
Influence of Plant and Animal Proteins on Inflammation Markers among Adults with Chronic Kidney Disease: A Systematic Review and Meta-Analysis



Abstract
1. Introduction
2. Materials and Methods
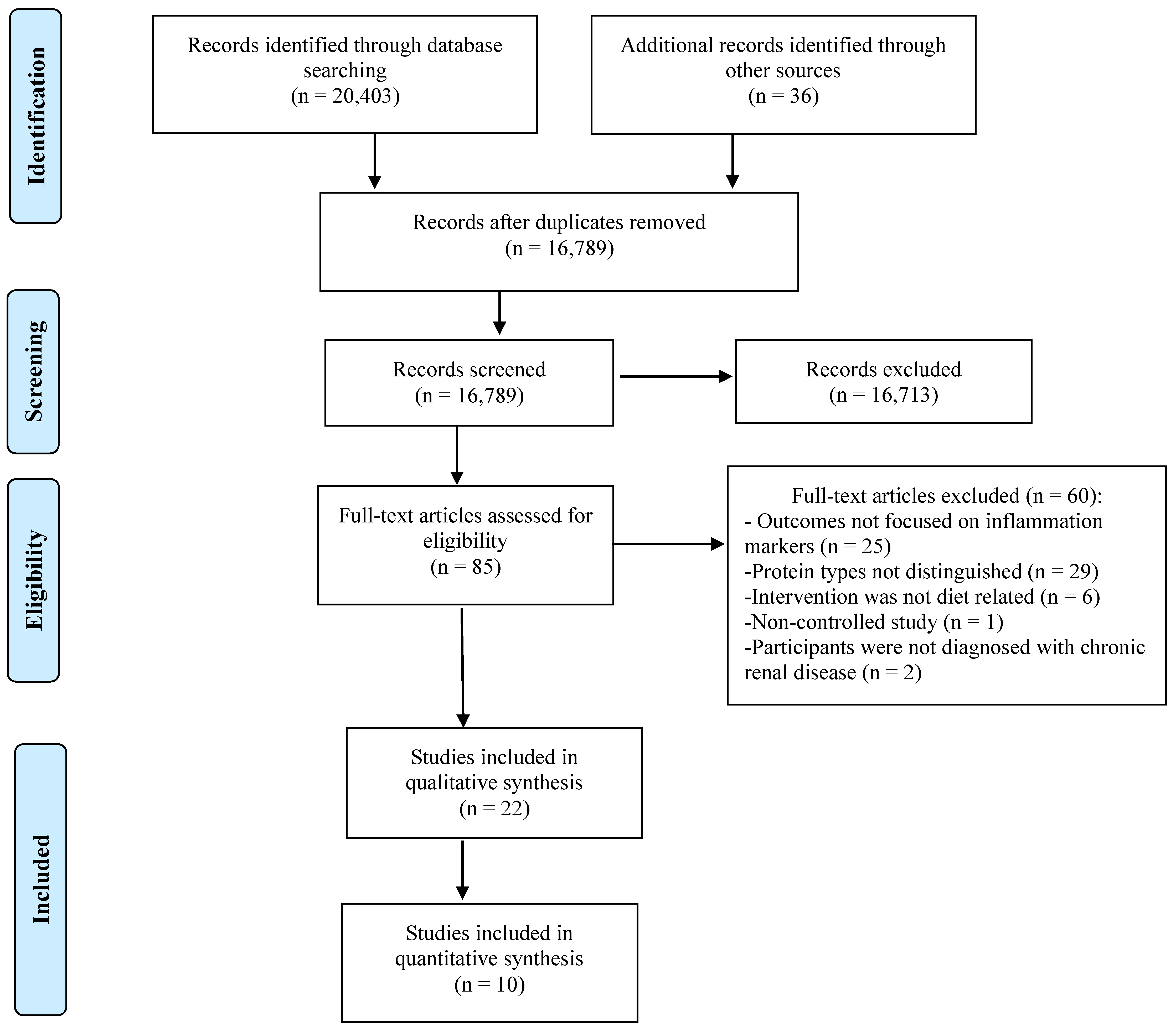
2.1. Selection of the Studies
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Quality and Risk of Bias Assessment
2.5. Assessment of Heterogeneity
2.6. Data Synthesis
3. Results
3.1. Study Characteristics
3.2. Quality and Risk of Bias
3.3. Publication Bias, Heterogeneity, and Risk of Bias
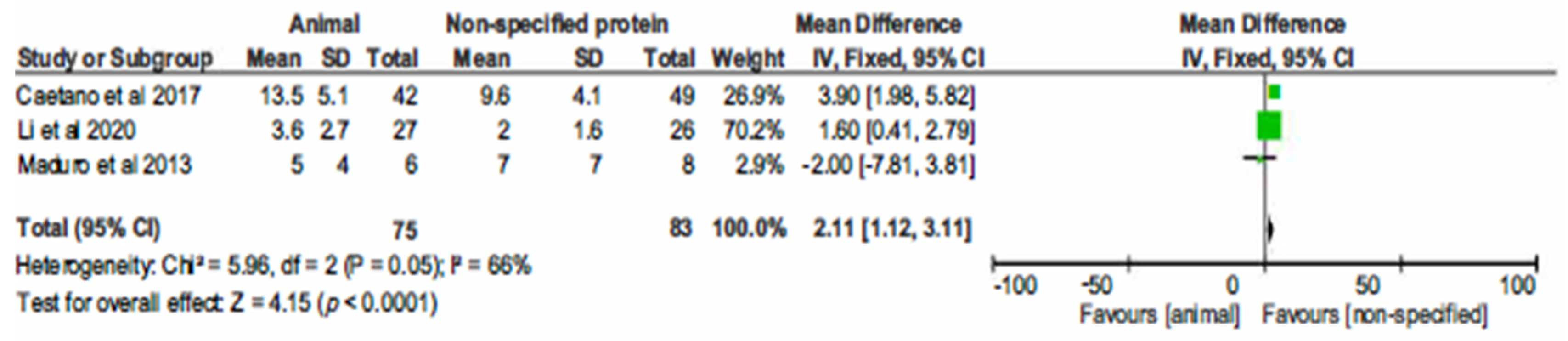
3.4. Meta-Analysis
The Effect of Protein Type on Inflammation Markers
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kopyt, N.P. Chronic kidney disease: The new silent killer. J. Am. Osteopath. Assoc. 2006, 106, 133–136. [Google Scholar]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic Kidney Disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Lisowska-Myjak, B. Uremic toxins and their effects on multiple organ systems. Nephron Clin. Pract. 2014, 128, 303–311. [Google Scholar] [CrossRef]
- ZoCCali, C.; Vanholder, R.; Massy, Z.A.; Ortiz, A.; Sarafidis, P.; Dekker, F.W.; Fliser, D.; Fouque, D.; Heine, G.; Jager, K.; et al. The systemic nature of CKD. Nat. Rev. Nephrol. 2017, 13, 344–358. [Google Scholar] [CrossRef]
- Cobo, G.; Lindholm, B.; Stenvinkel, P. Chronic inflammation in end-stage renal disease and dialysis. Nephrol. Dial. Transplant. 2018, 33, iii35–iii40. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Stenvinkel, P.; Pillon, L.; Kopple, J.D. Inflammation and nutrition in renal insufficiency. Adv. Ren. Replace. Ther. 2003, 10, 155–169. [Google Scholar] [CrossRef]
- del Giudice, M.; Gangestad, S.W. Rethinking IL-6 and CRP: Why they are more than inflammatory biomakers, and why it matters. Brain. Behav. Immun. 2018, 70, 61–75. [Google Scholar] [CrossRef]
- Stenvinkel, P.; Heimburger, O.; Paultre, F.; Diczfalusy, U.; Wang, T.; Berglund, L.; Jogestrand, T. Strong association between malnutrition, inflammation, and atherosclerosis in chronic renal failure. Kidney Int. 1999, 55, 1899–1911. [Google Scholar] [CrossRef]
- Zimmerman, J.; Herrlinger, S.; Pruy, A.; Metzger, T.; Wanner, C. Inflammation enhances cardiovascular risk and mortality in hemodialysis patients. Kidney Int. 1999, 55, 648–658. [Google Scholar] [CrossRef] [PubMed]
- Magno, A.L.; Herat, L.Y.; Carnagarin, R.; Schlaich, M.P.; Matthews, V.B. Current knowledge of IL-6 cytokine family members in acute and chronic kidney disease. Biomedicines 2019, 7, 19. [Google Scholar] [CrossRef]
- Oberg, B.P.; McMenamin, E.; Lucas, F.L.; McMonagle, E.; Morrow, J.; Ikizler, T.A.; Himmelfarb, J. Increased prevalence of oxidant stress and inflammation in patients with moderate to severe chronic kidney disease. Kidney Int. 2004, 65, 1009–1016. [Google Scholar] [CrossRef]
- Su, H.; Lei, C.-T.; Zhang, C. Interleukin-6 signaling pathway and its role in kidney disease: An update. Front. Immunol. 2017, 21, 405. [Google Scholar] [CrossRef] [PubMed]
- Jankowska, M.; Cobo, G.; Lindholm, B.; Stenvinkel, P. Inflammation and protein-energy wasting in the uremic milieu. Contrib. Nephrol. 2017, 191, 58–71. [Google Scholar]
- Mihai, S.; Codrici, E.; Popescu, I.D.; Enciu, A.M.; Albulescu, L.; Necula, L.G.; Mambet, C.; Anton, G.; Tanase, C. Inflammation-related mechanisms in chronic kidney disease prediction, progression, and outcome. J. Immunol. Res. 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Gansevoort, R.T.; Correa-Rotter, R.; Hemmelgarn, B.R.; Jafar, T.H.; Heerspink, H.J.L.; Mann, J.F.; Matsushita, K.; Wen, C.P. Chronic kidney disease and cardiovascular risk: Epidemiology, mechanisms, and prevention. Lancet 2013, 382, 339–352. [Google Scholar] [CrossRef]
- Jadoon, A.; Mathew, A.V.; Byun, J.; Gadegbeku, C.A.; Gipson, D.S.; Afshinnia, F.; Pennathur, S. Gut microbial product predicts cardiovascular risk in chronic kidney disease patients. Am. J. Nephrol. 2018, 48, 269–277. [Google Scholar] [CrossRef]
- Ruokonen, H.; Nylund, K.; Furuholm, J.; Meurman, J.H.; Sorsa, T.; Kotaniemi, K.; Ortiz, F.; Heikkinen, A.M. Oral health and mortality in patients with chronic kidney disease. J. Periodontol. 2017, 88, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Moore, L.W. Does kidney longevity mean healthy vegan food and less meat or is any low-protein diet good enough? J. Ren. Nutr. 2019, 29, 79–81. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI clinical practice guideline for nutrition in CKD: 2020 update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef]
- Kelly, J.T.; Palmer, S.C.; Wai, S.N.; Ruospo, M.; Carrero, J.J.; Campbell, K.L.; Strippoli, G.F.M. Healthy dietary patterns and risk of mortality and ESRD in CKD: A meta-analysis of cohort studies. Clin. J. Am. Soc. Nephrol. 2017, 12, 272–279. [Google Scholar] [CrossRef]
- Fouque, D.; Laville, M. Low protein diets for chronic kidney disease in non diabetic adults. Cochrane Database Syst. Rev. 2006, 19, CD001892. [Google Scholar]
- Hahn, D.; Hodson, E.M.; Fouque, D. Low protein diets for non-diabetic adults with chronic kidney disease. Cochrane Database Syst. Rev. 2020, 10, CD001892. [Google Scholar] [CrossRef]
- Kasiske, B.L.; Lakatua, J.D.A.; Ma, J.Z.; Louis, T.A. A meta-analysis of the effects of dietary protein restriction on the rate of decline in renal function. Am. J. Kidney Dis. 1998, 31, 954–961. [Google Scholar] [CrossRef]
- Rhee, C.M.; Ahmadi, S.F.; Kovesdy, C.P.; Kalantar-Zadeh, K. Low-protein diet for conservative management of chronic kidney disease: A systematic review and meta-analysis of controlled trials. J. Cachexia Sarcopenia Muscle 2018, 9, 235–245. [Google Scholar] [CrossRef]
- Yan, B.; Su, X.; Xu, B.; Qiao, X.; Wang, L. Effect of diet protein restriction on progression of chronic kidney disease: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0206134. [Google Scholar] [CrossRef]
- Mirmiran, P.; Yuzbashian, E.; Aghayan, M.; Mahdavi, M.; Asghari, G.; Azizi, F. A prospective study of dietary meat intake and risk of incident chronic kidney disease. J. Ren. Nutr. 2020, 30, 111–118. [Google Scholar] [CrossRef]
- Haring, B.; Selvin, E.; Liang, M.; Coresh, J.; Grams, M.E.; Petruski-Ivleva, N.; Steffen, L.M.; Rebholz, C.M. Dietary protein sources and risk for incident chronic kidney disease: Results from the atherosclerosis risk in communities (ARIC) study. J. Ren. Nutr. 2017, 27, 233–242. [Google Scholar] [CrossRef]
- Ko, G.J.; Obi, Y.; Tortoricci, A.R.; Kalantar-Zadeh, K. Dietary protein intake and chronic kidney disease. Curr. Opin. Clinc. Nutr. Metab. Care 2017, 20, 77–85. [Google Scholar] [CrossRef]
- Lew, Q.-L.J.; Jafar, T.H.; Koh, H.W.L.; Jin, A.; Chow, K.Y.; Yuan, J.-M.; Koh, W.-P. Red meat intake and risk of ESRD. J. Am. Soc. Nephrol. 2016, 28, 304–312. [Google Scholar] [CrossRef]
- Toumpanakis, A.; Turnbull, T.; Alba-Barba, I. Effectiveness of plant-based diets in promoting well-being in the management of type 2 diabetes: A systematic review. BMJ Open Diabetes Res. Care 2018, 6. [Google Scholar] [CrossRef]
- Zha, Y.; Qian, Q. Protein nutrition and malnutrition in CKD and ESRD. Nutrients 2017, 9, 208. [Google Scholar] [CrossRef] [PubMed]
- Medawar, E.; Huhn, S.; Villringer, A.; Veronica Witte, A. The effects of plant-based diets on the body and the brain: A systematic review. Transl. Psychiatry 2019, 9, 226. [Google Scholar] [CrossRef]
- Dinu, M.; Abbate, R.; Gensini, G.F.; Casini, A.; Sofi, F. Vegetarian, vegan diets and multiple health outcomes: A systematic review with meta-analysis of observational studies. Crit. Rev. Food Sci. Nutr. 2017, 57, 3640–3649. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Caulfield, L.E.; Garcia-Larsen, V.; Steffen, L.M.; Grams, M.E.; Coresh, J.; Rebholz, C.M. Plant-based diets and incident CKD and kidney function. Clin. J. Am. Soc. Nephrol. 2019, 14, 682–691. [Google Scholar] [CrossRef]
- Carrero, J.J.; González-Ortiz, A.; Avesani, C.M.; Bakker, S.J.L.; Bellizzi, V.; Chauveau, P.; Clase, C.M.; Cupisti, A.; Espino-sa-Cuevas, A.; Molina, P. Plant-based diets to manage the risks and complications of chronic kidney disease. Nat. Rev. Nephrol. 2020, 16, 525–542. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Joshi, S.; Schlueter, R.; Cooke, J.; Brown-Tortorici, A.; Donnelly, M.; Schulman, S.; Lau, W.L.; Rhee, C.M.; Streja, E.; et al. Plant-dominant low-protein diet for conservative management of chronic kidney disease. Nutrients 2020, 12, 1931. [Google Scholar] [CrossRef]
- Marks, K.J.; Hartman, T.J.; Judd, S.E.; Ilori, T.O.; Cheung, K.L.; Warnock, D.G.; Gutiérrez, O.M.; Goodman, M.; Cushman, M.; McClellan, W.M. Dietary oxidative balance scores and biomarkers of inflammation among individuals with and without chronic kidney disease. Nephron Extra 2018, 8, 11–23. [Google Scholar] [CrossRef]
- Chauveau, P.; Aparicio, M.; Bellizzi, V.; Campbell, K.L.; Hong, X.; Johansson, L.; Kolko, A.; Molina, P.; Sezer, S.; Wanner, C. Mediterranean diet as the diet of choice for patients with chronic kidney disease. Nephrol. Dial. Transplant. 2018, 33, 725–735. [Google Scholar] [CrossRef]
- Chauveau, P.; Koppe, L.; Combe, C.; Lasseur, C.; Trolonge, S.; Aparicio, M. Vegetarian diets and chronic kidney disease. Nephrol. Dial. Transplant. 2019, 34, 199–207. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 339, 1–8. [Google Scholar]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 6th ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Sterne, J.A.; Hernan, M.A.; Reeves, B.C.; Savovic, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355. [Google Scholar] [CrossRef]
- Bergesio, F.; Monzani, G.; Guasparini, A.; Ciuti, R.; Gallucci, M.; Cristofano, C.; Castrignano, E.; Cupisti, A.; Barsotti, G.; Marcucci, R.; et al. Cardiovascular risk factors in severe chronic renal failure: The role of dietry treatment. Clin. Nephrol. 2005, 64, 103–112. [Google Scholar] [CrossRef] [PubMed]
- di Iorio, B.R.; di Micco, L.; Marzocco, S.; de Simone, E.; de Blasio, A.; Sirico, M.L.; Nardone, L. Very low-protein diet (VLPD) reduces metabolic acidosis in subjects with chronic kidney disease: The “Nutritional light signal” of the renal acid load. Nutrients 2017, 9, 69. [Google Scholar] [CrossRef]
- Di Iorio, B.R.; Marzocco, S.; Bellasi, A.; De Simone, E.; Dal Piaz, F.; Rocchetti, M.T.; Cosola, C.; Di Micco, L.; Gesualdo, L. Nutritional therapy reduces protein carbamylation through urea lowering in chronic kidney disease. Nephrol. Dial. Transplant. 2018, 33, 804–813. [Google Scholar] [CrossRef]
- Fanti, P.; Asmis, R.; Stephenson, T.J.; Sawaya, B.P.; Franke, A.A. Positive effect of dietary soy in ESRD patients with systemic inflammation—Correlation between blood levels of the soy isoflavones and the acute-phase reactants. Nephrol. Dial. Transplant. 2006, 21, 2239–2246. [Google Scholar] [CrossRef] [PubMed]
- Rhee, C.M.; You, A.S.; Parsons, T.K.; Tortorici, A.R.; Bross, R.; St-Jules, D.E.; Jing, J.; Lee, M.L.; Benner, D.; Kovesdy, C.P.; et al. Effect of high-protein meals during hemodialysis combined with lanthanum carbonate in hypoalbuminemic dialysis patients: Findings from the FrEDI randomized controlled trial. Nephrol. Dial. Transplant. 2017, 32, 1233–1243. [Google Scholar] [CrossRef]
- Siefker, K.; DiSilvestro, R.A. Safety and antioxidant effects of a modest soy protein intervention in hemodialysis patients. J. Med. Food 2006, 9, 368–372. [Google Scholar] [CrossRef]
- Maduro, I.P.D.N.N.; Nonino, C.B.; Sakamoto, L.M.; Meirelles, M.G.; Cardeal Da Costa, J.A.; Marchini, J.S. Red meat snacks for chronic hemodialysis patients: Effect on inflammatory activity (A Pilot Study). Ren. Fail. 2013, 35, 830–834. [Google Scholar] [CrossRef]
- Li, J.; Hou, G.; Sun, X.; Chen, A.; Chai, Y. A low-cost, intradialytic, protein-rich meal improves the nutritional status in Chinese hemodialysis patients. J. Ren. Nutr. 2020, 30, e27–e34. [Google Scholar] [CrossRef]
- Sahathevan, S.; Se, C.H.; Ng, S.H.; Khor, B.H.; Chinna, K.; Goh, B.L.; Gafor, H.A.; Bavanandan, S.; Ahmad, G.; Karupaiah, T. Clinical efficacy and feasibility of whey protein isolates supplementation in malnourished peritoneal dialysis patients: A multicenter, parallel, open-label randomized controlled trial. Clin. Nutr. ESPEN 2018, 25, 68–77. [Google Scholar] [CrossRef]
- Caetano, C.; Valente, A.; Silva, F.J.; Antunes, J.; Garagarza, C. Effect of an intradialytic protein-rich meal intake in nutritional and body composition parameters on hemodialysis patients. Clin. Nutr. ESPEN 2017, 20, 29–33. [Google Scholar] [CrossRef]
- Ragel, P.; Raddatz, N.; Leidi, E.O.; Quintero, F.J.; Pardo, J.M. Regulation of K+ nutrition in plants. Front. Plant Sci. 2019, 10, 281. [Google Scholar] [CrossRef]
- Adeva, M.M.; Souto, G. Diet-induced metabolic acidosis. Clin. Nutr. 2011, 30, 416–421. [Google Scholar] [CrossRef]
- Scialla, J.J.; Appel, L.J.; Wolf, M.; Yang, W.; Zhang, X.; Sozio, S.M.; Miller, E.R.; Bazzano, L.A.; Cuevas, M.; Glenn, M.J. plant protein intake is associated with fibroblast growth factor 23 and serum bicarbonate levels in patients with chronic kidney disease: The chronic renal insufficiency cohort study. J. Ren. Nutr. 2012, 22, 379. [Google Scholar] [CrossRef]
- Gorissen, S.H.M.; Crombag, J.J.R.; Senden, J.M.G.; Waterval, W.A.H.; Bierau, J.; Verdijk, L.B.; VanLoon, L.J.C. Protein content and amino acid composition of commerically available plant-based protein isolates. Amino Acids 2018, 50, 1685–1695. [Google Scholar] [CrossRef]
- Fanti, P.; Sawaya, B.P.; Custer, L.J.; Franke, A.A. Serum levels and metabolic clearance of the isoflavones genistein and daidzein in hemodialysis patients. J. Am. Soc. Nephrol. 1999, 10, 864–871. [Google Scholar] [CrossRef]
- Jing, Z.; Wei-Jie, Y. Effects of soy protein containing isoflavones in patients with chronic kidney disease: A systematic review and meta-analysis. Clin. Nutr. 2016, 35, 117–124. [Google Scholar] [CrossRef]
- Menzel, J.; Biemann, R.; Longree, A.; Isermann, B.; Mai, K.; Schulze, M.B.; Abraham, K.; Weikert, C. Associations of a vegan diet with inflammatory biomarkers. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Shah, B.; Newman, J.D.; Woolf, K.; Ganguzza, L.; Guo, Y.; Allen, N.; Zhong, J.; Fisher, E.A.; Slater, J. Anti-inflammatory effects of a vegan diet versus the American heart association recommended diet in coronary artery disease trial. J. Am. Heart Assoc. 2018, 7, e011367. [Google Scholar] [CrossRef]
- Hruby, A.; Jacques, P.F. Dietary protein and changes in biomarkers of inflammation and oxidative stress in the Framinham heart study offspring cohort. Curr. Dev. Nutr. 2019, 3, nzz019. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.-M.; Xu, J.-Y.; Rao, C.-P.; Han, S.; Wan, Z.; Qin, L.-Q. Effect of whey supplementation on circulating C-reactive protein: A meta-analysis of randomized controlled trials. Nutrients 2015, 7, 1131–1143. [Google Scholar] [CrossRef] [PubMed]
- Xia, Z.; Cholewa, J.; Zhao, Y.; Shang, H.Y.; Yang, Y.Q.; Pessôa, K.A.; Su, Q.S.; Lima-Soares, F.; Zanchi, N. Targeting inflammation and downstream protein metabolism in sacropenia: A brief up-dated description of concurrent exercise and leucine-based multimodal intervention. Front. Physiol. 2017, 8, 434. [Google Scholar] [CrossRef]
- Crozier, S.J.; Kimball, S.R.; Emmert, S.W.; Anthony, J.C.; Jefferson, L.S. Oral leucine administration stimulates protein synthesis in rat skeletal muscle. J. Nutr. 2005, 135, 376–382. [Google Scholar] [CrossRef]
- Liberman, K.; Njemini, R.; Luiking, Y.; Forti, L.N.; Verlaan, S.; Bauer, J.M.; Memelink, R.; Brandt, K.; Donini, L.M.; Maggio, M.; et al. Thirteen weeks of supplementation of vitamin D and leucine-enriched whey protein nutritional supplement attenuates chronic low-grade inflammation in sarcopenic older adults: The PROVIDE study. Aging Clin. Exp. Res. 2019, 31, 845–854. [Google Scholar] [CrossRef]
- Yalcin, A. Emerging therapeutic potential of whey proteins and peptides. Curr. Pharm. Des. 2006, 12, 1637–1643. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Flakoll, P.J.; Parker, R.A.; Hakim, R.M. Amino acid and albumin losses during hemodialysis. Kidney Int. 1994, 46, 830–837. [Google Scholar] [CrossRef] [PubMed]
- Qin, A.; Liu, X.; Yin, X.; Zhou, H.; Tang, Y.; Qin, W. Normalized protein catabolic rate is a superior nutritional marker associated with dialysis adequacy in continuous ambulatory peritoneal dialysis patients. Front. Med. 2021, 7, 603725. [Google Scholar] [CrossRef]
- Sarav, M.; Kovesdy, C.P. Protein energy wasting in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2018, 13, 1558–1560. [Google Scholar] [CrossRef]
- Wright Nunes, J.A.; Wallston, K.A.; Eden, S.; Shintani, A.K.; Ikizler, T.A.; Cavanaugh, K. Associations among perceived and objective disease knowledge and satisfaction with physician communication in patients with chronic kidney disease. Kidney Int. 2011, 80, 1344–1351. [Google Scholar] [CrossRef]
- Marinac, C.R.; Sears, D.D.; Natarajan, L.; Gallo, L.C.; Breen, C.I.; Patterson, R.E. Frequency and circadian timing of eating may influence biomarkers of inflammation and insulin resistance associated with breast cancer risk. PLoS ONE 2015, 10, e0136240. [Google Scholar]
- Shankar, A.; Sun, L.; Klein, B.E.K.; Lee, K.E.; Muntner, P.; Nieto, F.J.; Tsai, M.Y.; Cruickshanks, K.; Schubert, C.R.; Brazy, P.C. Markers of inflammation predict the long-term risk of developing chronic kidney disease: A population-based cohort study. Kidney Int. 2011, 80, 1231–1238. [Google Scholar] [CrossRef] [PubMed]
- Ikizler, T.A. Nutrition, inflammation and chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2008, 17, 162–167. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author (Year) | Location and Sample Population. | Study Design and Duration | Study Intervention. | Inflammation Markers * and Collection Timing. | Methods/Techniques Used for Inflammation Markers. | Primary Outcome. |
|---|---|---|---|---|---|---|
| Bergesio et al. (2005) [43] | Florence, Italy. Adults on stable chronic kidney disease with moderate to severe renal failure (n = 60):
| Controlled cross sectional. 3 up to 12 months. | Control group: 0.6 g/kg/day of protein (animal and plant protein). Intervention group: 0.3 g/kg/day of plant-based protein and one tablet per 5–8 kg/day of essential amino acids. | C-reactive protein (CRP). Collected after overnight fast. | Immuno-nephelometry. | Significant decrease between control and intervention group post- intervention (p < 0.05). |
| Siefker et al. (2006) [48] | Ohio, United States. Adults on Hemodialysis (n = 17):
| Double-blind, randomized control trial. 1 month. | Control group: whey protein powder (25 g protein). Intervention group: soy protein powder (25 g protein). | CRP TNF-α. Collected before dialysis treatment. | CRP: ELISA TNF-α: enzyme immuno-assay. | CRP: No significant differences within groups (p > 0.05). Non-statistical increase within both intervention and control group post-intervention. TNF-α: No significant differences within groups (p > 0.05). Non-statistical decrease within the intervention group post-intervention. |
| Fanti et al. (2006) [46] | Texas, United States. Adults on Hemodialysis (n = 32):
| Double-blind, randomized controlled trial. 2 months. | Control group: isoflavone-free milk-based supplements. Intervention group: isoflavone containing soy-based nutritional supplements. | CRP IL-6 TNF-α. Collected before dialysis treatment. | CRP: Immuno-nephelometry IL-6, TNF-α: ELISA | No significant difference, based on medians, within intervention and control group for CRP, IL-6 and TNF-α. Non-statistical decrease between pre- and post-intervention group for CRP, IL-6, and TNF-α. |
| Maduro et al. (2013) [49] | Sao Paulo, Brazil.Adults on Hemodialysis (n = 14):
| Controlled, open-label prospective trial.1 month. | Group 1:
| CRPCollected before and after dialysis treatment. | Immuno-nephelometry. | Non-significant increase between groups 1 and 2 post-intervention. |
| Rhee et al. (2017) [47] | California, United States. Adults on Hemodialysis (n = 110):
| Double-blind, randomized controlled trial. 2 months. | Group 1: 50–55 g animal-based protein, 850 kcal, 400–450 mg of natural phosphorus. Group 2: <1 g plant-based protein, <50 calories, <20 mg phosphorus. | CRP IL-6 TNF-α Collection time unknown. | CRP: ** IL-6, TNF-α: enzyme immunoassay | CRP: Non-significant decrease between group 2 and 1 post- intervention (p = 0.74). IL-6: significant increase between group 2 and 1 post-intervention (p = 0.002). TNF-α: Non-significant decrease between group 2 and 1 post-intervention (p = 0.35). |
| Caetano et al. (2017) [52] | Lisbon, Portugal. Adults on Hemodialysis (n = 91):
| Non-randomized controlled study 6 months. | Control group: snack brought from home. Intervention group: 160 mL of a drink rich in high biological value protein (65% pasteurized egg albumin, milk proteins and whey proteins) and an egg sandwich. | CRP Collection time unknown. | ** | No significant difference within intervention group (p= 0.48) or control group (p = 0.74). In the intervention group, non-statistical increase post-intervention (+2.4 mean). |
| Di Iorio et al. (2017) [44] | Avellino, Italy. Adults on stages 3 to 4 of Chronic kidney disease (n = 146):
| Randomized, open label, controlled study. 12 months. | Control group: animal-based proteins, 0.6–1 g protein/kg/day. Intervention group: plant-based proteins, 0.3–0.4 g protein/kg/day, amino acid supplementation | CRP Collection time unknown. | ** | Non-statistical decrease post-intervention between intervention group compared to control group (p > 0.05). |
| Di Iorio et al. (2018) [45] | Avellino, Italy. Adults on stages 3 to 4 of Chronic kidney disease (n = 60):
| Prospective, randomized, crossover-controlled trial. 18 months | Free Diet (FD): proteins 1 g/kg body weight (bw)/day (animal proteins 50–70 g/day, plant-based proteins 15–20 g/day). Mediterranean diet (MD): proteins 0.7–0.8 g/kg (bw)/day (animal proteins 30–40 g/day, plant-based proteins 40–50 g/day). Very-low protein diet (VLPD): proteins 0.3–0.5 g/kg (bw)/day (animal proteins 0 g/day, plant-based proteins 30–40 g/day). Group A: 3 months FD/6 months VLPD and 3 months FD/6 months MD Group B: 3 months FD/6 months MD and 3 months FD/6 months VLPD. | CRP Collection time unknown | * | Significant decrease post- intervention between FD and VLPD (p = 0.01). |
| Sahathevan et al. (2018) [51] | Kuala Lumpur, Malaysia. Adults on Hemodialysis (n = 74):
| Multicenter, parallel, open label randomized controlled trial. 18 months. | Control group: nutrition counseling only. Intervention group: whey protein supplement (15 g protein) and nutrition counseling. | CRP Collection time unknown. | Immuno-turbidometric assay. | Non-significant decrease within or between intervention and control groups post-intervention (p = 0.87). |
| Li et al. (2020) [50] | Baotou, China. Adults on Hemodialysis (n = 53):
| Controlled, open-label, prospective trial. 3 months intervention + 3 months follow up. | Control group: nutritional counseling only, liberalized diet. Intervention group: nutritional counseling plus three intradialytic, protein-rich, animal-based meals 90 min after initiation of each HD session. | CRP Collected before dialysis treatment. | ** | Non-statistical increase between groups after 6 months (p = 0.36). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aycart, D.F.; Acevedo, S.; Eguiguren-Jimenez, L.; Andrade, J.M. Influence of Plant and Animal Proteins on Inflammation Markers among Adults with Chronic Kidney Disease: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 1660. https://doi.org/10.3390/nu13051660
Aycart DF, Acevedo S, Eguiguren-Jimenez L, Andrade JM. Influence of Plant and Animal Proteins on Inflammation Markers among Adults with Chronic Kidney Disease: A Systematic Review and Meta-Analysis. Nutrients. 2021; 13(5):1660. https://doi.org/10.3390/nu13051660
Chicago/Turabian StyleAycart, Danielle Francesca, Sofía Acevedo, Lucía Eguiguren-Jimenez, and Jeanette Mary Andrade. 2021. "Influence of Plant and Animal Proteins on Inflammation Markers among Adults with Chronic Kidney Disease: A Systematic Review and Meta-Analysis" Nutrients 13, no. 5: 1660. https://doi.org/10.3390/nu13051660
APA StyleAycart, D. F., Acevedo, S., Eguiguren-Jimenez, L., & Andrade, J. M. (2021). Influence of Plant and Animal Proteins on Inflammation Markers among Adults with Chronic Kidney Disease: A Systematic Review and Meta-Analysis. Nutrients, 13(5), 1660. https://doi.org/10.3390/nu13051660