
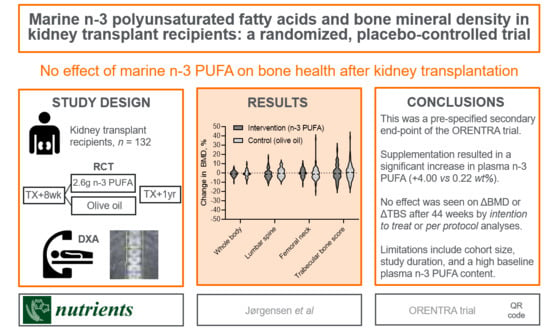
Marine n-3 Polyunsaturated Fatty Acids and Bone Mineral Density in Kidney Transplant Recipients: A Randomized, Placebo-Controlled Trial

 , , and
, , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Cohort
2.2. Immunosuppressive Protocol
2.3. Biochemical Analyses
2.4. Bone Density
2.5. Ethics
2.6. Statistics
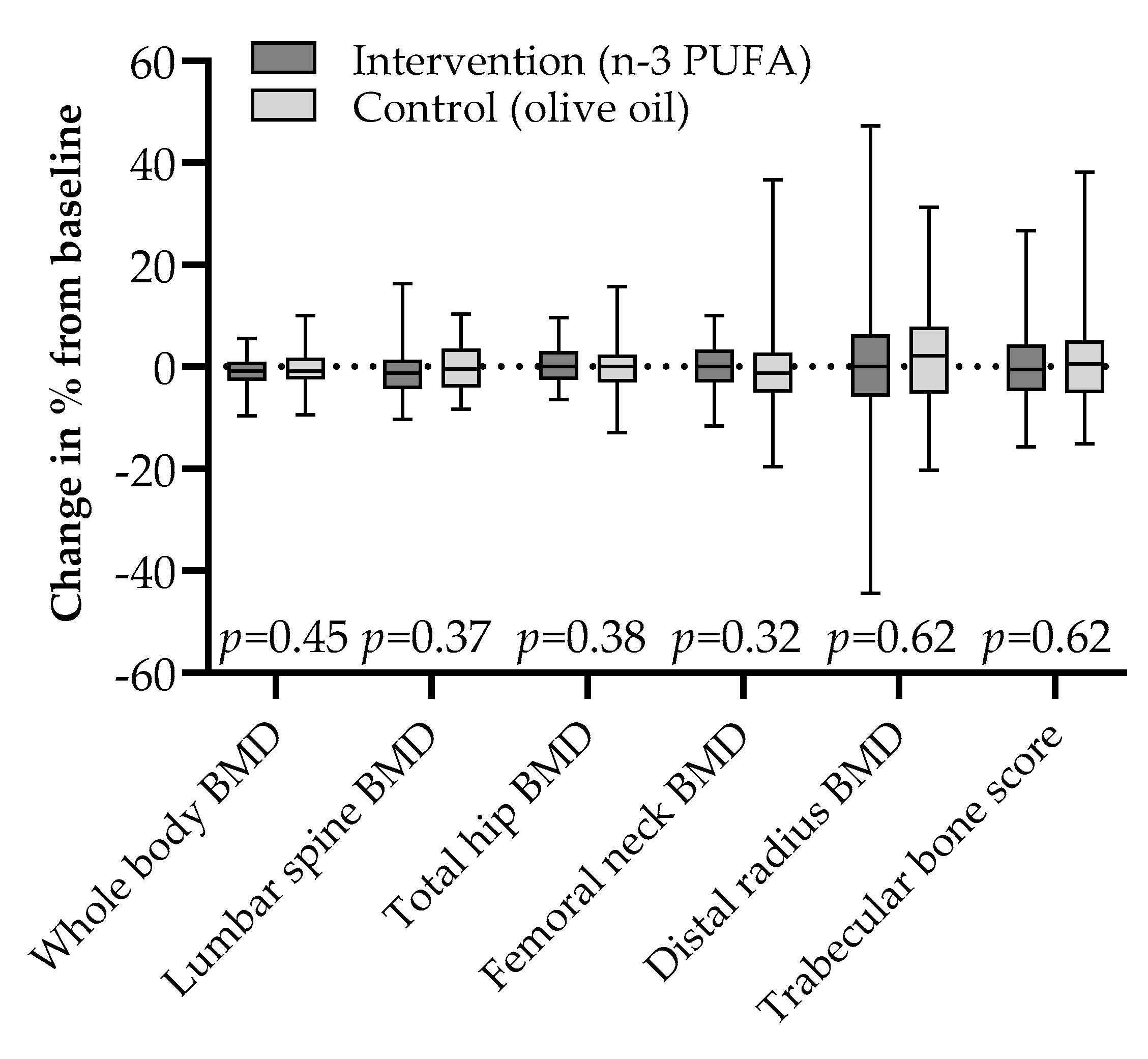
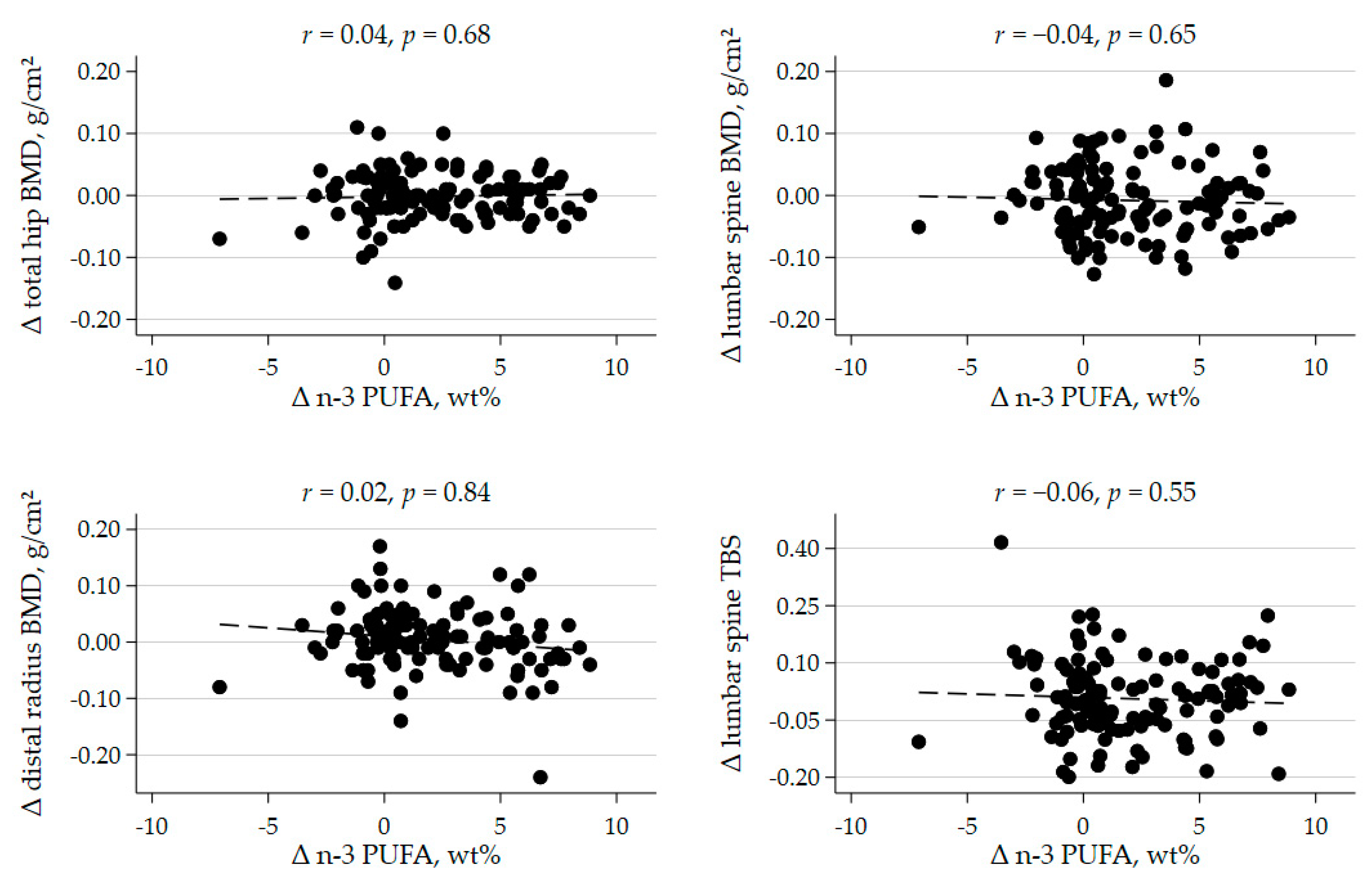
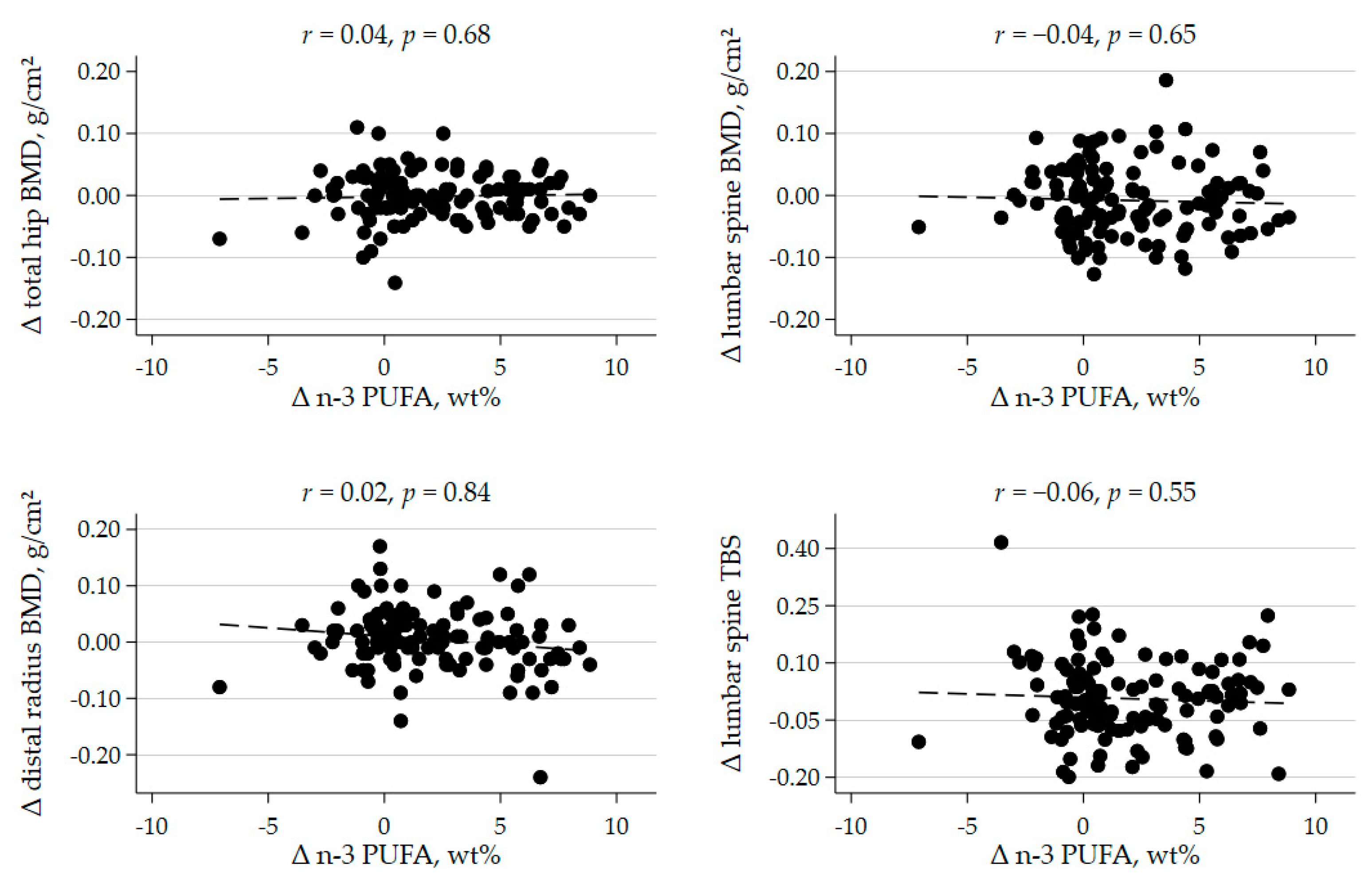
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hansen, D.; Olesen, J.B.; Gislason, G.; Abrahamsen, B.; Hommel, K. Risk of fracture in adults on renal replacement therapy: A Danish national cohort study. Nephrol. Dial. Transplant. 2016, 31, 1654–1662. [Google Scholar] [CrossRef]
- Vautour, L.M.; Melton, L.J.; Clarke, B.L.; Achenbach, S.J.; Oberg, A.L.; McCarthy, J.T. Long-term fracture risk following renal transplantation: A population-based study. Osteoporos. Int. 2004, 15, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Ramsey-Goldman, R.; Dunn, J.E.; Dunlop, D.D.; Stuart, F.P.; Abecassis, M.M.; Kaufman, D.B.; Langman, C.B.; Salinger, M.H.; Sprague, S.M. Increased Risk of Fracture in Patients Receiving Solid Organ Transplants. J. Bone Miner. Res. 1999, 14, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Kwan, J.T.C.; McCloskey, E.; McGee, G.; Thomas, G.; Johnson, D.; Wills, R.; Ogunremi, L.; Barron, J. Prevalence and Causes of Low Bone Density and Fractures in Kidney Transplant Patients. J. Bone Miner. Res. 2001, 16, 1863–1870. [Google Scholar] [CrossRef] [PubMed]
- Nikkel, L.E.; Hollenbeak, C.S.; Fox, E.J.; Uemura, T.; Ghahramani, N. Risk of Fractures After Renal Transplantation in the United States. Transplantation 2009, 87, 1846–1851. [Google Scholar] [CrossRef] [PubMed]
- Stehman-Breen, C.O.; Sherrard, D.J.; Alem, A.M.; Gillen, D.L.; Heckbert, S.R.; Wong, C.S.; Ball, A.; Weiss, N.S. Risk factors for hip fracture among patients with end-stage renal disease. Kidney Int. 2000, 58, 2200–2205. [Google Scholar] [CrossRef]
- Perrin, P.; Caillard, S.; Javier, R.M.; Braun, L.; Heibel, F.; Borni-Duval, C.; Muller, C.; Olagne, J.; Moulin, B. Persistent hyperparathyroidism is a major risk factor for fractures in the five years after kidney transplantation. Am. J. Transplant. 2013, 13, 2653–2663. [Google Scholar] [CrossRef]
- Nisbeth, U.; Lindh, E.; Ljunghall, S.; Backman, U.; Fellström, B. Increased Fracture Rate in Diabetes Mellitus And Females After Renal Transplantation. Transplantation 1999, 67, 1218–1222. [Google Scholar] [CrossRef]
- Nikkel, L.E.; Mohan, S.; Zhang, A.; McMahon, D.J.; Boutroy, S.; Dube, G.; Tanriover, B.; Cohen, D.; Ratner, L.; Hollenbeak, C.S.; et al. Reduced Fracture Risk With Early Corticosteroid Withdrawal After Kidney Transplant. Am. J. Transplant. 2012, 12, 649–659. [Google Scholar] [CrossRef] [Green Version]
- Kumar, N.G.; Contaifer, D.; Madurantakam, P.; Carbone, S.; Price, E.T.; Van Tassell, B.; Brophy, D.F.; Wijesinghe, D.S. Dietary Bioactive Fatty Acids as Modulators of Immune Function: Implications on Human Health. Nutriments 2019, 11, 2974. [Google Scholar] [CrossRef] [Green Version]
- Bao, M.; Zhang, K.; Wei, Y.; Hua, W.; Gao, Y.; Li, X.; Ye, L. Therapeutic potentials and modulatory mechanisms of fatty acids in bone. Cell Prolif. 2019, 53, e12735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coetzee, M.; Haag, M.; Joubert, A.; Kruger, M. Effects of arachidonic acid, docosahexaenoic acid and prostaglandin E2 on cell proliferation and morphology of MG-63 and MC3T3-E1 osteoblast-like cells. Prostaglandins Leukot. Essent. Fat. Acids 2007, 76, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Zwart, S.R.; Pierson, D.; Mehta, S.; Gonda, S.; Smith, S.M. Capacity of omega-3 fatty acids or eicosapentaenoic acid to counteract weightlessness-induced bone loss by inhibiting NF-kappaB activation: From cells to bed rest to astronauts. J. Bone Miner. Res. 2009, 25, 1049–1057. [Google Scholar] [CrossRef] [Green Version]
- Casado-Díaz, A.; Santiago-Mora, R.; Dorado, G.; Quesada-Gómez, J.M. The omega-6 arachidonic fatty acid, but not the omega-3 fatty acids, inhibits osteoblastogenesis and induces adipogenesis of human mesenchymal stem cells: Potential implication in osteoporosis. Osteoporos. Int. 2012, 24, 1647–1661. [Google Scholar] [CrossRef]
- Hogstrom, M.; Nordström, P.; Nordström, A. n−3 Fatty acids are positively associated with peak bone mineral density and bone accrual in healthy men: The NO2 Study. Am. J. Clin. Nutr. 2007, 85, 803–807. [Google Scholar] [CrossRef] [Green Version]
- Moon, H.-J.; Kim, T.-H.; Byun, D.-W.; Park, Y. Positive Correlation between Erythrocyte Levels of n–3 Polyunsaturated Fatty Acids and Bone Mass in Postmenopausal Korean Women with Osteoporosis. Ann. Nutr. Metab. 2012, 60, 146–153. [Google Scholar] [CrossRef]
- Harris, T.B.; Song, X.; Reinders, I.; Lang, T.F.; Garcia, E.M.; Siggeirsdottir, K.; Sigurdsson, S.; Gudnason, V.; Eiriksdottir, G.; Sigurdsson, G.; et al. Plasma phospholipid fatty acids and fish-oil consumption in relation to osteoporotic fracture risk in older adults: The Age, Gene/Environment Susceptibility Study. Am. J. Clin. Nutr. 2015, 101, 947–955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kruger, M.C.; Coetzer, H.; De Winter, R.; Gericke, G.; Van Papendorp, D.H. Calcium, gamma-linolenic acid and eicosapentaenoic acid supplementation in senile osteoporosis. Aging 1998, 10, 385–394. [Google Scholar] [CrossRef]
- Bassey, E.J.; Littlewood, J.J.; Rothwell, M.C.; Pye, D.W. Lack of effect of supplementation with essential fatty acids on bone mineral density in healthy pre- and postmenopausal women:two randomized controlled trials of Efacal® v. calcium alone. Br. J. Nutr. 2000, 83, 629–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baggio, B.; Budakovic, A.; Ferraro, A.; Checchetto, S.; Priante, G.; Musacchio, E.; Manzato, E.; Zaninotto, M.; Maresca, M.-C. Relationship between Plasma Phospholipid Polyunsaturated Fatty Acid Composition and Bone Disease in Renal Transplantation. Transplantation 2005, 80, 1349–1352. [Google Scholar] [CrossRef]
- Jørgensen, H.S.; Eide, I.A.; Hartmann, A.; Åsberg, A.; Christensen, J.H.; Schmidt, E.B.; Godang, K.; Bollerslev, J.; Svensson, M. Plasma n-3 Polyunsaturated Fatty Acids and Bone Mineral Density in Renal Transplant Recipients. J. Ren. Nutr. 2016, 26, 196–203. [Google Scholar] [CrossRef]
- Eide, I.A.; Reinholt, F.P.; Jenssen, T.; Hartmann, A.; Schmidt, E.B.; Åsberg, A.; Bergan, S.; Brabrand, K.; Svensson, M. Effects of marine n-3 fatty acid supplementation in renal transplantation: A randomized controlled trial. Am. J. Transplant. 2019, 19, 790–800. [Google Scholar] [CrossRef]
- Folch, J.; Lees, M.; Sloane-Stanley, G.H. A simple method for the isolation and purification of total lipides from animal tissues. J. Biol. Chem. 1957, 226, 497–509. [Google Scholar] [CrossRef]
- Burdge, G.C.; Wright, P.; Jones, A.E.; Wootton, S. A method for separation of phosphatidylcholine, triacylglycerol, non-esterified fatty acids and cholesterol esters from plasma by solid-phase extraction. Br. J. Nutr. 2000, 84, 781–787. [Google Scholar] [CrossRef] [Green Version]
- Gjesdal, C.G.; Aanderud, S.J.; Haga, H.-J.; Brun, J.G.; Tell, G.S. Femoral and whole-body bone mineral density in middle-aged and older Norwegian men and women: Suitability of the reference values. Osteoporos. Int. 2004, 15, 525–534. [Google Scholar] [CrossRef] [PubMed]
- Lau, B.Y.; Cohen, D.J.; Ward, W.E.; Ma, D.W. Investigating the Role of Polyunsaturated Fatty Acids in Bone Development Using Animal Models. Molecules 2013, 18, 14203–14227. [Google Scholar] [CrossRef] [Green Version]
- Haag, M.; Magada, O.N.; Claassen, N.; Böhmer, L.H.; Kruger, M.C. Omega-3 fatty acids modulate ATPases involved in duodenal Ca absorption. Prostaglandins Leukot. Essent. Fat. Acids 2003, 68, 423–429. [Google Scholar] [CrossRef]
- Coetzer, H.; Claassen, N.; van Papendorp, D.; Kruger, M. Calcium transport by isolated brush border and basolateral membrane vesicles: Role of essential fatty acid supplementation. Prostaglandins Leukot. Essent. Fat. Acids 1994, 50, 257–266. [Google Scholar] [CrossRef]
- McCloskey, E.V.; Odén, A.; Harvey, N.; Leslie, W.; Hans, D.; Johansson, H.; Kanis, J.A. Adjusting Fracture Probability by Trabecular Bone Score. Calcif. Tissue Int. 2015, 96, 500–509. [Google Scholar] [CrossRef] [PubMed]
- Orchard, T.S.; Ing, S.W.; Lu, B.; Belury, M.A.; Johnson, K.; Wactawski-Wende, J.; Jackson, R.D. The association of red blood cell n-3 and n-6 fatty acids with bone mineral density and hip fracture risk in the women’s health initiative. J. Bone Miner. Res. 2012, 28, 505–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farina, E.K.; Kiel, D.; Roubenoff, R.; Schaefer, E.J.; Cupples, L.A.; Tucker, K.L. Plasma phosphatidylcholine concentrations of polyunsaturated fatty acids are differentially associated with hip bone mineral density and hip fracture in older adults: The framingham osteoporosis study. J. Bone Miner. Res. 2012, 27, 1222–1230. [Google Scholar] [CrossRef] [Green Version]
- Abdelhamid, A.; the PUFAH Group; Hooper, L.; Sivakaran, R.; Hayhoe, R.P.G.; Welch, A. The Relationship Between Omega-3, Omega-6 and Total Polyunsaturated Fat and Musculoskeletal Health and Functional Status in Adults: A Systematic Review and Meta-analysis of RCTs. Calcif. Tissue Int. 2019, 105, 353–372. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.S.; Hill, C.L.; Lester, S.; Ruediger, C.D.; Battersby, R.; Jones, G.; Cleland, L.G.; March, L.M. Supplementation with omega-3 fish oil has no effect on bone mineral density in adults with knee osteoarthritis: A 2-year randomized controlled trial. Osteoporos. Int. 2015, 27, 1897–1905. [Google Scholar] [CrossRef]
- Evenepoel, P.; Claes, K.; Meijers, B.; Laurent, M.; Bammens, B.; Naesens, M.; Sprangers, B.; Cavalier, E.; Kuypers, D. Natural history of mineral metabolism, bone turnover and bone mineral density in de novo renal transplant recipients treated with a steroid minimization immunosuppressive protocol. Nephrol. Dial. Transplant. 2018, 35, 697–705. [Google Scholar] [CrossRef]
- Smerud, K.T.; Dolgos, S.; Olsen, I.C.; Åsberg, A.; Sagedal, S.; Reisaeter, A.V.; Midtvedt, K.; Pfeffer, P.; Ueland, T.; Godang, K.; et al. A 1-Year Randomized, Double-Blind, Placebo-Controlled Study of Intravenous Ibandronate on Bone Loss Following Renal Transplantation. Am. J. Transplant. 2012, 12, 3316–3325. [Google Scholar] [CrossRef]
- Bell, K.J.L.; Hayen, A.; Macaskill, P.; Irwig, L.; Craig, J.; Ensrud, K.; Bauer, D.C. Value of routine monitoring of bone mineral density after starting bisphosphonate treatment: Secondary analysis of trial data. BMJ 2009, 338, b2266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watts, N.B.; Lewiecki, E.M.; Bonnick, S.L.; Laster, A.J.; Binkley, N.; Blank, R.D.; Geusens, P.P.; Miller, P.D.; Petak, S.M.; Recker, R.R.; et al. Clinical Value of Monitoring BMD in Patients Treated with Bisphosphonates for Osteoporosis. J. Bone Miner. Res. 2009, 24, 1643–1646. [Google Scholar] [CrossRef] [PubMed]
- Kendler, D.L.; Compston, J.; Carey, J.J.; Wu, C.-H.; Ibrahim, A.; Lewiecki, E.M. Repeating Measurement of Bone Mineral Density when Monitoring with Dual-energy X-ray Absorptiometry: 2019 ISCD Official Position. J. Clin. Densitom. 2019, 22, 489–500. [Google Scholar] [CrossRef] [PubMed]
- Krohn, K.; Schwartz, E.N.; Chung, Y.-S.; Lewiecki, E.M. Dual-energy X-ray Absorptiometry Monitoring with Trabecular Bone Score: 2019 ISCD Official Position. J. Clin. Densitom. 2019, 22, 501–505. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Characteristic | All (n = 132) | Marine n-3 PUFA (n = 66) | Control (Olive Oil) (n = 66) |
|---|---|---|---|
| Age, years | 53 ± 14 | 53± 14 | 54 ± 14 |
| Women, % | 34 (26%) | 19 (29%) | 15 (23%) |
| Caucasian, % | 122 (92%) | 60 (91%) | 62 (94%) |
| Weight, kg | 80 ± 15 | 79 ± 15 | 81 ± 15 |
| Body mass index, kg/m² | 26.0 ± 3.9 | 25.7 ± 3.8 | 26.2 ± 4.0 |
| University degree, n (%) | 49 (37%) | 18 (30%) | 29 (44%) |
| Exercize ≥ 2 per week | 56 (42%) | 30 (45%) | 26 (39%) |
| Active smoker, % | 23 (17%) | 12 (18%) | 11 (17%) |
| Daily use of fish oil supplement, % | 19 (14%) | 8 (12%) | 11 (17%) |
| Dialysis pre-transplant, % | 90 (68%) | 45 (68%) | 45 (68%) |
| Living donor, % | 32 (24%) | 14 (21%) | 18 (27%) |
| HLA mismatches | |||
| None or 1 | 21 (16%) | 9 (14%) | 12 (18%) |
| 2 or 3 | 68 (51%) | 34 (51%) | 34 (51%) |
| ≥4 | 43 (33%) | 23 (35%) | 20 (30%) |
| eGFR, mL/min/1.73m² | 69 ± 21 | 71 ± 21 | 67 ± 22 |
| Total n-3 PUFA, wt% | 6.0 (4.7, 7.3) | 6.0 (4.6, 7.6) | 6.0 (4.8, 7.2) |
| Intact parathyroid hormone, ρmol/L | 11.1 (9.1, 16.5) | 10.9 (9.3, 16.4) | 11.5 (9.1, 16.7) |
| Calcium ion, mmol/L | 1.29 ± 0.07 | 1.30 ± 0.06 | 1.28 ± 0.06 |
| Phosphate, mmol/L | 0.84 ± 0.22 | 0.85 ± 0.23 | 0.86 ± 0.23 |
| Whole body T-score | −0.38 ± 1.27 | −0.40 ± 1.10 | −0.36 ± 1.45 |
| Lumbar spine T-score | −0.74 ± 1.44 | −0.73 ± 1.34 | −0.75 ± 1.55 |
| Total hip T-score | −1.42 ± 0.99 | −1.38 ± 0.86 | −1.46 ± 1.12 |
| Femoral neck T-score | −1.62 ± 1.05 | −1.66 ± 0.86 | −1.59 ± 1.23 |
| Distal radius T-score | −0.74 ± 1.93 | −0.92 ± 1.67 | −0.55 ± 2.17 |
| Lumbar spine TBS T-score | −2.35 ± 1.37 | −2.35 ± 1.37 | −2.34 ± 1.38 |
| Outcome Variable | n | Marine n-3 PUFA | n | Control (Olive Oil) | p |
|---|---|---|---|---|---|
| Fatty acids | |||||
| DHA + EPA, wt% | |||||
| ITT | 61 | 4.00 ± 2.68 | 65 | 0.22 ± 2.22 | <0.001 |
| PP | 50 | 4.44 ± 2.50 | 52 | 0.16 ± 2.28 | <0.001 |
| Bone density | |||||
| Whole body, g/cm² | |||||
| ITT | 61 | −0.009 ± 0.032 | 61 | −0.001 ± 0.080 | 0.45 |
| PP | 49 | −0.008 ± 0.033 | 50 | −0.009 ± 0.046 | 0.87 |
| Lumbar spine, g/cm² | |||||
| ITT | 61 | −0.014 ± 0.059 | 64 | −0.005 ± 0.052 | 0.37 |
| PP | 49 | −0.011 ± 0.062 | 51 | −0.003 ± 0.053 | 0.45 |
| Total hip, g/cm² | |||||
| ITT | 61 | 0.001 ± 0.031 | 62 | −0.005 ± 0.043 | 0.38 |
| PP | 49 | 0.000 ± 0.032 | 51 | −0.004 ± 0.042 | 0.53 |
| Femoral neck, g/cm² | |||||
| ITT | 60 | −0.000 ± 0.036 | 62 | −0.009 ± 0.061 | 0.32 |
| PP | 48 | 0.001 ± 0.037 | 51 | −0.009 ± 0.062 | 0.35 |
| Distal radius, g/cm² | |||||
| ITT | 61 | 0.002 ± 0.058 | 62 | 0.007 ± 0.049 | 0.62 |
| PP | 49 | −0.001 ± 0.057 | 51 | 0.004 ± 0.050 | 0.63 |
| Lumbar spine TBS | |||||
| ITT | 61 | 0.001 ± 0.096 | 64 | 0.009 ± 0.102 | 0.62 |
| PP | 49 | −0.004 ± 0.100 | 51 | 0.014 ± 0.104 | 0.38 |
| Biochemistry | |||||
| Intact PTH, ρmol/L | |||||
| ITT | 61 | −1.2 ± 5.3 | 66 | −2.0 ± 5.9 | 0.44 |
| PP | 49 | −1.1 ± 4.5 | 52 | −1.9 ± 5.7 | 0.41 |
| 25-OH Vit D, nmol/L | |||||
| ITT | 58 | 10.5 ± 3.6 | 58 | 6.74 ± 3.2 | 0.44 |
| PP | 53 | 8.06 ± 3.7 | 50 | 6.16 ± 3.5 | 0.71 |
| Calcium ion, mmol/L | |||||
| ITT | 61 | −0.01 ± 0.05 | 65 | 0.00 ± 0.06 | 0.47 |
| PP | 50 | −0.00 ± 0.05 | 51 | 0.00 ± 0.05 | 0.55 |
| Phosphate, mmol/L | |||||
| ITT | 62 | −0.15 ± 0.24 | 66 | 0.11 ± 0.23 | 0.45 |
| PP | 50 | 0.13 ± 0.24 | 52 | 0.13 ± 0.20 | 0.96 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jørgensen, H.S.; Eide, I.A.; Jenssen, T.; Åsberg, A.; Bollerslev, J.; Godang, K.; Hartmann, A.; Schmidt, E.B.; Svensson, M. Marine n-3 Polyunsaturated Fatty Acids and Bone Mineral Density in Kidney Transplant Recipients: A Randomized, Placebo-Controlled Trial. Nutrients 2021, 13, 2361. https://doi.org/10.3390/nu13072361
Jørgensen HS, Eide IA, Jenssen T, Åsberg A, Bollerslev J, Godang K, Hartmann A, Schmidt EB, Svensson M. Marine n-3 Polyunsaturated Fatty Acids and Bone Mineral Density in Kidney Transplant Recipients: A Randomized, Placebo-Controlled Trial. Nutrients. 2021; 13(7):2361. https://doi.org/10.3390/nu13072361
Chicago/Turabian StyleJørgensen, Hanne Skou, Ivar Anders Eide, Trond Jenssen, Anders Åsberg, Jens Bollerslev, Kristin Godang, Anders Hartmann, Erik Berg Schmidt, and My Svensson. 2021. "Marine n-3 Polyunsaturated Fatty Acids and Bone Mineral Density in Kidney Transplant Recipients: A Randomized, Placebo-Controlled Trial" Nutrients 13, no. 7: 2361. https://doi.org/10.3390/nu13072361
APA StyleJørgensen, H. S., Eide, I. A., Jenssen, T., Åsberg, A., Bollerslev, J., Godang, K., Hartmann, A., Schmidt, E. B., & Svensson, M. (2021). Marine n-3 Polyunsaturated Fatty Acids and Bone Mineral Density in Kidney Transplant Recipients: A Randomized, Placebo-Controlled Trial. Nutrients, 13(7), 2361. https://doi.org/10.3390/nu13072361