Abstract
Background: A balanced diet is an important lifestyle component and has been associated with a reduced risk of chronic diseases. Objectives: To assess dietary intake of adult residents in Luxembourg taking part in two population-based cross-sectional studies (ORISCAV-LUX, 2007–2008 and ORISCAV-LUX 2, 2016–2017). Methods: Dietary intake of the study participants (1242 in 2007/08 and 1326 in 2016/17), 25–69 years old, were evaluated using food-frequency questionnaires (134 items in 2007/2008 and 174 items in 2016/2017) according to the French ANSES-CIQUAL food composition database. Both food-group- and nutrient-based analyses were conducted. Results: Dietary patterns in ORISCAV-LUX 2, 2016–2017, were characterized by an increase in the estimated marginal means (EMM) of the intake of energy, total fat, saturated fatty acids, alcohol, and decreased EMM of total carbohydrates, magnesium, and calcium compared to 2007/08. We also observed an increased EMM of the intake of protein-rich food items and ready-to-eat foods/fast foods, together with a decreased intake of grains, dairy products, and vegetables (all p-values <0.05, linear mixed models). The intake of most micronutrients was stable or slightly increased in ORISCAV-LUX 2 vs. ORISCAV-LUX, except for the drop in magnesium and calcium, and generally met recommendations, in particular, EFSA population reference intakes (PRI), except for vitamin D. Conclusions: Though most micronutrient recommendations were met, nutrient consumption in terms of high energy, total fat, and sodium, as well as low carbohydrates, were not aligned with recommendations for balanced eating.
1. Introduction
Dietary patterns are an important nutritional and lifestyle component [1]. Poor dietary habits, such as over- or under-consumption of calories and macronutrients and a low intake of certain micronutrients or nonessential constituents, such as dietary fiber and secondary plant compounds, including carotenoids and polyphenols, have been related to several chronic noncommunicable diseases, such as cardiometabolic, neurodegenerative, and autoimmune diseases, as well as mental illnesses [1] and cancer [2]. Dietary patterns and food choices are influenced by various factors, such as age, gender, socioeconomic factors, and neurophysiological variations [3]. However, far from being fixed, these patterns might change over time at the population level due to changes in the population composition, sociodemographic factors, altered nutritional knowledge, and possibly food unavailability or inaccessibility, among others [4]. As improvements in dietary habits have been shown to be an important factor influencing overall health and all-cause mortality [5,6,7], monitoring dietary patterns is an important aspect for studying changes related to population health.
Luxembourg is characterized by a large percentage (about 50% of a total of ca. 650,000) of residents with foreign origin, possibly contributing to the diversity of eating habits [8]. Approximately 14.3% [8] of the population is 65 years old or older, a slightly higher fraction than in other European countries (12%) [9]. The country is also characterized, like many other Westernized countries, by a high prevalence of noncommunicable chronic diseases and related health conditions, potentially, although not exclusively, associated with a poor nutritional status, including prediabetes (25.6%) and diabetes (6.5%), overweight (37.3%) and obesity (20.6%), depression (21.6%), hypertension (31%), dyslipidemia (30.4%), cancer (3.6%), dementia (3.8%), cognitive impairment (26.1%), and Parkinson’s disease (0.2%) [10,11,12,13].
In Luxembourg, the dietary patterns, similar as to other Western-type diets [14], have been relatively high in saturated fat (18.4%), ready-made meals (7%), and alcohol consumption (13 L annual per capita) [15], all of which have been associated with cardiometabolic disturbances, such as a high incidence of metabolic syndrome, although this has been investigated in a cross-sectional study not adjusted for additional exposure [16]. In contrast, the Mediterranean dietary pattern, rich in unsaturated fats, whole grains, green leafy vegetables, fruits, and legumes, has been less frequently associated with various types of cancer and cardiometabolic diseases [17,18,19]. In general, dietary guidelines recommend choosing various vegetables, fruits, pulses, whole grains, and consuming a minimum amount of free sugars, processed/smoked meat, salt, and trans- and saturated fats, especially prevalent in ready-to-eat meals [20,21]. However, in Luxembourg, according to an earlier study in 2006/07, about 65% of the individuals did not reach the recommendations for dietary fiber intake [22], and about 50% did not consume five portions of 80–100 g of fruits and vegetables per day [22]. In addition, Luxembourg residents were ranked the highest meat consumers worldwide (136 kg per capita) in 2007 [23], with a large number of individuals regularly consuming ready-to-eat meals [16]. General dietary trends in the past years in most Westernized countries included tendencies for lower carbohydrate consumption [24], higher meat and processed food intake [25], but also leaning toward more organic/bio-foods [26].
Food choices, as a critical component in the overall dietary patterns, are complex and influenced by various factors [27]. One of the crucial goals of population-based longitudinal or repetitive cross-sectional studies is to monitor dietary changes to investigate food intake trends [28]. Such investigations are an important base for developing improved public health policy approaches [29]. This study was designed to investigate the changes in dietary patterns and habits concerning the intake of food groups, macro- and micronutrients, as well as non-nutrient compounds, in adult residents in Luxembourg taking part in two population-based, cross-sectional studies over the past decade (ORISCAV-LUX, 2007–2008 [8] and ORISCAV-LUX 2, 2016–2017 [30]).
2. Participants and Methods
2.1. Study Population and Design
The complete description of the study population and methods has previously been published in 2010 and 2019 [30]. Briefly, the Observation of Cardiovascular Risk Factors in Luxembourg (ORISCAV-LUX) surveys included two cross-sectional studies in adults residing in Luxembourg. In the original ORISCAV-LUX survey (2007–2008) [8], N = 1432 participants were included by a systematic random sampling procedure. In the original ORISCAV-LUX 2 survey (2016–2017) [30], N = 1558 participants were included by an initial baseline sampling plus complimentary sampling. A total of 660 individuals participated in both studies. The age ranges of the study participants in the original surveys were 18–69 years for ORISCAV-LUX and 25–79 years for ORISCAV-LUX 2.
In the present analysis, the same age ranges, 25–69 years, were retained to enable an accurate comparison between the two surveys (ORISCAV-LUX: N = 1242; ORISCAV-LUX 2: N = 1326). The participants were randomly selected based on sociodemographic attributes, including the district of residence, age, and gender. After a telephone appointment, the study participants were invited to take part in the surveys in the nearest study center from their domicile. During the study appointment, the study investigator gave the participants all the information related to the study, including the aim of the research project and the study protocol. The study participants received comprehensive guidance on the survey, including the general information questionnaire and the food frequency questionnaires (FFQ). In addition to the FFQ, selected parameters on anthropometric, demographic, and socioeconomic factors were collected. All the participants were duly informed and consented to take part in the study. The study design and information collected were approved by the National Research Ethics Committee (CNER) and the National Commission for Private Data Protection (CNPD).
2.2. Assessment of Dietary Intake
The dietary intake data were extracted from a validated quantitative FFQ [31]. In the ORISCAV-LUX study, a 134-item FFQ was used [31]. The FFQ was divided into nine food groups: 14 carbohydrate-related questions, 13 related to fruits, 13 to vegetables, 18 to meat–poultry–fish items, 11 to ready-made meals (prepared dishes), 22 to dairy products, 16 to fats (for spreading, cooking, and seasoning), 14 to drinks and beverages, and 13 to miscellaneous items. Miscellaneous items included jam, chocolate, peanut butter, dry biscuits, ice cream products, jellified desserts, sugar, and cocoa. The study participants indicated the portion size and frequency of all consumed beverages and food items on a scale ranging from “never or rarely”, “two or more times/day”, “once a day”, “3 to 5 times/week”, “1 to 2 times/week”, and “1 to 3 times/month”. The macro- and micronutrient intake was calculated by multiplying each food item’s consumption frequency by the specific nutrient content of each portion. Portion size images were used to accurately identify the portion sizes of all the consumed food and beverage items.
Similarly, in ORISCAV-LUX 2, a validated quantitative 174-item FFQ was used [32]. In fact, more questions about certain food items were asked in order to increase the accuracy in the second wave. For example, in the first wave, the question was about the total amount of “butter” consumed, while, in the second wave, the question was divided into two parts: “unsalted butter” and “lightly salted or salted butter”. The FFQ in the second wave comprised nine food groups, including 16 carbohydrate-related items, 12 fruit items, 13 vegetable items, 26 meat–poultry–fish items, 17 ready-made meal items, 22 dairy product items, 28 fat items, 21 drink and beverage items, and 18 miscellaneous items. The methods for completing the FFQ and extracting the data and the food database used [33] were similar for the two waves of the survey [33].
The amount of macro- and micronutrient intake was converted into a daily consumption and reported as median and interquartile range. For this purpose, the macro- and micronutrient intake amounts were obtained by linking the consumed food/beverage items with the ANSES-CIQUAL French Food Composition Table database [33]. The total energy was obtained as the sum of 37 kJ/g (9 kcal/g) for fat, 29 kJ/g (7 kcal/g) for alcohol, 17 kJ/g (4 kcal/g) for protein, 17 kJ/g (4 kcal/g) for carbohydrates (except for polyols), 13 kJ/g (3 kcal/g) for organic acids, 10 kJ/g (2.4 kcal/g) for polyols, and 8 kJ/g (2 kcal/g) for dietary fiber.
2.3. Anthropometric Measures
A trained research nurse performed the anthropometric measures of weight and height. Body mass index (BMI) was calculated. The height (cm) and body weight (kg) were measured in a slight dress without shoes. The participants’ BMI was estimated as weight in kg divided by the square of height in meters (kg/m2).
2.4. Demographic and Socioeconomic Factors
Age, gender, marital status, education, job, income, and the number of persons living in the same household were obtained from the General Information Questionnaire.
2.5. Data Management
From all the enrolled participants (ORISCAV-LUX = 1432, ORISCAV-LUX 2 = 1558), only the data of the participants who had completed the FFQ were considered in the present analysis. In this regard, 80 participants from ORISCAV-LUX and 127 participants from ORISCAV-LUX 2 were excluded due to the lack of FFQ data. From the 1352 participants who completed the FFQ in ORISCAV-LUX and the 1431 participants who completed the FFQ in ORISCAV-LUX 2, 110 participants under 25 years (ORISCAV-LUX) and 105 participants over 69 years (ORISCAV-LUX 2) were excluded to obtain the same age-range groups in the present paper.
Finally, the data of 1242 participants from ORISCAV-LUX and 1326 participants from ORISCAV-LUX 2 who completed the FFQ and were in the same age ranges were included in our analyses (see the flowchart of participants, Figure 1).
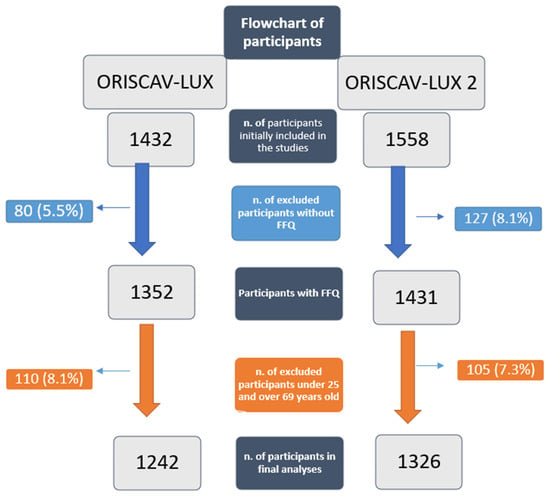
Figure 1.
Flowchart of participants in ORISCAV-LUX and ORISCAV-LUX 2.
Missing data: For the variable “income”, we grouped the missing data into “did not answer”. Therefore, no other participants were excluded from the analysis due to missing data in sociodemographic variables (Table 1). The replacement of missing data by the means or their imputation was not considered as a suitable strategy as data were not to be missing at random.

Table 1.
Distribution of demographic, anthropometric, and socioeconomic characteristics of participants.
2.6. Statistical Analyses
The normality of the data distribution and equality of variance were measured by Q–Q normality plots and the Kolmogorov–Smirnov test and box plots, respectively. A log transformation was performed for the non-normally distributed data.
Since about 45% of the participants in the second survey also participated in the first survey, linear mixed model (LMM) analyses were performed on log-transformed values to compare the estimated marginal means (EMMs) of the energy and macro- and micronutrient intake between the 2 surveys. LMMs included random intercepts for subjects and fixed effects for ORISCAV-LUX vs. ORISCAV-LUX 2, and adjustment for age at baseline, gender, marital status, education, job, income, and number of persons living in the same household. The LMMs, using an unstructured variance–covariance matrix, enabled the post hoc comparison of the estimated marginal means (EMMs) of the energy and macro- and micronutrient intake between the two surveys, and also according to the gender. A post hoc test (Tukey’s) was used. In order to decrease the false discovery rate due to the LMMS performed for each dietary parameter, we applied the Benjamini–Hochberg adjustment for multiple comparisons. The EMMs adjusted for age, gender, education, occupation (job), marital status, number of persons living in the household, and income were reported. In addition to the EMM and 95% confidence interval (95% CI), the raw data were reported as median and interquartile ranges. A p-value of 0.05 was considered as significant. The EMMs were also reported, adjusted only for age and gender, as a supplementary analysis. We also used the exploratory factor analysis (EFA) method to identify dietary patterns (2 major components), using the data from the FFQ, organized into 12 major food groups (Figure 2). Absolute values > 0.30 were considered to have a significant role in the components. Small coefficients below this value were suppressed.
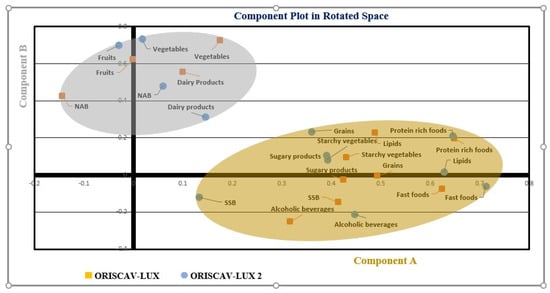
Figure 2.
The exploratory factor analysis (EFA) was used to identify two major components, using the data from the FFQ organized into 12 major food groups. A component plot in rotated space for both ORISCAV-LUX and ORISCAV-LUX 2 is represented. Component A included fast foods (ready-to-eat meals), lipids, grains, starchy vegetables, alcoholic beverages, SSB (sugar-sweetened beverages), sugary products, and protein-rich foods. Component B included fruits, vegetables, NAB (nonalcoholic beverages), and dairy products.
A comparison of the average intake of macro- and micronutrients of the study participants in the two surveys with the recommended values published by the World Health Organization (WHO), European Food Safety Authority (EFSA, PRI), United States Department of Agriculture (USDA, RDA) dietary guidance, British Nutrition Foundation (BNF), and German-(D), Austrian-(A), and Swiss (CH) (DACH) reference values was also carried out. The SPSS statistical software (IBM SPSS statistics 25.0, IBM Corp., Armonk, NY, USA) was used for the statistical analyses.
3. Results
Overall, 51% of the participants in the ORISCAV-LUX and 53.4% of the participants in the ORISCAV-LUX 2 were women. The mean age was 46.3 ± 11.6 years in the ORISCAV-LUX and 49.5 ± 10.0 years in the ORISCAV-LUX 2. The general characteristics of the study participants are presented in Table 1.
The EMM obtained from the linear mixed models, as well as the median and interquartile ranges of total energy, water, alcohol, and macronutrient intake of participants, are presented in Table 2. There was a significant increase in the EMMs of total energy intake, total water, total protein, animal protein, total fat, cholesterol, polyunsaturated fatty acids (PUFA), saturated fatty acids (SFA), monounsaturated fatty acids (MUFA), linoleic acid, alpha-linolenic acid, and alcohol, and a significant decrease in the EMMs of total carbohydrate, simple sugar, and added sugar intake in ORISCAV-LUX 2 compared to ORISCAV-LUX.
Table 2.
Median (interquartile range) and estimated marginal means of participants’ total energy, alcohol, and macronutrient intake (p-values are based on linear mixed models, as further detailed in footnotes).
Regarding micronutrient intake (Table 3), a significant reduction in the EMMs of magnesium and calcium intake was observed in ORISCAV-LUX 2 compared to ORISCAV-LUX.
Table 3.
Median (interquartile range) and estimated marginal means of micronutrient intake of participants (p-values are based on linear mixed models, as explained in footnotes).
The distribution of the participants’ food group intake is shown in Table 4. A significant decrease in the EMM of grains, vegetables, starchy vegetables, dairy products, and sugary products intake was found when comparing ORISCAV-LUX to ORISCAV-LUX 2, along with a significant increase in the EMM of protein-rich foods, ready-to-eat and fast food, lipids, noncaloric beverages, and alcoholic beverages. The same models for macro-, micro-nutrients and food groups adjusted only for age at baseline and gender are presented in Supplementary Tables S1–Table S3
Table 4.
Median (interquartile range) and estimated marginal means of food group intake of participants (p-values are based on linear mixed models, as explained in footnotes).
The within- and between-group comparisons of macronutrient (Table 5) and micronutrient (Table 6) intakes based on gender groups showed that men consumed significantly more energy, fat, proteins, total carbohydrates, cholesterol, total fiber, and alcohol compared to women in both ORISCAV-LUX and ORISCAV-LUX 2. The intake of most micronutrients (except folate, vitamin E, vitamin C, and calcium) were also lower in women compared to men in both waves of ORISCAV. In addition, there was a significant increase in the intake of total energy, total fat, and total alcohol in men participating in ORISCAV-LUX2 compared to men in ORISCAV-LUX. Similar significant increases were seen in women in ORISCAV-LUX 2 compared to ORISCAV-LUX.
Table 5.
Within- and between-group comparisons * of macronutrients based on gender groups (p-values are based on linear mixed model) e.
Table 6.
Within- and between-group comparisons* of micronutrients based on gender groups (p-values are based on linear mixed model) e.
On the other hand, there was a significant decrease in consumed total carbohydrates in both men and women in ORISCAV-LUX 2, compared to ORISCAV-LUX (Table 5). In parallel with the total increased fat intake, there was a significantly higher intake of fat-soluble vitamins (A, D, and E) in both men and women participating in ORISCAV-LUX 2 compared to ORISCAV-LUX. In accordance with the reduction in grains and dairy product consumption in ORISCAV-LUX 2 compared to the ORISCAV-LUX, the intake of calcium and magnesium showed a significant decrease in both genders in ORISCAV-LUX 2 (Table 6).
Finally, Table 7 displays the comparison of the average intake of macro- and micronutrients of the study participants in the two surveys with the recommended values published by the World Health Organization (WHO), European Food Safety Authority (EFSA), United States Department of Agriculture (USDA) dietary guidance, British Nutrition Foundation (BNF), and German-(D), Austrian-(A), and Swiss (CH) (DACH) reference values.
Table 7.
Mean intake of macro- and micronutrients of participants in ORISCAV-LUX and ORISCAV-LUX 2 compared to recommended values.
Adults residing in Luxembourg and participating in ORISCAV-LUX and ORISCAV-LUX 2 showed an intake of vitamin D, fiber, and folate below several recommendations, and a higher than recommended sodium and total fat intake.
4. Discussion
The present work used data from two large cross-sectional studies, ORISCAV-LUX (2007/2008) and ORISCAV-LUX 2 (2016/2017). We described the dietary patterns and their changes during the last decade (2007–2017) in adult residents in Luxembourg having taken part in the surveys. Our results highlight dietary changes over approximately 10 years amongst the study participants, with significant differences in the amount of some consumed macronutrients and micronutrients and underlying food groups. Most notably, total fat intake, MUFA, SFA, PUFA (including eicosapentaenoic acid, docosahexaenoic acid, and docosapentaenoic acid), cholesterol, alcohol, and total energy intake in men and women did increase significantly over the past decade (Table 2). In contrast, total carbohydrate, magnesium, and calcium intakes were significantly reduced (Table 3).
Regarding major food groups, there was a decrease over time in the intake of grains, vegetables, and dairy products. In contrast, the intake of protein-rich foods, ready-to-eat meals, fats, noncaloric beverages, and alcoholic beverages increased during the studied period (Table 4).
The strongest intake increases during this approximately 10-year period were seen for alcohol, ready-made meals, total fat, and SFA (Table 2 and Table 3). Compared to dietary recommendations (Table 7), the intake of total fat, energy, SFA, and sodium appeared relatively high. Especially in conjunction with the increased intake of ready-to-eat foods/fast foods that also included processed foods, such as meat products, such trends have been associated in the literature with a high incidence of type 2 diabetes and other cardiometabolic diseases [34,35,36,37]. However, these associations are typically based on cross-sectional studies, and other lifestyle factors could confound such relations [38]. Despite the fact that Luxembourg, similar to other countries, is engaged in health promotion programs to stimulate healthy eating [39], it appears that health-promotion-oriented measures were insufficient to turn the tide of poor dietary patterns. In line with these findings, when using the exploratory factor analysis to determine the main dietary components, two dietary patterns were obtained, which were either characterized by a rather Mediterranean pattern, rich in whole grains, fruits, vegetables, and dairy products, or a rather westernized pattern rich in starchy vegetables, animal-based proteins, fast foods, and fats (Figure 2). The first pattern would be in line with diets that have been associated with generally favorable health outcomes [40].
The estimated intake of most micronutrients appeared comparable over the years, or even increased (Table 3), with the exception of calcium and magnesium intake undergoing a significant decline during the past decade. Magnesium is an essential macro-mineral and a reduction in dietary intake of this mineral over the past decades has been reported for other countries, such as the US [41]. The intake of this micronutrient has been related in meta-analyses to the decreased incidence of type 2 diabetes, cardiovascular diseases, and all-cause mortality [42]. As magnesium is consumed partly within the grain/carbohydrate group and within vegetables, it is possible that its decline was related to the reduced intake of these food groups observed in the present study. Moreover, due to the lower consumption of food items from the dairy group, the decrease in calcium intake is conceivable and predictable. In addition to its importance in bone mass density [43], numerous studies have examined the association between low calcium intake and an increased risk of CVD. A population-based study for instance concluded that dietary calcium intake is associated with a decreased CVD risk [44].
Despite a significant reduction in the intake of grains and vegetables, dietary fiber intake did not significantly change. In a Europe-wide cohort study [45], including over half a million participants, researchers reported that fiber intake was associated with various types of cancers, with reduced fiber intake from fruit and vegetable sources as a major possible cause [45]. In addition, fiber and associated phytochemicals originating from a diverse intake of plant-based food items might positively affect gut microbiota diversity [46], which has also been inversely associated with several chronic diseases, including diabetes [47]. Despite dietary fiber intake being marginal compared to some intake recommendations, it was very close to reaching the 25 g/day as stipulated by EFSA (Table 7).
Despite these findings, the intake of a number of micronutrients has been increasing over the past decade. In parallel with a generally higher fat intake, the intake of multi-unsaturated fatty acids, including omega-3 fatty acids (EPA, DHA, and linolenic acid), also increased. These fatty acids have generally been related to anti-inflammatory processes [48] and have been correlated, e.g., to a lower incidence of coronary heart diseases [48]. Another positive aspect associated with the intake of higher amounts of dietary lipids is the increased intake of fat-soluble vitamins A, E, and D (Table 3). This increase has resulted in almost reaching the respective intake recommendations set by several health and nutrition-related organizations (Table 7). Moreover, despite the decreased vegetable intake, beta-carotene consumption slightly increased from 2007 to 2017. This contradictory result could be due to the intake of other beta-carotene sources, such as carrots, cabbages, and avocado, which, in our study, showed an increase in their intake (results not shown). Furthermore, possibly due to increased total energy and protein intake from animal sources, some water-soluble vitamins, such as niacin and pyridoxine, also increased significantly (Table 3), and their intake was generally in line with dietary recommendations (Table 7).
However, our study results showed that the dietary patterns in ORISCAV-LUX 2 are moving to a more Westernized-type diet, characterized by a higher intake of fat and alcohol and a lower total carbohydrate intake. In line with our findings, Marques-Vidal et al. reported similar results in the French-speaking part of Switzerland [49]. These results indicate that minor changes in dietary intakes and choices over time can significantly affect overall dietary patterns.
Differences between genders were also observed. Our study results showed that men consumed significantly more total energy, protein, total fat, cholesterol, and alcohol than women. To some extent, the higher intake might be attributed to the higher energy needs of men compared to women [50]). It was also found that men in the ORISCAV-LUX 2 consumed significantly higher amounts of total energy, animal-based protein, total fat, fat-soluble vitamins, SFA, MUFA, PUFA, cholesterol, sodium, and alcohol than men in the ORISCAV-LUX survey, but lower amounts of calcium and magnesium. Similar results were observed when comparing women in the two waves, except for sodium, where no significant difference was observed. According to other studies, in line with our findings, dietary patterns in men and women have changed in the last decade or so in other westernized countries [51]. Bédard et al. showed that men especially consumed more high-fat, high-protein, and ready-to-eat foods than women [52]. Somewhat contrarily, Macdiarmid et al., in a study in the UK, reported that associations between sugar and fat intake and BMI were different between men and women. They concluded that the consumption of products rich in fats and sugars might partly explain the higher BMI in women than men [53].
Moreover, in line with our results and with worldwide trends, Sánchez-Villegas et al., in a cohort study, showed that Spanish adult residents tended to consume more ready-to-eat foods and meals and increased their intake of processed foods, and thus consumed more saturated fat and more sodium but fewer vegetables, low-fat dairy products, and fruits over the past years [54]. As observed for ORISCAV-LUX 2, Bamia et al. reported that western dietary patterns, mainly including fat, animal-based protein, and fast foods, are also rising in the elderly Europeans [55]. They emphasized that these dietary patterns could be an essential contributing factor for various diet-related diseases, such as diabetes [55] and other inflammatory diseases. For instance, Harding et al., in the EPIC Cancer-Norfolk study, found a significant association between dietary fat and cholesterol intake and diabetes [56], though, in a pooled meta-analysis of cohort studies, only saturated fat intake was related to some types of cancer, not total fat and cholesterol intake [57]. Our results also indicate that grain intake, a rich source of soluble and insoluble fiber, has rather decreased over the past decade. According to the “Dietary Patterns Amongst Older Europeans” survey, fiber, one of the important characteristics of the Mediterranean dietary pattern, has been shown to be associated with a reduction in metabolic diseases, such as diabetes and hypertension [55], possibly due to their positive influence on the gut flora and increased formation of anti-inflammatory short-chain fatty acids [58]. A review article by Matthias et al. following a Mediterranean dietary pattern with recommended amounts of whole grains, fruits, and vegetables highlighted that these patterns were associated with a significant reduction in a number of cardiometabolic diseases, such as diabetes and hypertension [59]. Therefore, a higher intake of dietary fiber, as opposed to the 25 g/day in the present study, is desired.
Furthermore, Michelle et al. reported that Mediterranean dietary patterns were associated with a lower likelihood of developing obesity in people that are overweight, suggesting that improving the nutritional status might be part of the solution in tackling obesity or overweightness [60]. Both metabolically unhealthy obesity and metabolically unhealthy normal weight have been on the rise in Luxembourg [61] and other European countries in the past decades and were associated with inflammatory and oxidative stress processes. Similarly, Buckland et al. of the EPIC cohort survey reported that the Mediterranean dietary pattern was associated with reduced breast cancer and coronary heart disease [62].
Several factors have been highlighted as contributing to the changes in dietary patterns over time. The most important ones in literature were economic/social status, education, age, and gender [63,64,65]. However, what remains to be more fully explored is why dietary patterns have shifted toward rather less healthy attributes in westernized countries, if not globally. In general, it is believed that factors such as the globalization of the economy and food production, widespread advertising of fast-food companies, and a lack of physical activity play important roles [66,67,68,69]. In addition, with globalization, staple foods have been shifting from local to industrial products, which entail, to a large extent, low-cost and highly processed foods and, consequently, result in a deterioration in healthy dietary patterns [70]. On the other hand, increasing working hours (together with less time eating at home), and easy access to cheap and ready-to-eat meals have been highlighted as individual factors in the westernization of dietary patterns over time [66,67,68,69].
One of our study’s strengths is that it is the first survey to examine an example of a European country with a diverse demographic composition [71]. Another advantage of our study was using a validated FFQ, which allowed us to have a comprehensive interpretation of the study participants’ dietary intake, together with a geographically appropriate food database. Our study has a relatively high sample size given the total population of Luxembourg, which allowed us to perform analyses for different age and gender groups. However, ORISCAV-LUX 2 is not fully representative of the general adult population residing in Luxembourg. For example, the number of Portuguese participants in the second survey was lower than the number of Portuguese participants in the EHES (14.5%) study, which is considered representative of the general population and was conducted almost at the same time as ORISCAV LUX 2 [72]. Contrarily, ORISCAV-LUX (as ORISCAV-LUX 2), when comparing respondents vs. nonrespondents at baseline, can be considered representative regarding the place of residence [30], though not for other variables, such as age or education level.
As for other observational studies, our study had some limitations. One of the shortcomings was related to the use of two FFQ, with the second one being slightly more detailed. Recall bias is considered inevitable, as the FFQ inquired about food intake in the past 3 months. However, it seems that employing trained personnel might significantly reduce this bias [73]. As for all population-based longitudinal and cohort studies, another concern in our surveys is the quality of collected data in the two study waves, such as sample measurement by an accredited laboratory. Due to the generally small number of missing data (except for income) and percentage of completed questions, this limitation does not seem detrimental to the results of this study, despite nutrition playing a crucial role in these groups. Different dietary assessment tools (e.g., multiple 24-h recall methods or food records) may be more recommendable for those groups than FFQ [73]. Therefore, it is proposed that future studies focus on these groups to obtain a more comprehensive overview and formulate more targeted nutritional interventions, starting early in life.
5. Conclusions
As for other Westernized countries, adults in Luxembourg taking part in ORISCAV-LUX 2 have been consuming relatively high amounts of processed foods, animal-based products, and thus proteins, and also fat and sodium. Concomitantly, a trend appears to consume slightly fewer vegetables, below the recommended intake. It is acknowledged that, in addition to physiological needs, an array of other factors, such as access to food, taste, the influence of peers, neurophysiological pathways to food intake, and socioeconomic factors, along with health promotion and public health actions are essential for improving dietary habits and patterns and deserve more investigation. Meanwhile, the State of Luxembourg has taken further steps to improve population health by fostering a healthier diet, including efforts such as introducing the Nutri-Score labeling [74], and has also provided community-based training based on age and gender. These measures remain to be awaiting their efficiency; further large-scale efforts and interventions to produce more substantial and lasting effects are desired. Additional monitoring of dietary patterns, including the very young, is paramount to monitor population-based efforts to steer lifestyle patterns toward healthy directions and reduce possible associated diseases.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/nu13124382/s1, Table S1: Estimated marginal means of participants’ total energy, alcohol, and macronutrient intake, Table S2: Estimated marginal means of micronutrient intake of participants, Table S3: Estimated marginal means of food groups’ intake of participants.
Author Contributions
F.V. and T.B. performed the statistical analyses, interpreted the data, and drafted the manuscript. H.S. provided substantial contributions to the idea, conception, and design of the work, interpretation of the data, and guidance on the intellectual content and critical revision of the manuscript. M.V. and G.L.C. guided the statistical analyses, interpretation of the data, and critical revision of the manuscript. A.B. contributed to the revision of the manuscript. T.B. provided expertise and oversight on the intellectual content. All authors have read and agreed to the published version of the manuscript.
Funding
The ORISCAV-LUX and ORISCAV-LUX 2 data collection was funded by the LIH (MESR funding). A.B. was supported by the Ministry of Science and Higher Education of the Russian Federation within the framework of state support for creating and developing World-Class Research Centers “Digital biodesign and personalized healthcare No. 075-15-2020-926”.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the National Research Ethics Committee of Luxembourg (CNER, N° 201,505/12 and N° 200609/03).
Informed Consent Statement
Written informed consent was obtained by all participants.
Data Availability Statement
Not applicable.
Acknowledgments
We thank all the study participants of the ORISCAV-LUX and ORISCAV-LUX 2 surveys. We thank Ala’a Alkerwi, who was involved in the general conception and design of the ORISCAV-LUX survey. We also extend our gratitude to the ORISCAV-LUX researcher’s working group that has been fully involved in the conception and design of the ORISCAV-LUX 2 survey. ORISCAV Working Group: Gloria Aguayo, Ala’a Alkerwi, Brice Appenzeller, Jean Beissel, Dritan Bejko, Anna Chioti, Sophie Couffignal, Charles Delagardelle, Yvan Devaux, Isabelle Ernens, Guy Fagherazzi, Manon Gantenbein, Laetitia Huiart, Marylène D’Incau, Marie-Lise Lair, Stephanie Noppe, Laurent Malisoux, Jessica Pastore, Magali Perquin, Maria Ruiz-Castell, Jean-Claude Schmit and Saverio Stranges. We thank the research nurses involved in the ORISCAV-LUX and ORISCAV-LUX 2 surveys. Moreover, we are grateful to the Department of Public Health, University of Liège (Belgium), for allowing us to use their Food Frequency Questionnaire (https://www.dssp-uliege.be/FFQ (accessed on 22 May 2021)).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Engeset, D.; Alsaker, E.; Ciampi, A.; Lund, E. Dietary patterns and lifestyle factors in the Norwegian EPIC cohort: The Norwegian Women and Cancer (NOWAC) study. Eur. J. Clin. Nutr. 2005, 59, 675–684. [Google Scholar] [CrossRef]
- Grosso, G.; Bella, F.; Godos, J.; Sciacca, S.; Del Rio, D.; Ray, S.; Galvano, F.; Giovannucci, E.L. Possible role of diet in cancer: Systematic review and multiple meta-analyses of dietary patterns, lifestyle factors, and cancer risk. Nutr. Rev. 2017, 75, 405–419. [Google Scholar] [CrossRef]
- Sadeghi, M.; Vahid, F.; Rahmani, D.; Akbari, M.E.; Davoodi, S.H. The Association between Dietary Patterns and Breast Cancer Pathobiological Factors Progesterone Receptor (PR) and Estrogen Receptors (ER): New Findings from Iranian Case-Control Study. Nutr. Cancer 2019, 71, 1290–1298. [Google Scholar] [CrossRef]
- Johansson, L.; Thelle, D.S.; Solvoll, K.; Bjørneboe, G.-E.A.; Drevon, C.A. Healthy dietary habits in relation to social determinants and lifestyle factors. Br. J. Nutr. 1999, 81, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Pänkäläinen, M.; Fogelholm, M.; Valve, R.; Kampman, O.; Kauppi, M.; Lappalainen, E.; Hintikka, J. Pessimism, diet, and the ability to improve dietary habits: A three-year follow-up study among middle-aged and older Finnish men and women. Nutr. J. 2018, 17, 92. [Google Scholar] [CrossRef] [PubMed]
- Tapsell, L.C. Dietary behaviour changes to improve nutritional quality and health outcomes. Chronic. Dis. Transl. Med. 2017, 3, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Johansson, S.E.; Sundquist, J. Change in lifestyle factors and their influence on health status and all-cause mortality. Int. J. Epidemiol. 1999, 28, 1073–1080. [Google Scholar] [CrossRef]
- Alkerwi, A.a.; Sauvageot, N.; Donneau, A.-F.; Lair, M.-L.; Couffignal, S.; Beissel, J.; Delagardelle, C.; Wagener, Y.; Albert, A.; Guillaume, M. First nationwide survey on cardiovascular risk factors in Grand-Duchy of Luxembourg (ORISCAV-LUX). BMC Public Health. 2010, 10, 468. [Google Scholar] [CrossRef]
- Suetens, C. Healthcare-associated infections in European long-term care facilities: How big is the challenge? Eurosurveillance 2012, 17, 20259. [Google Scholar] [CrossRef] [PubMed]
- Bocquet, V.; Ruiz-Castell, M.; de Beaufort, C.; Barre, J.; de Rekeneire, N.; Michel, G.; Donahue, R.P.; Kuemmerle, A.; Stranges, S. Public health burden of pre-diabetes and diabetes in Luxembourg: Finding from the 2013-2015 European Health Examination Survey. BMJ Open 2019, 9, e022206. [Google Scholar] [CrossRef]
- Perquin, M.; Diederich, N.; Pastore, J.; Lair, M.L.; Stranges, S.; Vaillant, M.; MemoVie, G. Prevalence of Dementia and Cognitive Complaints in the Context of High Cognitive Reserve: A Population-Based Study. PLoS ONE 2015, 10, e0138818. [Google Scholar]
- Hipp, G.; Vaillant, M.; Diederich, N.J.; Roomp, K.; Satagopam, V.P.; Banda, P.; Sandt, E.; Mommaerts, K.; Schmitz, S.K.; Longhino, L.; et al. The Luxembourg Parkinson’s Study: A Comprehensive Approach for Stratification and Early Diagnosis. Front. Aging Neurosci. 2018, 10, 326. [Google Scholar] [CrossRef] [PubMed]
- Alkerwi, A.; Bahi, I.E.; Stranges, S.; Beissel, J.; Delagardelle, C.; Noppe, S.; Kandala, N.-B. Geographic variations in cardiometabolic risk factors in Luxembourg. Int. J. Environ. Res. 2017, 14, 648. [Google Scholar] [CrossRef]
- Naska, A.; Fouskakis, D.; Oikonomou, E.; Almeida, M.D.V.; Berg, M.A.; Gedrich, K.; Moreiras, O.; Nelson, M.; Trygg, K.; Turrini, A.; et al. Dietary patterns and their socio-demographic determinants in 10 European countries: Data from the DAFNE databank. Eur. J. Clin. Nutr. 2006, 60, 181–190. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Status Report on Alcohol and Health 2018; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Alkerwi, A.; Crichton, G.E.; Hébert, J.R. Consumption of ready-made meals and increased risk of obesity: Findings from the Observation of Cardiovascular Risk Factors in Luxembourg (ORISCAV-LUX) study. Br. J. Nutr. 2015, 113, 270–277. [Google Scholar] [CrossRef]
- Esposito, K.; Maiorino, M.I.; Bellastella, G.; Panagiotakos, D.B.; Giugliano, D. Mediterranean diet for type 2 diabetes: Cardiometabolic benefits. Endocrine 2017, 56, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Wilmot, K.A.; Ghasemzadeh, N.; Molloy, D.L.; Burkman, G.; Mekonnen, G.; Gongora, M.C.; Quyyumi, A.A.; Sperling, L.S. Mediterranean Dietary Patterns and Cardiovascular Health. Annu. Rev. Nutr. 2015, 35, 425–449. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: An updated systematic review and meta-analysis of observational studies. Cancer Med. 2015, 4, 1933–1947. [Google Scholar] [CrossRef]
- Herforth, A.; Arimond, M.; Álvarez-Sánchez, C.; Coates, J.; Christianson, K.; Muehlhoff, E. A Global Review of Food-Based Dietary Guidelines. Adv. Nutr. 2019, 10, 590–605. [Google Scholar] [CrossRef]
- Elmadfa, I. European Nutrition and Health Report 2009; Karger Medical and Scientific Publishers: Basel, Switzerland, 2009; Volume 62. [Google Scholar]
- Alkerwi, A.a.; Sauvageot, N.; Nau, A.; Lair, M.-L.; Donneau, A.-F.; Albert, A.; Guillaume, M. Population compliance with national dietary recommendations and its determinants: Findings from the ORISCAV-LUX study. Br. J. Nutr. 2012, 108, 2083–2092. [Google Scholar] [CrossRef] [PubMed]
- FAOSTAT 2007. Livestock and Fish Primary Equivalent, Food and Agriculture Organization of the United Nations, Viewed 31 March 2007. Available online: http://faostat.fao.org/site/610/DesktopDefault.aspx?PageID=610#ancor (accessed on 21 January 2021).
- McEvoy, C.T.; Temple, N.; Woodside, J.V. Vegetarian diets, low-meat diets and health: A review. Public Health Nutr. 2012, 15, 2287–2294. [Google Scholar] [CrossRef]
- McNeill, S.H. Inclusion of red meat in healthful dietary patterns. Meat. Sci. 2014, 98, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Kearney, J. Food consumption trends and drivers. Philos. Trans. R. Soc. B Biol. Sci. 2010, 365, 2793–2807. [Google Scholar] [CrossRef] [PubMed]
- Vilaro, M.J.; Colby, S.E.; Riggsbee, K.; Zhou, W.; Byrd-Bredbenner, C.; Olfert, M.D.; Barnett, T.E.; Horacek, T.; Sowers, M.; Mathews, A.E. Food Choice Priorities Change Over Time and Predict Dietary Intake at the End of the First Year of College Among Students in the U.S. Nutrients 2018, 10, 1296. [Google Scholar] [CrossRef] [PubMed]
- Caruana, E.J.; Roman, M.; Hernández-Sánchez, J.; Solli, P. Longitudinal studies. J. Thorac. Dis. 2015, 7, E537–E540. [Google Scholar] [PubMed]
- Karageorgou, D.; Magriplis, E.; Mitsopoulou, A.V.; Dimakopoulos, I.; Bakogianni, I.; Micha, R.; Michas, G.; Chourdakis, M.; Ntouroupi, T.; Tsaniklidou, S.M.; et al. Dietary patterns and lifestyle characteristics in adults: Results from the Hellenic National Nutrition and Health Survey (HNNHS). Public Health. 2019, 171, 76–88. [Google Scholar] [CrossRef]
- Alkerwi, A.a.; Pastore, J.; Sauvageot, N.; Coroller, G.L.; Bocquet, V.; d’Incau, M.; Aguayo, G.; Appenzeller, B.; Bejko, D.; Bohn, T.; et al. Challenges and benefits of integrating diverse sampling strategies in the observation of cardiovascular risk factors (ORISCAV-LUX 2) study. BMC Med. Res. Methodol. 2019, 19, 27. [Google Scholar] [CrossRef] [PubMed]
- Sauvageot, N.; Guillaume, M.; Albert, A. Validation of the food frequency questionnaire used to assess the association between dietary habits and cardiovascular risk factors in the NESCAV study. J. Food Sci. 2013, 3, 3. [Google Scholar] [CrossRef]
- Sauvageot, N.; Alkerwi, A.; Albert, A.; Guillaume, M. Use of food frequency questionnaire to assess relationships between dietary habits and cardiovascular risk factors in NESCAV study: Validation with biomarkers. Nutr. J. 2013, 12, 143. [Google Scholar] [CrossRef] [PubMed]
- French Agency for Food, Environmental and Occupational Health & Safety. ANSES-CIQUAL French Food Composition Table for Nutritional Intakes Calculation CALNUT. Available online: https://ciqual.anses.fr/ (accessed on 21 January 2021).
- Barnard, N.; Levin, S.; Trapp, C. Meat consumption as a risk factor for type 2 diabetes. Nutrients 2014, 6, 897–910. [Google Scholar] [CrossRef]
- Micha, R.; Wallace, S.K.; Mozaffarian, D. Red and processed meat consumption and risk of incident coronary heart disease, stroke, and diabetes mellitus: A systematic review and meta-analysis. Circulation 2010, 121, 2271–2283. [Google Scholar] [CrossRef]
- Ericson, U.; Sonestedt, E.; Gullberg, B.; Hellstrand, S.; Hindy, G.; Wirfält, E.; Orho-Melander, M. High intakes of protein and processed meat associate with increased incidence of type 2 diabetes. Br. J. Nutr. 2013, 109, 1143–1153. [Google Scholar] [CrossRef]
- Ibsen, D.B.; Steur, M.; Imamura, F.; Overvad, K.; Schulze, M.B.; Bendinelli, B.; Guevara, M.; Agudo, A.; Amiano, P.; Aune, D. Replacement of red and processed meat with other food sources of protein and the risk of type 2 diabetes in European populations: The EPIC-InterAct Study. Diab. Care 2020, 43, 2660–2667. [Google Scholar] [CrossRef]
- Arsenault, B.J.; Lamarche, B.; Després, J.-P. Targeting Overconsumption of Sugar-Sweetened Beverages vs. Overall Poor Diet Quality for Cardiometabolic Diseases Risk Prevention: Place Your Bets! Nutrients 2017, 9, 600. [Google Scholar] [CrossRef] [PubMed]
- Brambila-Macias, J.; Shankar, B.; Capacci, S.; Mazzocchi, M.; Perez-Cueto, F.J.; Verbeke, W.; Traill, W.B. Policy interventions to promote healthy eating: A review of what works, what does not, and what is promising. Food Nutr. Bull. 2011, 32, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Martínez-González, M.A.; Tong, T.Y.; Forouhi, N.G.; Khandelwal, S.; Prabhakaran, D.; Mozaffarian, D.; de Lorgeril, M. Definitions and potential health benefits of the Mediterranean diet: Views from experts around the world. BMC Med. 2014, 12, 112. [Google Scholar] [CrossRef]
- Ford, E.S.; Mokdad, A.H. Dietary Magnesium Intake in a National Sample of U.S. Adults. J. Nutr. 2003, 133, 2879–2882. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Wang, K.; Han, D.; He, X.; Wei, J.; Zhao, L.; Imam, M.U.; Ping, Z.; Li, Y.; Xu, Y.; et al. Dietary magnesium intake and the risk of cardiovascular disease, type 2 diabetes, and all-cause mortality: A dose-response meta-analysis of prospective cohort studies. BMC Med. 2016, 14, 210. [Google Scholar] [CrossRef] [PubMed]
- Tai, V.; Leung, W.; Grey, A.; Reid, I.R.; Bolland, M.J. Calcium intake and bone mineral density: Systematic review and meta-analysis. BMJ 2015, 351, h4183. [Google Scholar] [CrossRef] [PubMed]
- Kong, S.H.; Kim, J.H.; Hong, A.R.; Cho, N.H.; Shin, C.S. Dietary calcium intake and risk of cardiovascular disease, stroke, and fracture in a population with low calcium intake. Am. J. Clin. Nutr. 2017, 106, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Bradbury, K.E.; Appleby, P.N.; Key, T.J. Fruit, vegetable, and fiber intake in relation to cancer risk: Findings from the European Prospective Investigation into Cancer and Nutrition (EPIC). Am. J. Clin. Nutr. 2014, 100 (Suppl. 1), 394s–398s. [Google Scholar] [CrossRef]
- Dingeo, G.; Brito, A.; Samouda, H.; Iddir, M.; La Frano, M.R.; Bohn, T. Phytochemicals as modifiers of gut microbial communities. Food Funct. 2020, 11, 8444–8471. [Google Scholar] [CrossRef] [PubMed]
- Post, R.E.; Mainous, A.G., 3rd; King, D.E.; Simpson, K.N. Dietary fiber for the treatment of type 2 diabetes mellitus: A meta-analysis. J. Am. Board. Fam. Med. 2012, 25, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Vahid, F.; Goodarzi, R.; Shivappa, N.; Hébert, J.R.; Fazeli Moghadam, E. Dietary Inflammatory Index (DII®): A significant association between coronary heart disease and DII® in Armenian adults. Eur. J. Prev. Cardiol. 2020, 27, 2235–2237. [Google Scholar] [CrossRef]
- Marques-Vidal, P.; Gaspoz, J.-M.; Theler, J.-M.; Guessous, I. Twenty-year trends in dietary patterns in French-speaking Switzerland: Toward healthier eating. Am. J. Clin. Nutr. 2017, 106, 217–224. [Google Scholar] [CrossRef]
- CALERIE StudyGroup. Energy requirements in nonobese men and women: Results from CALERIE. Am. J. Clin. Nutr. 2013, 99, 71–78. [Google Scholar]
- Harrington, J.M.; Dahly, D.L.; Fitzgerald, A.P.; Gilthorpe, M.S.; Perry, I.J. Capturing changes in dietary patterns among older adults: A latent class analysis of an ageing Irish cohort. Public Health Nutr. 2014, 17, 2674–2686. [Google Scholar] [CrossRef] [PubMed]
- Bédard, A.; Riverin, M.; Dodin, S.; Corneau, L.; Lemieux, S. Sex differences in the impact of the Mediterranean diet on cardiovascular risk profile. Br. J. Nutr. 2012, 108, 1428–1434. [Google Scholar] [CrossRef] [PubMed]
- Macdiarmid, J.I.; Vail, A.; Cade, J.E.; Blundell, J.E. The sugar–fat relationship revisited: Differences in consumption between men and women of varying BMI. Int. J. Obes. 1998, 22, 1053–1061. [Google Scholar] [CrossRef]
- Sánchez-Villegas, A.; Delgado-Rodríguez, M.; Martínez-González, M.Á.; de Irala-Estévez, J.; for the Seguimiento Universidad de Navarra group. Gender, age, socio-demographic and lifestyle factors associated with major dietary patterns in the Spanish Project SUN (Seguimiento Universidad de Navarra). Eur. J. Clin. Nutr. 2003, 57, 285–292. [Google Scholar] [CrossRef]
- Bamia, C.; Orfanos, P.; Ferrari, P.; Overvad, K.; Hundborg, H.H.; Tjønneland, A.; Olsen, A.; Kesse, E.; Boutron-Ruault, M.-C.; Clavel-Chapelon, F.; et al. Dietary patterns among older Europeans: The EPIC-Elderly study. Br. J. Nutr. 2005, 94, 100–113. [Google Scholar] [CrossRef]
- Harding, A.-H.; Day, N.E.; Khaw, K.-T.; Bingham, S.; Luben, R.; Welsh, A.; Wareham, N.J. Dietary Fat and the Risk of Clinical Type 2 Diabetes: The European Prospective Investigation of Cancer-Norfolk Study. Am. J. Epidemiol. 2004, 159, 73–82. [Google Scholar] [CrossRef]
- Genkinger, J.M.; Hunter, D.J.; Spiegelman, D.; Anderson, K.E.; Beeson, W.L.; Buring, J.E.; Colditz, G.A.; Fraser, G.E.; Freudenheim, J.L.; Goldbohm, R.A.; et al. A pooled analysis of 12 cohort studies of dietary fat, cholesterol and egg intake and ovarian cancer. Cancer. Causes. Control. 2006, 17, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Morrison, D.J.; Preston, T. Formation of short chain fatty acids by the gut microbiota and their impact on human metabolism. Gut Microbes 2016, 7, 189–200. [Google Scholar] [CrossRef]
- Schulze, M.B.; Hu, F.B. Dietary patterns and risk of hypertension, type 2 diabetes mellitus, and coronary heart disease. Curr. Atheroscler. Rep. 2002, 4, 462–467. [Google Scholar] [CrossRef]
- Mendez, M.A.; Popkin, B.M.; Jakszyn, P.; Berenguer, A.; Tormo, M.J.; Sanchéz, M.J.; Quirós, J.R.; Pera, G.; Navarro, C.; Martinez, C.; et al. Adherence to a Mediterranean Diet Is Associated with Reduced 3-Year Incidence of Obesity. J. Nutr. 2006, 136, 2934–2938. [Google Scholar] [CrossRef] [PubMed]
- Europepan Commission. Report from the Commission to the European Parliament and the Council Regarding the Use of Additional Forms of Expression and Presentation of the Nutrition Declaration. 2020. Available online: https://eur-lex.europa.eu/legal-content/GA/TXT/?uri=CELEX:52020DC0207 (accessed on 25 February 2021).
- Buckland, G.; Travier, N.; Cottet, V.; González, C.A.; Luján-Barroso, L.; Agudo, A.; Trichopoulou, A.; Lagiou, P.; Trichopoulos, D.; Peeters, P.H.; et al. Adherence to the mediterranean diet and risk of breast cancer in the European prospective investigation into cancer and nutrition cohort study. Int. J. Cancer Res. 2013, 132, 2918–2927. [Google Scholar] [CrossRef]
- Mishra, G.; McNaughton, S.; Bramwell, G.a.; Wadsworth, M. Longitudinal changes in dietary patterns during adult life. Br. J. Nutr. 2006, 96, 735–744. [Google Scholar]
- Waid, J.L.; Sinharoy, S.S.; Ali, M.; Stormer, A.E.; Thilsted, S.H.; Gabrysch, S. Dietary patterns and determinants of changing diets in Bangladesh from 1985 to 2010. Curr. Dev. Nutr. 2019, 3, nzy091. [Google Scholar] [CrossRef]
- Mazzocchi, M.; Brasili, C.; Sandri, E. Trends in dietary patterns and compliance with World Health Organization recommendations: A cross-country analysis. Public Health Nutr. 2008, 11, 535–540. [Google Scholar] [CrossRef]
- Uusitalo, U.; Sobal, J.; Moothoosamy, L.; Chitson, P.; Shaw, J.; Zimmet, P.; Tuomilehto, J. Dietary Westernisation: Conceptualisation and measurement in Mauritius. Public Health Nutr. 2005, 8, 608–619. [Google Scholar] [CrossRef] [PubMed]
- Wakimoto, P.; Block, G. Dietary intake, dietary patterns, and changes with age: An epidemiological perspective. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, 65–80. [Google Scholar] [CrossRef] [PubMed]
- Lake, A.A.; Adamson, A.J.; Hyland, R.M.; Mathers, J.C. Dietary change and perceptions of change over time. Nutr. Bull. 2004, 29, 199–203. [Google Scholar] [CrossRef]
- Jiang, L.; Audouze, K.; Romero Herrera, J.A.; Ängquist, L.H.; Kjærulff, S.K.; Izarzugaza, J.M.G.; Tjønneland, A.; Halkjær, J.; Overvad, K.; Sørensen, T.I.A.; et al. Conflicting associations between dietary patterns and changes of anthropometric traits across subgroups of middle-aged women and men. Clin. Nutr. 2020, 39, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Vega Mejía, N.; Ponce Reyes, R.; Martinez, Y.; Carrasco, O.; Cerritos, R. Implications of the Western Diet for Agricultural Production, Health and Climate Change. Front. Sustain. Food Syst. 2018, 2, 88. [Google Scholar] [CrossRef]
- European Commission, Eurydice Network. Population: Demographic Situation, Languages and Religions of Luxembourg. 2020. Available online: https://eacea.ec.europa.eu/national-policies/eurydice/content/population-demographic-situation-languages-and-religions-46_en (accessed on 2 March 2021).
- Bocquet, V.; Barré, J.; Couffignal, S.; d’Incau, M.; Delagardelle, C.; Michel, G.; Schlesser, M.; Stranges, S.; Kuemmerle, A.; Ruiz-Castell, M. Study design and characteristics of the Luxembourg European Health Examination Survey (EHES-LUX). BMC Public Health. 2018, 18, 1169. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.-S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health. 2014, 36, e2014009. [Google Scholar] [CrossRef] [PubMed]
- Hercberg, S.; Touvier, M.; Salas-Salvado, J.; on behalf of the Group of European scientists supporting the implementation of Nutri-Score in Europe. The Nutri-Score nutrition label. Int. J. Vitam. Nutr. Res. 2021. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).