
Intake of Fish and Marine n-3 Polyunsaturated Fatty Acids and Risk of Cardiovascular Disease Mortality: A Meta-Analysis of Prospective Cohort Studies

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Statistical Analyses
3. Results
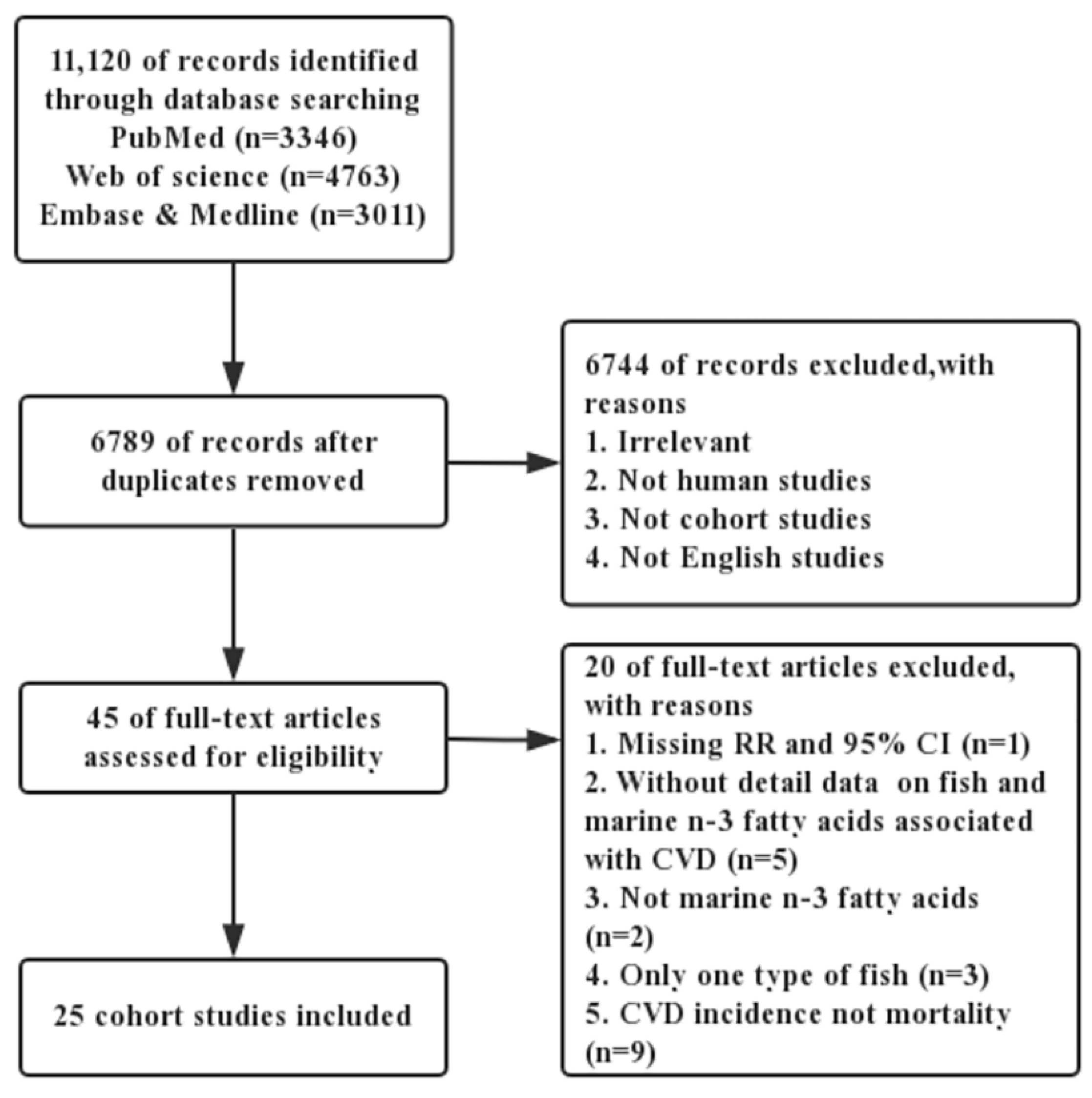
3.1. Literature Search and Study Characteristics
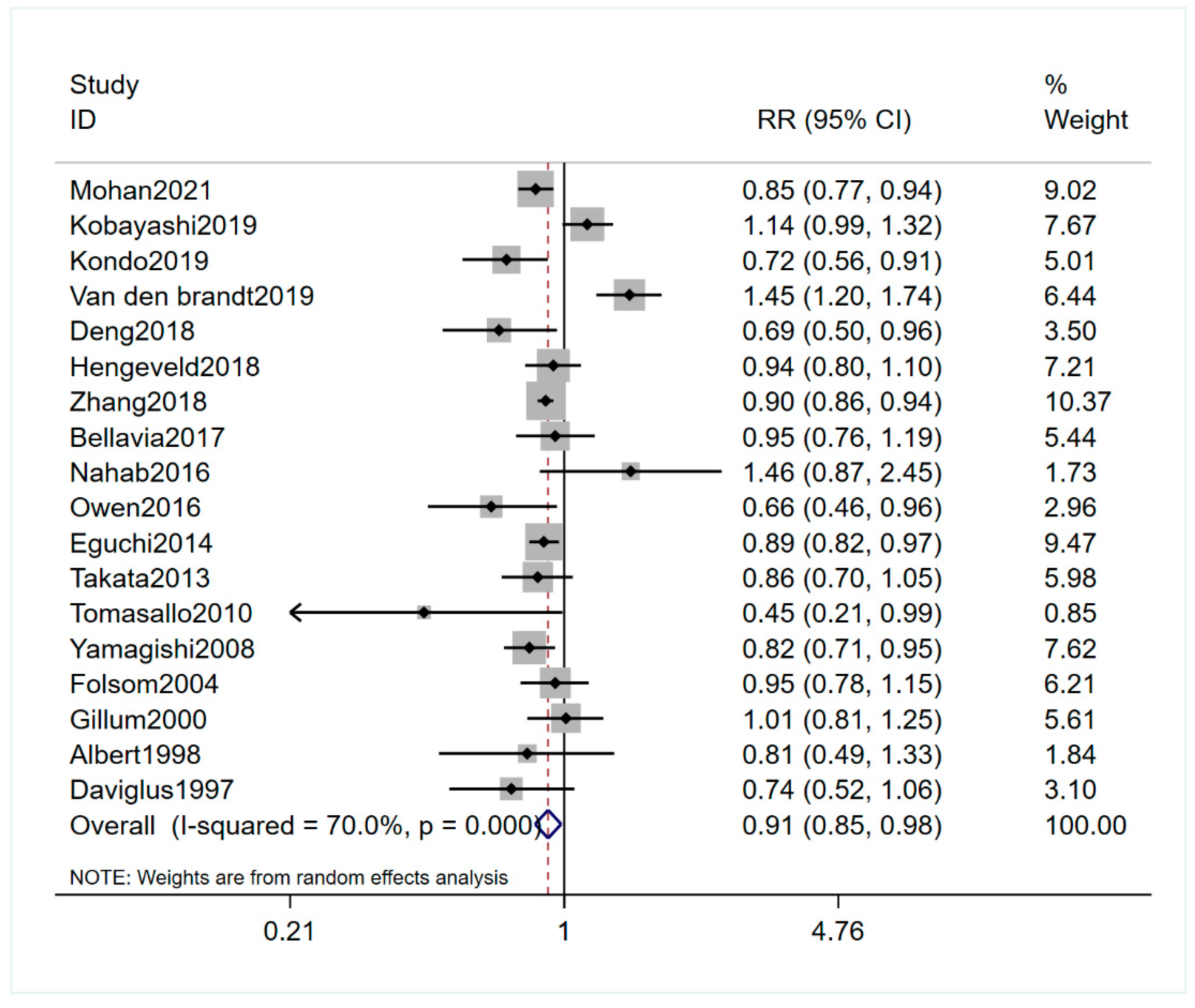
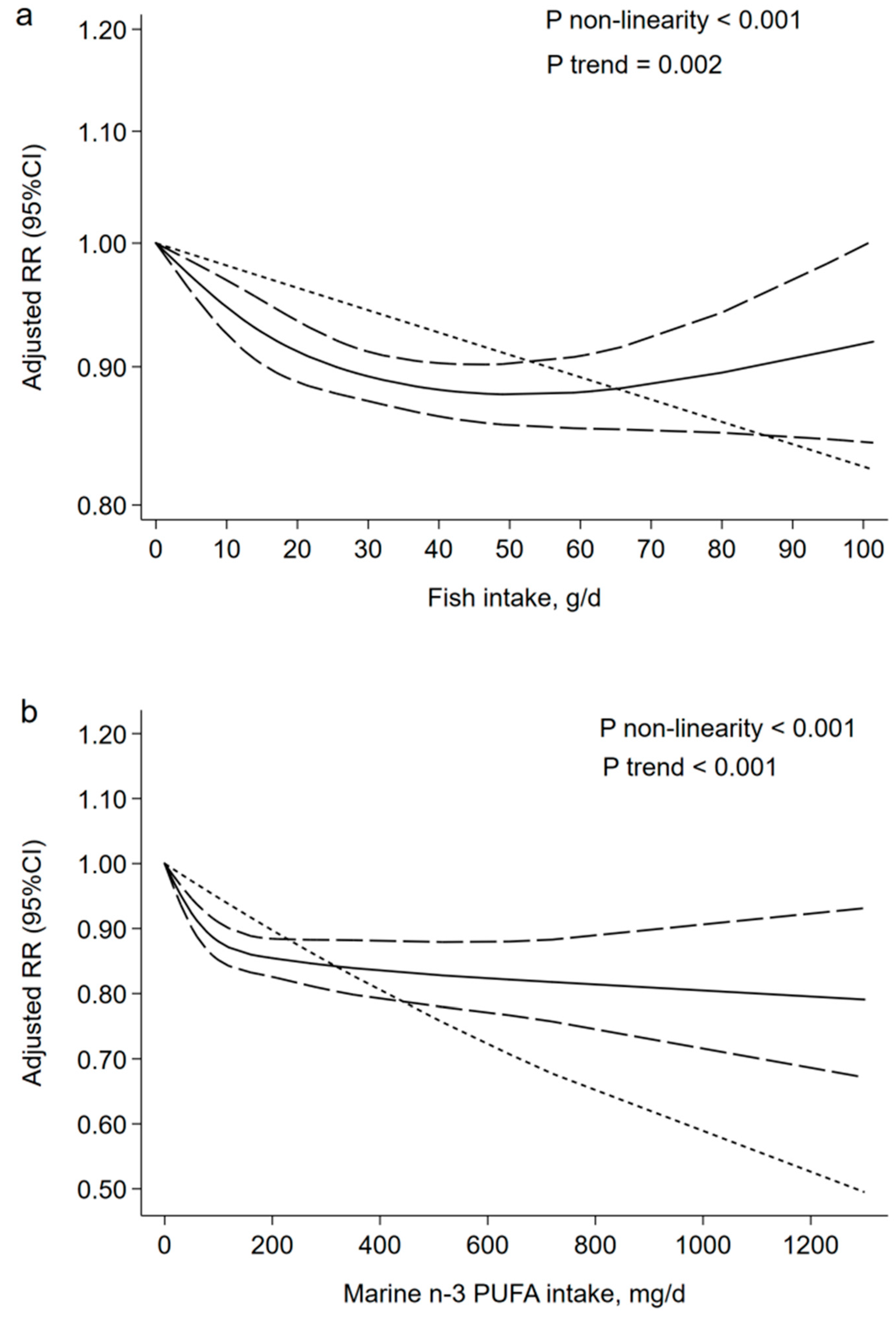
3.2. Fish Consumption and Cardiovascular Disease Mortality Risk
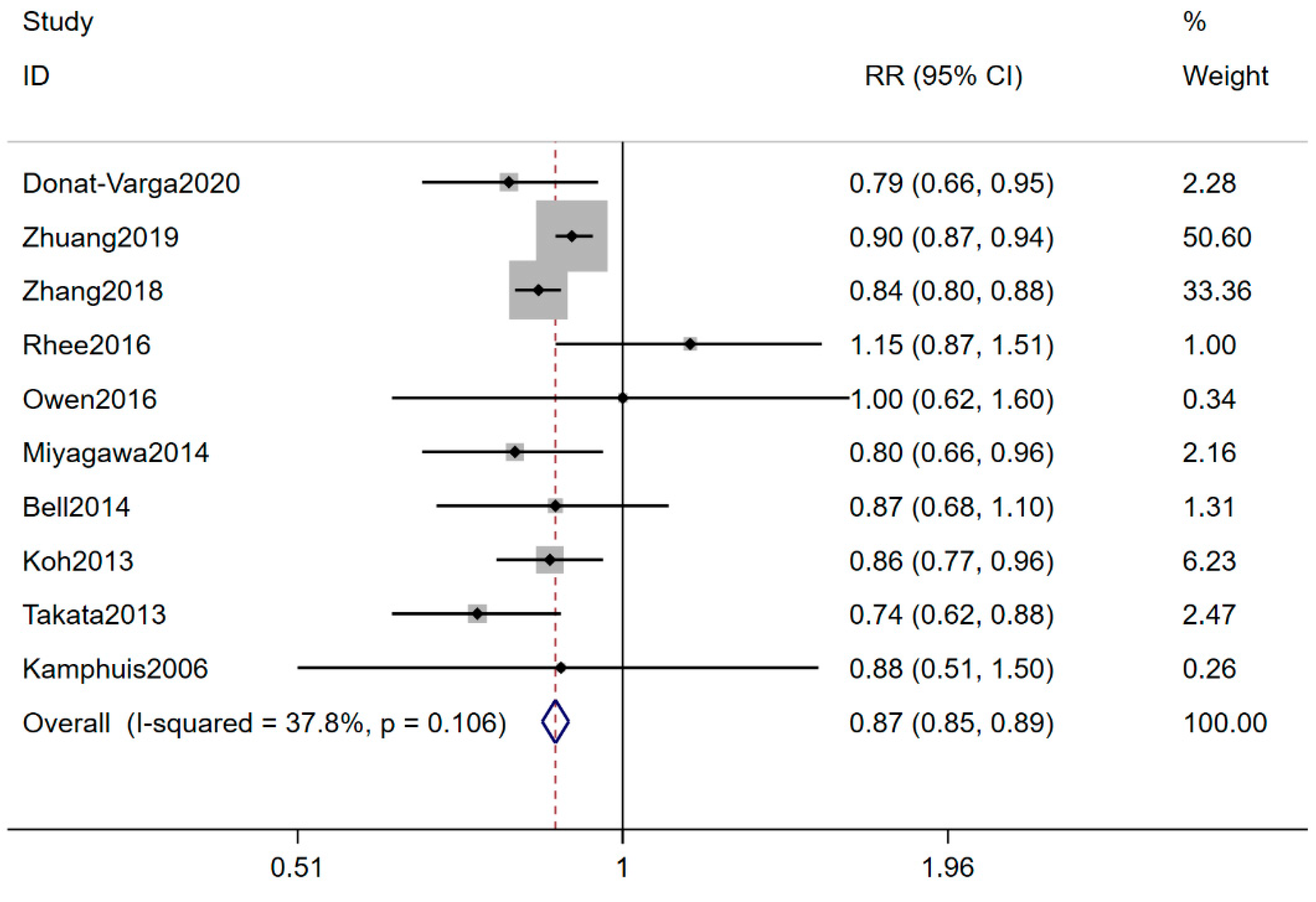
3.3. Marine n-3 PUFA and Cardiovascular Disease Mortality Risk
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Mortality, G.B.D.; Causes of Death, C. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [Green Version]
- Rosato, V.; Temple, N.J.; La Vecchia, C.; Castellan, G.; Tavani, A.; Guercio, V. Mediterranean diet and cardiovascular disease: A systematic review and meta-analysis of observational studies. Eur. J. Nutr. 2019, 58, 173–191. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Xiong, K.; Xu, L.; Zhang, C.; Zhao, S.; Liu, Y.; Ma, A. Dietary Intake of Vegetables and Cooking Oil Was Associated with Drug-Induced Liver Injury During Tuberculosis Treatment: A Preliminary Cohort Study. Front. Nutr. 2021, 8, 652311. [Google Scholar] [CrossRef] [PubMed]
- Xiong, K.; Zhou, L.; Wang, J.; Ma, A.; Fang, D.; Xiong, L.; Sun, Q. Construction of food-grade pH-sensitive nanoparticles for delivering functional food ingredients. Trends Food Sci. Technol. 2020, 96, 102–113. [Google Scholar] [CrossRef]
- Denissen, K.F.M.; Heil, S.G.; Eussen, S.; Heeskens, J.P.J.; Thijs, C.; Mommers, M.; Smits, L.J.M.; van Dongen, M.; Dagnelie, P.C. Intakes of Vitamin B-12 from Dairy Food, Meat, and Fish and Shellfish Are Independently and Positively Associated with Vitamin B-12 Biomarker Status in Pregnant Dutch Women. J. Nutr. 2019, 149, 131–138. [Google Scholar] [CrossRef]
- Bergqvist, C.; Ezzedine, K. Vitamin D and the skin: What should a dermatologist know? G. Ital. Dermatol. Venereol. 2019, 154, 669–680. [Google Scholar] [CrossRef]
- Hustad, K.S.; Rundblad, A.; Ottestad, I.; Christensen, J.J.; Holven, K.B.; Ulven, S.M. Comprehensive lipid and metabolite profiling in healthy adults with low and high consumption of fatty fish: A cross-sectional study. Br. J. Nutr. 2020, 1–23. [Google Scholar] [CrossRef]
- Asher, A.; Tintle, N.L.; Myers, M.; Lockshon, L.; Bacareza, H.; Harris, W.S. Blood omega-3 fatty acids and death from COVID-19: A pilot study. Prostaglandins Leukot. Essent. Fat. Acids 2021, 166, 102250. [Google Scholar] [CrossRef]
- O’Keefe, J.H., Jr.; Abuissa, H.; Sastre, A.; Steinhaus, D.M.; Harris, W.S. Effects of omega-3 fatty acids on resting heart rate, heart rate recovery after exercise, and heart rate variability in men with healed myocardial infarctions and depressed ejection fractions. Am. J. Cardiol. 2006, 97, 1127–1130. [Google Scholar] [CrossRef]
- Jayedi, A.; Shab-Bidar, S. Fish Consumption and the Risk of Chronic Disease: An Umbrella Review of Meta-Analyses of Prospective Cohort Studies. Adv. Nutr. 2020. [Google Scholar] [CrossRef]
- Rhee, J.J.; Kim, E.; Buring, J.E.; Kurth, T. Fish Consumption, Omega-3 Fatty Acids, and Risk of Cardiovascular Disease. Am. J. Prev. Med. 2017, 52, 10–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jayedi, A.; Shab-Bidar, S.; Eimeri, S.; Djafarian, K. Fish consumption and risk of all-cause and cardiovascular mortality: A dose-response meta-analysis of prospective observational studies. Public Health Nutr. 2018, 21, 1297–1306. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, M.; Sasazuki, S.; Shimazu, T.; Sawada, N.; Yamaji, T.; Iwasaki, M.; Mizoue, T.; Tsugane, S. Association of dietary diversity with total mortality and major causes of mortality in the Japanese population: JPHC study. Eur. J. Clin. Nutr. 2020, 74, 54–66. [Google Scholar] [CrossRef] [PubMed]
- Deng, A.; Pattanaik, S.; Bhattacharya, A.; Yin, J.; Ross, L.; Liu, C.; Zhang, J. Fish consumption is associated with a decreased risk of death among adults with diabetes: 18-year follow-up of a national cohort. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 1012–1020. [Google Scholar] [CrossRef]
- Kondo, K.; Miura, K.; Tanaka-Mizuno, S.; Kadota, A.; Arima, H.; Okuda, N.; Fujiyoshi, A.; Miyagawa, N.; Yoshita, K.; Okamura, T.; et al. Cardiovascular Risk Assessment Chart by Dietary Factors in Japan—NIPPON DATA80. Circ. J. 2019, 83, 1254–1260. [Google Scholar] [CrossRef] [Green Version]
- van den Brandt, P.A. Red meat, processed meat, and other dietary protein sources and risk of overall and cause-specific mortality in The Netherlands Cohort Study. Eur. J. Epidemiol. 2019, 34, 351–369. [Google Scholar] [CrossRef] [Green Version]
- Hengeveld, L.M.; Praagman, J.; Beulens, J.W.J.; Brouwer, I.A.; van der Schouw, Y.T.; Sluijs, I. Fish consumption and risk of stroke, coronary heart disease, and cardiovascular mortality in a Dutch population with low fish intake. Eur. J. Clin. Nutr. 2018, 72, 942–950. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhuang, P.; He, W.; Chen, J.N.; Wang, W.Q.; Freedman, N.D.; Abnet, C.C.; Wang, J.B.; Jiao, J.J. Association of fish and long-chain omega-3 fatty acids intakes with total and cause-specific mortality: Prospective analysis of 421 309 individuals. J. Intern. Med. 2018, 284, 399–417. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Orsini, N.; Bellocco, R.; Greenland, S. Generalized least squares for trend estimation of summarized dose–response data. STATA J. 2016, 6, 40–57. [Google Scholar] [CrossRef] [Green Version]
- Greenland, S.; Longnecker, M.P. Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. Am. J. Epidemiol. 1992, 135, 1301–1309. [Google Scholar] [CrossRef]
- Wang, X.; Ouyang, Y.; Liu, J.; Zhu, M.; Zhao, G.; Bao, W.; Hu, F.B. Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: Systematic review and dose-response meta-analysis of prospective cohort studies. BMJ 2014, 349, g4490. [Google Scholar] [CrossRef] [Green Version]
- Bellavia, A.; Larsson, S.C.; Wolk, A. Fish consumption and all-cause mortality in a cohort of Swedish men and women. J. Intern. Med. 2017, 281, 86–95. [Google Scholar] [CrossRef] [Green Version]
- Nahab, F.; Pearson, K.; Frankel, M.R.; Ard, J.; Safford, M.M.; Kleindorfer, D.; Howard, V.J.; Judd, S. Dietary fried fish intake increases risk of CVD: The REasons for Geographic and Racial Differences in Stroke (REGARDS) study. Public Health Nutr. 2016, 19, 3327–3336. [Google Scholar] [CrossRef] [Green Version]
- Owen, A.J.; Magliano, D.J.; O’Dea, K.; Barr, E.L.; Shaw, J.E. Polyunsaturated fatty acid intake and risk of cardiovascular mortality in a low fish-consuming population: A prospective cohort analysis. Eur. J. Nutr. 2016, 55, 1605–1613. [Google Scholar] [CrossRef]
- Eguchi, E.; Iso, H.; Tanabe, N.; Yatsuya, H.; Tamakoshi, A. Is the association between healthy lifestyle behaviors and cardiovascular mortality modified by overweight status? The Japan Collaborative Cohort Study. Prev. Med. 2014, 62, 142–147. [Google Scholar] [CrossRef]
- Takata, Y.; Zhang, X.; Li, H.; Gao, Y.T.; Yang, G.; Gao, J.; Cai, H.; Xiang, Y.B.; Zheng, W.; Shu, X.O. Fish intake and risks of total and cause-specific mortality in 2 population-based cohort studies of 134,296 men and women. Am. J. Epidemiol. 2013, 178, 46–57. [Google Scholar] [CrossRef] [Green Version]
- Tomasallo, C.; Anderson, H.; Haughwout, M.; Imm, P.; Knobeloch, L. Mortality among frequent consumers of Great Lakes sport fish. Environ. Res. 2010, 110, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Yamagishi, K.; Iso, H.; Date, C.; Fukui, M.; Wakai, K.; Kikuchi, S.; Inaba, Y.; Tanabe, N.; Tamakoshi, A.; Grp, J.S. Fish, omega-3 polyunsaturated fatty acids, and mortality from cardiovascular diseases in a nationwide community-based cohort of Japanese men and women—The JACC (Japan Collaborative Cohort Study for Evaluation of Cancer Risk) study. J. Am. Coll. Cardiol. 2008, 52, 988–996. [Google Scholar] [CrossRef] [Green Version]
- Folsom, A.R.; Demissie, Z. Fish intake, marine omega-3 fatty acids, and mortality in a cohort of postmenopausal women. Am. J. Epidemiol. 2004, 160, 1005–1010. [Google Scholar] [CrossRef]
- Gillum, R.F.; Mussolino, M.; Madans, J.H. The relation between fish consumption, death from all causes, and incidence of coronary heart disease. the NHANES I Epidemiologic Follow-up Study. J. Clin. Epidemiol. 2000, 53, 237–244. [Google Scholar] [CrossRef]
- Albert, C.M.; Hennekens, C.H.; O’Donnell, C.J.; Ajani, U.A.; Carey, V.J.; Willett, W.C.; Ruskin, J.N.; Manson, J.E. Fish consumption and risk of sudden cardiac death. J. Am. Med. Assoc. 1998, 279, 23–28. [Google Scholar] [CrossRef]
- Daviglus, M.L.; Stamler, J.; Orencia, A.J.; Dyer, A.R.; Liu, K.; Greenland, P.; Walsh, M.K.; Morris, D.; Shekelle, R.B. Fish consumption and the 30-year risk of fatal myocardial infarction. N. Engl. J. Med. 1997, 336, 1046–1053. [Google Scholar] [CrossRef]
- Donat-Vargas, C.; Bellavia, A.; Berglund, M.; Glynn, A.; Wolk, A.; Akesson, A. Cardiovascular and cancer mortality in relation to dietary polychlorinated biphenyls and marine polyunsaturated fatty acids: A nutritional-toxicological aspect of fish consumption. J. Intern. Med. 2020, 287, 197–209. [Google Scholar] [CrossRef] [Green Version]
- Zhuang, P.; Zhang, Y.; He, W.; Chen, X.; Chen, J.; He, L.; Mao, L.; Wu, F.; Jiao, J. Dietary Fats in Relation to Total and Cause-Specific Mortality in a Prospective Cohort of 521 120 Individuals with 16 Years of Follow-Up. Circ. Res. 2019, 124, 757–768. [Google Scholar] [CrossRef]
- Miyagawa, N.; Miura, K.; Okuda, N.; Kadowaki, T.; Takashima, N.; Nagasawa, S.Y.; Nakamura, Y.; Matsumura, Y.; Hozawa, A.; Fujiyoshi, A.; et al. Long-chain n-3 polyunsaturated fatty acids intake and cardiovascular disease mortality risk in Japanese: A 24-year follow-up of NIPPON DATA80. Atherosclerosis 2014, 232, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Bell, G.A.; Kantor, E.D.; Lampe, J.W.; Kristal, A.R.; Heckbert, S.R.; White, E. Intake of long-chain omega-3 fatty acids from diet and supplements in relation to mortality. Am. J. Epidemiol. 2014, 179, 710–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koh, A.S.; Pan, A.; Wang, R.; Odegaard, A.O.; Pereira, M.A.; Yuan, J.M.; Koh, W.P. The association between dietary omega-3 fatty acids and cardiovascular death: The Singapore Chinese Health Study. Eur. J. Prev. Cardiol. 2015, 22, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Kamphuis, M.H.; Geerlings, M.I.; Tijhuis, M.A.; Kalmijn, S.; Grobbee, D.E.; Kromhout, D. Depression and cardiovascular mortality: A role for n-3 fatty acids? Am. J. Clin. Nutr. 2006, 84, 1513–1517. [Google Scholar] [CrossRef] [Green Version]
- Mohan, D.; Mente, A.; Dehghan, M.; Rangarajan, S.; O’Donnell, M.; Hu, W.; Dagenais, G.; Wielgosz, A.; Lear, S.; Wei, L.; et al. Associations of Fish Consumption with Risk of Cardiovascular Disease and Mortality Among Individuals with or Without Vascular Disease From 58 Countries. JAMA Intern. Med. 2021, 181, 631–649. [Google Scholar] [CrossRef]
- Bechthold, A.; Boeing, H.; Schwedhelm, C.; Hoffmann, G.; Knuppel, S.; Iqbal, K.; De Henauw, S.; Michels, N.; Devleesschauwer, B.; Schlesinger, S.; et al. Food groups and risk of coronary heart disease, stroke and heart failure: A systematic review and dose-response meta-analysis of prospective studies. Crit. Rev. Food Sci. Nutr. 2019, 59, 1071–1090. [Google Scholar] [CrossRef] [Green Version]
- Kuhn, T.; Teucher, B.; Kaaks, R.; Boeing, H.; Weikert, C.; Buijsse, B. Fish consumption and the risk of myocardial infarction and stroke in the German arm of the European Prospective Investigation into Cancer and Nutrition (EPIC-Germany). Br. J. Nutr. 2013, 110, 1118–1125. [Google Scholar] [CrossRef] [Green Version]
- Myint, P.K.; Welch, A.A.; Bingham, S.A.; Luben, R.N.; Wareham, N.J.; Day, N.E.; Khaw, K.T. Habitual fish consumption and risk of incident stroke: The European Prospective Investigation into Cancer (EPIC)-Norfolk prospective population study. Public Health Nutr. 2006, 9, 882–888. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Liu, B.; Snetselaar, L.G.; Robinson, J.G.; Wallace, R.B.; Peterson, L.L.; Bao, W. Association of fried food consumption with all cause, cardiovascular, and cancer mortality: Prospective cohort study. BMJ 2019, 364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valenzuela, C.A.; Baker, E.J.; Miles, E.A.; Calder, P.C. Eighteencarbon trans fatty acids and inflammation in the context of atherosclerosis. Prog. Lipid Res. 2019, 76, 101009. [Google Scholar] [CrossRef]
- He, F.J.; MacGregor, G.A. Role of salt intake in prevention of cardiovascular disease: Controversies and challenges. Nat. Rev. Cardiol. 2018, 15, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Lastra, G.; Dhuper, S.; Johnson, M.S.; Sowers, J.R. Salt, aldosterone, and insulin resistance: Impact on the cardiovascular system. Nat. Rev. Cardiol. 2010, 7, 577–584. [Google Scholar] [CrossRef]
- VKM. Benefit-Risk Assessment of Fish and Fish Products in the Norwegian Diet—An Update. Scientific Opinion of the Scientific Steering Committee. VKM Report 15. Oslo, Norway, 2014; 293p, ISBN 978-82-8259-159-1. Available online: www.vkm.no (accessed on 25 April 2021).
- Zhang, J.; Wang, C.; Li, L.; Man, Q.; Meng, L.; Song, P.; Froyland, L.; Du, Z.Y. Dietary inclusion of salmon, herring and pompano as oily fish reduces CVD risk markers in dyslipidaemic middle-aged and elderly Chinese women. Br. J. Nutr. 2012, 108, 1455–1465. [Google Scholar] [CrossRef] [Green Version]
- Torris, C.; Smastuen, M.C.; Molin, M. Nutrients in Fish and Possible Associations with Cardiovascular Disease Risk Factors in Metabolic Syndrome. Nutrients 2018, 10, 952. [Google Scholar] [CrossRef] [Green Version]
- Hu, F.B.; Cho, E.; Rexrode, K.M.; Albert, C.M.; Manson, J.E. Fish and long-chain omega-3 fatty acid intake and risk of coronary heart disease and total mortality in diabetic women. Circulation 2003, 107, 1852–1857. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Shara, N.M.; Lee, E.T.; Devereux, R.; Calhoun, D.; de Simone, G.; Umans, J.G.; Howard, B.V. Hemoglobin A1c, fasting glucose, and cardiovascular risk in a population with high prevalence of diabetes: The strong heart study. Diabetes Care 2011, 34, 1952–1958. [Google Scholar] [CrossRef] [Green Version]
- Oh, D.Y.; Talukdar, S.; Bae, E.J.; Imamura, T.; Morinaga, H.; Fan, W.; Li, P.; Lu, W.J.; Watkins, S.M.; Olefsky, J.M. GPR120 is an omega-3 fatty acid receptor mediating potent anti-inflammatory and insulin-sensitizing effects. Cell 2010, 142, 687–698. [Google Scholar] [CrossRef] [Green Version]
- Kromhout, D.; Geleijnse, J.M.; de Goede, J.; Oude Griep, L.M.; Mulder, B.J.; de Boer, M.J.; Deckers, J.W.; Boersma, E.; Zock, P.L.; Giltay, E.J. n-3 fatty acids, ventricular arrhythmia-related events, and fatal myocardial infarction in postmyocardial infarction patients with diabetes. Diabetes Care 2011, 34, 2515–2520. [Google Scholar] [CrossRef] [Green Version]
- Bernasconi, A.A.; Lavie, C.J.; Milani, R.V.; Laukkanen, J.A. Omega-3 Benefits Remain Strong Post-STRENGTH. Mayo Clin. Proc. 2021, 96, 1371–1372. [Google Scholar] [CrossRef] [PubMed]
- Gammelmark, A.; Nielsen, M.S.; Bork, C.S.; Lundbye-Christensen, S.; Tjonneland, A.; Overvad, K.; Schmidt, E.B. Association of fish consumption and dietary intake of marine n-3 PUFA with myocardial infarction in a prospective Danish cohort study. Br. J. Nutr. 2016, 116, 167–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torris, C.; Molin, M.; Smastuen, M.C. Lean Fish Consumption Is Associated with Beneficial Changes in the Metabolic Syndrome Components: A 13-Year Follow-Up Study from the Norwegian Tromso Study. Nutrients 2017, 9, 247. [Google Scholar] [CrossRef] [Green Version]
- Jakobsen, M.U.; Due, K.M.; Dethlefsen, C.; Halkjaer, J.; Holst, C.; Forouhi, N.G.; Tjonneland, A.; Boeing, H.; Buijsse, B.; Palli, D.; et al. Fish consumption does not prevent increase in waist circumference in European women and men. Br. J. Nutr. 2012, 108, 924–931. [Google Scholar] [CrossRef] [Green Version]
- Bernasconi, A.A.; Wiest, M.M.; Lavie, C.J.; Milani, R.V.; Laukkanen, J.A. Effect of Omega-3 Dosage on Cardiovascular Outcomes: An Updated Meta-Analysis and Meta-Regression of Interventional Trials. Mayo Clin. Proc. 2021, 96, 304–313. [Google Scholar] [CrossRef]
- Okada, L.; Oliveira, C.P.; Stefano, J.T.; Nogueira, M.A.; Silva, I.; Cordeiro, F.B.; Alves, V.A.F.; Torrinhas, R.S.; Carrilho, F.J.; Puri, P.; et al. Omega-3 PUFA modulate lipogenesis, ER stress, and mitochondrial dysfunction markers in NASH—Proteomic and lipidomic insight. Clin. Nutr. 2018, 37, 1474–1484. [Google Scholar] [CrossRef]
- Harris, W.S.; Tintle, N.L.; Imamura, F.; Qian, F.; Korat, A.V.A.; Marklund, M.; Djousse, L.; Bassett, J.K.; Carmichael, P.H.; Chen, Y.Y.; et al. Blood n-3 fatty acid levels and total and cause-specific mortality from 17 prospective studies. Nat. Commun 2021, 12, 2329. [Google Scholar] [CrossRef]
- Rundblad, A.; Holven, K.B.; Bruheim, I.; Myhrstad, M.C.; Ulven, S.M. Effects of krill oil and lean and fatty fish on cardiovascular risk markers: A randomised controlled trial. J. Nutr. Sci. 2018, 7, e3. [Google Scholar] [CrossRef] [Green Version]
- Kromhout, D.; Giltay, E.J.; Geleijnse, J.M.; Alpha Omega Trial, G. n-3 fatty acids and cardiovascular events after myocardial infarction. N. Engl. J. Med. 2010, 363, 2015–2026. [Google Scholar] [CrossRef]
- Roger, V.L.; Weston, S.A.; Gerber, Y.; Killian, J.M.; Dunlay, S.M.; Jaffe, A.S.; Bell, M.R.; Kors, J.; Yawn, B.P.; Jacobsen, S.J. Trends in incidence, severity, and outcome of hospitalized myocardial infarction. Circulation 2010, 121, 863–869. [Google Scholar] [CrossRef]
- Elagizi, A.; Lavie, C.J.; O’Keefe, E.; Marshall, K.; O’Keefe, J.H.; Milani, R.V. An Update on Omega-3 Polyunsaturated Fatty Acids and Cardiovascular Health. Nutrients 2021, 13, 204. [Google Scholar] [CrossRef] [PubMed]
- Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: Results of the GISSI-Prevenzione trial. Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto miocardico. Lancet 1999, 354, 447–455. [CrossRef]
- Rauch, B.; Schiele, R.; Schneider, S.; Diller, F.; Victor, N.; Gohlke, H.; Gottwik, M.; Steinbeck, G.; Del Castillo, U.; Sack, R.; et al. OMEGA, a randomized, placebo-controlled trial to test the effect of highly purified omega-3 fatty acids on top of modern guideline-adjusted therapy after myocardial infarction. Circulation 2010, 122, 2152–2159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Einvik, G.; Klemsdal, T.O.; Sandvik, L.; Hjerkinn, E.M. A randomized clinical trial on n-3 polyunsaturated fatty acids supplementation and all-cause mortality in elderly men at high cardiovascular risk. Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 588–592. [Google Scholar] [CrossRef]
- Samieri, C.; Lorrain, S.; Buaud, B.; Vaysse, C.; Berr, C.; Peuchant, E.; Cunnane, S.C.; Barberger-Gateau, P. Relationship between diet and plasma long-chain n-3 PUFAs in older people: Impact of apolipoprotein E genotype. J. Lipid Res. 2013, 54, 2559–2567. [Google Scholar] [CrossRef] [Green Version]
- Hautero, U.; Poussa, T.; Laitinen, K. Simple dietary criteria to improve serum n-3 fatty acid levels of mothers and their infants. Public Health Nutr. 2017, 20, 534–541. [Google Scholar] [CrossRef] [Green Version]
- Mozaffarian, D.; Wu, J.H. Omega-3 fatty acids and cardiovascular disease: Effects on risk factors, molecular pathways, and clinical events. J. Am. Coll. Cardiol. 2011, 58, 2047–2067. [Google Scholar] [CrossRef] [Green Version]
- Bang, H.Y.; Park, S.A.; Saeidi, S.; Na, H.K.; Surh, Y.J. Docosahexaenoic Acid Induces Expression of Heme Oxygenase-1 and NAD(P)H:quinone Oxidoreductase through Activation of Nrf2 in Human Mammary Epithelial Cells. Molecules 2017, 22, 969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, W.; Ding, Y.; Kong, W.; Li, T.; Chen, H. Docosahexaenoic Acid (DHA) Provides Neuroprotection in Traumatic Brain Injury Models via Activating Nrf2-ARE Signaling. Inflammation 2018, 41, 1182–1193. [Google Scholar] [CrossRef] [PubMed]
- Clarke, S.D. Polyunsaturated fatty acid regulation of gene transcription: A molecular mechanism to improve the metabolic syndrome. J. Nutr. 2001, 131, 1129–1132. [Google Scholar] [CrossRef] [Green Version]
- Jump, D.B. Fatty acid regulation of hepatic lipid metabolism. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 115–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Roos, B.; Mavrommatis, Y.; Brouwer, I.A. Long-chain n-3 polyunsaturated fatty acids: New insights into mechanisms relating to inflammation and coronary heart disease. Br. J. Pharmacol. 2009, 158, 413–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egert, S.; Stehle, P. Impact of n-3 fatty acids on endothelial function: Results from human interventions studies. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 121–131. [Google Scholar] [CrossRef]
- Felau, S.M.; Sales, L.P.; Solis, M.Y.; Hayashi, A.P.; Roschel, H.; Sa-Pinto, A.L.; Andrade, D.C.O.; Katayama, K.Y.; Irigoyen, M.C.; Consolim-Colombo, F.; et al. Omega-3 Fatty Acid Supplementation Improves Endothelial Function in Primary Antiphospholipid Syndrome: A Small-Scale Randomized Double-Blind Placebo-Controlled Trial. Front. Immunol 2018, 9, 336. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author Name, Year, Country | Age Range/Mean Age (y) | Follow-Up Duration | Number of Cases/Size | Gender | Quantile | Adjusted RR (95% CI) | Quality Score | Adjustments |
|---|---|---|---|---|---|---|---|---|
| Mohan 2021, Asia, Africa, America, Europe and Oceania [40] | 54.1 | 7.5 | 6502/191,454 | M/F | 4 | 0.85 (0.77–0.94) | 6 | Age, sex, study center, BMI, educational level, smoking status, alcohol intake, physical activity, urban or rural location, history of diabetes, cancer, use of statin or antihypertension medications, and intake of fruit, vegetables, red meat, poultry, dairy, and total energy |
| Kobayashi 2019, Japan [13] | 45–74 | 14.9 | 2942/79,904 | M/F | 5 | 1.14 (0.99–1.32) | 9 | Age, area, BMI, alcohol intake total energy intake, coffee intake, green tea intake, smoking status, physical activity, occupation type, solitude and other food group |
| Kondo 2019, Japan [15] | 30–79 | 29 | 1070/9115 | M/F | 3 | 0.72 (0.57–0.91) | 8 | Age, sex, smoking status, drinking status, and total energy intake |
| Van den brandt 2019, The Netherlands [16] | 55–69 | 10 | 2985/120,852 | M/F | 4 | 1.45 (1.20–1.74) | 9 | Age at baseline, sex, cigarette smoking status, number of cigarettes smoked per day, years of smoking, diabetes, body height, non-occupational physical activity, highest level of education, intake of alcohol, vegetables and fruit, use of nutritional supplements and, in women, postmenopausal HRT |
| Deng 2018, USA [14] | ≥18 | 18 | 326/1136 | M/F | 3 | 0.69 (0.50–0.96) | 7 | Age, sex, race/ethnicity, family income, the type of residential area, cigarette smoking, alcohol drinking, and the history of cardiovascular disease assessed at the baseline survey, and the years of using insulin as the indicator of diabetes severity |
| Hengeveld 2018, The Netherlands [17] | 20–70 | 18 | 540/34,033 | M/F | 3 | 0.94 (0.80–1.10) | 9 | Age, sex, physical activity, smoking status, education level, BMI, alcohol intake, total energy intake, intakes of saturated fatty acids, trans fatty acids, fruit, vegetables, and dietary fiber |
| Zhang 2018, USA [18] | 50–71 | 16 | 14824/240,729 | M/F | 5 | 0.9 (0.86–0.94) | 8 | Age, BMI, race, education, marital status, smoking, alcohol, intake of total energy, red meat, saturated fat, vegetables and fruits, multi-vitamin use, aspirin use, history of diabetes, history of hypertension, history of high cholesterol level |
| Bellavia 2017, Sweden [23] | 45–83 | 17 | 5039/72,522 | M/F | 5 | 0.95 (0.94–0.95) | 9 | BMI, total physical activity, smoking status and pack-years of smoking, alcohol consumption, educational level (primary school, secondary school or university), total energy intake, fruit consumption, vegetable consumption, processed red meat consumption and non-processed red meat consumption |
| Nahab 2016, USA [24] | ≥40 | 5.1 | 582/16,479 | M/F | 4 | 1.46 (0.87–2.45) | 7 | Age, race, region, sex, income, education, exercise, smoking status, Mediterranean diet score, regular aspirin use, total energy intake (kcald−1), current use of hypertensive medication, diabetes status, systolic blood pressure, BMI and dyslipidaemia |
| Owen 2016, Australia [25] | ≥25 | 9.7 | 277/11,247 | M/F | 4 | 0.66 (0.46–0.96) | 7 | Age, previous CVD, education, exercise, diabetes, total dietary energy and smoking |
| Eguchi 2014, Japan [26] | 40–79 | 19.3 | 2412/42,946 | M/F | 2 | 0.89 (0.82–0.97) | 8 | Age, body mass index, history of hypertension, history of diabetes, education level, regular employment, perceived mental stress, and 7 health behaviors |
| Takata 2013, China [27] | 40–74 | 8.7 | 1789/134,296 | M/F | 5 | 0.86 (0.70–1.05) | 6 | Age at baseline, total energy intake, income, occupation, education, comorbidity index, physical activity level, red meat intake, poultry intake, total vegetable intake, total fruit intake, smoking history, and alcohol consumption |
| Tomasallo 2010, USA [28] | 45.8 | 12 | 44/1367 | M/F | 3 | 0.45 (0.21–0.99) | 7 | Age, sex, body mass index, and income at study baseline |
| Yamagishi 2008, Japan [29] | 40–79 | 12.7 | 2045/57,972 | M/F | 5 | 0.82 (0.71–0.95) | 7 | Age, gender, history of hypertension and diabetes mellitus, smoking status, alcohol consumption, body mass index, mental stress, walking, sports, education levels, total energy, and dietary intakes of cholesterol, saturated and n-6 polyunsaturated fatty acids, vegetables, and fruit |
| Folsom 2004, USA [30] | 55–69 | 14 | 1589/41,836 | F | 5 | 0.95 (0.78–1.15) | 7 | Age, energy intake, educational level, physical activity level, alcohol consumption, smoking status, pack-years of cigarette smoking, age at first livebirth, estrogen use, vitamin use, body mass index, waist/hip ratio, diabetes, hypertension, intake of whole grains, fruit and vegetables, red meat, cholesterol, and saturated fat |
| Gillum 2000, USA [31] | 25–74 | 18.8 | --/8825 | M/F | 4 | 1.01 (0.81–1.25) | 9 | Age, smoking, history of diabetes, education, high school graduate, systolic blood pressure, serum cholesterol concentration, body mass index, alcohol intake, and physical activity |
| Albert 1998 [32] | 40–84 | 11 | 548/20,551 | M | 5 | 0.81 (0.49–1.33) | 8 | Age, aspirin and beta carotene treatment assignment, evidence of cardiovascular disease, prior to 12-month questionnaire, body mass index, smoking status, history of diabetes, history of hypertension, history of hypercholesterolemia, alcohol consumption, vigorous exercise, and vitamin E, vitamin C, and multivitamin use |
| Daviglus 1997 [33] | 40–55 | 30 | 573/2107 | M | 4 | 0.74 (0.52–1.06) | 8 | Age, education, religion, systolic pressure, serum cholesterol, number of cigarettes smoked per day, body-mass index, presence or absence of diabetes, presence or absence of electrocardiographic abnormalities, daily intake of energy, cholesterol, saturated, monounsaturated, and polyunsaturated fatty acids, total protein, carbohydrate, alcohol, iron, thiamine, riboflavin, niacin, vitamin C, beta carotene, and retinol |
| Author Name, Year, Country | Age Range/Mean Age (y) | Follow-Up Duration | Number of Cases/Size | Gender | Quantile | Adjusted RR (95% CI) | Quality Score | Adjustments |
|---|---|---|---|---|---|---|---|---|
| Donat-Varga 2020, Sweden [34] | Men: 65.5 Women: 62.5 | 15.5 | 6338/69,497 | M/F | 5 | 0.79 (0.66–0.95) | 8 | Age, gender, education level, waist circumference, hypertension, hypercholesterolemia, weight loss > 5kg within 1 year, leisure-time inactivity and daily walking/cycling, family history of myocardial infarction before the age of 60 years, smoking status, use of aspirin, energy intake, Mediterranean diet, parity, use of hormone replacement therapy and dietary methylmercury exposure, dietary PCB exposure |
| Zhuang 2019, USA [35] | 50–71 | 16 | 38,747/521,120 | M/F | 5 | 0.9 (0.87–0.94) | 8 | Age, gender, BMI, race, education, marital status, household income, smoking, alcohol drinking, physical activity, multi-vitamin use, aspirin use, history of hypertension, history of hypercholesterolemia, perceived health condition, history of heart disease, stroke, diabetes, and cancer at baseline, hormones use for women, intake of total energy, percentages of energy intake from protein, and remaining fatty acids where appropriate (saturated, α-linolenic, marine omega-3, linoleic, arachidonic, monounsaturated and trans fatty acids) |
| Zhang 2018, USA [18] | 50–71 | 16 | 22,365/421,309 | M/F | 5 | 0.84 (0.80–0.88) | 8 | Age, BMI, race, education, marital status, smoking, alcohol, intake of total energy, red meat, saturated fat, vegetables and fruits, physical activity, multi-vitamin use, aspirin use, history of diabetes, history of hypertension, history of high cholesterol level and hormones use, intake of a-linolenic acid, omega-6 PUFAs, monounsaturated fatty acids and trans-fatty acid |
| Rhee 2016, USA [11] | ≥45 | 22 | 501/39,876 | F | 5 | 1.15 (0.87–1.51) | 9 | Age, BMI, smoking, alcohol intake, physical activity, randomized treatment, oral contraceptive use, use of hormones as defined under HRT, multivitamin use, family history of MI, baseline history of hypertension, high cholesterol, and diabetes, intakes of dietary fiber, fruits and vegetables, trans fat, ratio of polyunsaturated to saturated fat, and sodium |
| Owen 2016, Australia [25] | ≥25 | 9.7 | 277/11,247 | M/F | 5 | 1.00 (0.62–1.60) | 7 | Age, sex, previous CVD, education, exercise, diabetes, total dietary energy and smoking |
| Miyagawa 2014, Japan [36] | ≥30 | 24 | 879/9190 | M/F | 4 | 0.80 (0.66–0.96) | 7 | Age, sex, smoking status, drinking status, systolic blood pressure, blood glucose, serum total cholesterol, body mass index, antihypertensive medication status, residential area, dietary intakes of saturated fatty acids, total n-6 PUFA, vegetable protein, total dietary fiber and sodium |
| Bell 2014, USA [37] | 50–76 | 5 | 769/70,495 | M/F | 4 | 0.87 (0.68–1.10) | 6 | Age, sex, raceethnicity, marital status, education, body mass index, physical activity, smoking, alcohol intake, total energy intake, vegetables intake, dietary intake of arachidonic acid, aspirin use, use of non-aspirin nonsteroidal anti-inflammatory drugs, self-rated health, sigmoidoscopy, mammogram, prostate-specific antigen test, current use of cholesterol-lowering medication, history of cardiovascular disease, family history of heart attack, current use of blood pressure medication, percentage of calories derived from trans-fat, percentage of calories derived from saturated fat, years of estrogen therapy, and years of estrogen + progestin therapy etc. |
| Koh 2013, Singapore [38] | 45–74 | 14.8 | 4780/60,298 | M/F | 4 | 0.86 (0.77–0.96) | 8 | Age, sex, dialect, year of interview, educational level, body mass index, physical activity, smoking status, alcohol use, baseline history of self-reported diabetes, hypertension, coronary heart disease, stroke, and total energy, adjusted for intakes of protein, dietary fiber, monounsaturated fat, saturated fat, omega-6 fatty acids, and alternate omega-3 fatty acids |
| Takata 2013, China [27] | 40–74 | 8.7 | 1789/134,296 | M/F | 5 | 0.74 (0.62–0.88) | 6 | Age, total energy intake, income, occupation, education, comorbidity index, physical activity level, red meat intake, poultry intake, total vegetable intake, total fruit intake, smoking history, and alcohol consumption (among men only) |
| Kamphuis 2006, The Netherlands [39] | 70–79 | 10 | 92/332 | M | 3 | 0.88 (0.51–1.5) | 8 | Age, years of education, BMI, smoking, alcohol consumption, systolic blood pressure, total and HDL-cholesterol concentrations, physical activity, living alone, and energy intake |
| Comparison | N † | Pooled RRs (95% CI) | Heterogeneity (I2), p a Value | pb Value | pc Value | |
|---|---|---|---|---|---|---|
| Fish Intake and CVD Mortality Risk | 18 | 0.91 (0.85–0.98) | 70.0%, 0.000 | 0.015 | ||
| Country | Asia | 5 | 0.89 (0.78–1.01) | 74.1%, 0.004 | 0.081 | 0.216 |
| Europe and America | 11 | 0.95 (0.84–1.08) | 72.2%, 0.000 | 0.417 | ||
| Oceania | 1 | 0.66 (0.46–0.95) | -- | 0.027 | ||
| Asia, Africa, America, Europe and Oceania | 1 | 0.85 (0.77, 0.94) | -- | 0.001 | ||
| Gender | Men | 2 | 0.76 (0.57–1.02) | 0.0%, 0.773 | 0.067 | 0.442 |
| women | 1 | 0.95 (0.78–1.15) | -- | 0.605 | ||
| Both | 15 | 0.92 (0.85–1.00) | 74.5%, 0.000 | 0.040 | ||
| Follow-up duration | <9 years | 3 | 0.90 (0.76–1.07) | 50.6%, 0.132 | 0.234 | 0.851 |
| ≥9 years | 15 | 0.91 (0.84–0.99) | 72.7%, 0.000 | 0.035 | ||
| Dropout rate | <20% | 11 | 0.93 (0.82–1.06) | 76.7%, 0.000 | 0.284 | 0.557 |
| >20% | 7 | 0.88 (0.82–0.94) | 41.6%, 0.113 | 0.000 | ||
| Excluding history of CVD | Yes | 11 | 0.97 (0.88–1.06) | 77.0%, 0.000 | 0.492 | 0.905 |
| No | 7 | 0.82 (0.75–0.91) | 21.7%, 0.264 | 0.000 | ||
| Adjustment for diabetes | Yes | 11 | 0.93 (0.85, 1.01) | 72.9%, 0.000 | 0.094 | 0.040 |
| No | 4 | 0.84 (0.63, 1.12) | 80.9%, 0.001 | 0.233 | ||
| Others * | 3 | 0.89 (0.76, 1.04) | 34.5%, 0.217 | 0.149 | ||
| Adjustment for smoking | Yes | 16 | 0.92 (0.85, 1.00) | 71.8%, 0.000 | 0.050 | 0.484 |
| No | 2 | 0.71 (0.38, 1.33) | 66.0%, 0.087 | 0.285 | ||
| Marine n-3 PUFA and CVD mortality risk | 10 | 0.87 (0.85–0.89) | 37.8%, 0.106 | 0.000 | ||
| Country | Asia | 3 | 0.82 (0.75–0.89) | 4.9%, 0.349 | 0.000 | 0.212 |
| Europe and America | 6 | 0.88 (0.85–0.90) | 49.2%, 0.08 | 0.000 | ||
| Oceania | 1 | 1.00 (0.62–1.61) | -- | 1.000 | ||
| Gender | Men | 1 | 0.88 (0.51–1.51) | -- | 0.642 | 0.182 |
| Women | 1 | 1.15 (0.87–1.52) | -- | 0.320 | ||
| Both | 8 | 0.87 (0.84–0.89) | 33.3%, 0.162 | 0.000 | ||
| Follow-up duration | <9 years | 2 | 0.78 (0.68-0.90) | 12.1%, 0.286 | 0.001 | 0.192 |
| ≥9 years | 8 | 0.87 (0.85–0.90) | 37.0%, 0.134 | 0.000 | ||
| Dropout rate | <20% | 5 | 0.89 (0.86–0.92) | 51.8%, 0.08 | 0.000 | 0.114 |
| >20% | 5 | 0.84 (0.80–0.87) | 0.0%, 0.877 | 0.000 | ||
| Excluding history of CVD | Yes | 5 | 0.84 (0.81–0.88) | 29.9%, 0.222 | 0.000 | 0.536 |
| No | 5 | 0.89 (0.86–0.92) | 23.4%, 0.266 | 0.000 | ||
| Adjustment for diabetes | Yes | 6 | 0.88 (0.85, 0.90) | 44.4%, 0.109 | 0.000 | 0.060 |
| No | 3 | 0.77 (0.68, 0.88) | 0.0%, 0.745 | 0.000 | ||
| Others * | 1 | 0.79 (0.66, 0.95) | -- | 0.0 11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, L.; Wang, J.; Xiong, K.; Xu, L.; Zhang, B.; Ma, A. Intake of Fish and Marine n-3 Polyunsaturated Fatty Acids and Risk of Cardiovascular Disease Mortality: A Meta-Analysis of Prospective Cohort Studies. Nutrients 2021, 13, 2342. https://doi.org/10.3390/nu13072342
Jiang L, Wang J, Xiong K, Xu L, Zhang B, Ma A. Intake of Fish and Marine n-3 Polyunsaturated Fatty Acids and Risk of Cardiovascular Disease Mortality: A Meta-Analysis of Prospective Cohort Studies. Nutrients. 2021; 13(7):2342. https://doi.org/10.3390/nu13072342
Chicago/Turabian StyleJiang, Lan, Jinyu Wang, Ke Xiong, Lei Xu, Bo Zhang, and Aiguo Ma. 2021. "Intake of Fish and Marine n-3 Polyunsaturated Fatty Acids and Risk of Cardiovascular Disease Mortality: A Meta-Analysis of Prospective Cohort Studies" Nutrients 13, no. 7: 2342. https://doi.org/10.3390/nu13072342
APA StyleJiang, L., Wang, J., Xiong, K., Xu, L., Zhang, B., & Ma, A. (2021). Intake of Fish and Marine n-3 Polyunsaturated Fatty Acids and Risk of Cardiovascular Disease Mortality: A Meta-Analysis of Prospective Cohort Studies. Nutrients, 13(7), 2342. https://doi.org/10.3390/nu13072342