
Canadian Nationwide Survey on Pediatric Malnutrition Management in Tertiary Hospitals

Abstract
:1. Introduction
- To survey current in-hospital practices for the screening, assessment and management of pediatric DAM in Canadian tertiary hospitals.
- To obtain knowledge about current discharge practices and follow-up protocols for the management of DAM.
- To inquire about further education and training desires of tertiary care-level pediatric health care providers (registered dietitians (RDs), registered nurses (RNs) and medical doctors (MDs)) caring for malnourished children.
2. Materials and Methods
2.1. Survey Development and Distribution
2.2. Statistical Analysis
3. Results
3.1. Characteristics of Participants and Participating Hospitals
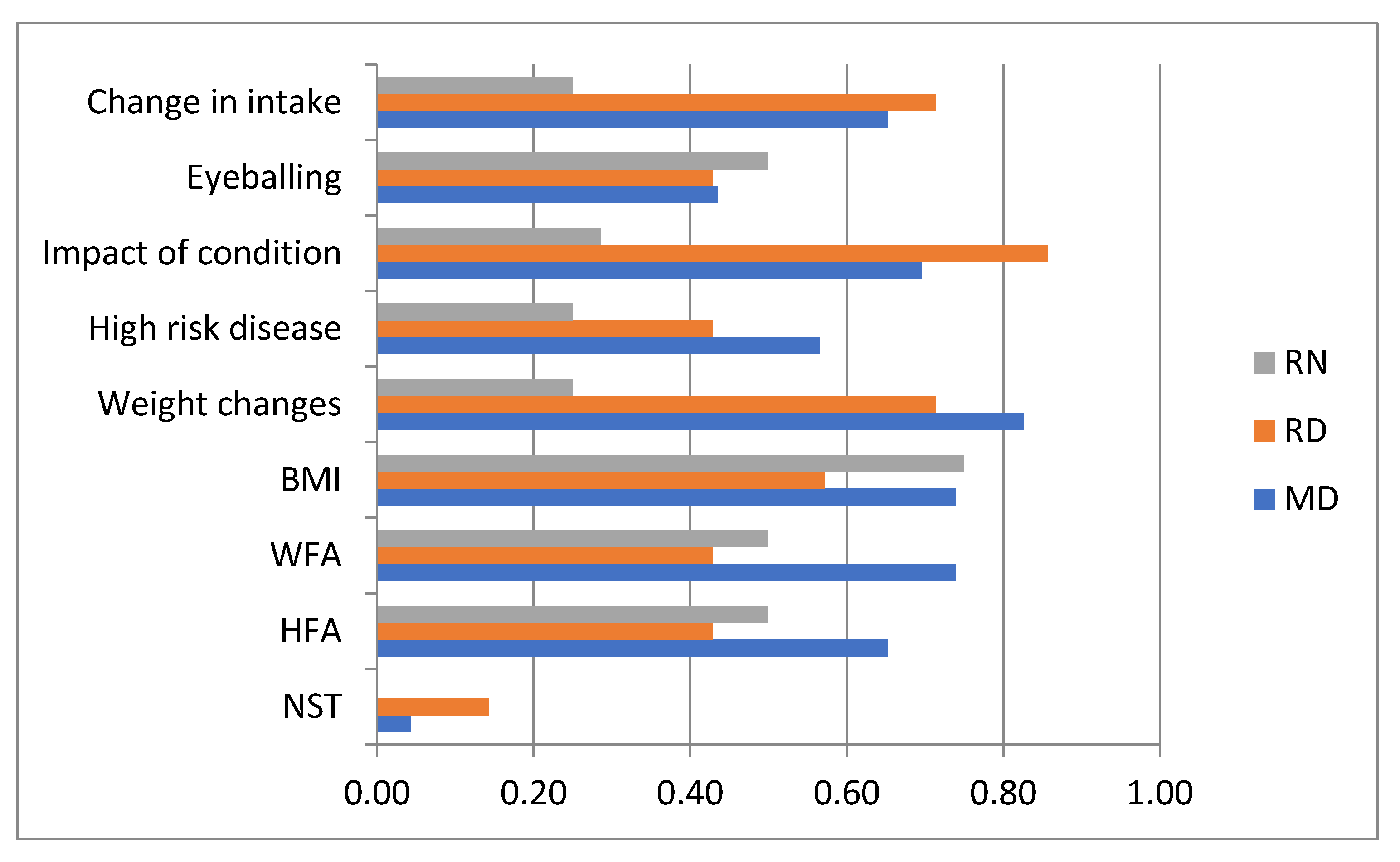
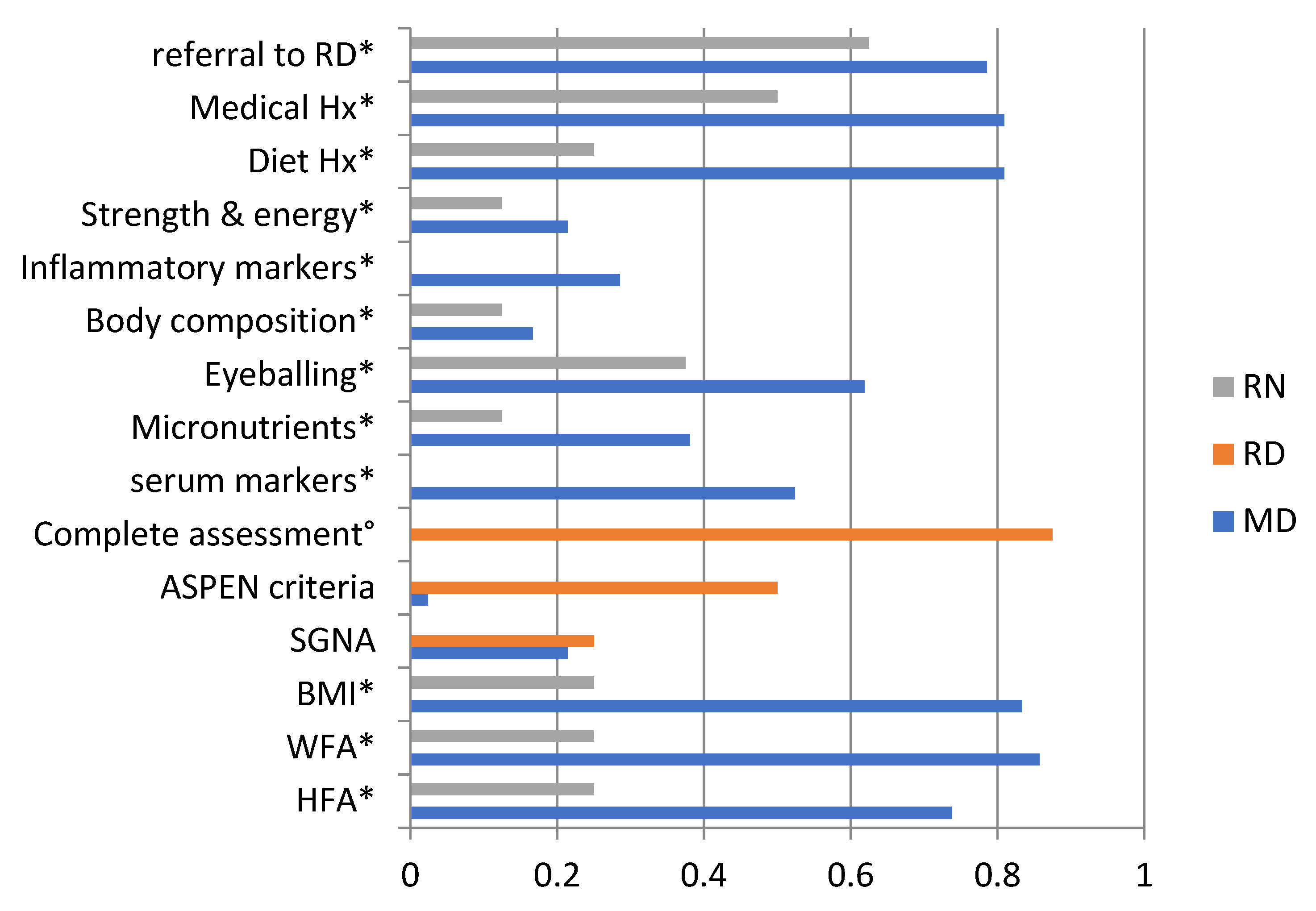
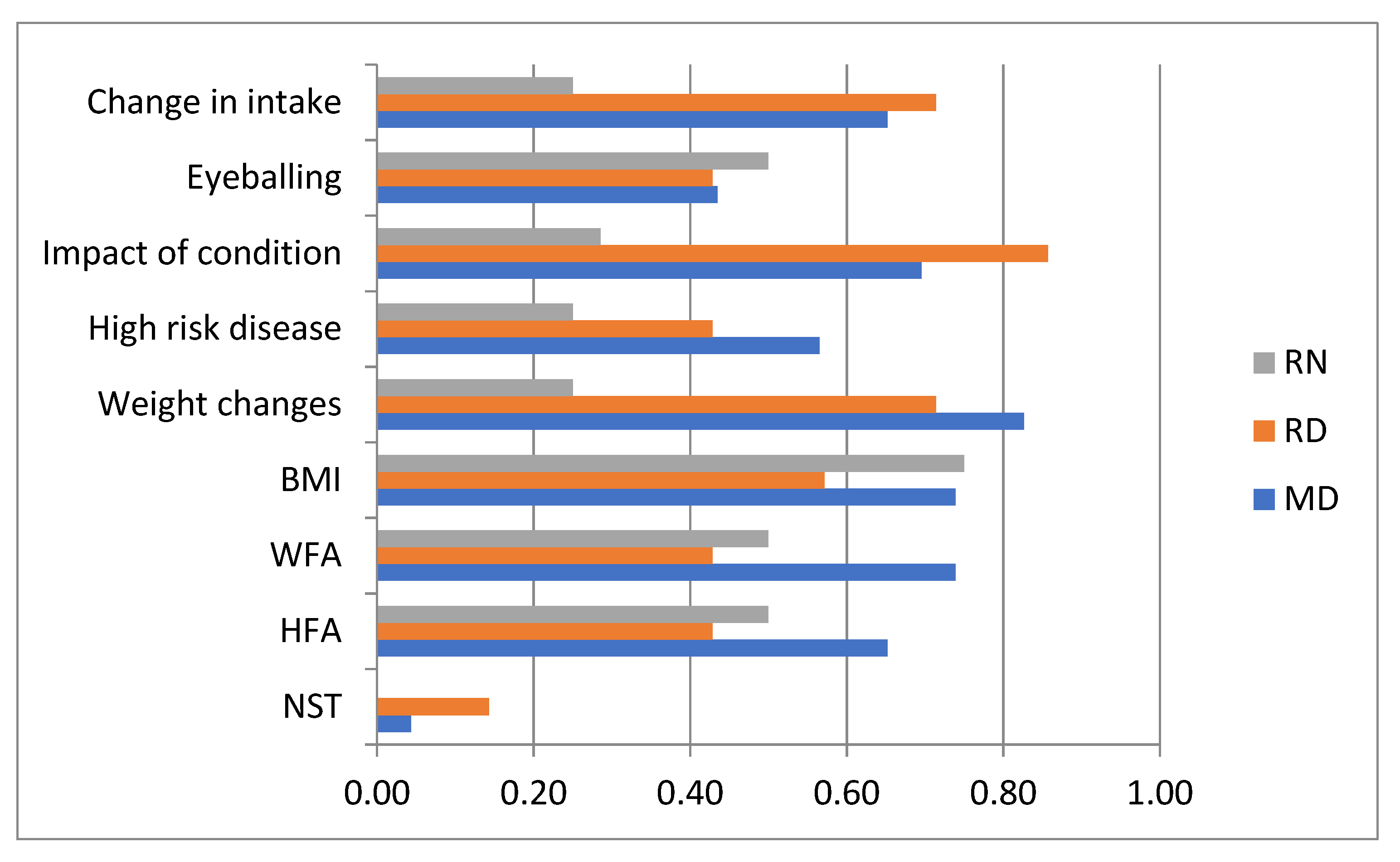
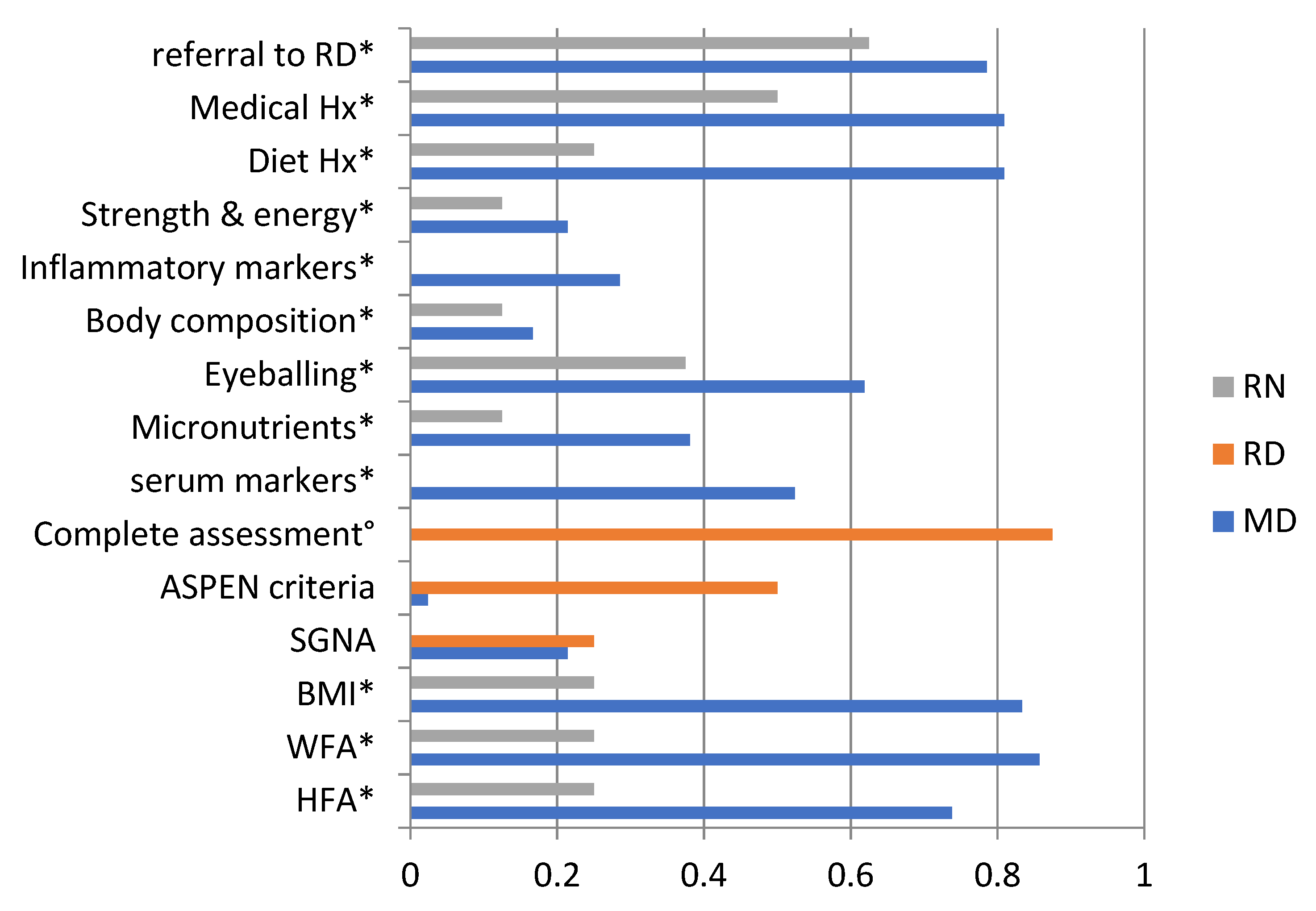
3.2. Nutritional Screening and Assessment
3.3. Nutritional Management
3.4. Discharge Practices and Follow-Up Protocols
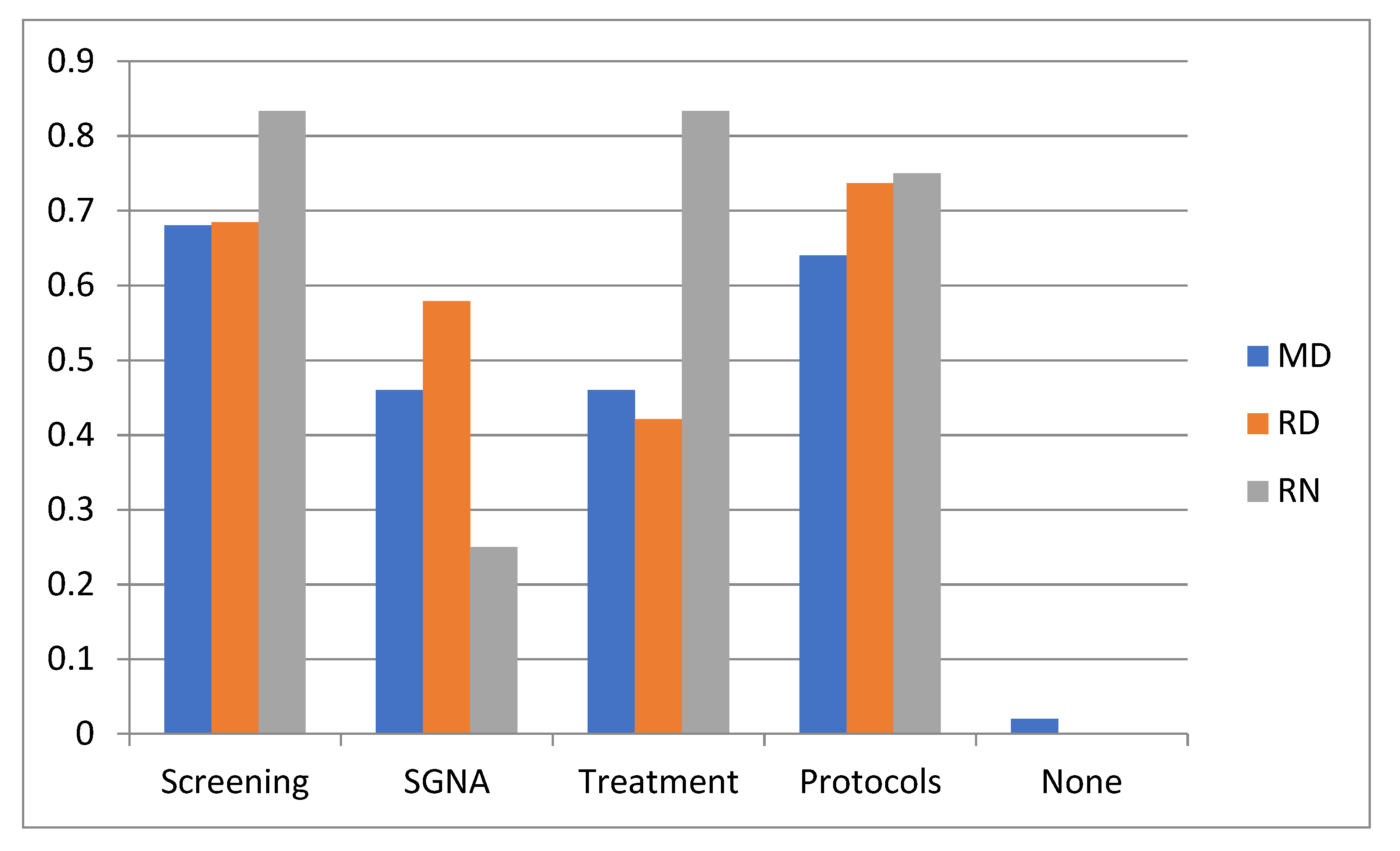
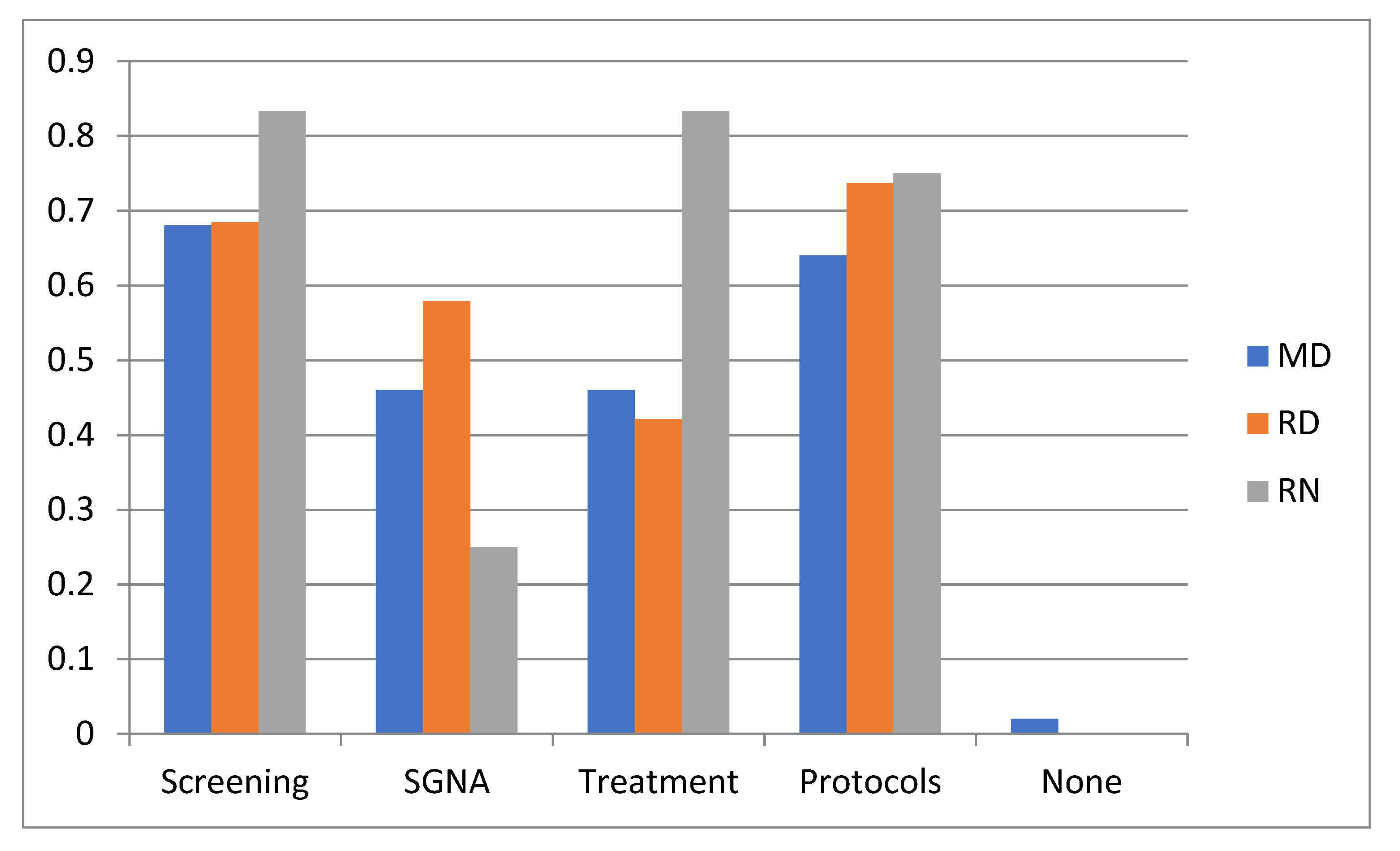
3.5. Further Education and Training Desires
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baxter, J.A.B.; Al-Madhaki, F.I.; Zlotkin, S.H. Prevalence of malnutrition at the time of admission among patients admitted to a Canadian tertiary-care paediatric hospital. Paediatr. Child Health 2014, 19, 413–417. [Google Scholar] [CrossRef] [Green Version]
- Belanger, V.; McCarthy, A.; Marcil, V.; Marchand, V.; Boctor, D.L.; Rashid, M.; Noble, A.; Avinashi, V.; Davidson, B.; Groleau, V.; et al. Assessment of Malnutrition Risk in Canadian Pediatric Hospitals: A Multicenter Prospective Cohort Study. J. Pediatr. 2019, 205, 160–167.e6. [Google Scholar] [CrossRef] [PubMed]
- Carter, L.E.; Shoyele, G.; Southon, S.; Farmer, A.; Persad, R.; Mazurak, V.C.; BrunetWood, M.K. Screening for Pediatric Malnutrition at Hospital Admission: Which Screening Tool Is Best? Nutr. Clin. Pract. Off. Publ. Am. Soc. Parenter. Enter. Nutr. 2019. [Google Scholar] [CrossRef] [Green Version]
- Huysentruyt, K.; De Schepper, J.; Bontems, P.; Alliet, P.; Peeters, E.; Roelants, M.; Van Biervliet, S.; Hauser, B.; Vandenplas, Y. Proposal for An Algorithm for Screening for Undernutrition in Hospitalized Children. J. Pediatr. Gastroenterol. Nutr. 2016, 63, e86–e91. [Google Scholar] [CrossRef]
- Mehta, N.M.; Corkins, M.R.; Lyman, B.; Malone, A.; Goday, P.S.; Carney, L.N.; Monczka, J.L.; Plogsted, S.W.; Schwenk, W.F. Defining pediatric malnutrition: A paradigm shift toward etiology-related definitions. J. Parenter. Enteral. Nutr. 2013, 37, 460–481. [Google Scholar] [CrossRef] [Green Version]
- Huysentruyt, K.; Hulst, J.; Bian, F.; Shamir, R.; White, M.; Galera-Martinez, R.; Morais-Lopez, A.; Kansu, A.; Gerasimidis, K. Opinions and practices of healthcare professionals on assessment of disease associated malnutrition in children: Results from an international survey. Clin. Nutr. 2019, 38, 708–714. [Google Scholar] [CrossRef] [Green Version]
- Huysentruyt, K.; Alliet, P.; Muyshont, L.; Devreker, T.; Bontems, P.; Vandenplas, Y. Hospital-related undernutrition in children: Still an often unrecognized and undertreated problem. Acta Paediatr. 2013, 102, e460–e466. [Google Scholar] [CrossRef]
- Kim, S.; Lee, E.H.; Yang, H.R. Current status of nutritional support for hospitalized children: A nationwide hospital-based survey in South Korea. Nutr. Res. Pract. 2018, 12, 215–221. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing, version 3.6.2; R Foundation for Statistical Computing: Vienna, Austria, 2014. [Google Scholar]
- Agostoni, C.; Axelson, I.; Colomb, V.; Goulet, O.; Koletzko, B.; Michaelsen, K.F.; Puntis, J.W.; Rigo, J.; Shamir, R.; Szajewska, H.; et al. The need for nutrition support teams in pediatric units: A commentary by the ESPGHAN committee on nutrition. J. Pediatr. Gastroenterol. Nutr. 2005, 41, 8–11. [Google Scholar] [CrossRef]
- Joosten, K.F.; Hulst, J.M. Nutritional screening tools for hospitalized children: Methodological considerations. Clin. Nutr. 2014, 33, 1–5. [Google Scholar] [CrossRef]
- Hankard, R.; Bloch, J.; Martin, P.; Randrianasolo, H.; Bannier, M.F.; Machinot, S.; Cezard, J.P. Nutritional status and risk in hospitalized children. Arch. Pediatr. 2001, 8, 1203–1208. [Google Scholar] [CrossRef]
- Olsen, E.M.; Petersen, J.; Skovgaard, A.M.; Weile, B.; Jorgensen, T.; Wright, C.M. Failure to thrive: The prevalence and concurrence of anthropometric criteria in a general infant population. Arch. Dis. Child 2007, 92, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Carvalho-Salemi, J.; Salemi, J.L.; Wong-Vega, M.R.; Spooner, K.K.; Juarez, M.D.; Beer, S.S.; Canada, N.L. Malnutrition among Hospitalized Children in the United States: Changing Prevalence, Clinical Correlates, and Practice Patterns between 2002 and 2011. J. Acad. Nutr. Diet. 2018, 118, 40–51.e7. [Google Scholar] [CrossRef]
- Becker, P.; Carney, L.N.; Corkins, M.R.; Monczka, J.; Smith, E.; Smith, S.E.; Spear, B.A.; White, J.V.; Academy of Nutrition and Dietetics; American Society for Parenteral and Enteral Nutrition. Consensus statement of the Academy of Nutrition and Dietetics/American Society for Parenteral and Enteral Nutrition: Indicators recommended for the identification and documentation of pediatric malnutrition (undernutrition). Nutr. Clin. Pract. 2015, 30, 147–161. [Google Scholar] [CrossRef]
- Obadia, M.; Rakhshani, N.; Jeffery, A.S.; Chahal, N.; Sangha, G.; McCrindle, B.W.; O’Connor, D.L.; Maccarone, T.; Hamilton, J.K. MEALTRAIN: What do inpatient hospitalized children choose to eat? J. Pediatr. 2010, 156, 685–686. [Google Scholar] [CrossRef]
- Carter, L.E.; Klatchuk, N.; Sherman, K.; Thomsen, P.; Mazurak, V.C.; Brunetwood, M.K. Barriers to Oral Food Intake for Children Admitted to Hospital. Can. J. Diet. Pract. Res. Publ. Dietit. Can. 2019, 80, 195–199. [Google Scholar] [CrossRef]
- Allard, J.P.; Keller, H.; Jeejeebhoy, K.N.; Laporte, M.; Duerksen, D.R.; Gramlich, L.; Payette, H.; Bernier, P.; Vesnaver, E.; Davidson, B.; et al. Malnutrition at Hospital Admission-Contributors and Effect on Length of Stay: A Prospective Cohort Study From the Canadian Malnutrition Task Force. J. Parenter. Enteral. Nutr. 2016, 40, 487–497. [Google Scholar] [CrossRef]
- Thibault, R.; Chikhi, M.; Clerc, A.; Darmon, P.; Chopard, P.; Genton, L.; Kossovsky, M.P.; Pichard, C. Assessment of food intake in hospitalised patients: A 10-year comparative study of a prospective hospital survey. Clin. Nutr. 2011, 30, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, E.; Ferguson, M.; Banks, M.; Batterham, M.; Bauer, J.; Capra, S.; Isenring, E. Malnutrition and poor food intake are associated with prolonged hospital stay, frequent readmissions, and greater in-hospital mortality: Results from the Nutrition Care Day Survey 2010. Clin. Nutr. 2013, 32, 737–745. [Google Scholar] [CrossRef] [Green Version]
- Allard, J.P.; Keller, H.; Teterina, A.; Jeejeebhoy, K.N.; Laporte, M.; Duerksen, D.R.; Gramlich, L.; Payette, H.; Bernier, P.; Davidson, B.; et al. Factors associated with nutritional decline in hospitalised medical and surgical patients admitted for 7 d or more: A prospective cohort study. Br. J. Nutr. 2015, 114, 1612–1622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiesmayr, M.; Schindler, K.; Pernicka, E.; Schuh, C.; Schoeniger-Hekele, A.; Bauer, P.; Laviano, A.; Lovell, A.D.; Mouhieddine, M.; Schuetz, T.; et al. Decreased food intake is a risk factor for mortality in hospitalised patients: The NutritionDay survey 2006. Clin. Nutr. 2009, 28, 484–491. [Google Scholar] [CrossRef]
- Jeejeebhoy, K.N.; Keller, H.; Gramlich, L.; Allard, J.P.; Laporte, M.; Duerksen, D.R.; Payette, H.; Bernier, P.; Vesnaver, E.; Davidson, B.; et al. Nutritional assessment: Comparison of clinical assessment and objective variables for the prediction of length of hospital stay and readmission. Am. J. Clin. Nutr. 2015, 101, 956–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keller, H.; Allard, J.P.; Laporte, M.; Davidson, B.; Payette, H.; Bernier, P.; Jeejeebhoy, K.; Duerksen, D.R.; Gramlich, L. Predictors of dietitian consult on medical and surgical wards. Clin. Nutr. 2015, 34, 1141–1145. [Google Scholar] [CrossRef] [PubMed]
- Palmer, M.; Miller, K.; Noble, S. The accuracy of food intake charts completed by nursing staff as part of usual care when no additional training in completing intake tools is provided. Clin. Nutr. 2015, 34, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Keller, H.H.; Valaitis, R.; Laur, C.V.; McNicholl, T.; Xu, Y.; Dubin, J.A.; Curtis, L.; Obiorah, S.; Ray, S.; Bernier, P.; et al. Multi-site implementation of nutrition screening and diagnosis in medical care units: Success of the More-2-Eat project. Clin. Nutr. 2019, 38, 897–905. [Google Scholar] [CrossRef] [Green Version]
- Braegger, C.; Decsi, T.; Dias, J.A.; Hartman, C.; Kolacek, S.; Koletzko, B.; Koletzko, S.; Mihatsch, W.; Moreno, L.; Puntis, J.; et al. Practical approach to paediatric enteral nutrition: A comment by the ESPGHAN committee on nutrition. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 110–122. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| D/C or Follow-Up Practice | N * (%) |
|---|---|
| Info on nutritional status in D/C summary: | |
| Yes | 20 (23.8) |
| Only if malnourished | 50 (59.5) |
| No/don’t know | 10 (11.9) |
| Other | 4 (4.8) |
| Weight and height measured at D/C: | |
| Always | 6 (7.2) |
| Mostly | 19 (22.9) |
| Sometimes | 29 (34.9) |
| Never | 10 (12.0) |
| Other | 19 (22.9) |
| Terms describing poor nutritional status in D/C summary °: | |
| Failure to thrive | 52 (74.3) |
| Growth failure | 22 (31.4) |
| ICD-10 code | 22 (31.4) |
| Not common/not applicable | 5 (7.1) |
| Other | 11 (15.7) |
| Post-D/C transfer of nutrition care of malnourished child: | |
| Always | 27 (39.7) |
| Sometimes | 32 (47.1) |
| Never | 1 (1.5) |
| Don’t know | 8 (11.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huysentruyt, K.; Brunet-Wood, K.; Bandsma, R.; Gramlich, L.; Fleming-Carroll, B.; Hotson, B.; Byers, R.; Lovelace, H.; Persad, R.; Kalnins, D.; et al. Canadian Nationwide Survey on Pediatric Malnutrition Management in Tertiary Hospitals. Nutrients 2021, 13, 2635. https://doi.org/10.3390/nu13082635
Huysentruyt K, Brunet-Wood K, Bandsma R, Gramlich L, Fleming-Carroll B, Hotson B, Byers R, Lovelace H, Persad R, Kalnins D, et al. Canadian Nationwide Survey on Pediatric Malnutrition Management in Tertiary Hospitals. Nutrients. 2021; 13(8):2635. https://doi.org/10.3390/nu13082635
Chicago/Turabian StyleHuysentruyt, Koen, Kim Brunet-Wood, Robert Bandsma, Leah Gramlich, Bonnie Fleming-Carroll, Brenda Hotson, Rebecca Byers, Heather Lovelace, Rabin Persad, Daina Kalnins, and et al. 2021. "Canadian Nationwide Survey on Pediatric Malnutrition Management in Tertiary Hospitals" Nutrients 13, no. 8: 2635. https://doi.org/10.3390/nu13082635
APA StyleHuysentruyt, K., Brunet-Wood, K., Bandsma, R., Gramlich, L., Fleming-Carroll, B., Hotson, B., Byers, R., Lovelace, H., Persad, R., Kalnins, D., Martinez, A., Marchand, V., Vachon, M., Hulst, J. M., & on behalf of the Canadian Malnutrition Task Force—Pediatric Working Group. (2021). Canadian Nationwide Survey on Pediatric Malnutrition Management in Tertiary Hospitals. Nutrients, 13(8), 2635. https://doi.org/10.3390/nu13082635