
The Christian Orthodox Church Fasting Diet Is Associated with Lower Levels of Depression and Anxiety and a Better Cognitive Performance in Middle Life

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
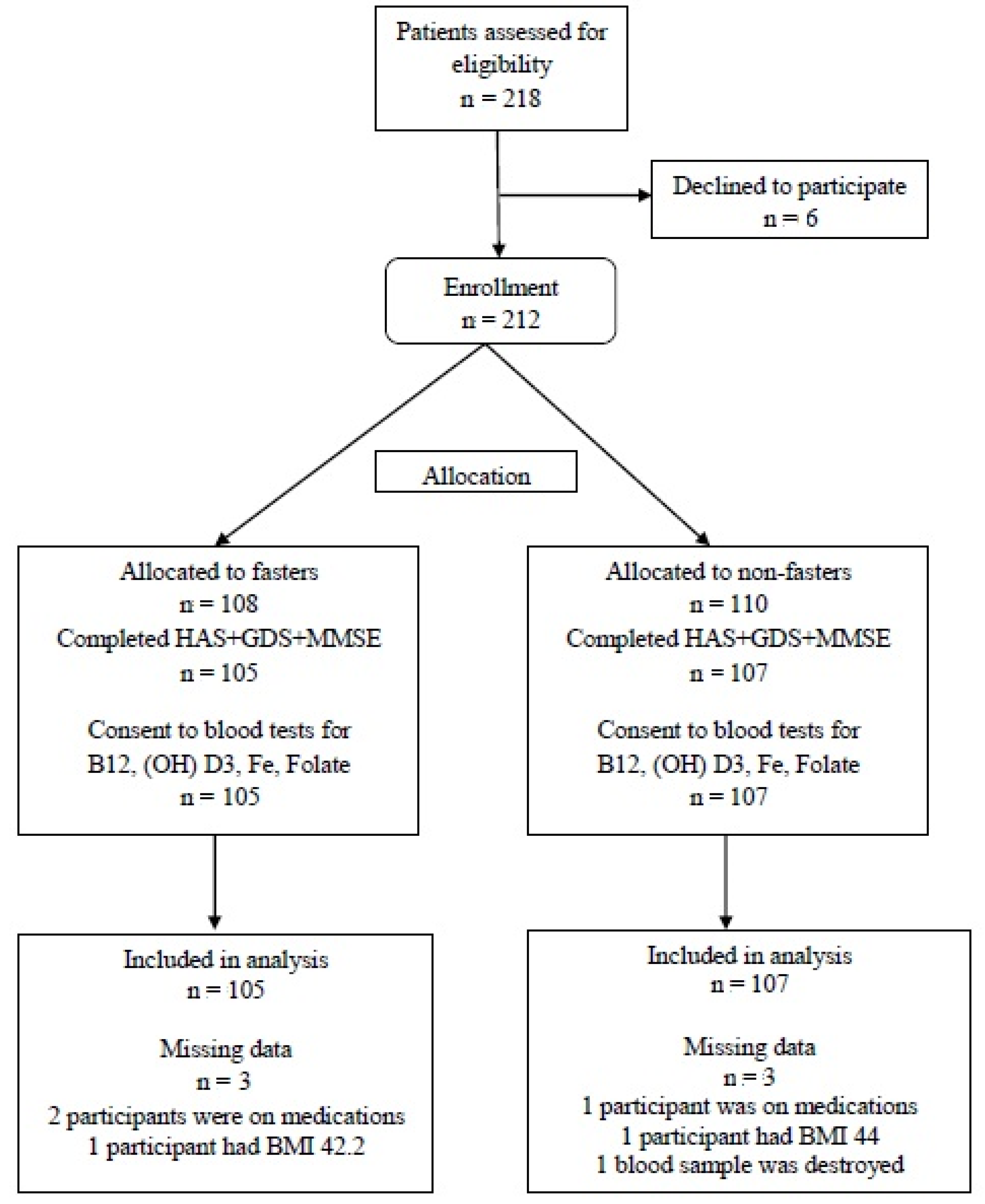
2.1. Subjects
2.2. Study Design
2.3. Dietary Data
2.4. Mental Health Evaluation
2.5. Statistical Analysis
3. Results
3.1. Sociodemographic, Health, and Diet Characteristics
3.2. Vitamins B12, 25 (OH) D3, Folate, and Ferrum
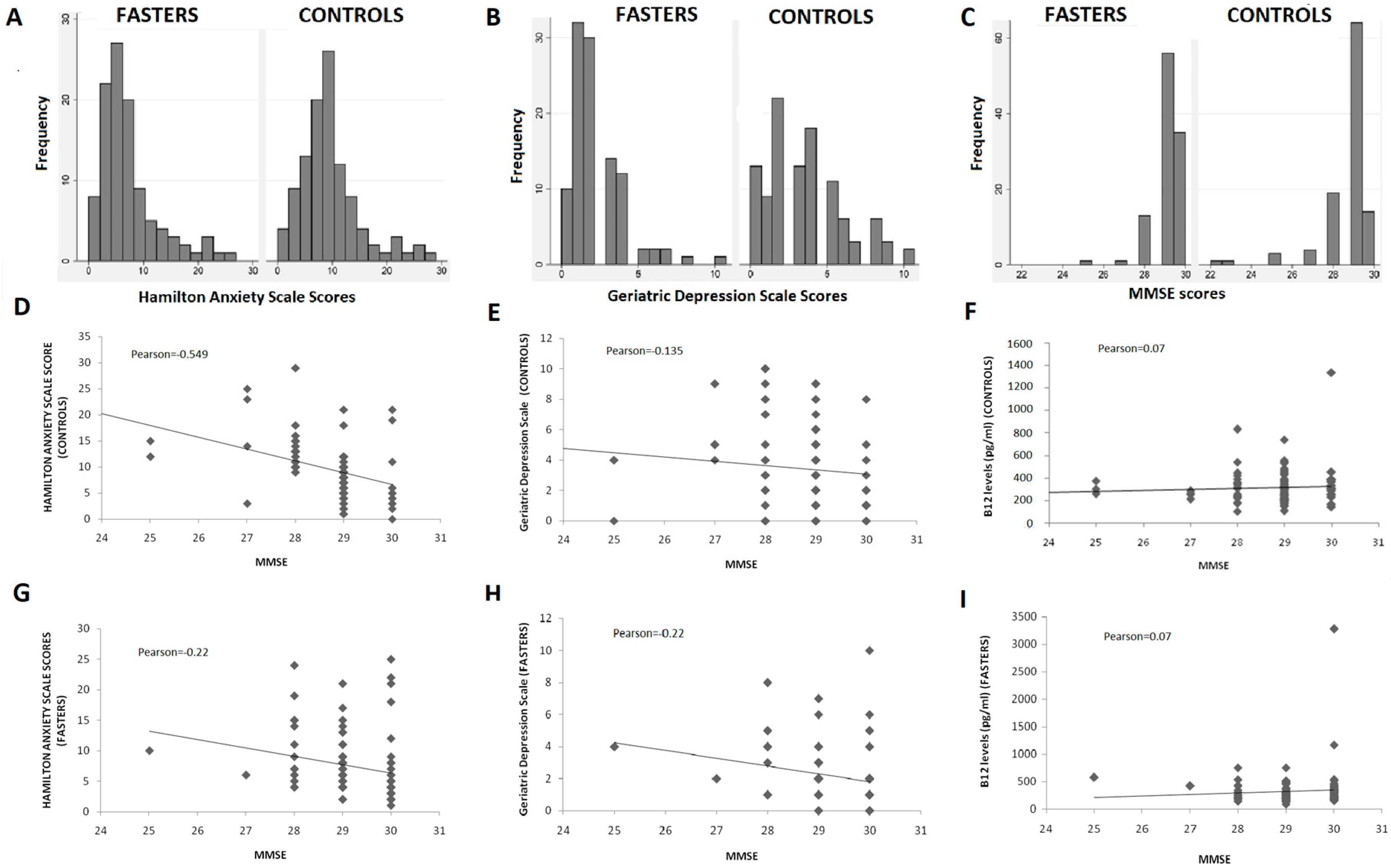
3.3. Depression and Anxiety
3.4. Cognitive Performance
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Daviglus, M.L.; Bell, C.C.; Berrettini, W.; Bowen, P.E.; Connolly, E.S.; Cox, N.J.; Dunbar-Jacob, J.M.; Granieri, E.C.; Hunt, G.; McGarry, K.; et al. NIH state-of-the-science conference statement: Preventing Alzheimer’s disease and cognitive decline. NIH Consens. State Sci. Statements 2010, 27, 1–30. [Google Scholar]
- Gill, S.S.; Seitz, D.P. Lifestyles and Cognitive Health: What Older Individuals Can Do to Optimize Cognitive Outcomes. JAMA 2015, 314, 774–775. [Google Scholar] [CrossRef]
- Vollset, S.E.; Goren, E.; Yuan, C.-W.; Cao, J.; Smith, A.E.; Hsiao, T.; Bisignano, C.; Azhar, G.S.; Castro, E.; Chalek, J.; et al. Fertility, mortality, migration, and population scenarios for 195 countries and territories from 2017 to 2100: A forecasting analysis for the Global Burden of Disease Study. Lancet 2020, 396, 1285–1306. [Google Scholar] [CrossRef]
- World Health Organization. Healthy Ageing and the Sustainable Development Goals. 2017. Available online: https://www.who.int/ageing/sdgs/en/ (accessed on 1 October 2020).
- Jacka, F.N.; Pasco, J.A.; Mykletun, A.; Williams, L.J.; Hodge, A.M.; O’Reilly, S.L.; Nicholson, G.C.; Kotowicz, M.A.; Berk, M. Association of Western and Traditional Diets with Depression and Anxiety in Women. Am. J. Psychiatry 2010, 167, 305–311. [Google Scholar] [CrossRef]
- Solfrizzi, V.; Colacicco, A.M.; D’Introno, A.; Capurso, C.; Torres, F.; Rizzo, C.; Capurso, A.; Panza, F. Dietary intake of unsaturated fatty acids and age-related cognitive decline: A 8.5-year follow-up of the Italian Longitudinal Study on Aging. Neurobiol. Aging 2006, 27, 1694–1704. [Google Scholar] [CrossRef]
- Sánchez-Villegas, A.; Verberne, L.; De Irala, J.; Ruíz-Canela, M.; Toledo, E.; Serra-Majem, L.; Martínez-González, M. Ángel Dietary Fat Intake and the Risk of Depression: The SUN Project. PLoS ONE 2011, 6, e16268. [Google Scholar] [CrossRef] [PubMed]
- Akbaraly, T.N.; Brunner, E.J.; Ferrie, J.E.; Marmot, M.G.; Kivimaki, M.; Singh-Manoux, A. Dietary pattern and depressive symptoms in middle age. Br. J. Psychiatry 2009, 195, 408–413. [Google Scholar] [CrossRef]
- Scarmeas, N.; Anastasiou, C.A.; Yannakoulia, M. Nutrition and prevention of cognitive impairment. Lancet Neurol. 2018, 17, 1006–1015. [Google Scholar] [CrossRef]
- Burlingame, B.; Dernini, S. Sustainable diets: The Mediterranean diet as an example. Public Health Nutr. 2011, 14, 2285–2287. [Google Scholar] [CrossRef] [PubMed]
- Sáez-Almendros, S.; Obrador, B.; Bach-Faig, A.; Serra-Majem, L. Environmental footprints of Mediterranean versus Western dietary patterns: Beyond the health benefits of the Mediterranean diet. Environ. Health 2013, 12, 118. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Psaltopoulou, T.; Sergentanis, T.N.; Panagiotakos, D.B.; Sergentanis, I.N.; Kosti, R.; Scarmeas, N. Mediterranean diet, stroke, cognitive impairment, and depression: A meta-analysis. Ann. Neurol. 2013, 74, 580–591. [Google Scholar] [CrossRef]
- Scarmeas, N.; Stern, Y.; Mayeux, R.; Luchsinger, J.A. Mediterranean Diet, Alzheimer Disease, and Vascular Mediation. Arch. Neurol. 2006, 63, 1709–1717. [Google Scholar] [CrossRef]
- Féart, C. Adherence to a Mediterranean Diet, Cognitive Decline, and Risk of Dementia. JAMA 2009, 302, 638–648. [Google Scholar] [CrossRef]
- Tsivgoulis, G.; Judd, S.; Letter, A.J.; Alexandrov, A.V.; Howard, G.; Nahab, F.; Unverzagt, F.W.; Moy, C.; Howard, V.J.; Kissela, B.; et al. Adherence to a Mediterranean diet and risk of incident cognitive impairment. Neurology 2013, 80, 1684–1692. [Google Scholar] [CrossRef]
- Sánchez-Villegas, A.; Martínez-González, M.A.; Estruch, R.; Salas-Salvadó, J.; Corella, D.; Covas, M.I.; Arós, F.; Romaguera, D.; Gómez-Gracia, E.; Lapetra, J.; et al. Mediterranean dietary pattern and depression: The PREDIMED randomized trial. BMC Med. 2013, 11, 208. [Google Scholar] [CrossRef]
- Godos, J.; Currenti, W.; Angelino, D.; Mena, P.; Castellano, S.; Caraci, F.; Galvano, F.; Del Rio, D.; Ferri, R.; Grosso, G. Diet and Mental Health: Review of the Recent Updates on Molecular Mechanisms. Antioxidants (Basel) 2020, 23, 346. [Google Scholar] [CrossRef] [PubMed]
- Adan, R.A.; Van Der Beek, E.M.; Buitelaar, J.K.; Cryan, J.F.; Hebebrand, J.; Higgs, S.; Schellekens, H.; Dickson, S.L. Nutritional psychiatry: Towards improving mental health by what you eat. Eur. Neuropsychopharmacol. 2019, 29, 1321–1332. [Google Scholar] [CrossRef] [PubMed]
- Sarri, K.O.; Linardakis, M.K.; Bervanaki, F.N.; Tzanakis, N.E.; Kafatos, A.G. Greek Orthodox fasting rituals: A hidden characteristic of the Mediterranean diet of Crete. Br. J. Nutr. 2004, 92, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Lazarou, C.; Matalas, A.-L. A critical review of current evidence, perspectives and research implications of diet-related traditions of the Eastern Christian Orthodox Church on dietary intakes and health consequences. Int. J. Food Sci. Nutr. 2010, 61, 739–758. [Google Scholar] [CrossRef]
- Rodopaios, N.E.; Mougios, V.; Konstantinidou, A.; Iosifidis, S.; Koulouri, A.A.; Vasara, E.; Papadopoulou, S.K.; Skepastianos, P.; Dermitzakis, E.; Hassapidou, M.; et al. Effect of periodic abstinence from dairy products for approximately half of the year on bone health in adults following the Christian Orthodox Church fasting rules for decades. Arch Osteoporos. 2019, 14, 68. [Google Scholar] [CrossRef]
- Mitchell, A.J. A meta-analysis of the accuracy of the mini-mental state examination in the detection of dementia and mild cognitive impairment. J. Psychiatr. Res. 2009, 43, 411–431. [Google Scholar] [CrossRef]
- Sheikh, J.I.; Yesavage, J.A. Geriatric Depression Scale (GDS): Recent evidence and development of a shorter version. Clin. Gerontol. J. Aging Ment. Health 1986, 5, 165–173. [Google Scholar]
- Maier, W.; Buller, R.; Philipp, M.; Heuser, I. The Hamilton Anxiety Scale: Reliability, validity and sensitivity to change in anxiety and depressive disorders. J. Affect. Disord. 1988, 14, 61–68. [Google Scholar] [CrossRef]
- Sarri, K.O.; Tzanakis, N.E.; Linardakis, M.K.; Mamalakis, G.D.; Kafatos, A.G. Effects of Greek orthodox christian church fasting on serum lipids and obesity. BMC Public Health 2003, 3, 16. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, A.; Vardavas, C.; Hatzis, C.; Kafatos, A. Calcium, nutrient and food intake of Greek Orthodox Christian monks during a fasting and non-fasting week. Public Health Nutr. 2008, 11, 1022–1029. [Google Scholar] [CrossRef]
- Koufakis, T.; Karras, S.N.; Zebekakis, P.; Kotsa, K. Orthodox religious fasting as a medical nutrition therapy for dyslipidemia: Where do we stand and how far can we go? Eur. J. Clin. Nutr. 2018, 72, 474–479. [Google Scholar] [CrossRef]
- Koufakis, T.; Karras, S.N.; Antonopoulou, V.; Angeloudi, E.; Zebekakis, P.; Kotsa, K. Effects of Orthodox religious fasting on human health: A systematic review. Eur. J. Nutr. 2017, 56, 2439–2455. [Google Scholar] [CrossRef]
- Sarri, K.O.; Kafatos, A.G.; Higgins, S. Is religious fasting related to iron status in Greek Orthodox Christians? Br. J. Nutr. 2005, 94, 198–203. [Google Scholar] [CrossRef]
- Lai, J.S.; Hiles, S.; Bisquera, A.; Hure, A.J.; McEvoy, M.; Attia, J. A systematic review and meta-analysis of dietary patterns and depression in community-dwelling adults. Am. J. Clin. Nutr. 2013, 99, 181–197. [Google Scholar] [CrossRef]
- Jacka, F.N.; Mykletun, A.; Berk, M.; Bjelland, I.; Tell, G.S. The association between habitual diet quality and the common mental disorders in community-dwelling adults: The Hordaland Health study. Psychosom. Med. 2011, 73, 483–490. [Google Scholar] [CrossRef]
- Féart, C.; Samieri, C.; Allès, B.; Barberger-Gateau, P. Potential benefits of adherence to the Mediterranean diet on cognitive health. Proc. Nutr. Soc. 2012, 72, 140–152. [Google Scholar] [CrossRef] [PubMed]
- Scarmeas, N. Physical Activity, Diet, and Risk of Alzheimer Disease. JAMA 2009, 302, 627–637. [Google Scholar] [CrossRef] [PubMed]
- Karras, S.N.; Persynaki, A.; Petróczi, A.; Barkans, E.; Mulrooney, H.; Kypraiou, M.; Tzotzas, T.; Tziomalos, K.; Kotsa, K.; Tsioudas, A.A.; et al. Health benefits and consequences of the Eastern Orthodox fasting in monks of Mount Athos: A cross-sectional study. Eur. J. Clin. Nutr. 2017, 71, 743–749. [Google Scholar] [CrossRef]
- Karras, S.N.; Koufakis, T.; Petroczi, A.; Folkerts, D.; Kypraiou, M.; Mulrooney, H.; Naughton, D.P.; Persynaki, A.; Zebekakis, P.; Skoutas, D.; et al. Christian Orthodox fasting in practice: A comparative evaluation between Greek Orthodox general pop-ulation fasters and Athonian monks. Nutrition 2019, 59, 69–76. [Google Scholar] [CrossRef]
- Mattson, M.P.; Longo, V.D.; Harvie, M. Impact of intermittent fasting on health and disease processes. Ageing Res. Rev. 2017, 39, 46–58. [Google Scholar] [CrossRef]
- Currenti, W.; Godos, J.; Castellano, S.; Mogavero, M.P.; Ferri, R.; Caraci, F.; Grosso, G.; Galvano, F. Time restricted feeding and mental health: A review of possible mechanisms on affective and cognitive disorders. Int. J. Food Sci. Nutr. 2020, 25, 1–11. [Google Scholar] [CrossRef]
- Currenti, W.; Godos, J.; Castellano, S.; Caruso, G.; Ferri, R.; Caraci, F.; Grosso, G.; Galvano, F. Association between Time Restricted Feeding and Cognitive Status in Older Italian Adults. Nutrients 2021, 13, 191. [Google Scholar] [CrossRef] [PubMed]
- European Commission. ECHI—European Core Health Indicators. Indicators and Data. 2015. Available online: https://ec.europa.eu/health/indicators/echi/list_en (accessed on 1 October 2020).
- Vlachadis, N.; Vlachadi, M.; Iliodromiti, Z.; Kornarou, E.; Vrachnis, N. Greece’s economic crisis and suicide rates: Overview and outlook. J. Epidemiol. Community Health 2014, 68, 1204–1205. [Google Scholar] [CrossRef]
- Fiske, A.; Wetherell, J.L.; Gatz, M. Depression in Older Adults. Annu. Rev. Clin. Psychol. 2009, 5, 363–389. [Google Scholar] [CrossRef]
- Heo, M.; Murphy, C.F.; Fontaine, K.R.; Bruce, M.L.; Alexopoulos, G.S. Population projection of US adults with lifetime experience of depressive disorder by age and sex from year 2005 to 2050. Int. J. Geriatr. Psychiatry 2008, 23, 1266–1270. [Google Scholar] [CrossRef]
- Meeks, T.W.; Vahia, I.V.; Lavretsky, H.; Kulkarni, G.; Jeste, D.V. A tune in “a minor” can “b major”: A review of epidemiology, illness course, and public health implications of subthreshold depression in older adults. J. Affect. Disord. 2011, 129, 126–142. [Google Scholar] [CrossRef] [PubMed]
- Bartels, S.J.; Dums, A.R.; Oxman, T.E.; Schneider, L.S.; Arean, P.A.; Alexopoulos, G.S.; Jeste, D.V. Evidence-Based Practices in Geriatric Mental Health Care. Psychiatr. Serv. 2002, 53, 1419–1431. [Google Scholar] [CrossRef]
- White, J.; Greer, K.; Russell, G.; Lalor, A.; Stolwyk, R.; Williams, C.; Brown, T.; Haines, T. Factors affecting services offered to older adults with psychological morbidity: An exploration of health pro-fessional attitudes. Aging Ment. Health 2019, 23, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Frost, R.; Beattie, A.; Bhanu, C.; Walters, K.; Ben-Shlomo, Y. Management of depression and referral of older people to psychological therapies: A systematic review of qualitative studies. Br. J. Gen. Pr. 2019, 69, e171–e181. [Google Scholar] [CrossRef]
- Rushing, N.C.; Corsentino, E.; Hames, J.L.; Sachs-Ericsson, N.; Steffens, D.C. The relationship of religious involvement indicators and social support to current and past suicidality among depressed older adults. Aging Ment. Health 2013, 17, 366–374. [Google Scholar] [CrossRef]
- Szcześniak, M.; Timoszyk-Tomczak, C. Religious Struggle and Life Satisfaction Among Adult Christians: Self-esteem as a Mediator. J. Relig. Health 2020, 59, 2833–2856. [Google Scholar] [CrossRef] [PubMed]
- Weber, S.R.; Pargament, K.I. The role of religion and spirituality in mental health. Curr. Opin. Psychiatry 2014, 27, 358–363. [Google Scholar] [CrossRef]
- Mehta, L.H.; Roth, G.S. Caloric restriction and longevity: The science and the ascetic experience. Ann. N. Y. Acad. Sci. 2009, 1172, 28–33. [Google Scholar] [CrossRef]
- Lawrence, D.; Mitrou, F.; Zubrick, S.R. Smoking and mental illness: Results from population surveys in Australia and the United States. BMC Public Health 2009, 9, 285. [Google Scholar] [CrossRef]
- Mykletun, A.; Overland, S.; Aarø, L.E.; Liabø, H.-M.; Stewart, R. Smoking in relation to anxiety and depression: Evidence from a large population survey: The HUNT study. Eur. Psychiatry 2008, 23, 77–84. [Google Scholar] [CrossRef]
- Taylor, G.M.J.; Munafò, M.R. Does smoking cause poor “metal” health? Lancet Psychiatry 2019, 6, 2–3. [Google Scholar] [CrossRef]
- Sabia, S.; Elbaz, A.; Dugravot, A.; Head, J.; Shipley, M.; Johnson, G.H.; Kivimaki, M.; Manoux, A.S. Impact of smoking on cognitive decline in early old age: The Whitehall II cohort study. Arch. Gen. Psychiatry 2012, 69, 627–635. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Fasting Group (n = 105) n (%) | Control Group (n = 107) n (%) | p-Value 1 | |||
|---|---|---|---|---|---|
| Gender | |||||
| Males | 37 (35.2%) | 33 (30.8%) | 0.496 | ||
| Females | 68 (64.8%) | 74 (69.2%) | |||
| Education | |||||
| Primary | 9 (8.6%) | 20 (18.7%) | |||
| Secondary | 39 (37.1%) | 41 (38.3%) | |||
| Tertiary | 44 (41.9%) | 39 (36.4%) | 0.098 | ||
| Postgraduate | 13 (12.4%) | 7 (6.5%) | |||
| Recent weight change | 0.808 | ||||
| Yes | 20 (19.0%) | 19 (17.8%) | |||
| No | 85 (81.0%) | 88 (82.2%) | |||
| Smoking | 4 (3.8%) | 39 (36.4%) | <0.001 | ||
| Alcohol | 0.002 | ||||
| No | 91 (86.7%) | 78 (72.9%) | |||
| Yes | 14 (13.3%) | 29 (27.1%) | |||
| Physical activity 2 | 0.352 | ||||
| No | 74 (70.5%) | 69 (64.5%) | |||
| Yes | 31 (29.5%) | 38 (35.5%) | |||
| Monks | 9 (8.6%) | 0 (0.0%) | 0.002 | ||
| Mean | SD | Mean | SD | p-value 1 | |
| Age (years) | 59 | 6.6 | 58 | 6.8 | 0.177 |
| DEXA body fatness (%) | 37.7 | 11.45 | 36.3 | 9.48 | 0.095 |
| BMI (kg/m2) | 28.7 | 4.12 | 28.5 | 4.44 | 0.748 |
| Waist circumference (cm) | 96.3 | 11.82 | 95.5 | 11.80 | 0.587 |
| Waist-to-hip ratio | 0.95 | 0.107 | 0.96 | 0.112 | 0.507 |
| Fasting Group (n = 105) | Control Group (n = 107) | p-Value 1 | |||||
|---|---|---|---|---|---|---|---|
| Variable | Mean | SD | Median | Mean | SD | Median | |
| Fe (μg/mL) | 99.56 | 33.4 | 94 | 97.37 | 37 | 92 | 0.662 |
| 25 (OH) D3 (ng/mL) | 17.4 | 6.3 | 16.5 | 17.9 | 6.7 | 17.8 | 0.593 |
| B12 (pg/mL) | 330 | 327 | 2.2 | 316 | 155 | 0.9 | 0.681 |
| Folate (ng/mL) | 3.9 | 5.4 | 272 | 2.4 | 4.5 | 285 | 0.005 |
| Fasting Group (n = 105) | Control Group (n = 107) | p-Value 1 | |||||
|---|---|---|---|---|---|---|---|
| Variables | Mean | SD | Median | Mean | SD | Median | |
| GDS | 2.24 | 1.77 | 2 | 3.48 | 2.52 | 3 | <0.001 |
| HAS | 7.49 | 4.98 | 6 | 9.68 | 5.24 | 9 | <0.001 |
| MMSE | 29.15 | 0.79 | 29 | 28.64 | 1.26 | 29 | <0.001 |
| Males | |||||||
| GDS | 1.84 | 1.44 | 2 | 3.21 | 2.20 | 3 | 0.007 |
| HAS | 5.86 | 3.37 | 5 | 7.82 | 4.25 | 8 | 0.016 |
| MMSE | 29.35 | 0.68 | 29 | 28.94 | 0.93 | 29 | 0.037 |
| Females | |||||||
| GDS | 2.43 | 1.90 | 2 | 3.63 | 2.66 | 3 | 0.003 |
| HAS | 8.35 | 5.48 | 7 | 10.56 | 5.46 | 9 | 0.002 |
| MMSE | 29.04 | 0.83 | 29 | 28.51 | 1.38 | 29 | 0.003 |
| Model 1 1 | Model 2 1 | Model 3 1 | Model 4 1 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IRR | 95% CI | p-Value | IRR | 95% CI | p-Value | IRR | 95% CI | p-Value | IRR | 95% CI | p-Value | |
| Group | ||||||||||||
| Control (ref) | - | - | - | - | - | - | - | - | - | - | - | - |
| Fasting | 0.64 | 0.52–0.79 | <0.001 | 0.67 | 0.55–0.81 | <0.001 | 0.66 | 0.54–0.81 | <0.001 | 0.69 | 0.56–0.85 | <0.001 |
| Sex | ||||||||||||
| Males (ref) | - | - | - | - | - | - | - | - | - | |||
| Females | 1.18 | 0.96–1.45 | 0.108 | 1.14 | 0.93–1.38 | 0.206 | 1.14 | 0.93–1.39 | 0.205 | |||
| Age (years) | 1.01 | 1.00–1.03 | 0.123 | 1.01 | 1.00–1.03 | 0.075 | 1.01 | 1.00–1.03 | 0.089 | |||
| Education | ||||||||||||
| Primary (ref) | - | - | - | - | - | - | - | - | - | |||
| Secondary | 0.85 | 0.63–1.14 | 0.284 | 0.91 | 0.68–1.22 | 0.528 | 0.90 | 0.67–1.20 | 0.463 | |||
| Tertiary | 0.87 | 0.63–1.20 | 0.393 | 0.95 | 0.69–1.31 | 0.767 | 0.96 | 0.70–1.31 | 0.800 | |||
| Postgraduate | 0.63 | 0.38–1.02 | 0.061 | 0.68 | 0.42–1.09 | 0.109 | 0.66 | 0.41–1.06 | 0.087 | |||
| DEXA body fatness (%) | 1.00 | 0.99–1.01 | 0.945 | 1.00 | 0.99–1.01 | 0.986 | ||||||
| Recent weight change | ||||||||||||
| No (ref) | - | - | - | - | - | - | ||||||
| Yes | 1.49 | 1.17–1.89 | 0.001 | 1.50 | 1.19–1.89 | 0.001 | ||||||
| Physical activity 2 | ||||||||||||
| No (ref) | - | - | - | - | - | - | ||||||
| Yes | 0.83 | 0.66–1.03 | 0.092 | 0.82 | 0.66–1.02 | 0.071 | ||||||
| Smoking | ||||||||||||
| No (ref) | - | - | - | - | - | - | ||||||
| Yes | 1.01 | 0.76–1.35 | 0.928 | 1.01 | 0.76–1.34 | 0.961 | ||||||
| Monks | ||||||||||||
| No (ref) | - | - | - | |||||||||
| Yes | 0.54 | 0.30–0.96 | 0.034 | |||||||||
| Model 1 1 | Model 2 1 | Model 3 1 | Model 4 1 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IRR | 95% CI | p | IRR | 95% CI | p | IRR | 95% CI | p | IRR | 95% CI | p | |
| Group | ||||||||||||
| Control (ref) | - | - | - | - | - | - | - | - | - | - | - | - |
| Fasting | 0.90 | 0.76–1.06 | 0.206 | 0.89 | 0.75–1.06 | 0.188 | 0.92 | 0.77–1.09 | 0.333 | 0.92 | 0.77–1.10 | 0.367 |
| Sex | ||||||||||||
| Males (ref) | - | - | - | - | - | - | - | - | - | |||
| Females | 1.11 | 0.95–1.31 | 0.183 | 1.09 | 0.95–1.26 | 0.231 | 1.09 | 0.94–1.26 | 0.269 | |||
| Age (years) | 1.00 | 0.99–1.01 | 0.731 | 1.00 | 0.98–1.01 | 0.525 | 1.00 | 0.98–1.01 | 0.535 | |||
| Education | ||||||||||||
| Primary (ref) | - | - | - | - | - | - | - | - | - | |||
| Secondary | 0.96 | 0.77–1.21 | 0.744 | 0.94 | 0.75–1.18 | 0.597 | 0.94 | 0.75–1.18 | 0.600 | |||
| Tertiary | 0.98 | 0.77–1.24 | 0.865 | 0.93 | 0.73–1.19 | 0.569 | 0.94 | 0.73–1.19 | 0.590 | |||
| Postgraduate | 0.99 | 0.68–1.45 | 0.976 | 1.01 | 0.71–1.43 | 0.945 | 1.01 | 0.71–1.43 | 0.971 | |||
| DEXA body fatness (%) | 1.01 | 1.00–1.01 | 0.080 | 1.01 | 1.00–1.01 | 0.083 | ||||||
| Recent weight change | ||||||||||||
| No (ref) | - | - | - | - | - | - | ||||||
| Yes | 1.10 | 0.92–1.31 | 0.303 | 1.10 | 0.92–1.31 | 0.308 | ||||||
| Physical activity 2 | ||||||||||||
| No (ref) | - | - | - | - | - | - | ||||||
| Yes | 1.09 | 0.92–1.29 | 0.324 | 1.08 | 0.92–1.28 | 0.345 | ||||||
| Smoking | ||||||||||||
| No (ref) | - | - | - | - | - | - | ||||||
| Yes | 1.02 | 0.83–1.25 | 0.859 | 1.02 | 0.83–1.25 | 0.856 | ||||||
| Monks | ||||||||||||
| No (ref) | - | - | - | |||||||||
| Yes | 0.91 | 0.75–1.10 | 0.333 | |||||||||
| Mean | SD | Median | Skewness | |
|---|---|---|---|---|
| GDS score | 2.86 | 2.27 | 2.00 | 1.09 |
| 0–5 (no symptoms): n = 186 (87.7%) | ||||
| 6–10 (mild depression): n = 26 (12.3%) | ||||
| HAS score | 8.59 | 5.23 | 7.50 | 1.33 |
| 0–17 (mild severity): n = 195 (92.0%) | ||||
| 18–24 (mild to moderate): n = 13 (6.1%) | ||||
| 25–30 (moderate to severe): n = 4 (1.9%) | ||||
| MMSE score | 28.90 | 1.08 | 29.00 | −2.84 |
| <24 (low cognition): n = 2 (0.9%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spanaki, C.; Rodopaios, N.E.; Koulouri, A.; Pliakas, T.; Papadopoulou, S.K.; Vasara, E.; Skepastianos, P.; Serafeim, T.; Boura, I.; Dermitzakis, E.; et al. The Christian Orthodox Church Fasting Diet Is Associated with Lower Levels of Depression and Anxiety and a Better Cognitive Performance in Middle Life. Nutrients 2021, 13, 627. https://doi.org/10.3390/nu13020627
Spanaki C, Rodopaios NE, Koulouri A, Pliakas T, Papadopoulou SK, Vasara E, Skepastianos P, Serafeim T, Boura I, Dermitzakis E, et al. The Christian Orthodox Church Fasting Diet Is Associated with Lower Levels of Depression and Anxiety and a Better Cognitive Performance in Middle Life. Nutrients. 2021; 13(2):627. https://doi.org/10.3390/nu13020627
Chicago/Turabian StyleSpanaki, Cleanthe, Nikolaos E. Rodopaios, Alexandra Koulouri, Triantafyllos Pliakas, Sousana K. Papadopoulou, Eleni Vasara, Petros Skepastianos, Tatiana Serafeim, Iro Boura, Emmanouil Dermitzakis, and et al. 2021. "The Christian Orthodox Church Fasting Diet Is Associated with Lower Levels of Depression and Anxiety and a Better Cognitive Performance in Middle Life" Nutrients 13, no. 2: 627. https://doi.org/10.3390/nu13020627
APA StyleSpanaki, C., Rodopaios, N. E., Koulouri, A., Pliakas, T., Papadopoulou, S. K., Vasara, E., Skepastianos, P., Serafeim, T., Boura, I., Dermitzakis, E., & Kafatos, A. (2021). The Christian Orthodox Church Fasting Diet Is Associated with Lower Levels of Depression and Anxiety and a Better Cognitive Performance in Middle Life. Nutrients, 13(2), 627. https://doi.org/10.3390/nu13020627