
The Short-Term Effects and Tolerability of Low-Viscosity Soluble Fibre on Gastroparesis Patients: A Pilot Clinical Intervention Study




Abstract
1. Introduction
2. Materials and Methods
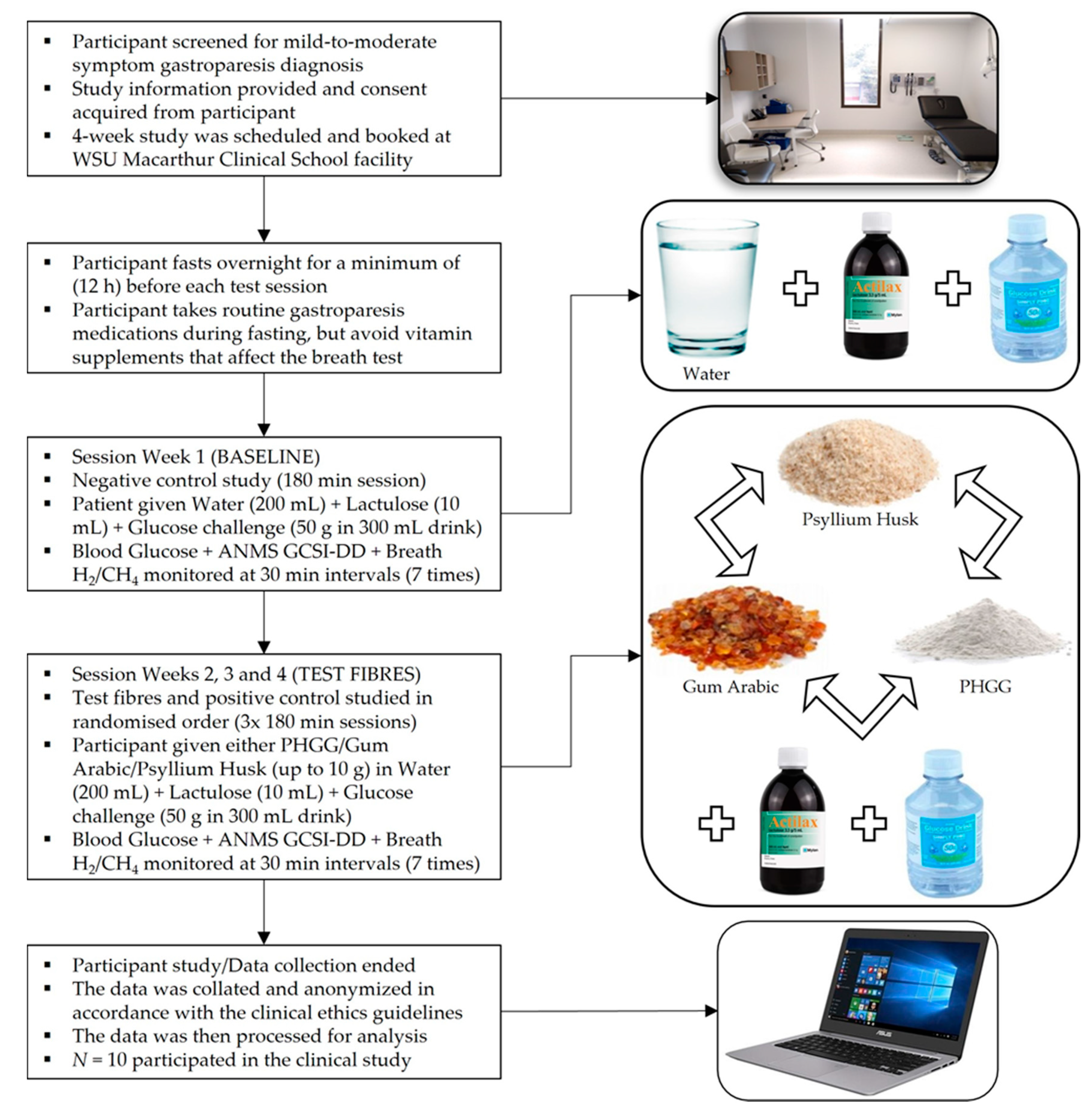
2.1. Study Design & Premises
2.2. Participant Diagnosis & Eligibility
2.3. Inclusion & Exclusion Criteria and Risks
2.4. Participant Recruitment
2.5. Data Curation & Analysis
3. Results
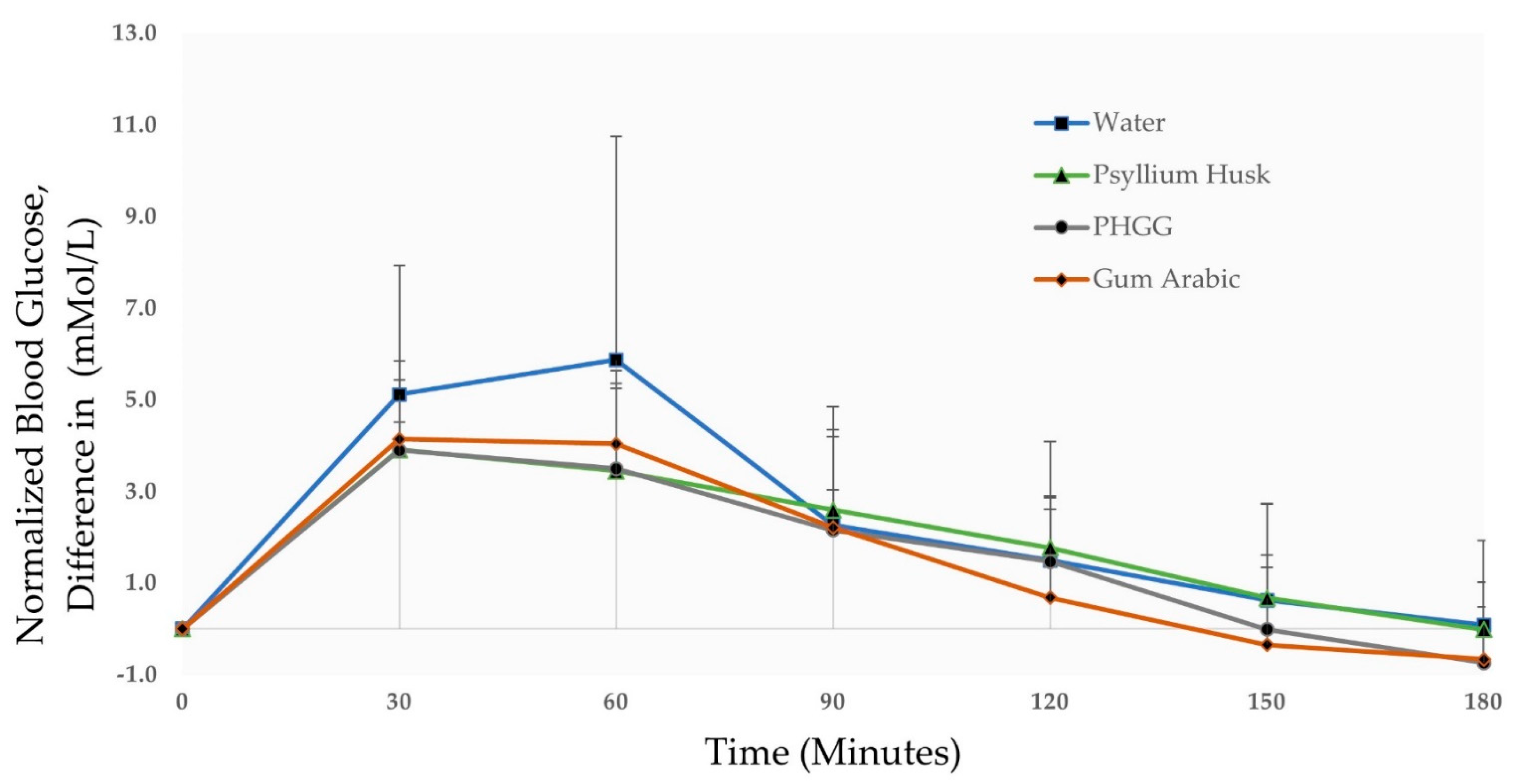
3.1. Blood Glucose Monitoring
3.2. ANMS GCSI-DD Monitoring
3.3. Breath Hydrogen/Methane Monitoring
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jehangir, A.; Parkman, H.P. Role of Gastric Emptying in Symptoms of Gastroparesis. Gastrointest. Disord. 2019, 1, 32. [Google Scholar] [CrossRef]
- Hasler, W.L. Gastroparesis: Symptoms, evaluation, and treatment. Gastroenterol. Clin. N. Am. 2007, 36, 619–647. [Google Scholar] [CrossRef] [PubMed]
- Woodhouse, S.; Hebbard, G.; Knowles, S.R. Psychological controversies in gastroparesis: A systematic review. World J. Gastroenterol. 2017, 23, 1298–1309. [Google Scholar] [CrossRef] [PubMed]
- Saliakellis, E.; Fotoulakib, M. Gastroparesis in children. Ann. Gastroenterol. 2013, 26, 204–211. [Google Scholar] [PubMed]
- Parkman, H.P.; Yates, K.; Hasler, W.L.; Nguyen, L.; Pasricha, P.J.; Snape, W.J.; Farrugia, G.; Koch, K.L.; Abell, T.L.; McCallum, R.W.; et al. Clinical features of idiopathic gastroparesis vary with sex, body mass, symptom onset, delay in gastric emptying, and gastroparesis severity. Gastroenterology 2011, 140, 101–115. [Google Scholar] [CrossRef]
- Liu, N.; Abell, T. Gastroparesis Updates on Pathogenesis and Management. Gut Liver 2017, 11, 579–589. [Google Scholar] [CrossRef] [PubMed]
- Heetun, Z.S.; Quigley, E.M. Gastroparesis and Parkinson’s disease: A systematic review. Parkinsonism. Relat. Disord. 2012, 18, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Alomari, M.; Hitawala, A.; Chadalavada, P.; Covut, F.; Al Momani, L.; Khazaaleh, S.; Gosai, F.; Al Ashi, S.; Abushahin, A.; Schneider, A. Prevalence and Predictors of Gastrointestinal Dysmotility in Patients with Hypermobile Ehlers-Danlos Syndrome: A Tertiary Care Center Experience. Cureus 2020, 12, e7881. [Google Scholar] [CrossRef] [PubMed]
- Reddymasu, S.C.; Bonino, J.; McCallum, R.W. Gastroparesis secondary to a demyelinating disease: A case series. BMC Gastroenterol. 2007, 7, 3. [Google Scholar] [CrossRef] [PubMed]
- Brand-Miller, J.C.; Atkinson, F.S.; Gahler, R.J.; Kacinik, V.; Lyon, M.R.; Wood, S. Effects of PGX, a novel functional fibre, on acute and delayed postprandial glycaemia. Eur. J. Clin. Nutr. 2010, 64, 1488–1493. [Google Scholar] [CrossRef]
- Office of Nutrition and Food Labeling. Science Review of Isolated and Synthetic Non-Digestible Carbohydrates; Center for Food Safety and Applied Nutrition, Food and Drug Administration, US Department of Health and Human Services: College Park, MD, USA, 2016. Available online: https://www.fda.gov/food/food-labeling-nutrition/science-review-isolated-and-synthetic-non-digestible-carbohydrates/ (accessed on 1 July 2021).
- Lattimer, J.M.; Haub, M.D. Effects of dietary fiber and its components on metabolic health. Nutrients 2010, 2, 1266–1289. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, M.P.; Ishihara, N.; Okubo, T. Soluble dietary fibre partially hydrolysed guar gum markedly impacts on postprandial hyperglycaemia, hyperlipidaemia and incretins metabolic hormones over time in healthy and glucose intolerant subjects. J. Funct. Foods 2016, 24, 207–220. [Google Scholar] [CrossRef]
- Babio, N.; Balanza, R.; Basulto, J.; Bulló, M.; Salas-Salvadó, J. Dietary fibre: Influence on body weight, glycemic control and plasma cholesterol profile. Nutr. Hosp. 2010, 25. [Google Scholar] [CrossRef]
- Chen, C.; Zeng, Y.; Xu, J.; Zheng, H.; Liu, J.; Fan, R.; Zhu, W.; Yuan, L.; Qin, Y.; Chen, S.; et al. Therapeutic effects of soluble dietary fiber consumption on type 2 diabetes mellitus. Exp. Ther. Med. 2016, 12, 1232–1242. [Google Scholar] [CrossRef] [PubMed]
- Ylönen, K.; Saloranta, C.; Kronberg-Kippilä, C.; Groop, L.; Aro, A.; Virtanen, S.M.; Study, B.D. Associations of Dietary Fiber With Glucose Metabolism in Nondiabetic Relatives of Subjects With Type 2 Diabetes. Diabetes Care 2003, 26, 1979–1985. [Google Scholar] [CrossRef]
- Niv, E.; Halak, A.; Tiommny, E.; Yanai, H.; Strul, H.; Naftali, T.; Vaisman, N. Randomized clinical study: Partially hydrolyzed guar gum (PHGG) versus placebo in the treatment of patients with irritable bowel syndrome. Nutr. Metab. 2016, 13, 10. [Google Scholar] [CrossRef] [PubMed]
- Russo, L.; Andreozzi, P.; Zito, F.P.; Vozzella, L.; Savino, I.G.; Sarnelli, G.; Cuomo, R. Partially hydrolyzed guar gum in the treatment of irritable bowel syndrome with constipation: Effects of gender, age, and body mass index. Saudi J. Gastroenterol. 2015, 21, 104–110. [Google Scholar] [CrossRef] [PubMed]
- McRorie, J.W., Jr. Evidence-Based Approach to Fiber Supplements and Clinically Meaningful Health Benefits, Part 1: What to Look for and How to Recommend an Effective Fiber Therapy. Nutr. Today 2015, 50, 82–89. [Google Scholar] [CrossRef] [PubMed]
- McRorie, J.W., Jr.; McKeown, N.M. Understanding the Physics of Functional Fibers in the Gastrointestinal Tract: An Evidence-Based Approach to Resolving Enduring Misconceptions about Insoluble and Soluble Fiber. J. Acad. Nutr. Diet. 2017, 117, 251–264. [Google Scholar] [CrossRef] [PubMed]
- Parada Venegas, D.; De la Fuente, M.K.; Landskron, G.; Gonzalez, M.J.; Quera, R.; Dijkstra, G.; Harmsen, H.J.M.; Faber, K.N.; Hermoso, M.A. Short Chain Fatty Acids (SCFAs)-Mediated Gut Epithelial and Immune Regulation and Its Relevance for Inflammatory Bowel Diseases. Front. Immunol. 2019, 10, 277. [Google Scholar] [CrossRef]
- Reider, S.J.; Moosmang, S.; Tragust, J.; Trgovec-Greif, L.; Tragust, S.; Perschy, L.; Przysiecki, N.; Sturm, S.; Tilg, H.; Stuppner, H.; et al. Prebiotic Effects of Partially Hydrolyzed Guar Gum on the Composition and Function of the Human Microbiota-Results from the PAGODA Trial. Nutrients 2020, 12, 1257. [Google Scholar] [CrossRef] [PubMed]
- Furnari, M.; Parodi, A.; Gemignani, L.; Giannini, E.G.; Marenco, S.; Savarino, E.; Assandri, L.; Fazio, V.; Bonfanti, D.; Inferrera, S.; et al. Clinical trial: The combination of rifaximin with partially hydrolysed guar gum is more effective than rifaximin alone in eradicating small intestinal bacterial overgrowth. Aliment. Pharm. Ther. 2010, 32, 1000–1006. [Google Scholar] [CrossRef]
- Howarth, N.C.; Saltzman, E.; Roberts, S.B. Dietary fiber and weight regulation. Nutr. Rev. 2001, 59, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Fayet-Moore, F.; Cassettari, T.; Tuck, K.; McConnell, A.; Petocz, P. Dietary Fibre Intake in Australia. Paper I: Associations with Demographic, Socio-Economic, and Anthropometric Factors. Nutrients 2018, 10, 599. [Google Scholar] [CrossRef]
- Parkman, H.P.; Yates, K.P.; Hasler, W.L.; Nguyan, L.; Pasricha, P.J.; Snape, W.J.; Farrugia, G.; Calles, J.; Koch, K.L.; Abell, T.L.; et al. Dietary intake and nutritional deficiencies in patients with diabetic or idiopathic gastroparesis. Gastroenterology 2011, 141, 486–498.e7. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M.; Parkman, H.P.; Shafi, M.A.; Abell, T.L.; Gerson, L.; American College of Gastroenterology. Clinical guideline: Management of gastroparesis. Am. J. Gastroenterol. 2013, 108, 18–37. [Google Scholar] [CrossRef]
- Parrish, C.R.; McCray, S. Gastroparesis & nutrition: The art. Pract. Gastroenterol. 2011, 35, 26–41. [Google Scholar]
- Suresh, H.; Ho, V.; Zhou, J. Rheological Characteristics of Soluble Fibres during Chemically Simulated Digestion and their Suitability for Gastroparesis Patients. Nutrients 2020, 12, 2479. [Google Scholar] [CrossRef]
- Pastors, J.G.; Blaisdell, P.W.; Balm, T.K.; Asplin, C.M.; Pohl, S.L. Psyllium fiber reduces rise in postprandial glucose and insulin concentrations in patients with non-insulin-dependent diabetes. Am. J. Clin. Nutr. 1991, 53, 1431–1435. [Google Scholar] [CrossRef] [PubMed]
- Abutair, A.S.; Naser, I.A.; Hamed, A.T. Soluble fibers from psyllium improve glycemic response and body weight among diabetes type 2 patients (randomized control trial). Nutr. J. 2016, 15, 86. [Google Scholar] [CrossRef]
- Yoon, S.; Chu, D.; Juneja, L.R. Physiological Functions of Partially Hydrolyzed Guar Gum. J. Clin. Biochem. Nutr. 2006, 39, 134–144. [Google Scholar] [CrossRef][Green Version]
- Alam, N.H.; Meier, R.; Rausch, T.; Meyer-Wyss, B.; Hildebrand, P.; Schnieder, H.; Bachmann, C.; Minder, E.; Fowler, B.; Gyr, K. Effects of a partially hydrolyzed guar gum on intestinal absorption of carbohydrate, protein and fat: A double-blind controlled study in volunteers. Clin. Nutr. 1998, 17, 125–129. [Google Scholar] [CrossRef]
- Cherbut, C.; Michel, C.; Raison, V.; Kravtchenko, T.; Severine, M. Acacia Gum is a Bifidogenic Dietary Fibre with High Digestive Tolerance in Healthy Humans. Microb. Ecol. Health Dis. 2009, 15, 43–50. [Google Scholar] [CrossRef]
- Babiker, R.; Elmusharaf, K.; Keogh, M.B.; Banaga, A.S.I.; Saeed, A.M. Metabolic effects of Gum Arabic (Acacia Senegal) in patients with Type 2 Diabetes Mellitus (T2DM): Randomized, placebo controlled double blind trial. Funct. Foods Health Dis. 2017, 7, 219–231. [Google Scholar] [CrossRef]
- Revicki, D.A.; Rentz, A.M.; Dubois, D.; Kahrilas, P.; Stanghellini, V.; Talley, N.J.; Tack, J. Gastroparesis Cardinal Symptom Index (GCSI): Development and validation of a patient reported assessment of severity of gastroparesis symptoms. Qual. Life Res. 2004, 13, 833–844. [Google Scholar] [CrossRef]
- Revicki, D.A.; Camilleri, M.; Kuo, B.; Norton, N.J.; Murray, L.; Palsgrove, A.; Parkman, H.P. Development and content validity of a gastroparesis cardinal symptom index daily diary. Aliment. Pharm. Ther. 2009, 30, 670–680. [Google Scholar] [CrossRef]
- Revicki, D.A.; Camilleri, M.; Kuo, B.; Szarka, L.A.; McCormack, J.; Parkman, H.P. Evaluating symptom outcomes in gastroparesis clinical trials: Validity and responsiveness of the Gastroparesis Cardinal Symptom Index-Daily Diary (GCSI-DD). Neurogastroenterol. Motil. 2012, 24, 456–463. [Google Scholar] [CrossRef]
- Revicki, D.A.; Lavoie, S.; Speck, R.M.; Puelles, J.; Kuo, B.; Camilleri, M.; Almansa, C.; Parkman, H.P. The content validity of the ANMS GCSI-DD in patients with idiopathic or diabetic gastroparesis. J. Patient Rep. Outcomes. 2018, 2, 61. [Google Scholar] [CrossRef]
- Rana, S.V.; Malik, A. Hydrogen breath tests in gastrointestinal diseases. Indian J. Clin. Biochem. 2014, 29, 398–405. [Google Scholar] [CrossRef]
- Cook, I.J.; Irvine, E.J.; Campbell, D.; Shannon, S.; Reddy, S.N.; Collins, S.M. Effect of dietary fiber on symptoms and rectosigmoid motility in patients with irritable bowel syndrome. A controlled, crossover study. Gastroenterology 1990, 98, 66–72. [Google Scholar] [CrossRef]
- The American Neurogastroenterology and Motility Society. User Manual for the ANMS GCSI-DD, The American Neurogastroenterology and Motility Society Gastroparesis Cardinal Symptom Index Daily Diary; The American Neurogastroenterology and Motility Society, USA. 2018. Available online: https://www.fda.gov/media/125038/download/ (accessed on 1 July 2021).
- Abell, T.L.; Camilleri, M.; Donohoe, K.; Hasler, W.L.; Lin, H.C.; Maurer, A.H.; McCallum, R.W.; Nowak, T.; Nusynowitz, M.L.; Parkman, H.P.; et al. Consensus recommendations for gastric emptying scintigraphy: A joint report of the American Neurogastroenterology and Motility Society and the Society of Nuclear Medicine. J. Nucl. Med. Technol. 2008, 36, 44–54. [Google Scholar] [CrossRef]
- Bielefeldt, K. Gastroparesis: Concepts, controversies, and challenges. Scientifica 2012, 2012, 424802. [Google Scholar] [CrossRef]
- Caio, G.; Volta, U.; Sapone, A.; Leffler, D.A.; De Giorgio, R.; Catassi, C.; Fasano, A. Celiac disease: A comprehensive current review. BMC Med. 2019, 17, 142. [Google Scholar] [CrossRef] [PubMed]
- Center for Drug Evaluation and Research (CDER). Gastroparesis: Clinical Evaluation of Drugs for Treatment Guidance for Industry; Food and Drug Administration, US Department of Health and Human Services: Maryland City, MD, USA, 2016. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/gastroparesis-clinical-evaluation-drugs-treatment-guidance-industry/ (accessed on 1 July 2021).
- Frier, B.M.; Schernthaner, G.; Heller, S.R. Hypoglycemia and cardiovascular risks. Diabetes Care 2011, 34 (Suppl. S2), S132–S137. [Google Scholar] [CrossRef] [PubMed]
- Cryer, P.E.; Axelrod, L.; Grossman, A.B.; Heller, S.R.; Montori, V.M.; Seaquist, E.R.; Service, F.J.; Endocrine, S. Evaluation and management of adult hypoglycemic disorders: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2009, 94, 709–728. [Google Scholar] [CrossRef] [PubMed]
- Aronoff, S.L.; Berkowitz, K.; Shreiner, B.; Want, L. Glucose Metabolism and Regulation: Beyond Insulin and Glucagon. Diabetes Spectr. 2004, 17, 183–190. [Google Scholar] [CrossRef]
- Farrell, M.B. Gastric Emptying Scintigraphy. J. Nucl. Med. Technol. 2019, 47, 111–119. [Google Scholar] [CrossRef]
- Dukowicz, A.C.; Lacy, B.E.; Levine, G.M. Small intestinal bacterial overgrowth: A comprehensive review. Gastroenterol. Hepatol. 2007, 3, 112–122. [Google Scholar]
- Chen, L.; Tuo, B.; Dong, H. Regulation of Intestinal Glucose Absorption by Ion Channels and Transporters. Nutrients. 2016, 8, 43. [Google Scholar] [CrossRef] [PubMed]
- Russell, W.R.; Baka, A.; Bjorck, I.; Delzenne, N.; Gao, D.; Griffiths, H.R.; Hadjilucas, E.; Juvonen, K.; Lahtinen, S.; Lansink, M.; et al. Impact of Diet Composition on Blood Glucose Regulation. Crit. Rev. Food Sci. Nutr. 2016, 56, 541–590. [Google Scholar] [CrossRef]
- Reynolds, A.N.; Akerman, A.P.; Mann, J. Dietary fibre and whole grains in diabetes management: Systematic review and meta-analyses. PLoS Med. 2020, 17, e1003053. [Google Scholar] [CrossRef] [PubMed]
- Kamal, E.; Kaddam, L.A.; Dahawi, M.; Osman, M.; Salih, M.A.; Alagib, A.; Saeed, A. Gum Arabic Fibers Decreased Inflammatory Markers and Disease Severity Score among Rheumatoid Arthritis Patients, Phase II Trial. Int. J. Rheumatol. 2018, 2018, 4197537. [Google Scholar] [CrossRef] [PubMed]
- Mann, J.I.; De Leeuw, I.; Hermansen, K.; Karamanos, B.; Karlström, B.; Katsilambros, N.; Riccardi, G.; Rivellese, A.A.; Rizkalla, S.; Slama, G.; et al. Evidence-based nutritional approaches to the treatment and prevention of diabetes mellitus. Nutr. Metab. Cardiovasc. Dis. 2004, 14, 373–394. [Google Scholar] [CrossRef]
- Rehman, K.U.; Codipilly, C.N.; Wapnir, R.A. Modulation of small intestinal nitric oxide synthase by gum arabic. Exp. Biol. Med. 2004, 229, 895–901. [Google Scholar] [CrossRef]
- Seino, S.; Shibasaki, T.; Minami, K. Dynamics of insulin secretion and the clinical implications for obesity and diabetes. J. Clin. Investig. 2011, 121, 2118–2125. [Google Scholar] [CrossRef] [PubMed]
- Gerich, J.E. Is Reduced First-Phase Insulin Release the Earliest Detectable Abnormality in Individuals Destined to Develop Type 2 Diabetes? Diabetes 2002, 51, S117–S121. [Google Scholar] [CrossRef]
- de Andrade Mesquita, L.; Pavan Antoniolli, L.; Cittolin-Santos, G.F.; Gerchman, F. Distinct metabolic profile according to the shape of the oral glucose tolerance test curve is related to whole glucose excursion: A cross-sectional study. BMC Endocr. Disord. 2018, 18, 56. [Google Scholar] [CrossRef] [PubMed]
- Draper, E.R.; Adams, D.J. Low-Molecular-Weight Gels: The State of the Art. Chem 2017, 3, 390–410. [Google Scholar] [CrossRef]
- Dikeman, C.L.; Fahey, G.C. Viscosity as related to dietary fiber: A review. Crit. Rev. Food Sci. Nutr. 2006, 46, 649–663. [Google Scholar] [CrossRef]
- Cronin, P.; Joyce, S.A.; O’Toole, P.W.; O’Connor, E.M. Dietary Fibre Modulates the Gut Microbiota. Nutrients 2021, 13, 1655. [Google Scholar] [CrossRef] [PubMed]
- Sanger, G.J.; Broad, J.; Andrews, P.L. The relationship between gastric motility and nausea: Gastric prokinetic agents as treatments. Eur. J. Pharm. 2013, 715, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Koch, K.L. Gastric dysrhythmias: A potential objective measure of nausea. Exp. Brain Res. 2014, 232, 2553–2561. [Google Scholar] [CrossRef]
- Yasukawa, Z.; Inoue, R.; Ozeki, M.; Okubo, T.; Takagi, T.; Honda, A.; Naito, Y. Effect of Repeated Consumption of Partially Hydrolyzed Guar Gum on Fecal Characteristics and Gut Microbiota: A Randomized, Double-Blind, Placebo-Controlled, and Parallel-Group Clinical Trial. Nutrients 2019, 11, 2170. [Google Scholar] [CrossRef]
- Kershaw, J.C.; Mattes, R.D. Nutrition and taste and smell dysfunction. World J. Otorhinolaryngol. Head Neck Surg. 2018, 4, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Mudgil, D.; Barak, S.; Khatkar, B.S. Guar gum: Processing, properties and food applications-A Review. J. Food Sci. Technol. 2014, 51, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, J.; Ramaswamy, H.S.; Ngadi, M.O. Rheological Characteristics of Arabic Gum in Combination with Guar and Xanthan Gum Using Response Surface Methodology: Effect of Temperature and Concentration. Int. J. Food Prop. 2005, 8, 179–192. [Google Scholar] [CrossRef]
- National Institute of Diabetes and Digestive and Kidney Diseases. Symptoms & Causes of Gastroparesis; US Department of Health and Human Services: Washington, DC, USA, 2016. Available online: https://www.niddk.nih.gov/health-information/digestive-diseases/gastroparesis/symptoms-causes/ (accessed on 1 September 2021).
- Lambeau, K.V.; McRorie, J.W., Jr. Fiber supplements and clinically proven health benefits: How to recognize and recommend an effective fiber therapy. J. Am. Assoc. Nurse Pract. 2017, 29, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Capuano, E. The behavior of dietary fiber in the gastrointestinal tract determines its physiological effect. Crit. Rev. Food Sci. Nutr. 2017, 57, 3543–3564. [Google Scholar] [CrossRef]
- Mariani, H.S.; Layden, B.T.; Aleppo, G. Continuous Glucose Monitoring: A Perspective on Its Past, Present, and Future Applications for Diabetes Management. Clin. Diabetes 2017, 35, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Bartholome, R.; Salden, B.; Vrolijk, M.F.; Troost, F.J.; Masclee, A.; Bast, A.; Haenen, G.R. Paracetamol as a Post Prandial Marker for Gastric Emptying, A Food-Drug Interaction on Absorption. PLoS ONE 2015, 10, e0136618. [Google Scholar] [CrossRef]
- Braden, B.; Lembcke, B.; Kuker, W.; Caspary, W.F. 13C-breath tests: Current state of the art and future directions. Dig. Liver Dis. 2007, 39, 795–805. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.W.; Lamont, K.L.; Stoltenberg, J.N.; Brannan, G.D. A Low Cost, Novel Treatment of Severe Diabetic Gastroparesis Based on Burkitt’s Dietary Fiber Hypothesis. Cureus 2021, 13, e18062. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographic Information (Units) | Value |
|---|---|
| Number of Participants | 10 |
| Gender (Female/Male) | 10/0 |
| Age (Years, Mean ± SD) | 38.5 ± 17.8 |
| BMI (Index, Mean ± SD) | 29.3 ± 11.7 |
| Etiology of Gastroparesis (Idiopathic/Diabetic) | 7/3 |
| Test Meal (In 200 mL Water) | Average Meal Consumed (g) ± (SD) | Mean Normalized Blood Glucose Differences (mMol/L) ± (SD), Interval Area under the Curve or iAUC (mMol·min/L), Time to Baseline (min) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| At 30 min | At 60 min | iAUC (1 h) | At 90 min | At 120 min | iAUC (2 h) | At 150 min | At 180 min | TTB | ||
| Water (Negative control) | 0 (0) * | 5.1 (2.8) | 5.9 (4.9) ** | 241.83 | 2.3 (0.8) | 1.5 (1.4) | 420.83 | 0.6 (2.1) | 0.1 (1.8) | 180 min |
| Psyllium Husk (Positive control) | 4.13 (1.18) | 3.9 (0.6) ** | 3.5 (1.9) | 169.13 | 2.6 (2.2) | 1.8 (2.3) | 325.50 | 0.7 (2.1) | 0.0 (1.0) | 180 min |
| PHGG (Test fibre 1) | 7.99 (1.92) | 3.9 (1.5) ** | 3.5 (1.8) | 169.50 | 2.2 (2.0) | 1.5 (1.4) | 309.00 | 0.0 (1.6) | −0.7 (1.2) | 150 min |
| Gum Arabic (Test fibre 2) | 7.57 (1.54) | 4.1 (1.7) ** | 4.0 (1.6) | 184.93 | 2.2 (2.1) | 0.7 (1.9) | 322.29 | −0.3 (1.7) | −0.7 (0.6) | 150 min |
| Mean Normalized ANMS GCSI-DD Scores ± (SD) (n = 10) | ||||||
|---|---|---|---|---|---|---|
| Symptom Subscale (Composite No.) | GCSI-DD (Symptom) | Baseline Mean (Pre-Meal Scores) * | Water (Negative Control) | Psyllium Husk (Positive Control) | PHGG (Test Fibre 1) | Gum Arabic (Test Fibre 2) |
| Nausea/Vomiting (1) | Nausea | 1.55 (1.15) | 0.04 (1.22) | 0.90 (0.73) | 1.00 (1.41) | 0.12 (0.72) |
| Retching | 0.45 (0.83) | −0.31 (1.03) | 0.04 (0.63) | 0.71 (1.47) | 0.05 (0.13) | |
| Vomiting | 0.40 (0.81) | −0.37 (1.11) | 0.60 (1.16) | 0.85 (1.33) | 0.05 (0.13) | |
| Post-prandial Fullness/Early Satiety (2) | Stomach Fullness | 2.43 (1.91) | 0.17 (1.22) | 1.40 (1.22) | 0.35 (1.04) | 0.40 (0.95) |
| Early Satiety * | 3.35 (0.91) | −0.78 (0.97) | 0.88 (0.64) ** | −0.38 (1.69) | 0.43 (0.98) | |
| Post-prandial Fullness * | 3.83 (0.73) | −0.22 (0.83) | 0.25 (0.46) | 0.00 (0.53) | 0.29 (0.76) | |
| Loss of Appetite | 2.58 (1.82) | −0.41 (0.92) | 1.10 (1.51) ** | 0.63 (1.02) ** | 1.17 (1.52) ** | |
| Bloating/Distension (3) | Bloating | 2.10 (1.68) | −0.17 (0.70) | 1.52 (1.14) ** | 0.44 (0.94) | 0.50 (0.64) **, *** |
| Belly Visibly Larger | 1.88 (1.77) | −0.17 (0.60) | 1.27 (1.09) ** | 0.35 (0.71) | 0.12 (0.44) *** | |
| Composite Scores | Composite (1) | 0.80 (1.06) | −0.22 (1.10) | 0.51 (0.48) ** | 0.85 (1.30) | 0.07 (0.29) |
| Composite (2) | 3.04 (1.50) | −0.31 (0.65) | 0.91 (0.70) ** | 0.15 (0.75) *** | 0.57 (0.64) **, *** | |
| Composite (3) | 1.99 (1.68) | −0.17 (0.56) | 1.40 (1.09) ** | 0.40 (0.82) | 0.31 (0.48) **, *** | |
| Demographic Information | Participants (out of 10) |
|---|---|
| Number of Participants | 10 |
| H2 producer | 7/10 |
| H2 + CH4 producer | 3/10 |
| SIBO (Already diagnosed) | 2/10 |
| Mouth-to-Caecum Reaching/Starting Transit (6 < ppm < 12, within 180 min) | Participants (out of 10) |
| Any sign of transit | 5/10 |
| Water meal | 3/10 |
| Psyllium Husk meal | 1/10 |
| PHGG meal | 4/10 |
| Gum Arabic meal | 2/10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suresh, H.; Zhou, J.; Ho, V. The Short-Term Effects and Tolerability of Low-Viscosity Soluble Fibre on Gastroparesis Patients: A Pilot Clinical Intervention Study. Nutrients 2021, 13, 4298. https://doi.org/10.3390/nu13124298
Suresh H, Zhou J, Ho V. The Short-Term Effects and Tolerability of Low-Viscosity Soluble Fibre on Gastroparesis Patients: A Pilot Clinical Intervention Study. Nutrients. 2021; 13(12):4298. https://doi.org/10.3390/nu13124298
Chicago/Turabian StyleSuresh, Harsha, Jerry Zhou, and Vincent Ho. 2021. "The Short-Term Effects and Tolerability of Low-Viscosity Soluble Fibre on Gastroparesis Patients: A Pilot Clinical Intervention Study" Nutrients 13, no. 12: 4298. https://doi.org/10.3390/nu13124298
APA StyleSuresh, H., Zhou, J., & Ho, V. (2021). The Short-Term Effects and Tolerability of Low-Viscosity Soluble Fibre on Gastroparesis Patients: A Pilot Clinical Intervention Study. Nutrients, 13(12), 4298. https://doi.org/10.3390/nu13124298