
Cost and Cost Effectiveness of a Pilot m-Health Intervention Targeting Parents of School-Aged Children to Improve the Nutritional Quality of Foods Packed in the Lunchbox

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Intervention
2.1.1. Study Design and Setting
2.1.2. Participants and Recruitment
2.1.3. SWAP IT Intervention
- Weekly support messages to parents: an existing school mobile communication app (Skoolbag) was used to communicate healthy lunchbox messages to parents. For one school term, push notifications were sent to parents providing tips and suggestions to assist in encouraging simple swaps from common discretionary foods to ‘everyday’ foods consistent with dietary guidelines.
- Physical resources: Students were provided with an information package with tools and resources that included a lunchbox ideas booklet, an ice brick and a drink bottle.
- School nutrition guidelines: Schools received support from health promotion project officers to develop nutrition guidelines that encouraged the packing of ‘everyday’ foods in the lunchbox in place of discretionary food products.
- Lunchbox flipchart lessons: Teachers were provided with a ten-page flipchart that featured different lunchbox examples and ideas to facilitate discussion in the classroom on healthy lunchboxes.
2.1.4. Control Schools
2.1.5. Measurement of Trial Outcomes
2.1.6. School Lunchbox Energy
2.2. Economic Study
2.2.1. Intervention Costs (Procedures and Measures)
2.2.2. Cost Effectiveness Analysis
2.2.3. Stochastic Analysis of Uncertainty
2.2.4. Handling of Missing Data
3. Results
3.1. Schools and Participants
3.2. Trial Outcomes
3.3. Intervention Costs
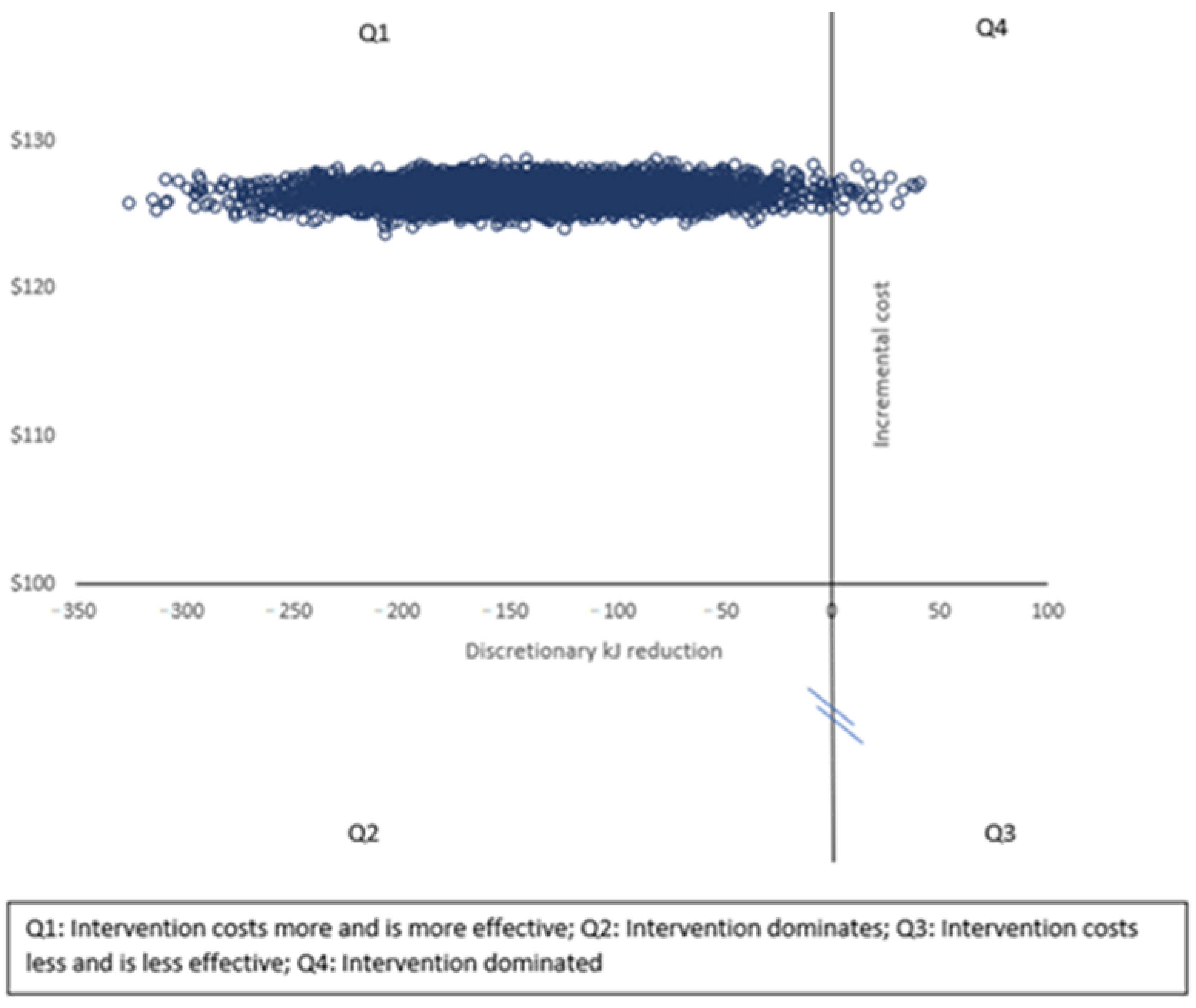
3.4. Incremental Cost Effectiveness Ratios
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Section/Item | Item No | Recommendation | Reported on Page No/Line No |
|---|---|---|---|
| Title and abstract | |||
| Title | 1 | Identify the study as an economic evaluation or use more specific terms such as “cost-effectiveness analysis”, and describe the interventions compared. | 1 (Lines 2–5) |
| Abstract | 2 | Provide a structured summary of objectives, perspective, setting, methods (including study design and inputs), results (including base case and uncertainty analyses), and conclusions. | 1 (Lines 11–24) |
| Introduction | |||
| Background and objectives | 3 | Provide an explicit statement of the broader context for the study. Present the study question and its relevance for health policy or practice decisions. | 1–2 (Lines 30–91) |
| Methods | |||
| Target population and subgroups | 4 | Describe characteristics of the base case population and subgroups analysed, including why they were chosen. | 3 (Lines 114–126) |
| Setting and location | 5 | State relevant aspects of the system(s) in which the decision(s) need(s) to be made | 3 (Lines 95–111) |
| Study perspective | 6 | Describe the perspective of the study and relate this to the costs being evaluated. | 4 (Line 172) |
| Comparators | 7 | Describe the interventions or strategies being compared and state why they were chosen. | 4 (Lines 147–149) |
| Time horizon | 8 | State the time horizon(s) over which costs and consequences are being evaluated and say why appropriate. | 4 (Lines 152–155) |
| Discount rate | 9 | Report the choice of discount rate(s) used for costs and outcomes and say why it is appropriate. | NA |
| Choice of health outcomes | 10 | Describe what outcomes were used as the measure(s) of benefit in the evaluation and their relevance for the type of analysis performed. | 4 (Lines 156–177) |
| Measurement of effectiveness | 11a | Single study-based estimates: Fully describe the design features of the single effectiveness study and why the single study was a sufficient source of clinical effectiveness data. | 4 (Lines 156–177) |
| 11b | Synthesis-based estimates: Fully describe the methods used for identification of included studies and synthesis of clinical effectiveness data. | NA | |
| Measurement and valuation of preference based outcomes | 12 | If applicable, describe the population and methods used to elicit preferences for outcomes. | NA |
| Estimating resources and costs | 13a | Single study-based economic evaluation: Describe approaches used to estimate resource use associated with the alternative interventions. Describe primary or secondary research methods for valuing each resource item in terms of its unit cost. Describe any adjustments made to approximate to opportunity costs. | 4–5 (Lines 178–202) |
| 13b | Model-based economic evaluation: Describe approaches and data sources used to estimate resource use associated with model health states. Describe primary or secondary research methods for valuing each resource item in terms of its unit cost. Describe any adjustments made to approximate to opportunity costs. | NA | |
| Currency, price date, and conversion | 14 | Report the dates of the estimated resource quantities and unit costs. Describe methods for adjusting estimated unit costs to the year of reported costs if necessary. Describe methods for converting costs into a common currency base and the exchange rate. | 5 (Lines 196–202) |
| Choice of model | 15 | Describe and give reasons for the specific type of decision analytical model used. Providing a figure to show model structure is strongly recommended. | NA |
| Assumptions | 16 | Describe all structural or other assumptions underpinning the decision-analytical model. | 5 (Table 1) |
| Analytical methods | 17 | Describe all analytical methods supporting the evaluation. This could include methods for dealing with skewed, missing, or censored data; extrapolation methods; methods for pooling data; approaches to validate or make adjustments (such as half cycle corrections) to a model; and methods for handling population heterogeneity and uncertainty. | 5–6 (Lines 204–232) |
| Results | |||
| Study parameters | 18 | Report the values, ranges, references, and, if used, probability distributions for all parameters. Report reasons or sources for distributions used to represent uncertainty where appropriate. Providing a table to show the input values is strongly recommended. | 6 (Table 2) |
| Incremental costs and Outcomes | 19 | For each intervention, report mean values for the main categories of estimated costs and outcomes of interest, as well as mean differences between the comparator groups. If applicable, report incremental cost-effectiveness ratios. | 7–8 (Lines 253–268) |
| Characterising uncertainty | 20a | Single study-based economic evaluation: Describe the effects of sampling uncertainty for the estimated incremental cost and incremental effectiveness parameters, together with the impact of methodological assumptions (such as discount rate, study perspective). | 8 (Lines 269–276) |
| 20b | Model-based economic evaluation: Describe the effects on the results of uncertainty for all input parameters, and uncertainty related to the structure of the model and assumptions. | NA | |
| Characterising heterogeneity | 21 | If applicable, report differences in costs, outcomes, or cost effectiveness that can be explained by variations between subgroups of patients with different baseline characteristics or other observed variability in effects that are not reducible by more information. | NA |
| Discussion | |||
| Study findings, limitations, generalisability, and current knowledge | 22 | Summarise key study findings and describe how they support the conclusions reached. Discuss limitations and the generalisability of the findings and how the findings fit with current knowledge. | 10–11 |
| Other | |||
| Source of funding | 23 | Describe how the study was funded and the role of the funder in the identification, design, conduct, and reporting of the analysis. Describe other non-monetary sources of support. | 11 |
| Conflicts of interest | 24 | Describe any potential for conflict of interest of study contributors in accordance with journal policy. In the absence of a journal policy, we recommend authors comply with International Committee of Medical Journal Editors recommendations. | 11 |
References
- World Health Organization. Obesity and Overweight: WHO. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 12 March 2021).
- Australian Institute of Health and Welfare. Overweight and Obesity among Australian Children and Adolescents; AIHW: Canberra, Australia, 2020.
- Sanders, R.H.; Han, A.; Baker, J.S.; Cobley, S. Childhood obesity and its physical and psychological co-morbidities: A systematic review of Australian children and adolescents. Eur. J. Pediatr. 2015, 174, 715–746. [Google Scholar] [CrossRef]
- Finkelstein, E.A.; Graham, W.C.K.; Malhotra, R. Lifetime Direct Medical Costs of Childhood Obesity. Pediatrics 2014, 133, 854–862. [Google Scholar] [CrossRef] [Green Version]
- National Audit Office. Childhood Obesity; Department of Health and Social Care, Ed.; National Audit Office: London, UK, 2020.
- Black, N.; Hughes, R.; Jones, A.M. The health care costs of childhood obesity in Australia: An instrumental variables approach. Econ. Hum. Biol. 2018, 31, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Chung, A.; Peeters, A.; Gearon, E.; Backholer, K. Contribution of discretionary food and drink consumption to socio-economic inequalities in children’s weight: Prospective study of Australian children. Int. J. Epidemiol. 2018, 47, 820–828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Department of Health and Human Services; U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans 2015. 8th. Available online: http://health.gov/dietaryguidelines/2015/guidelines/chapter-2/a-closer-look-at-current-intakes-and-recommended-shifts/ (accessed on 8 February 2020).
- Bates, B.; Cox, L.; Nicholson, S.; Page, P.; Prentice, A.; Steer, T.; Swan, G.; National Diet and Nutrition Survey. Results from Years 5–6 (Combined) of the Rolling Programme (2012/13–2013/14). 2016. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/551352/NDNS_Y5_6_UK_Main_Text.pdf (accessed on 8 December 2017).
- Centre for Epidemiology and Evidence. What NSW Children Eat and Drink; Ministry of Health: Sydney, Australia, 2017.
- Australian Institute of Health and Welfare. Nutrition across the Life Stages; AIHW: Canberra, Australia, 2018.
- Hardy, L.; Mihrshahi, S.; Drayton, B.; Bauman, A. NSW Schools Physical Activity and Nutrition Survey (SPANS) 2015: Full Report; Department of Health: Sydney, Australia, 2016.
- World Health Organisation. Health Promoting Schools: An Effective Approach to Early Action on Noncommunicable Disease Risk Factors 2017. Available online: http://apps.who.int/iris/bitstream/handle/10665/255625/WHO-NMH-PND-17.3-eng.pdf?sequence=1 (accessed on 12 March 2021).
- Bell, A.C.; Swinburn, B.A. What are the key food groups to target for preventing obesity and improving nutrition in schools? Eur. J. Clin. Nutr. 2004, 58, 258–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, C.E.L.; Greenwood, D.C.; Thomas, J.D.; Cleghorn, C.L.; Kitchen, M.S.; Cade, J.E. SMART lunch box intervention to improve the food and nutrient content of children’s packed lunches: UK wide cluster randomised controlled trial. J. Epidemiol. Community Health 2010, 64, 970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horne, P.J.; Hardman, C.A.; Lowe, C.F.; Tapper, K.; Le Noury, J.; Madden, P.; Patel, P.; Doody, M. Increasing parental provision and children’s consumption of lunchbox fruit and vegetables in Ireland: The Food Dudes intervention. Eur. J. Clin. Nutr. 2008, 63, 613. [Google Scholar] [CrossRef] [Green Version]
- Sanigorski, A.M.; Bell, A.C.; Kremer, P.; Swinburn, B.A. Lunchbox contents of Australian school children: Room for improvement. Eur. J. Clin. Nutr. 2005, 59, 1310–1316. [Google Scholar] [CrossRef] [Green Version]
- Sutherland, R.; Nathan, N.; Brown, A.; Yoong, S.; Finch, M.; Lecathelinais, C.; Reynolds, R.; Walton, A.; Janssen, L.; Desmet, C.; et al. A randomized controlled trial to assess the potential efficacy, feasibility and acceptability of an m-health intervention targeting parents of school aged children to improve the nutritional quality of foods packed in the lunchbox ‘SWAP IT’. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 54. [Google Scholar] [CrossRef]
- Nathan, N.; Janssen, L.; Sutherland, R.; Hodder, R.K.; Evans, C.E.L.; Booth, D.; Yoong, S.L.; Reilly, K.; Finch, M.; Wolfenden, L. The effectiveness of lunchbox interventions on improving the foods and beverages packed and consumed by children at centre-based care or school: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 38. [Google Scholar] [CrossRef] [Green Version]
- Drummond, M.F.; Sculpher, M.J.; Claxton, K.; Stoddart, G.L.; Torrance, G.W. Methods for the Economic Evaluation of Health Care Programmes; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Flego, A.; Keating, C.; Moodie, M. Cost–effectiveness of whole-of-community obesity prevention programs: An overview of the evidence. Expert Rev. Pharmacoecon. Outcomes Res. 2014, 14, 719–727. [Google Scholar] [CrossRef]
- Reeves, P.; Edmunds, K.; Searles, A.; Wiggers, J. Economic evaluations of public health implementation-interventions: A systematic review and guideline for practice. Public Health 2019, 169, 101–113. [Google Scholar] [CrossRef]
- Graziose, M.M.; Koch, P.A.; Wang, Y.C.; Lee Gray, H.; Contento, I.R. Cost-effectiveness of a Nutrition Education Curriculum Intervention in Elementary Schools. J. Nutr. Educ. Behav. 2017, 49, 684–691.e1. [Google Scholar] [CrossRef] [PubMed]
- Rush, E.; Obolonkin, V.; McLennan, S.; Graham, D.; Harris, J.D.; Mernagh, P.; Weston, A.R. Lifetime cost effectiveness of a through-school nutrition and physical programme: Project Energize. Obes. Res. Clin. Pract. 2014, 8, e115–e122. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Xu, H.; Liu, A.; Van Raaij, J.; Bemelmans, W.; Hu, X.; Zhang, Q.; Du, S.; Fang, H.; Ma, J.; et al. The Costs and Cost-Effectiveness of a School-Based Comprehensive Intervention Study on Childhood Obesity in China. PLoS ONE 2013, 8, e77971. [Google Scholar] [CrossRef] [Green Version]
- Nathan, N.K.; Sutherland, R.L.; Hope, K.; McCarthy, N.J.; Pettett, M.; Elton, B.; Jackson, R.; Trost, S.G.; Lecathelinais, C.; Reilly, K.; et al. Implementation of a School Physical Activity Policy Improves Student Physical Activity Levels: Outcomes of a Cluster-Randomized Controlled Trial. J. Phys. Act. Health 2020, 17, 1009. [Google Scholar] [CrossRef]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. BMJ 2016, 355, i5239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Husereau, D.; Drummond, M.; Petrou, S.; Carswell, C.; Moher, D.; Greenberg, D.; Augustovski, F.; Briggs, A.H.; Mauskopf, J.; Loder, E. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. Br. Med. J. 2013, 346, f1049. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- National Health and Medical Research Council. Australian Dietary Guidelines. Canberra: 2013 Contract No.: 1864965754. Available online: https://www.nhmrc.gov.au/adg (accessed on 8 March 2018).
- Kremer, P.J.; Bell, A.C.; Swinburn, B.A. Calibration and reliability of a school food checklist: A new tool for assessing school food and beverage consumption. Asia Pac. J. Clin. Nutr. 2006, 15, 465–473. [Google Scholar]
- Mitchell, S.A.; Miles, C.L.; Brennan, L.; Matthews, J. Reliability of the School Food Checklist for in-school audits and photograph analysis of children’s packed lunches. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2010, 23, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. BMJ 2009, 338, b2393. [Google Scholar] [CrossRef] [PubMed]
- Vieira, M.; Carvalho, G.S. Costs and benefits of a school-based health intervention in Portugal. Health Promot. Int. 2019, 34, 1141–1148. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.Y.; Gutin, B.; Barbeau, P.; Moore, J.B.; Hanes, J.; Johnson, M.H.; Cavnar, M.; Thornburg, J.; Yin, Z. Cost-Effectiveness of a School-Based Obesity Prevention Program. J. Sch. Health 2008, 78, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Li, Y.; Du, S.; Zhang, Q.; Liu, A.; Sun, J.; Ma, G. Cost–utility and cost–benefit analyses of school-based obesity prevention program. BMC Public Health 2020, 20, 1608. [Google Scholar] [CrossRef]
- Reilly, K.L.; Reeves, P.; Deeming, S.; Yoong, S.L.; Wolfenden, L.; Nathan, N.; Wiggers, J. Economic analysis of three interventions of different intensity in improving school implementation of a government healthy canteen policy in Australia: Costs, incremental and relative cost effectiveness. BMC Public Health 2018, 18, 378. [Google Scholar] [CrossRef] [Green Version]
- Fayet-Moore, F.; McConnell, A.; Cassettari, T.; Tuck, K.; Petocz, P.; Kim, J. Vegetable intake in Australian children and adolescents: The importance of consumption frequency, eating occasion and its association with dietary and sociodemographic factors. Public Health Nutr. 2020, 23, 474–487. [Google Scholar] [CrossRef]
- Cochrane, T.; Davey, R.; de Castella, F.R. Estimates of the energy deficit required to reverse the trend in childhood obesity in Australian schoolchildren. Aust. N. Z. J. Public Health 2016, 40, 62–67. [Google Scholar] [CrossRef] [Green Version]
- Gortmaker, S.L.; Long, M.W.; Resch, S.C.; Ward, Z.J.; Cradock, A.L.; Barrett, J.L.; Wright, D.R.; Sonneville, K.R.; Giles, C.M.; Carter, R.C.; et al. Cost Effectiveness of Childhood Obesity Interventions: Evidence and Methods for CHOICES. Am. J. Prev. Med. 2015, 49, 102–111. [Google Scholar] [CrossRef]
- Oosterhoff, M.; Bosma, H.; Van Schayck, O.C.; Joore, M. A Cost Analysis of School-Based Lifestyle Interventions. Prev. Sci. 2018, 19, 716–727. [Google Scholar] [CrossRef] [Green Version]
- Sutherland, R.; Brown, A.; Nathan, N.; Yoong, S.; Janssen, L.; Chooi, A.; Hudson, N.; Wiggers, J.; Kerr, N.; Evans, N.; et al. A Multicomponent mHealth-Based Intervention (SWAP IT) to Decrease the Consumption of Discretionary Foods Packed in School Lunchboxes: Type I Effectiveness—Implementation Hybrid Cluster Randomized Controlled Trial. J. Med. Internet Res. 2021, 23, e25256. [Google Scholar] [CrossRef] [PubMed]

| Intervention Strategy | Details and Assumptions | Sources of Unit Costs |
|---|---|---|
| Weekly support messages to parents | ||
| Meetings with mobile communication app partner | Health promotion officers employed to support schools | Wage rates (Health Managers (State) Award 2019 Industrial Relations Commission Of New South Wales): HSM Project officer level B midpoint of AUD 43.11 per hour including on-costs |
| Graphic design revisions | Exact cost from invoice records | Market rates |
| Physical resources for parents | ||
| Water bottles, ice bricks, lunchbox ideas booklet | Production, printing and postage (to the health service) from invoice records | Market rates |
| Graphic design revisions | Exact cost from invoice records | Market rates |
| Lunchbox flipchart lessons | ||
| Flipchart | Production, printing and postage (to the health service) from invoice records | Market rates |
| Graphic design revisions | Exact cost from invoice records | Market rates |
| Health promotion officer implementation costs | ||
| Liaising with schools (face to face or phone calls or email); Development of nutrition guidelines in collaboration with schools; Management of the weekly support messages to parents | Health promotion officer implementation costs were collected retrospectively via project officer logs and were collected as the overall time spent on the implementation of the intervention, per school. | Wage rates (Health Managers (State) Award 2019 Industrial Relations Commission Of New South Wales): HSM Project officer level B midpoint of AUD 43.11 per hour including on-costs |
| Intervention n | Control n | |
|---|---|---|
| Number of schools | 6 | 6 |
| Locations | ||
| - Urban | 4 | 5 |
| - Rural | 2 | 1 |
| School socioeconomic status | ||
| - Most disadvantaged | 4 | 4 |
| - Least disadvantaged | 2 | 2 |
| Total students | 778 | 991 |
| Sex | ||
| - Female | 379 | 480 |
| - Male | 394 | 501 |
| Sex missing = 15 | ||
| Mean age (years) | 7.99 | 7.94 |
| Strategy | Description | Cost (AUD AUD2019) |
|---|---|---|
| Weekly support messages to parents | The intervention utilised an existing school mobile communication app (Skoolbag) to communicate lunchbox messages to parents/carers that addressed the barriers to packing a healthy lunchbox. Costs were associated with graphic design revisions and health promotion officer time spent liaising with mobile communication app partner. | 774 |
| Physical resources for parents | Each student received an information package containing tools and resources, including a lunchbox ideas booklet, which provided easy, seasonal and low-cost lunchbox ideas, ice-brick and a ‘water only’ drink bottle. Costs associated with the physical resources were in relation to printing and production, postage and graphic design revisions. | 51,789 |
| Lunchbox flipchart lessons | Schools and teachers were provided with a ten- page flipchart for each classroom at the launch of the intervention. The flipchart featured a different lunchbox sample for each week of the intervention and provided ideas for teachers to facilitate discussion on healthy lunchboxes in the classroom. Costs associated with flipcharts were in relation to printing, postage and graphic design revisions. | 2818 |
| Health promotion officer implementation costs | This included health promotion officer time to liaise with schools, develop lunchbox nutrition guidelines and to manage the ‘push’ for weekly support messages to parents | 86 |
| Total costs | 55,467 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brown, A.; Sutherland, R.; Reeves, P.; Nathan, N.; Wolfenden, L. Cost and Cost Effectiveness of a Pilot m-Health Intervention Targeting Parents of School-Aged Children to Improve the Nutritional Quality of Foods Packed in the Lunchbox. Nutrients 2021, 13, 4136. https://doi.org/10.3390/nu13114136
Brown A, Sutherland R, Reeves P, Nathan N, Wolfenden L. Cost and Cost Effectiveness of a Pilot m-Health Intervention Targeting Parents of School-Aged Children to Improve the Nutritional Quality of Foods Packed in the Lunchbox. Nutrients. 2021; 13(11):4136. https://doi.org/10.3390/nu13114136
Chicago/Turabian StyleBrown, Alison, Rachel Sutherland, Penny Reeves, Nicole Nathan, and Luke Wolfenden. 2021. "Cost and Cost Effectiveness of a Pilot m-Health Intervention Targeting Parents of School-Aged Children to Improve the Nutritional Quality of Foods Packed in the Lunchbox" Nutrients 13, no. 11: 4136. https://doi.org/10.3390/nu13114136
APA StyleBrown, A., Sutherland, R., Reeves, P., Nathan, N., & Wolfenden, L. (2021). Cost and Cost Effectiveness of a Pilot m-Health Intervention Targeting Parents of School-Aged Children to Improve the Nutritional Quality of Foods Packed in the Lunchbox. Nutrients, 13(11), 4136. https://doi.org/10.3390/nu13114136