
The Attitudes of Polish Women towards Breastfeeding Based on the Iowa Infant Feeding Attitude Scale (IIFAS)


 ,
,
Abstract
:1. Introduction
Purpose of the Study
2. Materials and Methods
2.1. Assessments
2.2. Translation Procedures
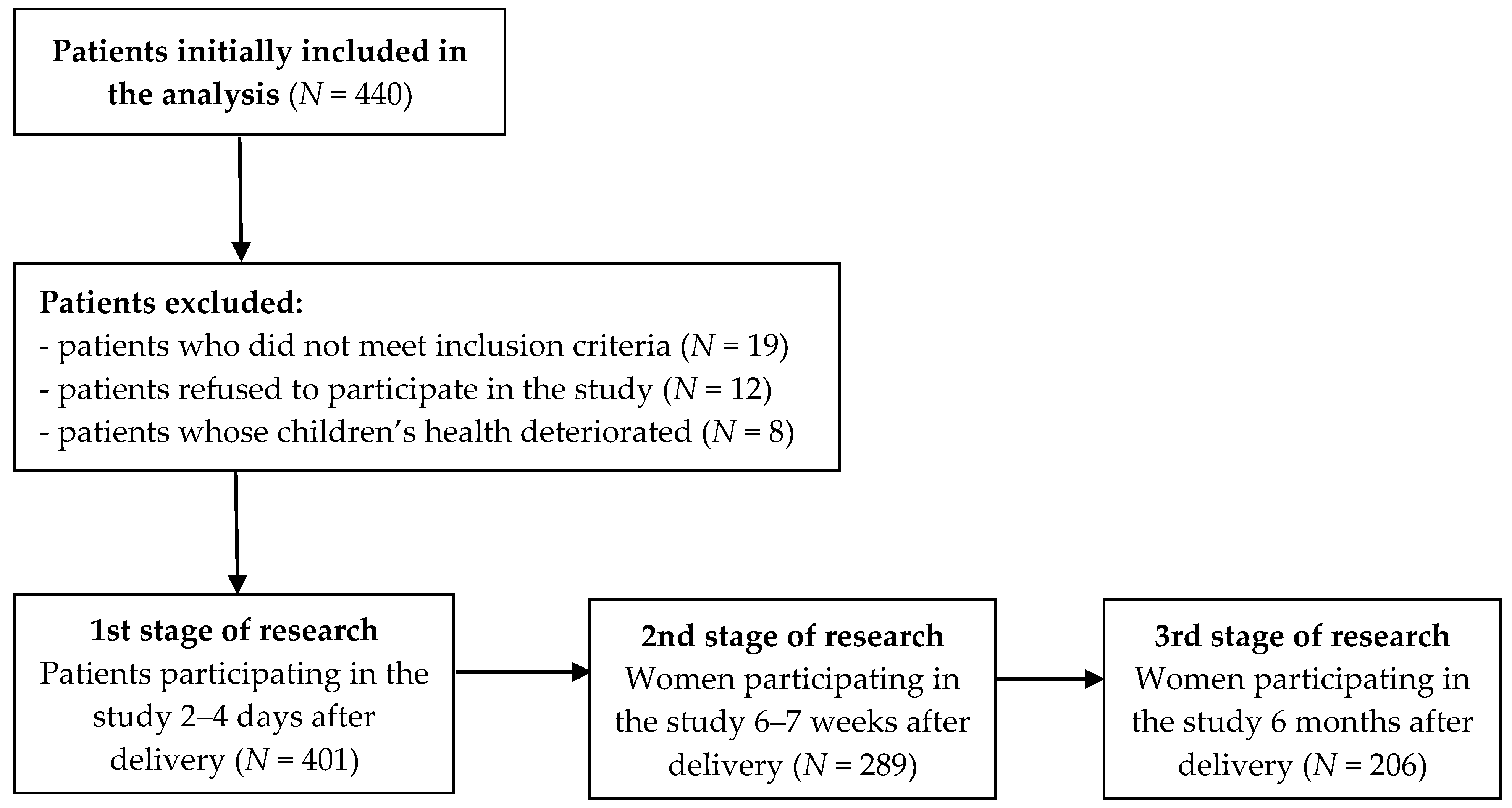
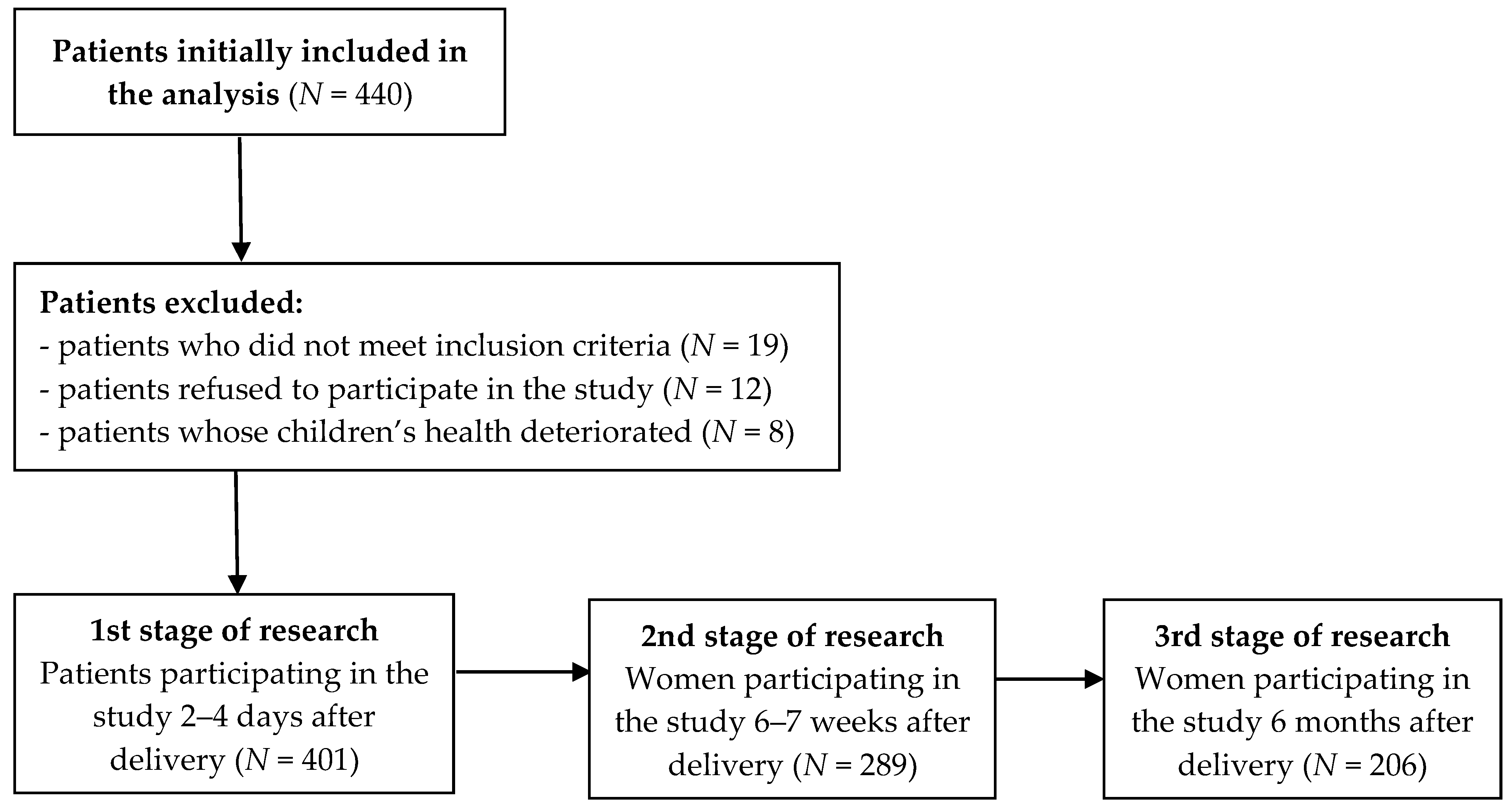
2.3. Study Groups
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| 1. | Korzyści z karmienia piersią trwają tylko do momentu odstawienia dziecka od piersi. | 1 | 2 | 3 | 4 | 5 |
| 2. | Karmienie mieszanką sztuczną jest wygodniejsze niż karmienie piersią. | 1 | 2 | 3 | 4 | 5 |
| 3. | Karmienie piersią wzmacnia więź między matką a dzieckiem. | 1 | 2 | 3 | 4 | 5 |
| 4. | W mleku matki brakuje żelaza. | 1 | 2 | 3 | 4 | 5 |
| 5. | Niemowlęta karmione mieszanką sztuczną są częściej przekarmiane niż dzieci karmione piersią. | 1 | 2 | 3 | 4 | 5 |
| 6. | Karmienie mieszanką sztuczną jest lepszym rozwiązaniem dla matki, która chce wrócić do pracy. | 1 | 2 | 3 | 4 | 5 |
| 7. | Matki karmiące mieszanką sztuczną tracą jedną z największych radości macierzyństwa. | 1 | 2 | 3 | 4 | 5 |
| 8. | Kobiety nie powinny karmić piersią w miejscach publicznych, takich jak restauracje. | 1 | 2 | 3 | 4 | 5 |
| 9. | Niemowlęta karmione piersią są zdrowsze niż dzieci karmione mieszanką sztuczną. | 1 | 2 | 3 | 4 | 5 |
| 10. | Niemowlęta karmione piersią są częściej przekarmiane niż dzieci karmione mieszanką sztuczną. | 1 | 2 | 3 | 4 | 5 |
| 11. | Ojcowie czują się pominięci, jeśli matka karmi piersią. | 1 | 2 | 3 | 4 | 5 |
| 12. | Mleko matki jest idealnym pożywieniem dla niemowląt. | 1 | 2 | 3 | 4 | 5 |
| 13. | Mleko matki jest bardziej lekkostrawne niż mieszanka sztuczna. | 1 | 2 | 3 | 4 | 5 |
| 14. | Mieszanka sztuczna jest tak samo zdrowa dla niemowlęcia jak mleko matki. | 1 | 2 | 3 | 4 | 5 |
| 15. | Karmienie piersią jest wygodniejsze niż karmienie mieszanką sztuczną. | 1 | 2 | 3 | 4 | 5 |
| 16. | Mleko matki jest tańsze niż mieszanka sztuczna. | 1 | 2 | 3 | 4 | 5 |
References
- Agostoni, C.; Decsi, T.; Fewtrell, M.; Goulet, O.; Kolacek, S.; Koletzko, B.; Michaelsen, K.F.; Moreno, L.; Puntis, J.; Rigo, J.; et al. Complementary Feeding: A Commentary by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2008, 46, 99–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Work Group on Breastfeeding. Section on Breastfeeding. Breastfeeding and the Use of Human Milk. Pediatrics 2012, 129, e827–e841. [Google Scholar] [CrossRef] [Green Version]
- Bosi, A.T.B.; Eriksen, K.G.; Sobko, T.; Wijnhoven, T.M.; Breda, J. Breastfeeding practices and policies in WHO European Region Member States. Public Health Nutr. 2016, 19, 753–764. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. UNICEF Increasing Commitment to Breastfeeding through Funding and Improved Policies and Programmes: Global Breastfeeding Scorecard 2019; World Health Organization: New York, NY, USA; Geneva, Switzerland, 2019. [Google Scholar]
- Bonia, K.; Twells, L.; Halfyard, B.; Ludlow, V.; Newhook, L.A.; Murphy-Goodridge, J. A qualitative study exploring factors associated with mothers’ decisions to formula-feed their infants in Newfoundland and Labrador, Canada. BMC Public Health 2013, 13, 645. [Google Scholar] [CrossRef] [Green Version]
- Senghore, T.; Omotosho, T.A.; Ceesay, O.; Williams, D.C.H. Predictors of exclusive breastfeeding knowledge and intention to or practice of exclusive breastfeeding among antenatal and postnatal women receiving routine care: A cross-sectional study. Int. Breastfeed. J. 2018, 13, 9. [Google Scholar] [CrossRef]
- Abdulahi, M.; Fretheim, A.; Argaw, A.; Magnus, J.H. Adaptation and validation of the Iowa Infant Feeding Attitude Scale and the breastfeeding knowledge questionnaire for use in an Ethiopian setting. Int. Breastfeed. J. 2020, 15, 24. [Google Scholar] [CrossRef]
- Chen, S.; Binns, C.W.; Liu, Y.; Maycock, B.; Zhao, Y.; Tang, L. Attitudes towards breastfeeding—The Iowa Infant Feeding Attitude Scale in Chinese mothers living in China and Australia. Asia Pac. J. Clin. Nutr. 2013, 22, 266–269. [Google Scholar]
- Inoue, M.; Binns, C.W.; Katsuki, Y.; Ouchi, M. Japanese mothers’ breastfeeding knowledge and attitudes assessed by the Iowa Infant Feeding Attitudes Scale. Asia Pac. J. Clin. Nutr. 2013, 22, 261–265. [Google Scholar]
- Cox, K.N.; Giglia, R.C.; Binns, C.W. The influence of infant feeding attitudes on breastfeeding duration: Evidence from a cohort study in rural Western Australia. Int. Breastfeed. J. 2015, 10, 25. [Google Scholar] [CrossRef] [Green Version]
- Abu Shosha, G.M. The Influence of Infants’ Characteristics on Breastfeeding Attitudes among Jordanian Mothers. Open J. Nurs. 2015, 5, 295–302. [Google Scholar] [CrossRef] [Green Version]
- Balyakina, E.; Fulda, K.G.; Franks, S.F.; Cardarelli, K.M.; Hinkle, K. Association Between Healthcare Provider Type and Intent to Breastfeed Among Expectant Mothers. Matern. Child Health J. 2015, 20, 993–1000. [Google Scholar] [CrossRef]
- Costanian, C.; MacPherson, A.K.; Tamim, H. Inadequate prenatal care use and breastfeeding practices in Canada: A national survey of women. BMC Pregnancy Childbirth 2016, 16, 100. [Google Scholar] [CrossRef] [Green Version]
- Cotelo, M.D.C.S.; Movilla-Fernández, M.J.; Pita-García, P.; Novío, S. Infant Feeding Attitudes and Practices of Spanish Low-Risk Expectant Women Using the IIFAS (Iowa Infant Feeding Attitude Scale). Nutrients 2018, 10, 520. [Google Scholar] [CrossRef] [Green Version]
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, M.; Fidler Mis, N.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapil-lonne’a, A.; et al. Complementary feeding: A position paper by the European Society for Paediatric Gastroenterolo-gy, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132. [Google Scholar] [CrossRef]
- WHO; UNICEF. Nurturing the Health and Wealth of Nations: The Investment Case for Breastfeeding. Global Breastfeeding Investment Case, 2017; UNICEF: New York, NY, USA; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization; UNICEF. Tracking Progress for Breastfeeding Policies and Programmes: Global Breastfeeding Scorecard 2017; UNICEF: New York, NY, USA; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Lis-Kuberka, J.; Orczyk-Pawiłowicz, M. Polish Women Have Moderate Knowledge of Gestational Diabetes Mellitus and Breastfeeding Benefits. Int. J. Environ. Res. Public Health 2021, 18, 10409. [Google Scholar] [CrossRef]
- Baranowska, B.; Malinowska, M.; Stanaszek, E.; Sys, D.; Bączek, G.; Doroszewska, A.; Tataj-Puzyna, U.; Rabijewski, M. Extended Breastfeeding in Poland: Knowledge of Health Care Providers and Attitudes on Breastfeeding Beyond Infancy. J. Hum. Lact. 2018, 35, 371–380. [Google Scholar] [CrossRef]
- De la Mora, A.; Russell, D.W.; Dungy, C.I.; Losch, M.; Dusdieker, L. The Iowa Infant Feeding Attitude Scale: Analysis of reli-ability and validity. J. Appl. Soc. Psychol. 1999, 29, 2362–2380. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics; Pearson: Los Angeles, CA, USA, 2019. [Google Scholar]
- Cristobal-Fransi, E.; Flavián, C.; Guinalíu, M. Perceived E-Service Quality (PeSQ) measurement validation and effects on consumer satisfaction and web site loyalty. Int. J. Qual. Serv. Sci. 2007, 17, 317–340. [Google Scholar] [CrossRef]
- Karmienie Piersią w Polsce Raport 2015; Kampania Mleko Mamy Rządzi; Patronat Merytoryczny Centrum Nauki o Laktacji: Warsaw, Poland, 2015.
- Królak-Olejnik, B.; Błasiak, I.; Szczygieł, A. Promotion of breastfeeding in Poland: The current situation. J. Int. Med. Res. 2017, 45, 1976–1984. [Google Scholar] [CrossRef]
- Family Larrson-Rosenquist Foudation. Breastfeeding and Breast Milk—From Biochemistry to Impact: A Multidisciplinary Introduction; Georg Thieme: Stuttgart, Germany; New York, NY, USA, 2018; pp. 32–38. [Google Scholar]
- Iliadou, M.; Lykeridou, K.; Prezerakos, P.; Tzavara, C.; Tziaferi, S. Reliability and Validity of the Greek Version of the Iowa Infant Feeding Attitude Scale among Pregnant Women. Mater. Socio-Med. 2019, 31, 160–165. [Google Scholar] [CrossRef]
- Nanishi, K.; Jimba, M. Reliability and Validity of the Japanese Version of the Iowa Infant Feeding Attitude Scale. J. Hum. Lact. 2014, 30, 346–352. [Google Scholar] [CrossRef]
- Charafeddine, L.; Tamim, H.; Soubra, M.; De La Mora, A.; Nabulsi, M.; Kabakian, T.; Yehya, N.; Sinno, D.; Masri, S. Research and Advocacy Breastfeeding Team Validation of the Arabic Version of the Iowa Infant Feeding Attitude Scale among Lebanese Women. J. Hum. Lact. 2015, 32, 309–314. [Google Scholar] [CrossRef]
- Ungváry, R.; Ittzés, A.; Bóné, V.; Török, S. Psychometric properties of the original and short Hungarian version of the Iowa Infant Feeding Attitude Scale. Int. Breastfeed. J. 2021, 16, 54. [Google Scholar] [CrossRef]
- Mathew, A.C.; Benny, J.K.; Philip, D.M.; Dhanya, C.; Joy, M.; Sandhiya, V.; Ramesh, S.; Neelakandan, K. Socio-Demographic and Clinical Correlates of Exclusive Breastfeeding practices up to Six Months of Age. Nepal J. Epidemiol. 2019, 9, 772–780. [Google Scholar] [CrossRef]
- Sarki, M.; Parlesak, A.; Robertson, A. Comparison of national cross-sectional breast-feeding surveys by maternal education in Europe (2006–2016). Public Health Nutr. 2018, 22, 848–861. [Google Scholar] [CrossRef] [Green Version]
- Masho, S.W.; Morris, M.R.; Wallenborn, J.T. Role of Marital Status in the Association between Prepregnancy Body Mass Index and Breastfeeding Duration. Women’s Health Issues 2016, 26, 468–475. [Google Scholar] [CrossRef]
- Barennes, H.; Empis, G.; Quang, T.D.; Sengkhamyong, K.; Phasavath, P.; Harimanana, A.; Sambany, E.M.; Koffi, P.N. Breast-Milk Substitutes: A New Old-Threat for Breastfeeding Policy in Developing Countries. A Case Study in a Traditionally High Breastfeeding Country. PLoS ONE 2012, 7, e30634. [Google Scholar] [CrossRef]
- Persad, M.D.; Mensinger, J.L. Maternal Breastfeeding Attitudes: Association with Breastfeeding Intent and Socio-demographics Among Urban Primiparas. J. Community Health 2007, 33, 53–60. [Google Scholar] [CrossRef]
- Perera, P.J.; Ranathunga, N.; Fernando, M.P.; Sampath, W.; Samaranayake, G.B. Actual exclusive breastfeeding rates and determinants among a cohort of children living in Gampaha district Sri Lanka: A prospective observational study. Int. Breastfeed. J. 2012, 7, 21. [Google Scholar] [CrossRef] [Green Version]
- Balogun, O.O.; Dagvadorj, A.; Anigo, K.M.; Ota, E.; Sasaki, S. Factors influencing breastfeeding exclusivity during the first 6 months of life in developing countries: A quantitative and qualitative systematic review. Matern. Child Nutr. 2015, 11, 433–451. [Google Scholar] [CrossRef]
- Ustawa z Dnia 26 Czerwca 1974 r. Kodeks Pracy. Dz.U.2020.1320. Obwieszczenie Marszałka Sejmu Rzeczypospolitej Polskiej z Dnia 18 Czerwca 2020 r. w Sprawie Ogłoszenia Jednolitego Tekstu Ustawy—Kodeks Pracy. Dz.U.2020.1320. Available online: http://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU20200001320/U/D20201320Lj.pdf (accessed on 2 October 2021).
- Laanterä, S.; Pölkki, T.; Ekström, A.; Pietilä, A.-M. Breastfeeding attitudes of Finnish parents during pregnancy. BMC Pregnancy Childbirth 2010, 10, 79. [Google Scholar] [CrossRef] [Green Version]
- Mbada, C.E.; Olowookere, A.E.; Faronbi, J.O.; Oyinlola-Aromolaran, F.C.; Faremi, F.A.; Ogundele, A.O.; Awotidebe, T.O.; Ojo, A.A.; Augustine, O.A. Knowledge, attitude and techniques of breastfeeding among Nigerian mothers from a semi-urban community. BMC Res. Notes 2013, 6, 552. [Google Scholar] [CrossRef] [Green Version]
- Cato, K.; Sylvén, S.M.; Henriksson, H.W.; Rubertsson, C. Breastfeeding as a balancing act—Pregnant Swedish women’s voices on breastfeeding. Int. Breastfeed. J. 2020, 15, 16–19. [Google Scholar] [CrossRef]
- Weker, H.; Barańska, M.; Riahi, A.; Strucińska, M.; Więch, M.; Rowicka, G.; Dyląg, H.; Klemarczyk, W.; Bzikowska, A.; Socha, P. Nutrition of infants and young children in Poland—Pitnuts 2016. Dev. Period. Med. 2017, 21, 13–28. [Google Scholar] [CrossRef]
- Guelinckx, I.; Devlieger, R.; Bogaerts, A.; Pauwels, S.; Vansant, G. The effect of pre-pregnancy BMI on intention, initiation and duration of breast-feeding. Public Health Nutr. 2012, 15, 840–848. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Escamilla, R.; Martinez, J.L.; Segura-Pérez, S. Impact of the Baby-friendly Hospital Initiative on breastfeeding and child health outcomes: A systematic review. Matern. Child Nutr. 2016, 12, 402–417. [Google Scholar] [CrossRef] [Green Version]
- Rozporządzenie Ministra Zdrowia z Dnia 16 Sierpnia 2018 r. w Sprawie Standardu Organizacyjnego Opieki Okołoporodowej. Dz.U. 2018.1756. Available online: https://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU20180001756/O/D20181756.pdf (accessed on 12 October 2021).
- Lyons, S.; Currie, S.; Peters, S.; Lavender, T.; Smith, D.M. The association between psychological factors and breastfeeding behaviour in women with a body mass index (BMI) ≥ 30 kg m−2: A systematic review. Obes. Rev. 2018, 19, 947–959. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.who.int/news-room/commentaries/detail/breastfeeding-and-covid-19 (accessed on 12 November 2021).
- Boateng, G.O.; Neilands, T.B.; Frongillo, E.A.; Melgar-Quiñonez, H.R.; Young, S. Best Practices for Developing and Validating Scales for Health, Social, and Behavioral Research: A Primer. Front. Public Health 2018, 6, 149. [Google Scholar] [CrossRef]
| Participants’ Characteristics | N | % | |
|---|---|---|---|
| Mean age (SD) | 29.90 (± 4.95), range 18–43 y/o * | ||
| Residence | Urban—province capital | 250 | 62.3 |
| Urban—other | 68 | 17.0 | |
| Rural | 83 | 20.7 | |
| Education | Primary/vocational | 40 | 10.0 |
| High school | 110 | 27.4 | |
| College/university | 251 | 62.6 | |
| Relationship status | Single | 61 | 15.2 |
| Married/in a stable relationship | 340 | 84.8 | |
| Self-assessed socio-economic status | Very good, good | 165 | 41.1 |
| Average | 228 | 56.9 | |
| Bad/very bad | 8 | 2.0 | |
| Worked before the pregnancy | Yes | 329 | 82.0 |
| No | 72 | 18.0 | |
| Return to work after the end of maternity leave | Yes | 323 | 80.5 |
| No | 78 | 19.5 | |
| Mode of delivery | Vaginal delivery | 217 | 54.1 |
| Cesarean section | 184 | 45.9 | |
| Parity | 1 | 195 | 48.6 |
| 2 | 144 | 35.9 | |
| 3 or higher | 62 | 15.5 | |
| Way of feeding the previous baby | Breastfeeding | 132 | 64.1 |
| Formula/combined | 74 | 35.9 | |
| Planned way of feeding now | Breastfeeding | 324 | 80.8 |
| Formula/combined | 77 | 19.2 | |
| Items | Positive Attitude towards Breastfeeding | Positive Attitude towards Formula Feeding | Item-Total Correlations | Cronbach’s α If Item Deleted |
|---|---|---|---|---|
| 1. The nutritional benefits of breast milk last only until the baby is weaned from breast milk. | 0.501 | 0.238 | 0.721 | |
| 2. Formula feeding is more convenient than breast-feeding. | 0.387 | 0.323 | 0.712 | |
| 3. Breast-feeding increases mother–infant bonding. | 0.467 | 0.214 | 0.722 | |
| 4. Breast milk is lacking in iron. | 0.608 | 0.201 | 0.728 | |
| 5. Formula-fed babies are more likely to be overfed than breast-fed babies. | 0.559 | 0.311 | 0.713 | |
| 6. Formula-feeding is the better choice if a mother plans to work outside the home. | 0.352 | 0.274 | 0.718 | |
| 7. Mothers who formula-feed miss one of the great joys of motherhood. | 0.651 | 0.398 | 0.703 | |
| 8. Women should not breast-feed in public places such as restaurants. | 0.452 | 0.201 | 0.724 | |
| 9. Babies fed breast milk are healthier than babies who are fed formula. | 0.687 | 0.377 | 0.706 | |
| 10. Breast-fed babies are more likely to be overfed than formula fed babies. | 0.501 | 0.387 | 0.706 | |
| 11. Fathers feel left out if a mother breast-feeds. | 0.715 | 0.289 | 0.715 | |
| 12. Breast milk is the ideal food for babies. | 0.570 | 0.380 | 0.708 | |
| 13. Breast milk is more easily digested than formula. | 0.535 | 0.395 | 0.705 | |
| 14. Formula is as healthy for an infant as breast milk. | 0.631 | 0.492 | 0.694 | |
| 15. Breast-feeding is more convenient than formula feeding. | 0.570 | 0.410 | 0.702 | |
| 16. Breast milk is less expensive than formula. | 0.505 | 0.313 | 0.714 | |
| 17. A mother who occasionally drinks alcohol should not breast-feed her baby. | −0.194 | −0.184 | --- | --- |
| % of variance explained | 19.90 | 11.28 | --- | --- |
| Attitude towards Feeding | 1st Stage of Research * M (±SD) (95% CI) | 2nd Stage of Research ** M (±SD) (95% CI) | 3rd Stage of Research *** M (±SD) (95% CI) | Statistical Analysis | |
|---|---|---|---|---|---|
| F | p | ||||
| Positive attitude towards breastfeeding | 32.67 (±4.57) (32.22–33.12) | 32.80 (±4.57) (32.37–33.23) | 32.04 (±3.82) (31.62–32.60) | 2.149 | 0.117 |
| Positive attitude towards formula feeding | 30.45 (±4.57) (30.00–30.90) | 30.81 (±4.13) (28.36–31.28) | 30.28 (±4.16) (29.76–30.76) | 1.105 | 0.332 |
| Total score | 63.12(±7.34) (62.40–63.85) | 63.60 (±6.29) (62.90–64.37) | 62.29 (±6.52) (61.36–63.17) | 2.251 | 0.106 |
| Variables | PolIIFAS | Statistical Analysis | |||
|---|---|---|---|---|---|
| M | (±SD) | F/t | p | ||
| Age | 0.108 ** | 0.031 | |||
| Residence | Urban—province capital | 63.83 | 7.37 | 3.227 | 0.041 |
| Urban—other | 61.60 | 7.48 | |||
| Rural | 62.25 | 6.96 | |||
| Education | Primary/vocational | 61.08 | 6.24 | 3.541 | 0.030 |
| High school | 62.25 | 7.39 | |||
| College/university | 63.83 | 7.41 | |||
| Relationship status | Single | 59.05 | 5.89 | −4.837 | <0.001 |
| Married/in a stable relationship | 63.86 | 7.35 | |||
| Perceived family wealth | Very wealthy/rather wealthy | 64.20 | 7.39 | 3.481 | 0.032 |
| Average | 62.46 | 7.18 | |||
| Rather poor/poor | 60.00 | 8.78 | |||
| Worked before the pregnancy | Yes | 63.89 | 7.12 | 4.594 | <0.001 |
| No | 59.61 | 7.35 | |||
| Return to work after the end of maternity leave | Yes | 63.97 | 7.10 | 4.814 | <0.001 |
| No | 59.63 | 7.33 | |||
| Parity | 1 | 63.30 | 7.28 | 0.500 | 0.607 |
| 2 | 62.66 | 7.78 | |||
| 3 or higher | 63.65 | 6.49 | |||
| Mode of delivery | Vaginal delivery | 63.62 | 6.86 | 1.462 | 0.145 |
| Cesarean section | 62.54 | 7.86 | |||
| Way of feeding the previous baby | Breastfeeding | 64.30 | 6.87 | 6.969 | <0.001 |
| Formula/combined | 58.17 | 7.23 | |||
| Planned way of feeding now | Breastfeeding | 63.95 | 6.40 | 2.618 | 0.010 |
| Formula/combined | 61.18 | 8.71 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bień, A.; Kulesza-Brończyk, B.; Przestrzelska, M.; Iwanowicz-Palus, G.; Ćwiek, D. The Attitudes of Polish Women towards Breastfeeding Based on the Iowa Infant Feeding Attitude Scale (IIFAS). Nutrients 2021, 13, 4338. https://doi.org/10.3390/nu13124338
Bień A, Kulesza-Brończyk B, Przestrzelska M, Iwanowicz-Palus G, Ćwiek D. The Attitudes of Polish Women towards Breastfeeding Based on the Iowa Infant Feeding Attitude Scale (IIFAS). Nutrients. 2021; 13(12):4338. https://doi.org/10.3390/nu13124338
Chicago/Turabian StyleBień, Agnieszka, Bożena Kulesza-Brończyk, Monika Przestrzelska, Grażyna Iwanowicz-Palus, and Dorota Ćwiek. 2021. "The Attitudes of Polish Women towards Breastfeeding Based on the Iowa Infant Feeding Attitude Scale (IIFAS)" Nutrients 13, no. 12: 4338. https://doi.org/10.3390/nu13124338
APA StyleBień, A., Kulesza-Brończyk, B., Przestrzelska, M., Iwanowicz-Palus, G., & Ćwiek, D. (2021). The Attitudes of Polish Women towards Breastfeeding Based on the Iowa Infant Feeding Attitude Scale (IIFAS). Nutrients, 13(12), 4338. https://doi.org/10.3390/nu13124338