
Supplementation with Octacosanol Affects the Level of PCSK9 and Restore Its Physiologic Relation with LDL-C in Patients on Chronic Statin Therapy

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
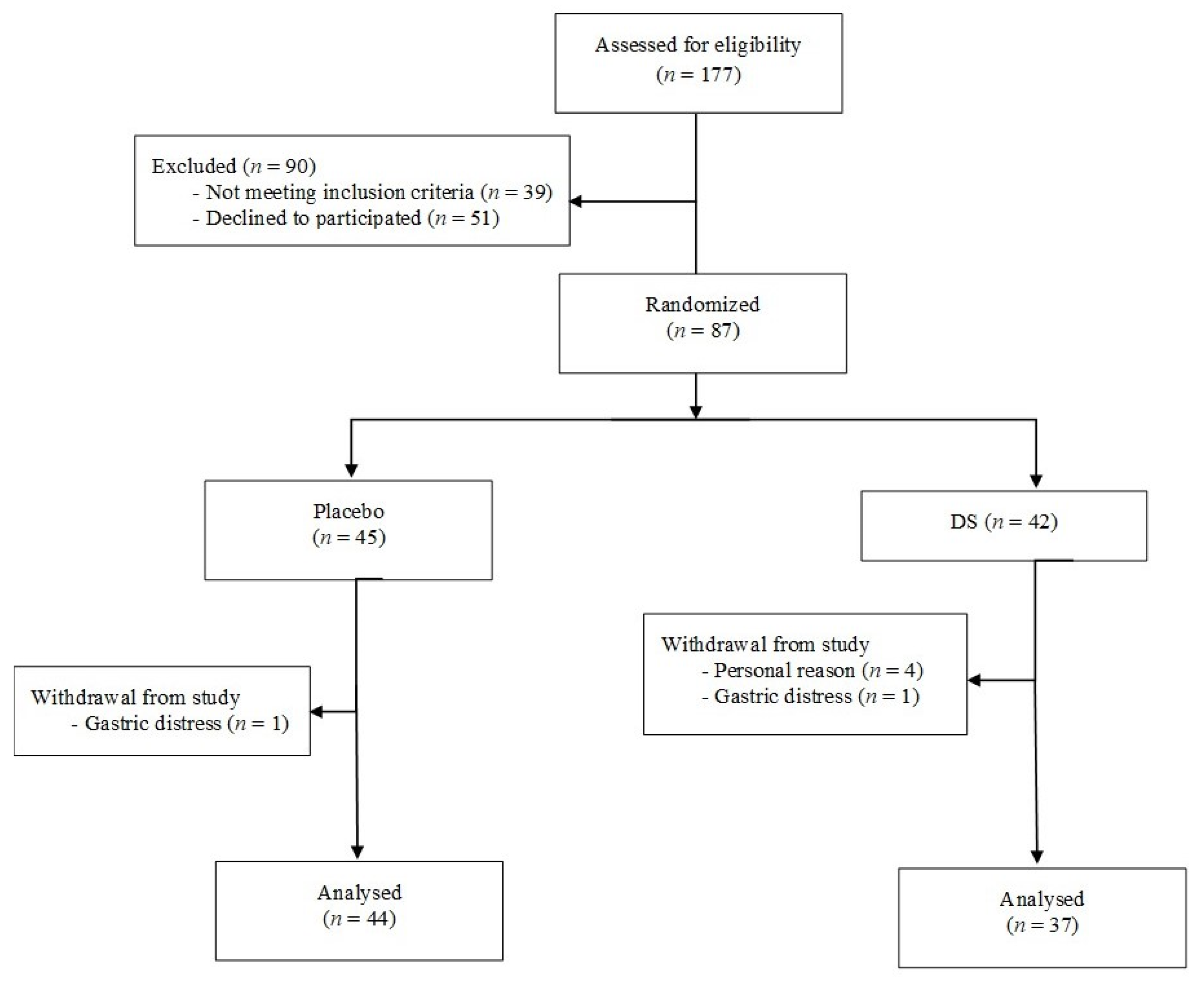
2.1. Study Population
2.2. Study Design and Protocol
2.3. Outcomes
2.4. Safety Evaluation
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
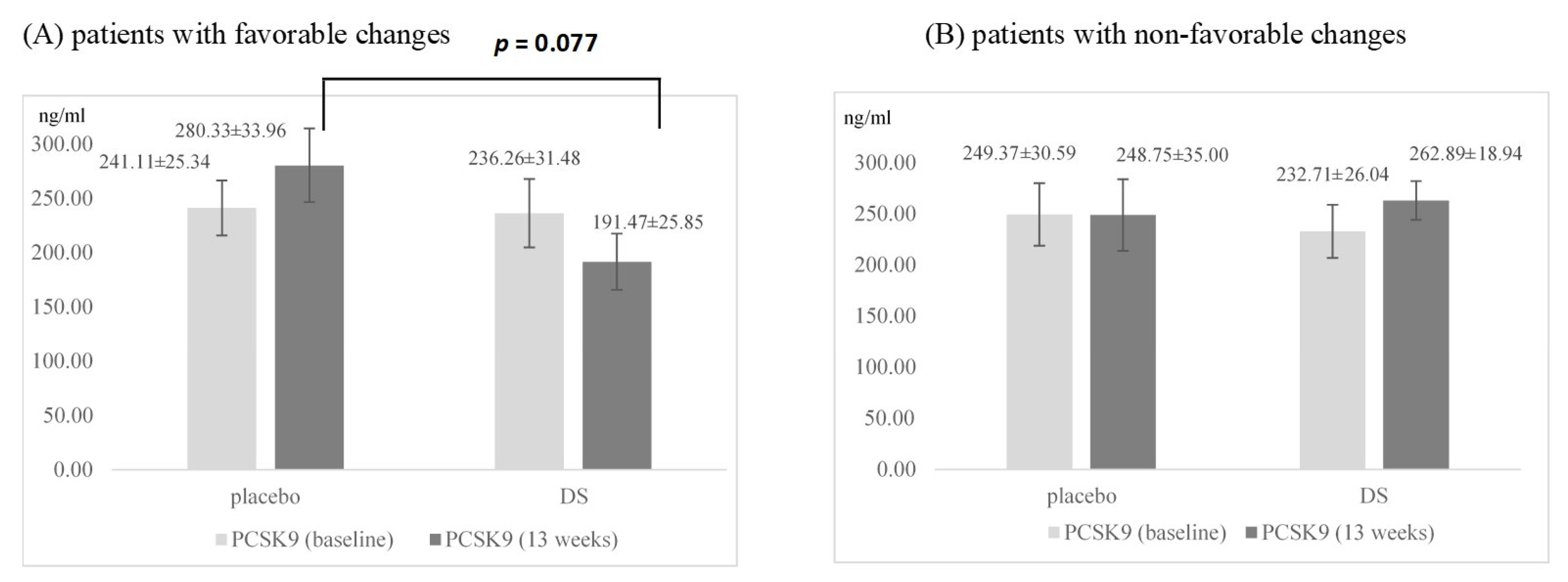
3.2. Effects on PCSK9 and Lipids Parameters
3.3. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gong, J.; Qin, X.; Yuan, F.; Hu, M.; Chen, G.; Fang, K.; Wang, D.; Jiang, S.; Li, J.; Zhao, Y.; et al. Efficacy and Safety of Sugarcane Policosanol on Dyslipidemia: A Meta-Analysis of Randomized Controlled Trials. Mol. Nutr. Food Res. 2018, 62. [Google Scholar] [CrossRef]
- Backes, J.M.; Gibson, C.A.; Ruisinger, J.F.; Moriarty, P.M. Modified-Policosanol Does Not Reduce Plasma Lipoproteins in Hyperlipidemic Patients When Used Alone or in Combination with Statin Therapy. Lipids 2011, 46, 923–929. [Google Scholar] [CrossRef] [PubMed]
- Berthold, H.K.; Unverdorben, S.; Degenhardt, R.; Bulitta, M.; Gouni-Berthold, I. Effect of Policosanol on Lipid Levels Among Patients With Hypercholesterolemia or Combined Hyperlipidemia: A Randomized Controlled Trial. JAMA 2006, 295, 2262–2269. [Google Scholar] [CrossRef] [PubMed]
- Cubeddu, L.X.; Cubeddu, R.J.; Heimowitz, T.; Restrepo, B.; Lamas, G.A.; Weinberg, G.B. Comparative Lipid-Lowering Effects of Policosanol and Atorvastatin: A Randomized, Parallel, Double-Blind, Placebo-Controlled Trial. Am. Heart J. 2006, 152, 982.e1. [Google Scholar] [CrossRef] [PubMed]
- Francini-Pesenti, F.; Beltramolli, D.; Dall’acqua, S.; Brocadello, F. Effect of Sugar Cane Policosanol on Lipid Profile in Primary Hypercholesterolemia. Phytother. Res. 2008, 22, 318–322. [Google Scholar] [CrossRef]
- Greyling, A.; De Witt, C.; Oosthuizen, W.; Jerling, J.C. Effects of a Policosanol Supplement on Serum Lipid Concentrations in Hypercholesterolaemic and Heterozygous Familial Hypercholesterolaemic Subjects. Br. J. Nutr. 2006, 95, 968–975. [Google Scholar] [CrossRef]
- Catapano, A.L.; Graham, I.; De Backer, G.; Wiklund, O.; Chapman, M.J.; Drexel, H.; Hoes, A.W.; Jennings, C.S.; Landmesser, U.; Pedersen, T.R.; et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias. Eur. Heart J. 2016, 37, 2999–3058. [Google Scholar] [CrossRef]
- Abifadel, M.; Varret, M.; Rabès, J.-P.; Allard, D.; Ouguerram, K.; Devillers, M.; Cruaud, C.; Benjannet, S.; Wickham, L.; Erlich, D.; et al. Mutations in PCSK9 Cause Autosomal Dominant Hypercholesterolemia. Nat. Genet. 2003, 34, 154–156. [Google Scholar] [CrossRef]
- Lagace, T.A. PCSK9 and LDLR Degradation: Regulatory Mechanisms in Circulation and in Cells. Curr. Opin. Lipidol. 2014, 25, 387–393. [Google Scholar] [CrossRef]
- Careskey, H.E.; Davis, R.A.; Alborn, W.E.; Troutt, J.S.; Cao, G.; Konrad, R.J. Atorvastatin Increases Human Serum Levels of Proprotein Convertase Subtilisin/Kexin Type 9. J. Lipid Res. 2008, 49, 394–398. [Google Scholar] [CrossRef]
- Welder, G.; Zineh, I.; Pacanowski, M.A.; Troutt, J.S.; Cao, G.; Konrad, R.J. High-Dose Atorvastatin Causes a Rapid Sustained Increase in Human Serum PCSK9 and Disrupts Its Correlation with LDL Cholesterol. J. Lipid Res. 2010, 51, 2714–2721. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.-L.; Xu, R.-X.; Zhu, C.-G.; Wu, N.-Q.; Cui, Z.-P.; Li, J.-J. Policosanol Attenuates Statin-Induced Increases in Serum Proprotein Convertase Subtilisin/Kexin Type 9 When Combined with Atorvastatin. Evid. Based Complement. Alternat. Med. 2014, 2014, 926087. [Google Scholar] [CrossRef] [PubMed]
- Momtazi, A.A.; Banach, M.; Pirro, M.; Katsiki, N.; Sahebkar, A. Regulation of PCSK9 by Nutraceuticals. Pharmacol. Res. 2017, 120, 157–169. [Google Scholar] [CrossRef]
- Adorni, M.P.; Zimetti, F.; Lupo, M.G.; Ruscica, M.; Ferri, N. Naturally Occurring PCSK9 Inhibitors. Nutrients 2020, 12, 1440. [Google Scholar] [CrossRef] [PubMed]
- Fogacci, F.; Grassi, D.; Rizzo, M.; Cicero, A.F.G. Metabolic Effect of Berberine-Silymarin Association: A Meta-Analysis of Randomized, Double-Blind, Placebo-Controlled Clinical Trials. Phytother. Res. 2019, 33, 862–870. [Google Scholar] [CrossRef]
- Li, H.; Dong, B.; Park, S.W.; Lee, H.-S.; Chen, W.; Liu, J. Hepatocyte Nuclear Factor 1alpha Plays a Critical Role in PCSK9 Gene Transcription and Regulation by the Natural Hypocholesterolemic Compound Berberine. J. Biol. Chem. 2009, 284, 28885–28895. [Google Scholar] [CrossRef] [PubMed]
- Tai, M.-H.; Chen, P.-K.; Chen, P.-Y.; Wu, M.-J.; Ho, C.-T.; Yen, J.-H. Curcumin Enhances Cell-Surface LDLR Level and Promotes LDL Uptake through Downregulation of PCSK9 Gene Expression in HepG2 Cells. Mol. Nutr. Food Res. 2014, 58, 2133–2145. [Google Scholar] [CrossRef] [PubMed]
- Nozue, T. Lipid Lowering Therapy and Circulating PCSK9 Concentration. J. Atheroscler. Thromb. 2017, 24, 895–907. [Google Scholar] [CrossRef]
- Gouni-Berthold, I.; Berthold, H.K. PCSK9 Antibodies for the Treatment of Hypercholesterolemia. Nutrients 2014, 6, 5517–5533. [Google Scholar] [CrossRef] [PubMed]
- Leander, K.; Mälarstig, A.; van’t Hooft, F.M.; Hyde, C.; Hellénius, M.L.; Troutt, J.S.; de Faire, U. Convertase Subtilisin/Kexin Type 9 (PCSK9) Predicts Future Risk of Cardiovascular Events Independently of Established Risk Factors. Circulation 2016, 133, 1230–1239. [Google Scholar] [CrossRef] [PubMed]
- Liberale, L.; Carbone, F.; Bertolotto, M.; Bonaventura, A.; Vecchié, A.; Mach, F.; Burger, F.; Pende, A.; Spinella, G.; Pane, B.; et al. Serum PCSK9 Levels Predict the Occurrence of Acute Coronary Syndromes in Patients with Severe Carotid Artery Stenosis. Int. J. Cardiol. 2018, 263, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Rifai, N.; Bradwin, G.; Rose, L. Plasma Proprotein Convertase Subtilisin/Kexin Type 9 Levels and the Risk of First Cardiovascular Events. Eur. Heart J. 2016, 37, 554–560. [Google Scholar] [CrossRef]
- Gencer, B.; Montecucco, F.; Nanchen, D.; Carbone, F.; Klingenberg, R.; Vuilleumier, N.; Aghlmandi, S.; Heg, D.; Räber, L.; Auer, R.; et al. Prognostic Value of PCSK9 Levels in Patients with Acute Coronary Syndromes. Eur. Heart J. 2016, 37, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.K.; Wright, R.S.; Kallend, D.; Koenig, W.; Leiter, L.A.; Raal, F.J.; Bisch, J.A.; Richardson, T.; Jaros, M.; Wijngaard, P.L.J.; et al. Two Phase 3 Trials of Inclisiran in Patients with Elevated LDL Cholesterol. N. Engl. J. Med. 2020, 382, 1507–1519. [Google Scholar] [CrossRef]
- National Clinical Guideline Centre (UK). Lipid Modification: Cardiovascular Risk Assessment and the Modification of Blood Lipids for the Primary and Secondary Prevention of Cardiovascular Disease; National Institute for Health and Clinical Excellence: Guidance; National Institute for Health and Care Excellence: London, UK, 2014.
- Berthold, H.K.; Seidah, N.G.; Benjannet, S.; Gouni-Berthold, I. Evidence from a Randomized Trial That Simvastatin, but Not Ezetimibe, Upregulates Circulating PCSK9 Levels. PLoS ONE 2013, 8, e60095. [Google Scholar] [CrossRef] [PubMed]
- Taylor, B.A.; Thompson, P.D. Statins and Their Effect on PCSK9-Impact and Clinical Relevance. Curr. Atheroscler. Rep. 2016, 18, 46. [Google Scholar] [CrossRef] [PubMed]
- Filippatos, T.D.; Kei, A.; Rizos, C.V.; Elisaf, M.S. Effects of PCSK9 Inhibitors on Other than Low-Density Lipoprotein Cholesterol Lipid Variables. J. Cardiovasc. Pharmacol. Ther. 2018, 23, 3–12. [Google Scholar] [CrossRef]
- De Castro-Orós, I.; Solà, R.; Valls, R.M.; Brea, A.; Mozas, P.; Puzo, J.; Pocoví, M. Genetic Variants of LDLR and PCSK9 Associated with Variations in Response to Antihypercholesterolemic Effects of Armolipid Plus with Berberine. PLoS ONE 2016, 11, e0150785. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef]
- De Sauvage Nolting, P.R.W.; Buirma, R.J.A.; Hutten, B.A.; Kastelein, J.J.P. Dutch ExPRESS investigators Group Baseline Lipid Values Partly Determine the Response to High-Dose Simvastatin in Patients with Familial Hypercholesterolemia. The Examination of Probands and Relatives in Statin Studies with Familial Hypercholesterolemia (ExPRESS FH). Atherosclerosis 2002, 164, 347–354. [Google Scholar] [PubMed]
- McPherson, R.; Angus, C.; Murray, P.; Genest, J. WATCH Investigators Efficacy of Atorvastatin in Achieving National Cholesterol Education Program Low-Density Lipoprotein Targets in Women with Severe Dyslipidemia and Cardiovascular Disease or Risk Factors for Cardiovascular Disease: The Women’s Atorvastatin Trial on Cholesterol (WATCH). Am. Heart J. 2001, 141, 949–956. [Google Scholar] [CrossRef] [PubMed]
- Lakoski, S.G.; Lagace, T.A.; Cohen, J.C.; Horton, J.D.; Hobbs, H.H. Genetic and Metabolic Determinants of Plasma PCSK9 Levels. J. Clin. Endocrinol. Metab. 2009, 94, 2537–2543. [Google Scholar] [CrossRef] [PubMed]
- Willems, B.A.G.; Vermeer, C.; Reutelingsperger, C.P.M.; Schurgers, L.J. The Realm of Vitamin K Dependent Proteins: Shifting from Coagulation toward Calcification. Mol. Nutr. Food Res. 2014, 58, 1620–1635. [Google Scholar] [CrossRef]
- Brandenburg, V.M.; Schurgers, L.J.; Kaesler, N.; Püsche, K.; van Gorp, R.H.; Leftheriotis, G.; Reinartz, S.; Koos, R.; Krüger, T. Prevention of Vasculopathy by Vitamin K Supplementation: Can We Turn Fiction into Fact? Atherosclerosis 2015, 240, 10–16. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients (n = 87) | Placebo (n = 45) | Dietary Supplement (n = 42) | p Value |
|---|---|---|---|---|
| Age (years) | 62.6 ± 0.8 | 61.5 ± 1.2 | 63.8 ± 1.1 | 0.165 |
| Sex | 0.806 | |||
| male | 55 (63.2) | 29 (64.4) | 26 (61.9) | |
| female | 32 (36.8) | 16 (35.6) | 16 (38.1) | |
| Body weight (kg) | 80.68 ± 1.35 | 81.05 ± 1.85 | 80.27 ± 2.00 | 0.774 |
| Height (cm) | 1.71 ± 0.01 | 1.71 ± 0.01 | 1.71 ± 0.01 | 0.773 |
| BMI (kg/m2) | 27.6 ± 0.4 | 27.8 ± 0.5 | 27.4 ± 0.6 | 0.604 |
| WC (cm) | 97.65 ± 1.08 | 98.44 ± 1.48 | 96.79 ± 1.59 | 0.446 |
| WHR | 0.92 ± 0.01 | 0.93 ± 0.01 | 0.90 ± 0.01 | 0.090 |
| Family history of | ||||
| coronary heart disease | 46 (52.9) | 26 (57.8) | 20 (47.6) | 0.343 |
| Smoker | 21 (24.1) | 11 (24.4) | 10 (23.8) | 0.945 |
| Diabetes mellitus | 23 (26.4) | 12 (26.7) | 11 (26.2) | 0.960 |
| History of hypertension | 84 (96.6) | 43 (95.6) | 41 (97.6) | 0.598 |
| Previous myocardial | ||||
| infarction | 52 (59.8) | 29 (64.4) | 23 (54.8) | 0.357 |
| Coronarography | 63 (72.4) | 33 (73.3) | 30 (71.4) | 0.843 |
| Stent | 54 (62.1) | 28 (62.2) | 26 (61.9) | 0.976 |
| Bypass | 4 (4.6) | 2 (4.4) | 2 (4.8) | 0.944 |
| Primary prevention | 20 (23.0) | 9 (20.0) | 11 (26.2) | 0.493 |
| CRP (mg/L) † | 1.44 (0.90–2.45) | 1.59 (0.88–2.45) | 1.34 (0.96–2.37) | 0.865 |
| Glucose (mmol/L) ‡ | 5.64 (5.14–6.19) | 5.62 (4.94–6.28) | 5.72 (5.19–6.18) | 0.494 |
| BP (mm Hg) | ||||
| Systolic ‡ | 130 (120–140) | 130 (120–140) | 130 (120–140) | 0.368 |
| Diastolic ‡ | 80 (80–80) | 80 (80–80) | 80 (80–80) | 0.345 |
| Cardioprotective medications | ||||
| Aspirin/clopidogrel | 77 (88.5) | 39 (86.7) | 38 (90.5) | 0.578 |
| Beta-blocker | 70 (80.5) | 38 (84.4) | 32 (76.2) | 0.332 |
| CCB | 25 (28.7) | 12 (26.7) | 13 (31.0) | 0.659 |
| ACEI/ARB | 75 (86.2) | 41 (91.1) | 34 (81.0) | 0.170 |
| Other antihypertensive | ||||
| drugs | 11 (12.6) | 4 (8.9) | 7 (16.7) | 0.275 |
| Diuretics | 41 (47.1) | 23 (51.1) | 18 (42.9) | 0.441 |
| Antianginal drugs | 40 (46.0) | 20 (44.4) | 20 (47.6) | 0.767 |
| Atorvastatin | 87 (100.0) | 45 (100.0) | 42 (100.0) | |
| TC (mmol/L) | 4.60 ± 0.12 | 4.61 ± 0.16 | 4.60 ± 0.18 | 0.944 |
| TG (mmol/L) † | 1.33 (1.20–1.47) | 1.49 (1.28–1.72) | 1.16 (1.03–1.32) | 0.012 |
| HDL-C (mmol/L) | 1.36 ± 0.04 | 1.30 ± 0.05 | 1.45 ± 0.06 | 0.053 |
| LDL-C (mmol/L) | 2.66 ± 0.10 | 2.70 ± 0.15 | 2.61 ± 0.16 | 0.685 |
| Variable | Placebo (n = 44) | Dietary Supplement (n = 37) | ANOVA (p) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | 8 Weeks | 13 Weeks | Baseline | 8 Weeks | 13 Weeks | T | S | T × S | |
| PCSK9 (ng/mL) | 245.24 ± 19.03 | 264.91 ± 14.92 | 264.54 ± 20.46 | 233.96 ± 20.75 | 236.41 ± 16.27 | 237.80 ± 22.31 | 0.698 | 0.218 | 0.807 |
| TC (mmol/L) | 4.61 ± 0.16 | 4.53 ± 0.16 | 4.69 ± 0.16 | 4.60 ± 0.18 | 4.85 ± 0.17 | 4.84 ± 0.18 | 0.192 | 0.479 | 0.165 |
| TG (mmol/L) † | 1.49 (1.28–1.72) | 1.64 (1.43–1.87) | 1.55 (1.34–1.79) | 1.16 (1.03–1.32) | 1.35 (1.17–1.56) * | 1.20 (1.03–1.41) | 0.007 | 0.012 | 0.731 |
| HDL-C (mmol/L) | 1.30 ± 0.05 | 1.37 ± 0.05 | 1.50 ± 0.06 **,# | 1.45 ± 0.06 | 1.40 ± 0.06 | 1.47 ± 0.06 | 0.007 | 0.416 | 0.041 |
| LDL-C (mmol/L) | 2.70 ± 0.15 | 2.36 ± 0.14 * | 2.53 ± 0.16 | 2.61 ± 0.16 | 2.81 ± 0.16 | 2.73 ± 0.17 | 0.761 | 0.341 | 0.023 |
| ApoA1 (g/L) | 1.41 ± 0.04 | 1.44 ± 0.04 | 1.42 ± 0.04 | 1.48 ± 0.04 | 1.46 ± 0.04 | 1.45 ± 0.04 | 0.638 | 0.389 | 0.309 |
| ApoB100 (g/L) | 1.87 ± 0.07 | 1.86 ± 0.08 | 1.97 ± 0.08 | 1.84 ± 0.08 | 2.02 ± 0.09 * | 1.98 ± 0.09 | 0.025 | 0.632 | 0.084 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciric, M.Z.; Ostojic, M.; Baralic, I.; Kotur-Stevuljevic, J.; Djordjevic, B.I.; Markovic, S.; Zivkovic, S.; Stankovic, I. Supplementation with Octacosanol Affects the Level of PCSK9 and Restore Its Physiologic Relation with LDL-C in Patients on Chronic Statin Therapy. Nutrients 2021, 13, 903. https://doi.org/10.3390/nu13030903
Ciric MZ, Ostojic M, Baralic I, Kotur-Stevuljevic J, Djordjevic BI, Markovic S, Zivkovic S, Stankovic I. Supplementation with Octacosanol Affects the Level of PCSK9 and Restore Its Physiologic Relation with LDL-C in Patients on Chronic Statin Therapy. Nutrients. 2021; 13(3):903. https://doi.org/10.3390/nu13030903
Chicago/Turabian StyleCiric, Milica Zrnic, Miodrag Ostojic, Ivana Baralic, Jelena Kotur-Stevuljevic, Brizita I. Djordjevic, Stana Markovic, Stefan Zivkovic, and Ivan Stankovic. 2021. "Supplementation with Octacosanol Affects the Level of PCSK9 and Restore Its Physiologic Relation with LDL-C in Patients on Chronic Statin Therapy" Nutrients 13, no. 3: 903. https://doi.org/10.3390/nu13030903
APA StyleCiric, M. Z., Ostojic, M., Baralic, I., Kotur-Stevuljevic, J., Djordjevic, B. I., Markovic, S., Zivkovic, S., & Stankovic, I. (2021). Supplementation with Octacosanol Affects the Level of PCSK9 and Restore Its Physiologic Relation with LDL-C in Patients on Chronic Statin Therapy. Nutrients, 13(3), 903. https://doi.org/10.3390/nu13030903