSMO Study Team. Physical activity during COVID-19 in German adults: Analyses in the COVID-19 Snapshot Monitoring Study (COSMO). Int. J. Environ. Res. Public Health 2021, 18, 507. [Google Scholar] [CrossRef] [PubMed]
- Antunes, R.; Frontini, R.; Amaro, N.; Salvador, R.; Matos, R.; Morouço, P.; Rebelo-Gonçalves, R. Exploring lifestyle habits, physical activity, anxiety and basic psychological needs in a sample of Portuguese adults during COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 4360. [Google Scholar] [CrossRef] [PubMed]
- Khoramipour, K.; Basereh, A.; Hekmatikar, A.A.; Castell, L.; Ruhee, R.T.; Suzuki, K. Physical activity and nutrition guidelines to help with the fight against COVID-19. J. Sports Sci. 2021, 39, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Polero, P.; Rebollo-Seco, C.; Adsuar, J.C.; Pérez-Gómez, J.; Rojo-Ramos, J.; Manzano-Redondo, F.; Garcia-Gordillo, M.Á.; Carlos-Vivas, J. Physical activity recommen-dations during COVID-19: Narrative review. Int. J. Environ. Res. Public Health 2020, 18, 65. [Google Scholar] [CrossRef]
- Marks, D.F. A General Theory of Behaviour; SAGE Publications Ltd.: London, UK, 2018. [Google Scholar]
- Silva, A.M.; Júdice, P.B.; Carraça, E.V.; King, N.; Teixeira, P.J.; Sardinha, L.B. What is the effect of diet and/or exercise interventions on behavioural compensation in non-exercise physical activity and related energy expenditure of free-living adults? A systematic review. Br. J. Nutr. 2018, 119, 1327–1345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauman, A.; Bull, F.; Chey, T.; Craig, C.L.; Ainsworth, B.E.; Sallis, J.F.; Bowles, H.R.; Hagstromer, M.; Sjostrom, M.; Pratt, M.; et al. The International Prevalence Study on Physical Activity: Results from 20 countries. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 21. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- IPAQ Research Committee. Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ)-Short and Long Forms. IPAQ Research Committee. Available online: https://docs.google.com/viewer?a=v&pid=sites&srcid=ZGVmYXVsdGRvbWFpbnx0aGVpcGFxfGd4OjE0NDgxMDk3NDU1YWRlZTM (accessed on 10 August 2020).
- Rezende, L.F.M.; Sá, T.H.; Mielke, G.I.; Viscondi, J.Y.K.; Rey-López, J.P.; Garcia, L.M.T. All-cause mortality attributable to sitting time: Analysis of 54 countries worldwide. Am. J. Prev. Med. 2016, 51, 253–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes, C.; Torres, D.; Oliveira, A.; Severo, M.; Guiomar, S.; Alarcão, V.; Vilela, S.; Ramos, E.; Rodrigues, S.; Oliveira, L.; et al. National food, nutrition and physical activity survey of the Portuguese general population. EFSA Supporting Publ. 2017, 14, 1341E. [Google Scholar] [CrossRef] [Green Version]
- Smith, J. Overcoming the ‘tyranny of the urgent’: Integrating gender into disease outbreak preparedness and response. Gend. Dev. 2019, 27, 355–369. [Google Scholar] [CrossRef]
- Kriaucioniene, V.; Bagdonaviciene, L.; Rodríguez-Pérez, C.; Petkeviciene, J. Associations between changes in health behaviours and body weight during the COVID-19 quarantine in Lithuania: The Lithuanian COVIDiet Study. Nutrients 2020, 12, 3119. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef]
- Sidor, A.; Rzymski, P. Dietary choices and habits during COVID-19 lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef]
- Błaszczyk-Bębenek, E.; Jagielski, P.; Bolesławska, I.; Jagielska, A.; Nitsch-Osuch, A.; Kawalec, P. Nutrition behaviors in Polish adults before and during COVID-19 lockdown. Nutrients 2020, 12, 3084. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, M.; Ponzo, V.; Rosato, R.; Scumaci, E.; Goitre, I.; Benso, A.; Belcastro, S.; Crespi, C.; de Michieli, F.; Ghigo, E.; et al. Changes in weight and nutritional habits in adults with obesity during the "lockdown" period caused by the COVID-19 virus emergency. Nutrients 2020, 12, 2016. [Google Scholar] [CrossRef] [PubMed]
- Reyes-Olavarría, D.; Latorre-Román, P.; Guzmán-Guzmán, I.P.; Jerez-Mayorga, D.; Caamaño-Navarrete, F.; Delgado-Floody, P. Positive and negative changes in food habits, physical activity patterns, and weight status during COVID-19 confinement: Associated factors in the Chilean population. Int. J. Environ. Res. Public Health 2020, 17, 5431. [Google Scholar] [CrossRef]
- Abbas, A.M.; Kamel, M.M. Dietary habits in adults during quarantine in the context of COVID-19 pandemic. Obes. Med. 2020, 19, 100254. [Google Scholar] [CrossRef]
- Zupo, R.; Castellana, F.; Sardone, R.; Sila, A.; Giagulli, V.A.; Triggiani, V.; Cincione, R.I.; Giannelli, G.; de Pergola, G. Preliminary trajectories in dietary behaviors during the COVID-19 pandemic: A public health call to action to face obesity. Int. J. Environ. Res. Public Health 2020, 17, 7073. [Google Scholar] [CrossRef] [PubMed]
- Gregório, M.J.; Rodrigues, A.M.; Graça, P.; de Sousa, R.D.; Dias, S.S.; Branco, J.C.; Canhão, H. Food insecurity is associated with low adherence to the Mediterranean Diet and adverse health conditions in Portuguese adults. Front. Public Health 2018, 6, 38. [Google Scholar] [CrossRef] [PubMed]
- Huizar, M.I.; Arena, R.; Laddu, D.R. The global food syndemic: The impact of food insecurity, malnutrition and obesity on the healthspan amid the COVID-19 pandemic. Prog. Cardiovasc. Dis. 2021, 64, 105–107. [Google Scholar] [CrossRef] [PubMed]
- Mata, J.; Silva Marlene, N.; Vieira Paulo, N.; Carraça Eliana, V.; Andrade Ana, M.; Coutinho Sílvia, R.; Sardinha Luis, B.; Teixeira Pedro, J. Motivational “spill-over” during weight control: Increased self-determination and exercise intrinsic motivation predict eating self-regulation. Health Psychol. 2009, 28, 709–716. [Google Scholar] [CrossRef] [Green Version]
- Carraça, E.V.; Rodrigues, B.; Teixeira, D.S. A motivational pathway linking physical activity to body-related eating cues. J. Nutr. Educ. Behav. 2020, 52, 1001–1007. [Google Scholar] [CrossRef]
- Horton, R. Offline: COVID-19 is not a pandemic. Lancet 2020, 396, 874. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Participants’ Characteristics | Total | Men | Women | p |
|---|---|---|---|---|
| % (95% CI) | % (95% CI) | % (95% CI) | ||
| Age | 45.8 (45.4, 46.3) | 45.5 (44.9, 46.1) | 46.2 (45.6, 46.8) | |
| Age-group | <0.001 | |||
| 16–34 years | 27.9 (26.8, 29.1) | 29.5 (27.8, 31.2) | 26.4 (24.8, 27.9) | |
| 35–54 years | 34.9 (33.7, 36.1) | 35.9 (34.2, 37.7) | 34.0 (32.3, 35.7) | |
| ≥55 years | 37.2 (35.9, 38.4) | 34.5 (32.7, 36.3) | 39.6 (37.9, 41.3) | |
| Education | <0.001 | |||
| Secondary school or below | 81.5 (80.5, 82.5) | 83.5 (82.1, 84.9) | 79.9 (78.5, 81.4) | |
| Higher education | 18.5 (17.5, 19.5) | 16.5 (15.1, 17.9) | 20.1 (18.6, 21.5) | |
| Professional situation | <0.001 | |||
| Employee | 57.4 (56.1, 58.8) | 58.7 (56.8, 60.6) | 56.2 (54.4, 58.0) | |
| Student | 15.1 (14.1, 16.0) | 14.9 (13.5, 16.3) | 15.2 (13.8, 16.5) | |
| Retired | 17.4 (16.4, 18.4) | 19.3 (17.8, 20.9) | 15.7 (14.3, 17.0) | |
| Housekeeper | 3.4 (2.9, 3.8) | 0.1 (0.0, 0.2) | 6.4 (5.5, 7.3) | |
| Unemployed | 6.7 (6.1, 7.4) | 6.9 (6.0, 7.9) | 6.6 (5.7, 7.5) | |
| Subjective financial well-being | 0.004 | |||
| Comfortable or very comfortable | 30.1 (28.9, 31.3) | 30.3 (28.6, 32.1) | 29.9 (28.3, 31.6) | |
| Reasonable | 51.3 (50.0, 52.6) | 52.8 (50.9, 54.7) | 49.8 (48.1, 51.6) | |
| Difficult or very difficult | 18.6 (17.6, 19.7) | 16.8 (15.4, 18.3) | 20.2 (18.8, 21.7) | |
| Children | 0.448 | |||
| No | 67.8 (66.6, 69.0) | 67.3 (65.5, 69.1) | 68.2 (66.6, 69.9) | |
| Yes | 32.2 (31.0, 33.4) | 32.7 (30.9, 34.5) | 31.8 (30.1, 33.4) | |
| Social confinement (reasons) | ||||
| Sickness (COVID-19) | 1.2 (1.0, 1.5) | 1.9 (1.4, 2.4) | 0.7 (0.4, 1.0) | <0.001 |
| Sickness (other) | 2.2 (1.8, 2.6) | 1.3 (0.9, 1.8) | 3.0 (2.4, 3.6) | <0.001 |
| Family support | 16.6 (15.6, 17.6) | 14.3 (12.9, 15.6) | 18.7 (17.3, 20.1) | 0.064 |
| Telework | 30.3 (29.1, 31.5) | 31.5 (29.8, 33.2) | 29.3 (27.7, 30.9) | <0.001 |
| Prophylactic isolation | 5.5 (4.9, 6.1) | 7.9 (6.9, 9.0) | 3.3 (2.7, 4.0) | |
| Lockdown (time) | 0.246 | |||
| Up to 3 weeks | 26.0 (24.9, 27.1) | 26.7 (25.0, 28.3) | 25.5 (23.9, 27.0) | |
| Up to 4 weeks | 43.6 (42.3, 44.9) | 44.0 (42.1, 45.8) | 43.2 (41.5, 44.9) | |
| Up to 5 weeks | 30.3 (29.2, 31.5) | 29.4 (27.7, 31.1) | 31.3 (29.7, 33.0) | |
| Self-rated health | <0.001 | |||
| Very good | 37.4 (36.2, 38.7) | 43.0 (41.2, 44.9) | 32.5 (30.8, 34.1) | |
| Good | 37.2 (36.0, 38.4) | 35.6 (33.8, 37.4) | 38.7 (36.9, 40.4) | |
| Reasonable | 25.4 (24.3, 26.5) | 21.4 (19.9, 22.9) | 28.9 (27.3, 30.5) | |
| Participants’ Characteristics | IPAQ Categories | p | Sitting Time (min/day) | p | ||||
|---|---|---|---|---|---|---|---|---|
| % (95% CI) | % (95% CI) | |||||||
| Low Active | Active | HEPA | <180 | 181–419 | ≥420 | |||
| Total | 33.5 (32.3, 34.7) | 20.5 (19.5, 21.5) | 46.0 (44.7, 47.2) | 34.4 (33.2, 35.7) | 28.4 (27.3, 29.6) | 37.1 (35.9, 38.4) | ||
| Gender | <0.001 | <0.001 | ||||||
| Men | 29.4 (27.7, 31.1) | 20.7 (19.2, 22.2) | 49.9 (48.0, 51.7) | 29.8 (28.1, 31.5) | 30.8 (29.1, 32.5) | 39.4 (37.5, 41.2) | ||
| Women | 37.1 (35.4, 38.8) | 20.3 (18.9, 21.7) | 42.6 (40.9, 44.4) | 38.5 (36.7, 40.2) | 26.4 (24.8, 27.9) | 35.2 (33.5, 36.8) | ||
| Age-group | <0.001 | <0.001 | ||||||
| 16–34 years | 27.5 (25.3, 29.6) | 18.6 (16.7, 20.5) | 53.9 (51.5, 56.3) | 24.4 (22.3, 26.4) | 26.1 (24.0, 28.3) | 49.6 (47.1, 52.0) | ||
| 35–54 years | 37.0 (34.9, 39.1) | 16.3 (14.7, 17.9) | 46.6 (44.4, 48.8) | 36.0 (33.9, 38.1) | 29.0 (27.0, 31.0) | 35.0 (32.9, 37.0) | ||
| ≥55 years | 34.8 (32.8, 36.8) | 25.8 (24.0, 27.7) | 39.4 (37.3, 41.4) | 40.6 (38.5, 42.6) | 29.6 (27.7, 31.5) | 29.8 (27.8, 31.7) | ||
| Education | <0.001 | <0.001 | ||||||
| Secondary school or below | 34.6 (33.3, 36.0) | 20.8 (19.7, 22.0) | 44.6 (43.1, 46.0) | 37.4 (36.0, 38.8) | 28.9 (27.6, 30.1) | 33.7 (32.4, 35.1) | ||
| Higher education | 28.7 (26.0, 31.4) | 19.1 (16.8, 21.4) | 52.2 (49.2, 55.2) | 21.4 (19.0, 23.8) | 26.7 (24.0, 29.3) | 52.0 (49.1, 55.0) | ||
| Family income perception | <0.001 | <0.001 | ||||||
| Good | 25.6 (23.5, 27.6) | 21.7 (19.8, 23.7) | 52.7 (50.3, 55.1) | 33.7 (31.5, 36.0) | 26.4 (24.3, 28.5) | 39.9 (37.5, 42.2) | ||
| Reasonable | 34.9 (33.2, 36.6) | 21.7 (20.2, 23.2) | 43.4 (41.6, 45.3) | 31.4 (29.7, 33.1) | 29.1 (27.5, 30.8) | 39.5 (37.7, 41.3) | ||
| Poor | 40.8 (37.8, 43.7) | 16.9 (14.7, 19.2) | 42.3 (39.3, 45.3) | 39.7 (36.8, 42.7) | 29.8 (27.0, 32.5) | 30.5 (27.7, 33.3) | ||
| PA recommendation knowledge | <0.001 | 0.234 | ||||||
| Yes | 34.8 (33.0, 36.6) | 19.5 (18.0, 21.0) | 45.7 (43.8, 47.6) | 37.6 (35.7, 39.4) | 27.5 (25.8, 29.2) | 34.9 (33.1, 36.7) | ||
| No | 32.5 (30.8, 34.1) | 21.3 (19.9, 22.7) | 46.3 (44.5, 48.0) | 31.8 (30.2, 33.4) | 29.2 (27.6, 30.8) | 38.9 (37.2, 40.6) | ||
| PA usefulness of recommendations | <0.001 | <0.001 | ||||||
| Not useful | 36.2 (30.9, 41.5) | 13.7 (9.9, 17.4) | 50.2 (44.6, 55.7) | 24.4 (19.7, 29.2) | 38.1 (32.7, 43.5 | 37.1 (31.8, 42.5) | ||
| I am not sure | 41.7 (35.9, 47.5) | 23.0 (18.1, 28.0) | 35.3 (29.6, 40.9) | 36.3 (30.7, 42.0) | 19.1 (14.4, 23.7) | 45.0 (39.1, 50.8) | ||
| Very useful | 33.7 (31.7, 35.7) | 19.9 (18.2, 21.6) | 46.4 (44.2, 48.5) | 39.7 (37.6, 41.8) | 27.0 (25.1, 28.9) | 33.3 (31.2, 35.3) | ||
| Lockdown (time) | 0.005 | 0.015 | ||||||
| Up to 3 weeks | 35.5 (33.1, 37.9) | 19.0 (17.0, 20.9) | 45.5 (43.0, 48.0) | 37.9 (35.4, 40.3) | 28.1 (25.9, 30.4) | 34.1 (31.7, 36.4) | ||
| Up to 4 weeks | 31.0 (29.2, 32.8) | 21.7 (20.1, 23.3 | 47.3 (45.4, 49.3) | 33.1 (31.3, 34.9) | 28.5 (26.7, 30.2) | 38.4 (36.5, 40.3) | ||
| Up to 5 weeks | 35.6 (33.3, 37.8) | 20.1 (18.2, 22.0) | 44.3 (42.0, 46.7) | 33.4 (31.2, 35.6) | 28.7 (26.6, 30.8) | 37.9 (35.7, 40.2) | ||
| Physical Activities and Sedentary Behaviours | Men | Women | p |
|---|---|---|---|
| % (95% CI) | % (95% CI) | ||
| Types of physical activities | |||
| House cleaning | 51.1 (49.2, 52.9) | 86.7 (85.5, 87.9) | <0.001 |
| Up and down stairs | 49.3 (47.4, 51.2) | 50.6 (48.9, 52.4) | 0.294 |
| Walking | 31.5 (29.8, 33.3) | 32.9 (31.3, 34.6) | 0.253 |
| Fitness activities | 21.5 (19.9, 23.0) | 28.9 (27.3, 30.5) | <0.001 |
| Gardening | 21.8 (20.2, 23.3) | 23.3 (21.9, 24.8) | 0.147 |
| Bricolage | 24.0 (22.4, 25.6) | 14.2 (13.0, 15.4) | <0.001 |
| Strength training | 23.7 (22.1, 25.3) | 12.9 (11.7, 14.1) | <0.001 |
| Jogging | 22.7 (21.1, 24.2) | 6.5 (5.6, 7.3) | <0.001 |
| Static bicycle | 11.7 (10.5, 12.9) | 5.3 (4.5, 6.0) | <0.001 |
| Dance | 2.2 (1.6, 2.7) | 10.1 (9.1, 11.2) | <0.001 |
| Types of sedentary behaviours | |||
| Watching television | 70.6 (68.9, 72.3) | 69.5 (67.8, 71.1) | 0.359 |
| Computer, tablet, smartphone | 66.5 (64.7, 68.2) | 55.4 (53.7, 57.2) | <0.001 |
| Telework | 39.0 (37.2, 40.8) | 34.4 (32.7, 36.1) | <0.001 |
| Read | 28.6 (26.9, 30.3) | 33.8 (32.2, 35.5) | <0.001 |
| Board games, puzzles, Legos | 8.2 (7.2, 9.2) | 9.2 (8.2, 10.2) | 0.191 |
| Play musical instrument | 3.7 (3.0, 4.4) | 1.2 (0.8, 1.6) | <0.001 |
| Self-Reported Changes of Food Behaviours | Total | Men | Women | p |
|---|---|---|---|---|
| % (95% CI) | % (95% CI) | % (95% CI) | ||
| Changes in dietary habits | <0.001 | |||
| Yes | 45.1 (43.9, 46.4) | 42.6 (40.8, 44.5) | 47.3 (45.5, 49.0) | |
| No | 54.9 (53.6, 56.1) | 57.4 (55.5, 59.2) | 52.7 (50.9, 54.4) | |
| Changes in diet quality | 0.037 | |||
| No changes/do not know | 62.2 (60.4, 64.0) | 63.8 (61.3, 66.5) | 60.9 (48.5, 63.4) | |
| Yes | 37.8 (36.5, 39.0) | 36.2 (34.4, 38.0) | 39.1 (37.4, 40.8) | |
| Improved (from those who reported changes) | 58.1 (56.1, 60.2) | 59.7 (56.6, 62.7) | 56.9 (54.2, 59.7) | 0.193 |
| Worsened (from those who reported changes) | 41.9 (39.8, 43.9) | 40.3 (37.3, 43.4) | 43.1 (40.3, 45.9) | |
| Cook more often | <0.001 | |||
| Yes | 56.9 (55.6, 58.1) | 51.8 (49.9, 53.6) | 61.4 (59.7, 63.1) | |
| No | 43.1 (41.9, 44.4) | 48.2 (46.4, 50.1) | 38.6 (36.9, 40.3) | |
| Change in the number of meals | 0.007 | |||
| No | 69.8 (68.6, 71.0) | 71.6 (69.9, 73.3) | 68.4 (66.7, 70.0) | |
| Yes | 30.2 (29.0,31.3) | 28.4 (26.7, 30.1) | 31.6 (30.0, 33.3) | |
| Increased (from those who reported changes) | 67.8 (65.6, 69.9) | 66.5 (63.1, 69.7) | 68.8 (65.8, 71.6) | 0.328 |
| Decreased (from those who reported changes) | 32.2 (30.1, 34.4) | 33.5 (30.1, 36.7) | 31.2 (28.4, 34.2) | |
| Snacking more often * | 0.186 | |||
| Yes | 31.4 (30.2, 32.6) | 32.2/30.5, 34.0) | 30.6 (29.0, 32.3) | |
| No | 68.6 (67.4, 69.8) | 67.8 (66.0, 69.5) | 69.4 (67.7, 71.0) | |
| Changes on shopping frequency | <0.001 | |||
| Decreased | 87.3 (86.3, 88.3) | 82.5 (80.7, 84.2) | 91.1 (89.9, 92.3) | |
| Increased | 12.7 (11.7, 13.7) | 17.5 (15.8, 19.3) | 8.9 (7.7, 10.1) | 0.317 |
| Self-reported changes in body weight | ||||
| No changes/do not know | 66.1 (63.8, 68.4) | 63.4 (60.2, 66.7) | 68.4 (65.2, 71.7) | |
| Increased | 21.0 (20.0, 22.0) | 22.3 (20.8, 23.9) | 19.8 (18.5, 21.3) | |
| Decreased | 12.9 (12.1, 13.8) | 14.3 (13.0, 15.6) | 11.7 (10.7, 12.9) | |
| Knowledge about dietary recommendations for lockdown period | <0.001 | |||
| Yes | 45.3 (44.0, 46.6) | 38.5 (36.7, 40.3) | 51.4 (49.6, 53.2) | |
| No | 54.7 (53.4, 56.0) | 61.5 (59.7, 63.3) | 48.6 (46.8, 50.4) | |
| Usefulness of dietary recommendations for lockdown period | <0.001 | |||
| None | 11.9 (10.7, 13.2) | 14.7 (12.7, 17.0) | 10.0 (8.6, 11.5) | |
| I am not sure | 10.5 (9.4, 11.7) | 9.2 (7.6, 11.0) | 11.3 (9.8, 12.9) | |
| Very useful | 77.6 (76.0, 79.2) | 76.0 (73.4, 78.5) | 78.7 (76.6, 80.6) |
| Food Category | Reduced Intake | p | Increased Intake | p | Maintained Intake | |||
|---|---|---|---|---|---|---|---|---|
| Men | Women | Men | Women | Men | Women | |||
| % (95% CI) | % (95% CI) | % (95% CI) | % (95% CI) | % (95% CI) | % (95% CI) | |||
| Take-away or delivered meals | 43.3 (41.5, 45.2) | 44.3 (42.6, 46.1) | 0.459 | 9.8 (8.8, 11.0) | 5.5 (4.7, 6.3) | <0.001 | 46.9 (45.0, 48.7) | 50.2 (48.4, 52.0) |
| Ready meals | 40.5 (38.7, 42.4) | 40.8 (39.1, 42.6) | 0.831 | 6.7 (5.9, 7.7) | 3.3 (2.7, 3.9) | <0.001 | 52.7 (50.8, 54.6) | 55.9 (54.1, 57.6) |
| Soft drinks | 33.5 (31.7, 35.2) | 32.2 (30.6, 33.9) | 0.328 | 4.6 (3.8, 5.4) | 3.0 (2.5, 3.7) | 0.003 | 62.0 (60.2, 63.8) | 64.8 (63.0, 66.4) |
| Alcoholic beverages | 30.3 (28.6, 32.0) | 26.4 (24.9, 28.0) | 0.001 | 12.7 (11.6, 14.0) | 6.8 (6.0, 7.7) | <0.001 | 57.0 (55.2, 58.9) | 66.8 (65.1, 68.4) |
| Savoury snacks | 28.2 (26.6, 29.9) | 30.7 (29.0, 32.3 | 0.044 | 9.3 (8.3, 10.4) | 8.5 (7.6, 9.5) | 0.311 | 62.5 (60.7, 64.3) | 60.8 (59.1, 62.5) |
| Sweet snacks | 19.0 (17.6, 20.5) | 20.9 (19.5, 22.3) | 0.082 | 28.8 (27.2, 30.6) | 32.8 (31.1, 34.4) | 0.001 | 52.2 (50.3, 54.0) | 46.4 (44.6, 48.1) |
| Fish and other seafood | 17.0 (15.7, 18.5) | 15.1 (13.8, 16.3) | 0.041 | 15.5 (14.2, 16.9) | 13.7 (12.5, 14.9) | 0.053 | 67.5 (65.7, 69.2) | 71.2 (69.6, 72.8) |
| Fruit juices | 14.1 (12.8, 15.4) | 17.0 (15.7, 18.3) | 0.003 | 12.6 (11.4, 13.9) | 12.0 (10.9, 13.2) | 0.498 | 73.2 (71.6, 74.9) | 71.0 (69.4, 72.6) |
| Other canned food (not seafood) | 13.8 (12.6, 15.1) | 16.4 (15.1, 17.7) | 0.006 | 9.5 (8.5, 10.7) | 9.9 (8.8, 10.9) | 0.69 | 76.7 (75.1, 78.3) | 73.8 (72.2, 75.3) |
| Meat | 12.5 (11.3, 13.7) | 11.8 (10.7, 13.0) | 0.47 | 8.6 (7.6, 9.7) | 6.8 (5.9, 7.7) | 0.012 | 78.9 (77.4, 80.5) | 81.4 (80.0, 82.7) |
| Canned seafood | 12.0 (10.8, 13.2) | 14.1 (12.9, 15.4) | 0.018 | 13.2 (11.9, 14.5) | 11.6 (10.5, 12.8) | 0.079 | 74.8 (73.2, 76.4) | 74.3 (72.7, 75.8) |
| Vegetables | 10.8 (9.6, 12.0) | 9.9 (8.9, 11.0) | 0.301 | 19.9 (18.4, 21.4) | 22.1 (20.7, 23.6) | 0.04 | 69.4 (67.6, 71.1) | 68.0 (66.3, 69.6) |
| Water | 10.2 (9.1, 11.4) | 14.2 (13.0, 15.5) | <0.001 | 31.4 (29.7, 33.1) | 30.8 (29.2, 32.4) | <0.001 | 58.4 (56.6, 60.3) | 55.0 (53.3, 56.8) |
| Fruit | 8.2 (7.2, 9.3) | 8.0 (7.1, 9.0) | 0.773 | 32.2 (30.5, 34.0) | 27.4 (25.9, 29.0) | <0.001 | 59.6 (57.8, 61.4) | 64.6 (62.9, 66.2) |
| Dietary patterns | Total; % (95% CI) | Men; % (95% CI) | Women; % (95% CI) | p | ||||
| Improved dietary patterns | 18.2 (17.2, 19.2) | 18.1 (16.7, 19.6) | 18.3 (16.9, 19.7) | 0.193 | ||||
| Worsened dietary patterns | 10.8 (10.1, 11.7) | 12.9 (11.7, 14.2) | 9.0 (8.0, 10.1) | |||||
| Reasons for Changes in Food Intake | Total | Men | Women | p |
|---|---|---|---|---|
| % (95% CI) | % (95% CI) | % (95% CI) | ||
| Changes in shopping frequency | 34.3 (33.1, 35.5) | 34.8 (33.0, 36.6) | 33.9 (32.3, 35.6) | 0.469 |
| Changes in appetite | 19.3 (18.3, 20.3) | 18.0 (16.6, 19.4) | 20.5 (19.1, 21.9) | 0.015 |
| Changes in appetite caused by stress | 18.6 (17.6, 19.6) | 14.1 (12.9, 15.5) | 22.6 (21.1, 24.0) | <0.001 |
| Different work schedule | 17.6 (16.6, 18.6) | 19.5 (18.0, 21.0) | 15.9 (14.7, 17.2) | <0.001 |
| Changes in regular place for shopping | 10.6 (9.9, 11.4) | 10.5 (9.4, 11.7) | 10.6 (9.6, 11.7) | 0.91 |
| Concerns with the economic context | 10.3 (9.5, 11.1) | 9.9 (8.8, 11.0) | 10.6 (9.5, 11.7) | 0.391 |
| Different people at meals time | 9.7 (9.0, 10.5) | 9.8 (8.8, 11.0) | 9.7 (8.7, 10.8) | 0.873 |
| Problems with access to usually bought food | 9.1 (8.4, 9.9) | 9.5 (8.5, 10.7) | 8.7 (7.8, 9.8) | 0.311 |
| Because diet can protect against the novel coronavirus | 5.5 (5.0, 6.1) | 6.0 (5.2, 7.0) | 5.1 (4.3, 5.9) | 0.114 |
| Changes on food prices | 4.8 (4.3, 5.4) | 5.3 (4.5, 6.2) | 4.3 (3.7, 5.1) | 0.087 |
| Fear of getting infected with the novel coronavirus through food | 3.8 (3.3, 4.3) | 4.0 (3.4, 4.8) | 3.5 (2.9, 4.2) | 0.264 |
| Concerns with possible stock rupture of food in supermarkets | 2.5 (2.1, 2.9) | 3.5 (2.9, 4.3) | 1.6 (1.2, 2.0) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, M.N.; Gregório, M.J.; Santos, R.; Marques, A.; Rodrigues, B.; Godinho, C.; Silva, C.S.; Mendes, R.; Graça, P.; Arriaga, M.; et al. Towards an In-Depth Understanding of Physical Activity and Eating Behaviours during COVID-19 Social Confinement: A Combined Approach from a Portuguese National Survey. Nutrients 2021, 13, 2685. https://doi.org/10.3390/nu13082685
Silva MN, Gregório MJ, Santos R, Marques A, Rodrigues B, Godinho C, Silva CS, Mendes R, Graça P, Arriaga M, et al. Towards an In-Depth Understanding of Physical Activity and Eating Behaviours during COVID-19 Social Confinement: A Combined Approach from a Portuguese National Survey. Nutrients. 2021; 13(8):2685. https://doi.org/10.3390/nu13082685
Chicago/Turabian StyleSilva, Marlene Nunes, Maria João Gregório, Rute Santos, Adilson Marques, Bruno Rodrigues, Cristina Godinho, Catarina Santos Silva, Romeu Mendes, Pedro Graça, Miguel Arriaga, and et al. 2021. "Towards an In-Depth Understanding of Physical Activity and Eating Behaviours during COVID-19 Social Confinement: A Combined Approach from a Portuguese National Survey" Nutrients 13, no. 8: 2685. https://doi.org/10.3390/nu13082685
APA StyleSilva, M. N., Gregório, M. J., Santos, R., Marques, A., Rodrigues, B., Godinho, C., Silva, C. S., Mendes, R., Graça, P., Arriaga, M., & Freitas, G. (2021). Towards an In-Depth Understanding of Physical Activity and Eating Behaviours during COVID-19 Social Confinement: A Combined Approach from a Portuguese National Survey. Nutrients, 13(8), 2685. https://doi.org/10.3390/nu13082685