
Prevalence, Trends, and Socioeconomic Determinants of Coexisting Forms of Malnutrition Amongst Children under Five Years of Age in Pakistan


Abstract
:1. Introduction
2. Materials and Methods
2.1. Datasets
2.2. Study Participants and Eligibility Criteria
2.3. Sample Size and Sampling Strategy
2.4. Data Collection Method and Data Collection Tool
2.5. Measurement of Outcome Variable
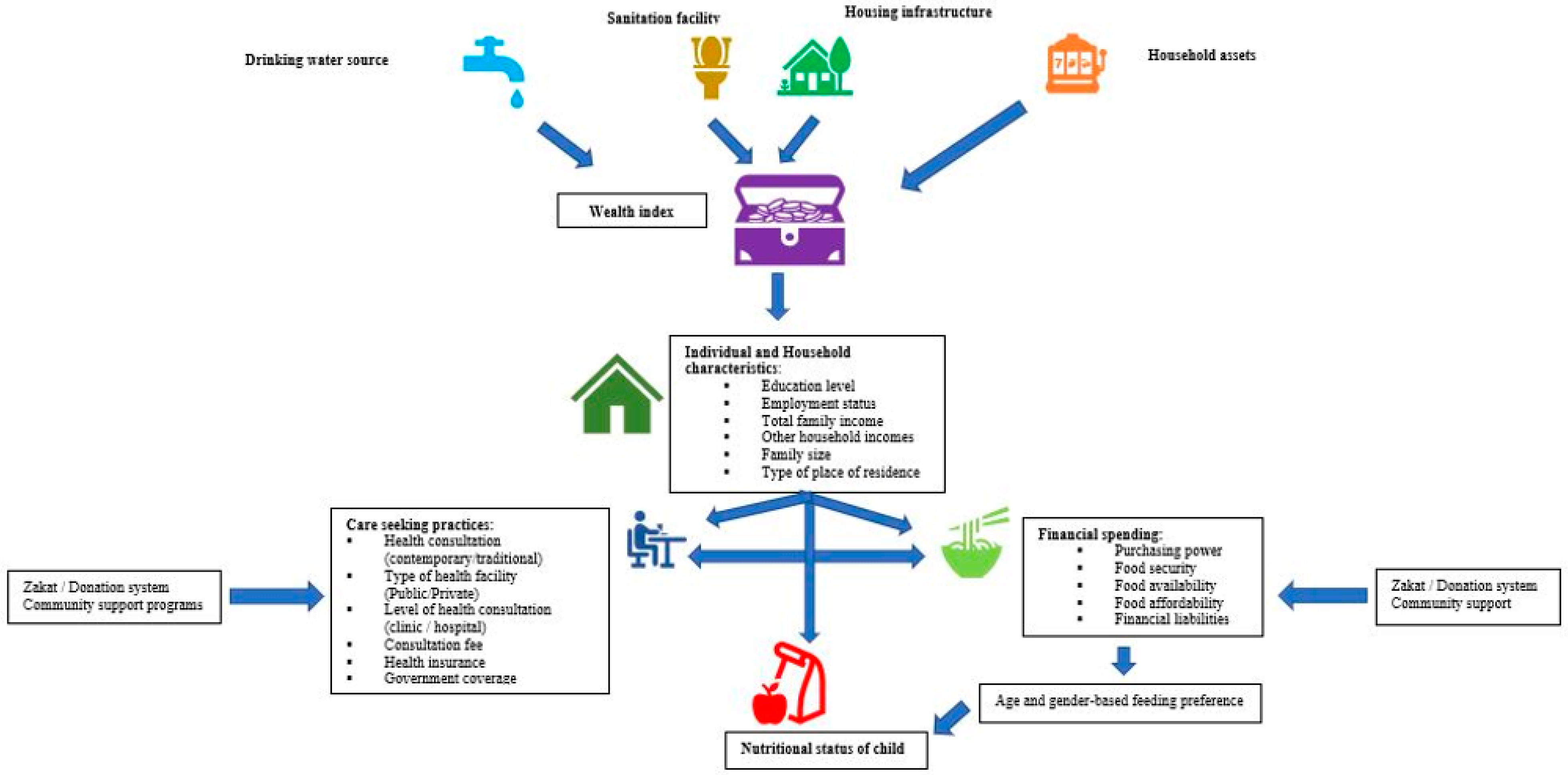
2.6. Conceptual Framework
2.7. Study Covariates
2.8. Measurement of Predictor Variable
2.9. Statistical Analysis and Inference
2.10. Ethics
3. Results
3.1. Characteristics of Study Population—PDHS 2012–2013 and PDHS 2017–2018 Datasets
3.2. National Prevalence and Trends of CFM
3.3. Regional Distribution of Various Types of Malnutrition
3.4. Determinants of Coexistence of Underweight with Wasting
3.5. Determinants of Coexistence of Underweight with Stunting
3.6. Determinants of Coexistence of Underweight with Both Stunting and Wasting
3.7. Determinants of Coexistence of Stunting with Overweight/Obesity
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cederholm, T.; Jensen, G.L.; Correia, M.I.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.J.; et al. GLIM criteria for the diagnosis of malnutrition–A consensus report from the global clinical nutrition community. J. Cachexia Sarc. Muscle 2019, 10, 207–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, T.; Hossain, M.; Sanin, K.I. Global burden of maternal and child undernutrition and micronutrient deficiencies. Ann. Nutr. Metab. 2012, 61 (Suppl. S1), 8–17. [Google Scholar] [CrossRef]
- Müller, O.; Krawinkel, M. Malnutrition and health in developing countries. Can. Med. Assoc. J. 2005, 173, 279–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.-Q.; Li, H.; Wu, H.-H.; Zong, X.-N. Stunting, wasting, overweight and their coexistence among children under 7 years in the context of the social rapidly developing: Findings from a population-based survey in nine cities of China in 2016. PLoS ONE 2021, 16, e0245455. [Google Scholar]
- Wali, N.; Agho, K.; Renzaho, A.M.N. Past drivers of and priorities for child undernutrition in South Asia: A mixed methods systematic review protocol. Syst. Rev. 2019, 8, 189. [Google Scholar] [CrossRef] [Green Version]
- Akhtar, S. Malnutrition in South Asia—A critical reappraisal. Crit. Rev. Food Sci. 2016, 56, 2320–2330. [Google Scholar] [CrossRef]
- World Health Organization. Nutrition Landscape Information System (NLIS) Country Profile Indicators: Interpretation Guide; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Popkin, B.M.; Corvalan, C.; Grummer-Strawn, L.M. Dynamics of the double burden of malnutrition and the changing nutrition reality. Lancet 2020, 395, 65–74. [Google Scholar] [CrossRef]
- Engle-Stone, R.; Guo, J.; Ismaily, S.; Addo, O.Y.; Ahmed, T.; Oaks, B.; Suchdev, P.S.; Flores-Ayala, R.; Williams, A.M. Intraindividual double burden of overweight and micronutrient deficiencies or anemia among preschool children. Am. J. Clin. Nutr. 2020, 112 (Suppl. S1), 478S–487S. [Google Scholar] [CrossRef]
- Global Nutrition Report. Pakistan Nutrition Profile. 2018. Available online: https://globalnutritionreport.org/documents/96/Pakistan.pdf (accessed on 4 May 2021).
- World Health Organization. Malnutrition–Key Facts 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/malnutrition (accessed on 4 May 2021).
- McDonald, C.M.; Olofin, I.; Flaxman, S.; Fawzi, W.W.; Spiegelman, D.; Caulfield, L.E.; Black, R.E.; Ezzati, M.; Danaei, G.; Nutrition Impact Model Study. The effect of multiple anthropometric deficits on child mortality: Meta-analysis of individual data in 10 prospective studies from developing countries. Am. J. Clin. Nutr. 2013, 97, 896–901. [Google Scholar] [CrossRef] [Green Version]
- Poirier, M.J.P.; Grépin, K.A.; Grignon, M. Approaches and alternatives to the wealth index to measure socioeconomic status using survey data: A critical interpretive synthesis. Soc. Indic. Res. 2020, 148, 1–46. [Google Scholar] [CrossRef] [Green Version]
- Rutstein, S.O.; Staveteig, S. Making the Demographic and Health Surveys Wealth Index Comparable; ICF International: Rockville, MD, USA, 2014. [Google Scholar]
- Brooks-Gunn, J.; Klebanov, P.; Liaw, F.-R.; Duncan, G. Toward an understanding of the effects of poverty upon children. In Children of Poverty; Routledge: Oxfordshire, UK, 2021; pp. 3–41. [Google Scholar]
- Siponen, S.M.; Ahonen, R.S.; Savolainen, P.H.; Hämeen-Anttila, K.P. Children’s health and parental socioeconomic factors: A population-based survey in Finland. BMC Public Health 2011, 11, 457. [Google Scholar] [CrossRef] [Green Version]
- Fernald, L.C.; Neufeld, L.M. Overweight with concurrent stunting in very young children from rural Mexico: Prevalence and associated factors. Eur. J. Clin. Nutr. 2007, 61, 623–632. [Google Scholar] [CrossRef]
- Keino, S.; Plasqui, G.; Ettyang, G.; van den Borne, B. Determinants of stunting and overweight among young children and adolescents in sub-Saharan Africa. Food Nutr. Bull. 2014, 35, 167–178. [Google Scholar] [CrossRef]
- Zhang, N.; Bécares, L.; Chandola, T. Patterns and determinants of double-burden of malnutrition among rural children: Evidence from China. PLoS ONE 2016, 11, e0158119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhruv, K.; Chokshi, D.A. Health, income, & poverty: Where we are & what could help. Health Aff. 2018, 10. [Google Scholar] [CrossRef]
- Asim, M.; Nawaz, Y. Child malnutrition in Pakistan: Evidence from literature. Children 2018, 5, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Kim, R.; Vollmer, S.; Subramanian, S.V. Factors associated with child stunting, wasting, and underweight in 35 low-and middle-income countries. JAMA Netw. Open 2020, 3, e203386. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, D.; Afzal, M.; Imtiaz, A. Effect of socioeconomic factors on malnutrition among children in Pakistan. Future Bus. J. 2020, 6, 30. [Google Scholar] [CrossRef]
- Shinsugi, C.; Gunasekara, D.; Gunawardena, N.K.; Subasinghe, W.; Miyoshi, M.; Kaneko, S.; Takimoto, H. Double burden of maternal and child malnutrition and socioeconomic status in urban Sri Lanka. PLoS ONE 2019, 14, e0224222. [Google Scholar] [CrossRef]
- Pakistan Demographic and Health Survey. Pakistan Demographic and Health Survey 2017–2018. Available online: https://dhsprogram.com/pubs/pdf/FR354/FR354.pdf (accessed on 19 October 2019).
- Mei, Z.; Grummer-Strawn, L.M. Standard deviation of anthropometric Z-scores as a data quality assessment tool using the 2006 WHO growth standards: A cross country analysis. J. Bull. World Health Organ. 2007, 85, 441–448. [Google Scholar] [CrossRef]
- World Health Organization. Recommendations for Data Collection, Analysis and Reporting on Anthropometric Indicators in Children under 5 Years Old; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- National Institute of Population Studies (NIPS). Pakistan Demographic and Health Survey 1990–1991. Available online: https://dhsprogram.com/pubs/pdf/FR29/FR29.pdf (accessed on 21 October 2019).
- Pakistan Demographic and Health Survey. Pakistan Demographic and Health Survey 2012–2013. Available online: https://dhsprogram.com/pubs/pdf/FR290/FR290.pdf (accessed on 21 October 2019).
- ClinCalc.com. Post-Hoc Power Calculator: Evaluate Statistical Power of An Existing Study. 2018. Available online: https://clincalc.com/stats/Power.aspx (accessed on 4 November 2021).
- United Nations. The Millennium Development Goals Report 2015. 2015. Available online: https://www.un.org/millenniumgoals/2015_MDG_Report/pdf/MDG%202015%20rev%20(July%201).pdf (accessed on 30 August 2021).
- The DHS Program. Demographic & Health Surveys. Wealth Index Construction. Available online: https://dhsprogram.com/topics/wealth-index/Wealth-Index-Construction.cfm (accessed on 7 January 2021).
- Myatt, M.; Khara, T.; Schoenbuchner, S.; Pietzsch, S.; Dolan, C.; Lelijveld, N.; Briend, A. Children who are both wasted and stunted are also underweight and have a high risk of death: A descriptive epidemiology of multiple anthropometric deficits using data from 51 countries. Arch. Public Health 2018, 76, 28. [Google Scholar] [CrossRef] [Green Version]
- Muhammad, H.F.L. Obesity as the Sequel of Childhood Stunting: Ghrelin and GHSR Gene Polymorphism Explained. Acta Med. Indones. 2018, 50, 159–164. [Google Scholar]
- Khaliq, A.; Wraith, D.; Nambiar-Mann, S.; Miller, Y. A Review of the Prevalence, Trends, and Determinants of Coexisting Forms of Malnutrition. BMC Public Health 2021, 1–21. [Google Scholar] [CrossRef]
- Global Nutrition Report. Global Overview: Malnutrition Burden: Global Nutrition Report. 2019. Available online: https://globalnutritionreport.org/resources/nutrition-profiles/ (accessed on 18 August 2020).
- Global Nutrition Report. The Burden of Malnutrition 2018. Available online: https://globalnutritionreport.org/reports/global-nutrition-report-2018/burden-malnutrition/ (accessed on 18 August 2020).
- Islam, M.S.; Biswas, T. Prevalence and correlates of the composite index of anthropometric failure among children under 5 years old in Bangladesh. Matern. Child. Nutr. 2020, 16, e12930. [Google Scholar] [CrossRef] [Green Version]
- da Silva Ferreira, H. Anthropometric assessment of children’s nutritional status: A new approach based on an adaptation of Waterlow’s classification. BMC Pediatr. 2020, 20, 65. [Google Scholar]
- Bhutta, Z.A.; Black, R.E. Global maternal, newborn, and child health—so near and yet so far. N. Engl. J. Med. 2013, 369, 2226–2235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- World Health Organization. Global Health Observatory (GHO) Data Child Mortality and Causes of Death l Under-Five Mortality. 2018. Available online: https://www.who.int/gho/child_health/mortality/mortality_under_five/en/ (accessed on 27 March 2020).
- Hossain, F.B.; Shawon, M.S.R.; Al-Abid, M.S.U.; Mahmood, S.; Adhikary, G.; Bulbul, M.M.I. Double burden of malnutrition in children aged 24 to 59 months by socioeconomic status in five South Asian countries: Evidence from demographic and health surveys. BMJ Open 2020, 10, e032866. [Google Scholar] [CrossRef] [Green Version]
- Zahid Khan, A.; Rafique, G.; Qureshi, H.; Halai Badruddin, S. A nutrition education intervention to combat undernutrition: Experience from a developing country. Int. Sch. Res. Not. 2013, 2013, 210287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, A. Current Status of Malnutrition and Stunting in Pakistani Children: What Needs to Be Done? J. Am. Coll. Nutr. 2021, 40, 180–192. [Google Scholar] [CrossRef]
- Zhou, D.; Shah, T.; Ali, S.; Ahmad, W.; Din, I.U.; Ilyas, A. Factors affecting household food security in rural northern hinterland of Pakistan. J. Saudi Soc. Agric. Sci. 2019, 18, 201–210. [Google Scholar]
- Khan, M.H.; Zerby, J.A. The socioeconomic position of Pakistan in the third world. Pak. Dev. Rev. 1981, 20, 347–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Majid, H.; Siegmann, K.A. The Effects of Growth on Women’s Employment in Pakistan. Fem. Econ. 2021, 27, 29–61. [Google Scholar] [CrossRef]
- Siegmann, K.A.; Majid, H. Empowering growth in Pakistan? Indian J. Labour Econ. 2021, 64, 309–331. [Google Scholar] [CrossRef]
- Bashir, D.; Ahmad, T.; Hidayat, T. Causes of Unemployment among Highly Educated Women in Pakistan: A Case Study of Bahawalnagar District. Pak. J. Humanit. Soc. Sci. 2013, 1, 1–10. [Google Scholar] [CrossRef]
- Kirsch, T.D.; Wadhwani, C.; Sauer, L.; Doocy, S.; Catlett, C. Impact of the 2010 Pakistan floods on rural and urban populations at six months. PLoS Curr. 2012, 4, 4. [Google Scholar] [CrossRef]
- Hashmi, H.N.; Siddiqui, Q.T.M.; Ghumman, A.R.; Kamal, M.A. A critical analysis of 2010 floods in Pakistan. Afr. J. Agric. Res. 2012, 7, 1054–1067. [Google Scholar]
- Schütte, S.; Kreutzmann, H. Social Vulnerability in Sindh. Recent Floods as Amplifiers of Social Crisis in Pakistan. Int. Asienforum 2012, 43, 199–221. [Google Scholar]
- Yaseen, Z.; Muzaffar, M. Extremism in Pakistan: Issues and challenges. J. Politics Int. Stud. 2018, 4, 31–42. [Google Scholar]
- Sayed, S.A.; González, P.A. Flood disaster profile of Pakistan: A review. Sci. J. Public Health 2014, 2, 144–149. [Google Scholar] [CrossRef] [Green Version]
- Di Cesare, M.; Bhatti, Z.; Soofi, S.B.; Fortunato, L.; Ezzati, M.; Bhutta, Z.A. Geographical and socioeconomic inequalities in women and children’s nutritional status in Pakistan in 2011: An analysis of data from a nationally representative survey. Lancet Glob. Health 2015, 3, e229–e239. [Google Scholar] [CrossRef] [Green Version]
- Nishtar, S.; A Bhutta, Z.; Jafar, T.H.; Ghaffar, A.; Akhtar, T.; Bengali, K.; Isa, Q.A.; Rahim, E. Health reform in Pakistan: A call to action. Lancet 2013, 381, 2291–2297. [Google Scholar] [CrossRef]
- Zaidi, S.A.; Bigdeli, M.; Langlois, E.V.; Riaz, A.; Orr, D.W.; Idrees, N.; Bump, J.B. Health systems changes after decentralisation: Progress, challenges and dynamics in Pakistan. BMJ Glob. Health 2019, 4, e001013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, S.M.; Bhutta, Z.A. Reform of primary health care in Pakistan. Lancet 2018, 392, 1375–1377. [Google Scholar] [CrossRef]
- UNICEF. Trends in Under-Five Mortality Rate in Pakistan. 2020. Available online: https://data.unicef.org/country/pak/ (accessed on 31 May 2021).
- Zaidi, S.; Bhutta, Z.; Hussain, S.S.; Rasanathan, K. Multisector governance for nutrition and early childhood development: Overlapping agendas and differing progress in Pakistan. BMJ Glob. Health 2018, 3 (Suppl. S4), e000678. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. Evaluation Report: United Nations Maternal and Child Stunting Reduction Programme in Three Target Districts in Sindh, Pakistan. Available online: https://www.unicef.org/pakistan/media/3251/file/Evaluation%20Report%20-%20United%20Nations%20Maternal%20and%20Child%20Stunting%20Reduction%20Programme.pdf (accessed on 24 August 2021).
- United Nations Children’s Funds. National Nutrition Survey 2018, Key Finding Report; UNICEF: New York, NY, USA, 2019. [Google Scholar]
- 2014 MICS-.Punjab—Key Findings Report: Monitoring the Situation of Children and Women. 2015. Available online: https://mics-surveys-prod.s3.amazonaws.com/MICS5/South%20Asia/Pakistan%20%28Punjab%29/2014/Key%20findings/Pakistan%20%28Punjab%29%202014%20MICS%20KFR_English.pdf (accessed on 24 September 2021).
- 2017–2018 MICS-.Punjab—Survey Finding Report: Monitoring the Situation of Children and Women. 2019. Available online: https://mics-surveys-prod.s3.amazonaws.com/MICS6/South%20Asia/Pakistan%20%28Punjab%29/2017-2018/Survey%20findings/MICS%20SFR_Final_English.pdf (accessed on 24 September 2021).
- 2014 MICS-Sindh. Key Findings Report: Monitoring the Situation of Children and Women. Available online: https://mics-surveys-prod.s3.amazonaws.com/MICS5/South%20Asia/Pakistan%20%28Sindh%29/2014/Key%20findings/Pakistan%202014%20MICS%20%28Sindh%29%20KFR_English.pdf (accessed on 31 July 2021).
- 2018–2019 MICS. Sindh-Survey Findings Report: Monitoring the Situation of Children and Women. 2020. Available online: https://mics-surveys-prod.s3.amazonaws.com/MICS6/South Asia/Pakistan %28Sindh%29/2018-2019/Survey findings/Pakistan 2018-19 MICS %28Sindh%29_English.pdf (accessed on 24 September 2021).
- Tokyo Nutrition for Growth Summit, Editor Tokyo Compact on Global Nutrition for Growth—Annex: Commitments 2021. Tokyo Nutrition Summit, December 2021. Available online: https://www.n4g-tokyo2021.jp/en/ (accessed on 11 December 2021).
- Integrated Food Security Phase Classification. Pakistan-Baluchistan: IPC Acute Malnutrition Analysis. Available online: http://www.ipcinfo.org/fileadmin/user_upload/ipcinfo/docs/IPC_Balochistan_AcuteMalnutrition_2019MayNov.pdf (accessed on 24 August 2021).
- Kunbher, A.D.; Ullah, S.; Alam, M. Multi-sector, nutrition-sensitive response to drought emergency in Pakistan. Field Exch. 2017, 55, 98. [Google Scholar]
- Shahzad, L.; Yasin, A. Analyzing Resilience and Food Insecurity of Drought Prone Communities of Tharparkar Desert, Pakistan. 2021. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/multi-sector_nutrition_sensitive_response_to_drought_emergency_in_pakistan.pdf (accessed on 24 September 2021).
- Talpur, M.A.; Mari, S.A. Seasonal Migration in Tharparkar District of Sindh Province, Pakistan: An In-depth Empirical Analysis. Pak. J. App. Eco. 2020. Available online: https://www.researchgate.net/publication/344725676_Seasonal_Migration_in_Tharparkar_district_of_Sindh_province_Pakistan_An_In-depth_Empirical_Analysis (accessed on 24 September 2021).
- DAWN. Women, Children in Balochistan Suffering from Malnutrition Due to Drought-Like Situation. Available online: https://www.dawn.com/news/1435348 (accessed on 24 August 2021).
- Rachmi, C.N.; Agho, K.E.; Li, M.; Baur, L.A. Stunting coexisting with overweight in 20–49-year-old Indonesian children: Prevalence, trends and associated risk factors from repeated cross-sectional surveys. Public Health Nutr. 2016, 19, 2698–2707. [Google Scholar] [CrossRef] [Green Version]
- Khan, G.N.; Turab, A.; Khan, M.I.; Rizvi, A.; Shaheen, F.; Ullah, A.; Hussain, A.; Hussain, I.; Ahmed, I.; Yaqoob, M.; et al. Prevalence and associated factors of malnutrition among children under-five years in Sindh, Pakistan: A cross-sectional study. BMC Nutr. 2016, 2, 69. [Google Scholar] [CrossRef]
- Díaz-Rodríguez, M.; Pérez-Muñoz, C.; Lendínez-de la Cruz, J.M.; Fernández-Gutiérrez, M.; Bas-Sarmiento, P.; Ferriz-Mas, B.C. Effectiveness of a multifactorial intervention in the first 1000 days of life to prevent obesity and overweight in childhood: Study protocol. Int. J. Environ. Res. Public Health 2020, 17, 2239. [Google Scholar] [CrossRef] [Green Version]
- Eshete, H.; Abebe, Y.; Loha, E.; Gebru, T.; Tesheme, T. Nutritional status and effect of maternal employment among children aged 6–59 months in Wolayta Sodo Town, Southern Ethiopia: A cross-sectional study. Ethiop. J. Health Sci. 2017, 27, 155–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez-Escamilla, R.; Bermudez, O.; Buccini, G.S.; Kumanyika, S.; Lutter, C.; Monsivais, P.; Victora, C. Nutrition disparities and the global burden of malnutrition. BMJ 2018, 361, k2252. [Google Scholar] [CrossRef] [PubMed]
- Schuftan, C. “Household purchasing-power deficit” A more operational indicator to express malnutrition. Ecol. Food Nutr. 1979, 8, 29–35. [Google Scholar] [CrossRef]
- Siddiqui, F.; Salam, R.A.; Lassi, Z.S.; Das, J.K. The intertwined relationship between malnutrition and poverty. Front. Public Health 2020, 8, 453. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | Category | PDHS 2012–2013 | PDHS 2017–2018 | Total | p-Value |
|---|---|---|---|---|---|
| Wealth index | Poorest | 639 (21.7%) | 661 (20.5%) | 1300 (21.1%) | 0.008 |
| Poorer | 583 (19.8%) | 745 (23.1%) | 1328 (21.5%) | ||
| Middle | 524 (17.8%) | 600 (18.6%) | 1124 (18.2%) | ||
| Richer | 630 (21.4%) | 619 (19.2%) | 1249 (20.2%) | ||
| Richest | 571 (19.4%) | 596 (18.5%) | 1167 (18.9%) | ||
| Sex of child | Male | 1488 (50.5%) | 1651 (51.3%) | 3139 (50.9%) | 0.548 |
| Female | 1459 (49.5%) | 1570 (48.7%) | 3029 (49.1%) | ||
| Child age in months | 0 to 11.9 months | 542 (18.4%) | 619 (19.2%) | 1161 (18.8%) | 0.053 |
| 12 to 23.9 months | 522(17.7%) | 647 (20.1%) | 1169 (19%) | ||
| 24 to 35.9 months | 636 (21.6%) | 631 (19.6%) | 1267 (20.5%) | ||
| 36 to 47.9 months | 613 (20.8%) | 673 (20.9%) | 1286 (20.8%) | ||
| 48 to 59.9 months | 634 (21.5%) | 651 (20.2%) | 1285 (20.8%) | ||
| Maternal education | No education | 1573 (53.4%) | 1650 (51.2%) | 3223 (52.3%) | <0.001 |
| Primary | 473 (16.1%) | 426 (13.2%) | 899 (14.6%) | ||
| Secondary or Higher | 901 (30.6%) | 1145 (35.5%) | 2046 (33.2%) | ||
| Maternal work status | Unemployed | 2334 (79.2%) | 2816 (87.5%) | 5152 (83.5%) | <0.001 |
| Employed | 613 (20.8%) | 403 (12.5%) | 1016 (16.5%) | ||
| Paternal education | No education | 885 (30%) | 937 (29.5%) | 1822 (29.7%) | 0.892 |
| Primary | 439 (14.9%) | 476 (15%) | 915 (14.9%) | ||
| Secondary or Higher | 1623 (55.1%) | 1766 (55.6%) | 3389 (55.3%) | ||
| Paternal work status ¥* | Unemployed | 75 (2.5%) | 93 (2.9%) | 168 (2.7%) | 0.409 |
| Employed | 2872 (97.5%) | 3128 (97.1%) | 6000 (97.3%) | ||
| Family size | 1 to 7 members | 1301 (44.1%) | 1321 (41%) | 2622 (42.5%) | 0.013 |
| 8 or more members | 1646 (55.9%) | 1900 (59%) | 3546 (57.5%) | ||
| Source of drinking water * | Improved | 2617 (88.8%) | 2907 (90.3%) | 5524 (89.6%) | 0.063 |
| Unimproved | 330 (11.2%) | 314 (7.7%) | 644 (10.4%) | ||
| Type of toilet * | Improved | 2207 (74.9%) | 2631 (81.7%) | 4839 (78.5%) | <0.001 |
| Unimproved | 740 (25.1%) | 589 (18.3%) | 1329 (21.5%) | ||
| Housing infrastructure * | Fully constructed. | 1336 (45.3%) | 1725 (53.6%) | 3061 (49.6%) | <0.001 |
| Semi-constructed | 576 (19.5%) | 662 (20.6%) | 1238 (20.1%) | ||
| Unconstructed | 1035 (35.1%) | 834 (25.9%) | 1869 (30.3%) | ||
| Region *¥ | Punjab | 920 (31.2%) | 839 (26%) | 1759 (28.5%) | <0.001 |
| Sindh | 682 (23.1%) | 754 (23.4%) | 1436 (23.3%) | ||
| Khyber Pakhtunkhwa | 532 (18.1%) | 671 (20.8%) | 1204 (19.5%) | ||
| Baluchistan | 301 (10.2%) | 465 (14.4%) | 766(12.4%) | ||
| Gilgit Baltistan | 300 (10.2%) | 269 (8.4%) | 569 (9.2%) | ||
| Islamabad | 212 (7.2%) | 223 (6.9%) | 434 (7%) | ||
| Type of place of residence | Urban | 1256 (42.6%) | 1517 (47.1%) | 2773 (45%) | <0.001 |
| Rural | 1691 (57.4%) | 1704 (52.9%) | 3395 (55%) | ||
| Year of survey | 2012–2013 | 2947 (47.8%) | - | 6168 (100%) | - |
| 2017–2018 | - | 3221 (52.2%) |
| Year | Pakistan | Punjab | Sindh | KPK | Baluchistan | GB | ICT |
|---|---|---|---|---|---|---|---|
| POR (95% CI) | POR (95% CI) | POR (95% CI) | POR (95% CI) | POR (95% CI) | POR (95% CI) | POR (95% CI) | |
| Malnutrition | |||||||
| 2012–2013 | 54.4% | 44.6% | 64.4% | 47.7% | 86% | 55.7% | 35.1% |
| (52.6 to 56.2%) | (41.3 to 47.8%) * | (60.6 to 67.9%) * | (43.3 to 51.9%) * | (81.6 to 89.7%) * | (49.8 to 61.3%) | (28.6 to 41.9%) * | |
| 2017–2018 | 43.3% | 30.3% | 51.6% | 42.8% | 64.1% | 40.5% | 25.6% |
| (41.5 to 45%) ¥ | (27.1 to 33.5%) *¥ | (47.9 to 55.2%) *¥ | (38.9 to 46.6%) | (59.5 to 68.4%) *¥ | (34.6 to 46.6%) ¥ | (19.9 to 31.8%) * | |
| Standalone forms of malnutrition | |||||||
| 2012–2013 | 23.8% | 22% | 23.3% | 22.5% | 25.6% | 33% | 20.4% |
| (20.8 to 26.7%) | (19.3 to 24.7%) | (20.1 to 26.6%) | (19 to 26.3%) | (20.7 to 30.9%) | (27.7 to 38.6%) * | (15.1% to 26.4%) | |
| 2017–2018 | 21.7% | 18.7% | 19.6% | 25.5% | 25.6% | 25.7% | 16.1% |
| (20.3 to 23.2%) | (16.1 to 21.5%) | (16.8 to 22.6%) | (22.2 to 28.9%) | (21.6 to 29.8%) | (20.5 to 31.3%) | (11.5 to 21.6%) | |
| Coexisting forms of malnutrition | |||||||
| 2012–2013 | 30.6% | 22.6% | 41.1% | 25.1% | 60.5% | 22.7% | 14.7% |
| (27.1 to 34.5%) | (19.9 to 25.4%) * | (37.3 to 44.8%) * | (21.5 to 29%) | (50.1 to 71.4%) * | (18 to 27.8%) * | (10.2 to 20.2%) * | |
| 2017–2018 | 21.5% | 11.6% | 32% | 17.3% | 38.5% | 14.9% | 9.4% |
| (20.1 to 23%) ¥ | (9.4 to 13.9%) *¥ | (28.6 to 35.4%) *¥ | (14.5 to 20.3%) ¥ | (34 to 43.1%) *¥ | (10.8 to 19.6%) | (5.9 to 14%) * | |
| Coexisting forms of undernutrition | |||||||
| 2012–2013 | 24.5% | 21.5% | 37.1% | 22.1% | 30.9% | 11.7% | 11.8% |
| (21.8 to 27.4%) | (18.9 to 24.3%) | (33.4 to 40.8%) * | (18.6 to 25.9%) | (25.7 to 36.4%) * | (8.2 to 15.8%) * | (7.8 to 16.9%) * | |
| 2017–2018 | 20.1% | 11.2% | 30.1% | 15.9% | 36.3% | 11.9% | 8.8% |
| (18.7 to 21.5%) ¥ | (9.1 to 13.5%) *¥ | (26.8 to 33.5%) *¥ | (13.2 to 18.9%) ¥ | (31.9 to 40.9%) * | (8.2 to 16.3%) * | (5.3 to 12.9%) * | |
| Coexisting forms of overnutrition (Paradox) | |||||||
| 2012–2013 | 6.1% | 1.1% | 4% | 3% | 29.6% | 11% | 2.8% |
| (5.3 to 7.1%) | (0.5 to 1.9%) * | (2.6 to 5.7%) | (1.7 to 4.8%) | (24.4 to 35.1%) * | (7.6 to 15.1%) * | (1.1 to 6.1%) | |
| 2017–2018 | 1.4% | 0.4% | 1.9% | 1.3% | 2.2% | 3.0% | 0.9% |
| (1 to 1.9%) ¥ | (0.01 to 0.1%) * | (1 to 3.1%) | (0.6 to 2.5%) | (1 to 3.9%) ¥ | (1.2 to 5.7%) ¥ | (0.1 to 3.2%) | |
| Coexistence of underweight with stunting | |||||||
| 2012–2013 | 17.2% | 16.2% | 26.5% | 14.6% | 19.9% | 8.3% | 6.2% |
| (15.8 to 18.6%) | (13.8 to 18.7%) | (23.2 to 30.2%) * | (11.7 to 17.9%) | (15.5 to 24.9%) | (5.4 to 12.1%) * | (3.3 to 10.3%) * | |
| 2017–2018 | 14.3% | 8.6% | 22.7% | 11.6% | 21.1% | 10.8% | 5.4% |
| (13.1 to 15.5%) ¥ | (6.7 to 10.7%) *¥ | (19.7 to 25.8%) * | (9.2 to 14.2%) | (17.4 to 25.1%) * | (7.3 to 15.1%) | (2.8 to 9.2%) * | |
| Coexistence of underweight with wasting | |||||||
| 2012–2013 | 2.9% | 2.7% | 3.7% | 3% | 2% | 2.3% | 3.3% |
| (2.3 to 3.6%) | (1.7 to 3.9%) | (2.3 to 5.3%) | (1.7 to 4.8%) | (0.7 to 4.2%) | (0.9 to 4.7%) | (1.3 to 6.7%) | |
| 2017–2018 | 3.1% | 1.1% | 3.3% | 3.1% | 8.8% | 0% ¥ | 2.2% |
| (2.5 to 3.8%) | (0.5 to 2%) * | (2.1 to 4.8%) | (1.9 to 4.7%) | (6.4 to 11.7%) * | (0.7 to 5.1%) | ||
| Coexistence of underweight with stunting and wasting | |||||||
| 2012–2013 | 4.4% | 2.6% | 6.9% | 4.5% | 9% | 1% | 2.4% |
| (3.7 to 5.2%) | (1.6 to 3.8%) | (5.1 to 9.1%) | (2.9 to 6.6%) | (5.9 to 12.7%) * | (0.2 to 2.8%) * | (0.7 to 5.4%) | |
| 2017–2018 | 2.7% | 1.5% | 4.1% | 1.2% | 6.5% | 1.1% | 0.9% |
| (2.1 to 3.3%) ¥ | (0.8 to 2.6%) | (2.8 to 5.7%) | (0.5 to 2.3%) ¥ | (4.3 to 9.1%) *¥ | (0.2 to 3.2%) | (0.1 to 3.2%) | |
| Year Interaction with Variables | Year * Categories | Coexistence of Underweight with Wasting ¥ | Coexistence of Underweight with Stunting ¥ | Coexistence of Underweight with Wasting and Stunting Both ¥ | Coexistence of Stunting with Overweight/Obesity ¥¥ |
|---|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | ||
| Year * Socioeconomic status | Year * Poorest | Ref | Ref | Ref | Ref |
| Year * Poorer | 2.08 (0.40 to 10.67) | 0.83 (0.19 to 3.64) | 2.77 (0.56 to 13.63) | 3.06 (0.95 to 9.83) | |
| Year * Middle | 0.76 (0.13 to 4.41) | 0.42 (0.09 to 2.02) | 0.69 (0.12 to 3.98) | 2.66 (0.77 to 9.12) | |
| Year * Richer | 2.17 (0.29 to 16.01) | 0.70 (0.11 to 4.11) | 1.17 (0.17 to 7.94) | 5.68 (1.67 to 19.30) * | |
| Year * Richest | 0.30 (0.05 to 1.79) | 0.53 (0.12 to 2.40) | 0.32 (0.03 to 2.66) | 5.27 (1.72 to 16.11) * | |
| Year * Sex | Year * Male | Ref | Ref | Ref | Ref |
| Year * Female | 1.09 (0.35 to 3.31) | 0.76 (0.28 to 2.04) | 0.61 (0.20 to 1.84) | 1.25 (0.62 to 2.51) | |
| Year * Age | Year * 0–11 mo | Ref | Ref | Ref | Ref |
| Year * 12–23 mo | 1.88 (0.27 to 12.67) | 5.65 (0.93 to 34.37) | 2.15 (0.31 to 15.28) | 0.63 (0.16 to 2.40) | |
| Year * 24–35 mo | 2.15 (0.38 to 12.14) | 1.91 (0.39 to 9.22) | 0.72 (0.12 to 4.37) | 1.63 (0.55 to 4.74) | |
| Year * 36–47 mo | 4.66 (0.68 to 31.90) | 9.80 (1.66 to 57.65) * | 3.92 (0.55 to 27.57) | 0.20 (0.05 to 0.78) * | |
| Year * 48–59 mo | 1.53 (0.30 to 7.77) | 2.42 (0.57 to 10.19) | 1.77 (0.33 to 9.53) | 0.43 (0.13 to 1.37) | |
| Year * Maternal education | Year * No education | Ref | Ref | Ref | Ref |
| Year * Primary | 1.65 (0.29 to 9.38) | 1.07 (0.23 to 4.86) | 1.00 (0.16 to 6.25) | 0.96 (0.29 to 3.22) | |
| Year * Secondary or higher | 0.48 (0.13 to 1.75) | 0.54 (0.17 to 1.65) | 0.36 (0.10 to 1.32) | 2.29 (1.07 to 4.86) * | |
| Year * Maternal working status | Year * No | Ref | Ref | Ref | Ref |
| Year * Yes | 0.46 (0.11 to 1.81) | 0.59 (0.19 to 1.86) | 0.63 (0.17 to 2.32) | 0.27 (0.03 to 2.11) | |
| Year * Paternal education | Year * No education | Ref | Ref | Ref | Ref |
| Year * Primary | 1.04 (0.13 to 8.08) | 1.55 (0.24 to 10.04) | 1.81 (0.24 to 13.14) | 0.61 (0.14 to 2.58) | |
| Year * Secondary or higher | 0.68 (0.19 to 2.37) | 0.71 (0.23 to 2.14) | 0.82 (0.24 to 2.81) | 2.32 (0.99 to 5.41) | |
| Year * Paternal working status | Year * No | Ref | Ref | Ref | Ref |
| Year * Yes | 1.81 (0.00 to inf) | 1.42 (0.00 to inf) | 1.01 (0.00 to inf) | 1.91 × 106 (1.92 × 10−286 to 1.89 × 10298) | |
| Year * Family size | Year * 1 to 7 members | Ref | Ref | Ref | Ref |
| Year * 8 or more members | 1.20 (0.39 to 3.67) | 1.34 (0.50 to 3.60) | 1.48 (0.49 to 4.47) | 0.64 (0.32 to 1.31) | |
| Year * Type of place of residence | Year * Rural | Ref | Ref | Ref | Ref |
| Year * Urban | 0.71 (0.22 to 2.25) | 0.36 (0.13 to 1.02) | 0.45 (0.14 to 1.41) | 1.69 (0.83 to 3.41) |
| Variable | Categories | Coexistence of Underweight with Wasting ¥ | Coexistence of Underweight with Stunting ¥ | Coexistence of Underweight with Wasting and Stunting Both ¥ | Coexistence of Stunting with Overweight/Obesity ¥¥ | ||||
|---|---|---|---|---|---|---|---|---|---|
| Unadjusted Odds (95% CI) | Adjusted Odds (95% CI) 1 | Unadjusted Odds (95% CI) | Adjusted Odds (95% CI) 2 | Unadjusted Odds (95% CI) | Adjusted Odds (95% CI) 3 | Unadjusted Odds (95% CI) | Adjusted Odds (95% CI) 4 | ||
| Socioeconomic status | Poorest | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Poorer | 1.15 (0.52 to 2.54) | 0.99 (0.43 to 2.23) | 0.60 (0.29 to 1.22) | 0.66 (0.31 to 1.37) | 0.61 (0.28 to 1.32) | 0.55 (0.23 to 1.27) | 0.59 (0.39 to 0.91) * | 0.50 (0.32 to 0.79) * | |
| Middle | 0.77 (0.32 to 1.86) | 0.68 (0.28 to 1.67) | 0.45 (0.21 to 0.98) * | 0.47 (0.21 to 1.05) | 0.41 (0.17 to 0.97) * | 0.34 (0.13 to 0.87) * | 0.58 (0.37 to 0.91) * | 0.48 (0.29 to 0.78) * | |
| Richer | 0.91 (0.34 to 2.36) | 0.72 (0.26 to 1.93) | 0.72 (0.31 to 1.69) | 0.67 (0.28 to 1.62) | 0.78 (0.31 to 1.94) | 0.78 (0.29 to 2.11) | 0.59 (0.37 to 0.95) * | 0.39 (0.22 to 0.66) * | |
| Richest | 0.45 (0.19 to 1.05) | 0.36 (0.15 to 0.87) * | 0.16 (0.08 to 0.34) * | 0.18 (0.08 to 0.41) * | 0.13 (0.05 to 0.32) * | 0.10 (0.04 to 0.27) * | 1.75 (1.14 to 2.67) * | 1.18 (0.70 to 1.99) | |
| Sex | Male | Ref | Ref | Ref | Ref | ||||
| Female | 1.25 (0.72 to 2.15) | 1.11 (0.68 to 1.80) | 0.74 (0.43 to 1.28) | 1.11 (0.83 to 1.48) | |||||
| Age | 0–11 mo | Ref | Ref | Ref | Ref | Ref | Ref | Ref | |
| 12–23 mo | 2.33 (1.00 to 5.42) * | 5.59 (2.55 to 12.25) * | 5.08 (2.28 to 11.29) * | 8.47 (3.55 to 20.23) * | 9.45 (3.75 to 23.78) * | 0.11 (0.06 to 0.21) * | 0.11 (0.06 to 0.21) * | ||
| 24–35 mo | 2.08 (0.88 to 4.89) | 9.42 (4.33 to 20.50) * | 8.82 (4.01 to 19.43) * | 5.88 (2.42 to 14.25) * | 5.64 (2.22 to 14.28) * | 0.16 (0.09 to 0.26) * | 0.14 (0.08 to 0.25) * | ||
| 36–47 mo | 1.60 (0.69 to 3.70) | 8.90 (4.21 to 18.82) * | 8.50 (3.96 to 18.21) * | 6.03 (2.56 to 14.17) * | 8.53 (3.36 to 21.61) * | 0.18 (0.11 to 0.29) * | 0.16 (0.09 to 0.28) * | ||
| 48–59 mo | 1.29 (0.57 to 2.87) | 6.97 (3.44 to 14.13) * | 6.22 (3.02 to 12.79) * | 3.79 (1.65 to 8.72) * | 4.52 (1.84 to 11.08) * | 0.24 (0.14 to 0.39) * | 0.22 (0.13 to 0.38) * | ||
| Maternal education | No education | Ref | Ref | Ref | Ref | ||||
| Primary | 0.45 (0.20 to 0.99) * | 0.57 (0.29 to 1.12) | 0.28 (0.12 to 0.64) * | 1.02 (0.66 to 1.57) | |||||
| Secondary and higher | 0.47 (0.25 to 0.89) * | 0.32 (0.19 to 0.56) * | 0.36 (0.19 to 0.68) * | 1.33 (0.96 to 1.84) | |||||
| Maternal working status | No | Ref | Ref | Ref | Ref | Ref | Ref | ||
| Yes | 0.55 (0.28 to 1.07) | 0.47 (0.23 to 0.95) * | 0.95 (0.55 to 1.67) | 0.82 (0.44 to 1.55) | 0.62 (0.40 to 0.95) * | 0.49 (0.31 to 0.79) * | |||
| Paternal education | No education | Ref | Ref | Ref | Ref | ||||
| Primary | 0.97 (0.38 to 2.49) | 1.06 (0.46 to 2.44) | 1.10 (0.45 to 2.72) | 0.81 (0.49 to 1.32) | |||||
| Secondary and higher | 0.67 (0.36 to 1.25) | 0.46 (0.26 to 0.78) * | 0.47 (0.25 to 0.86) * | 1.43 (1.03 to 1.98) * | |||||
| Paternal working status ∞ | No | Ref | |||||||
| Yes | 0.51 (0.25 to 1.05) | ||||||||
| Family size | 1 to 7 members | Ref | Ref | Ref | Ref | ||||
| 8 or more members | 1.14 (0.66 to 1.98) | 1.14 (0.70 to 1.85) | 1.17 (0.68 to 2.01) | 1.20 (0.89 to 1.61) | |||||
| Type of place of residence | Rural | Ref | Ref | Ref | Ref | Ref | |||
| Urban | 0.80 (0.46 to 1.38) | 0.52 (0.32 to 0.85) * | 0.92 (0.53 to 1.57) | 1.41 (1.06 to 1.88) * | 1.50 (1.04 to 2.16) * | ||||
| Survey year | 2012–2013 | Ref | Ref | Ref | Ref | Ref | |||
| 2017–2018 | 1.85 (1.06 to 3.21) | 1.43 (0.87 to 2.33) | 1.05 (0.61 to 1.82) | 0.25 (0.17 to 0.35) * | 0.22 (0.15 to 0.32) * | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khaliq, A.; Wraith, D.; Miller, Y.; Nambiar-Mann, S. Prevalence, Trends, and Socioeconomic Determinants of Coexisting Forms of Malnutrition Amongst Children under Five Years of Age in Pakistan. Nutrients 2021, 13, 4566. https://doi.org/10.3390/nu13124566
Khaliq A, Wraith D, Miller Y, Nambiar-Mann S. Prevalence, Trends, and Socioeconomic Determinants of Coexisting Forms of Malnutrition Amongst Children under Five Years of Age in Pakistan. Nutrients. 2021; 13(12):4566. https://doi.org/10.3390/nu13124566
Chicago/Turabian StyleKhaliq, Asif, Darren Wraith, Yvette Miller, and Smita Nambiar-Mann. 2021. "Prevalence, Trends, and Socioeconomic Determinants of Coexisting Forms of Malnutrition Amongst Children under Five Years of Age in Pakistan" Nutrients 13, no. 12: 4566. https://doi.org/10.3390/nu13124566
APA StyleKhaliq, A., Wraith, D., Miller, Y., & Nambiar-Mann, S. (2021). Prevalence, Trends, and Socioeconomic Determinants of Coexisting Forms of Malnutrition Amongst Children under Five Years of Age in Pakistan. Nutrients, 13(12), 4566. https://doi.org/10.3390/nu13124566