
Type of Milk Feeding and Introduction to Complementary Foods in Relation to Infant Sleep: A Systematic Review


Abstract
1. Introduction
2. Materials and Methods
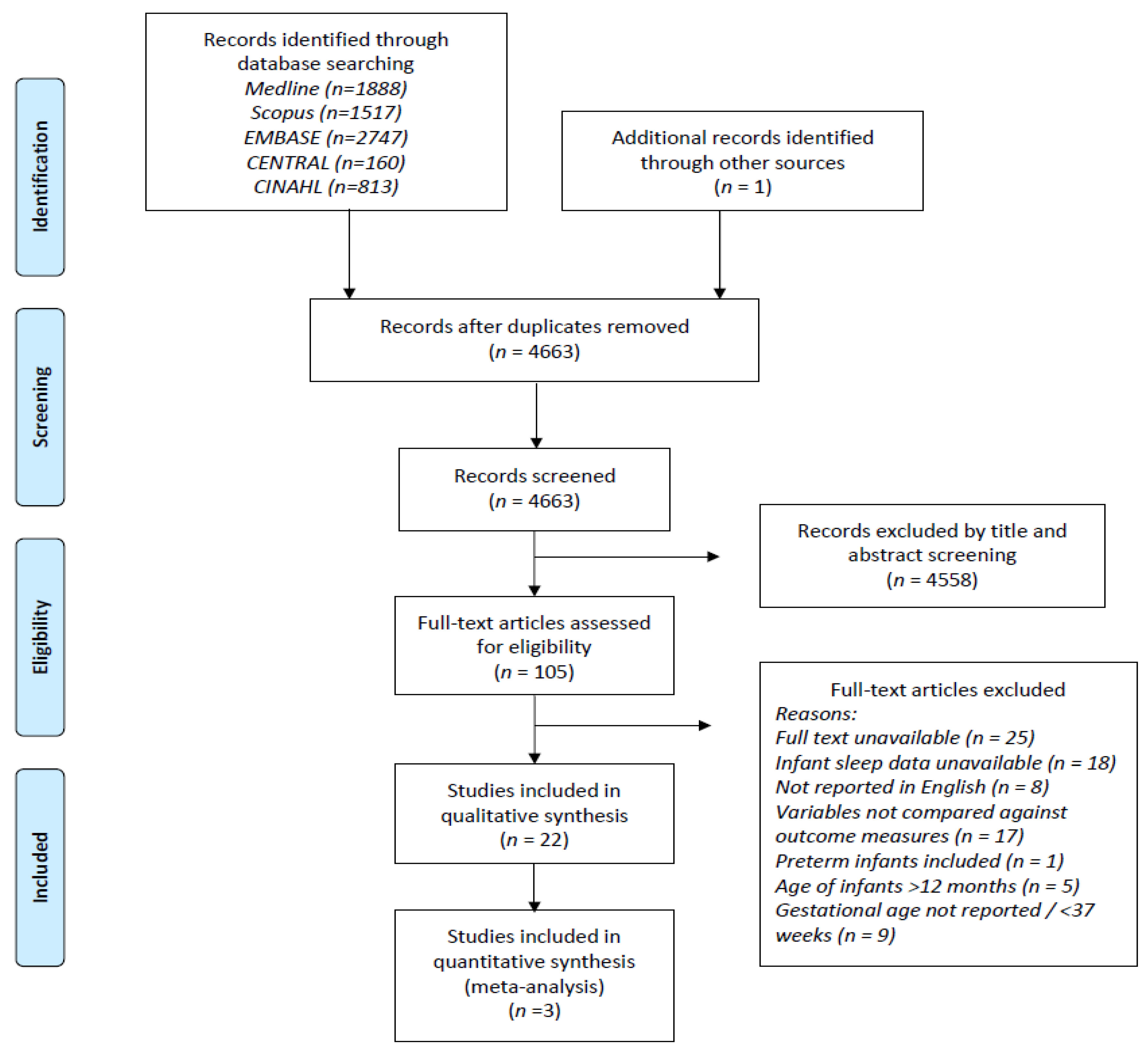
2.1. Search Strategy
2.2. Selection of Studies
2.3. Data Extraction and Quality Assessment
3. Results
3.1. Type of Milk Feeding and Infant Sleep
3.1.1. 24 h Sleep Duration
3.1.2. Total Night-Time Sleep
3.1.3. Night-Waking Frequency
3.1.4. Duration of Night Wakings
3.1.5. Longest Sleep Period
3.1.6. Sleep Onset Latency
3.2. Introduction to Complementary Foods and Infant Sleep
3.2.1. 24 h Sleep Duration
3.2.2. Night-Waking Frequency
3.3. Quality Assessment
4. Discussion
Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Hillard, P.J.A.; Katz, E.S.; et al. National Sleep Foundation’s updated sleep duration recommendations: Final report. Sleep Health 2015, 1, 233–243. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Infant and Young Child Feeding: Model Chapter for Textbooks for Medical Students and Allied Health Professionals; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- León-Cava, N.; Lutter, C.; Ross, J.; Martin, L. Quantifying the Benefits of Breastfeeding: A Summary of the Evidence; Pan American Health Organization: Washington, DC, USA, 2002. [Google Scholar]
- Horta, B.L.; Bahl, R.; Martinés, J.C.; Victora, C.G.; World Health Organization. Evidence on the Long-Term Effects of Breastfeeding: Systematic Review and Meta-Analyses; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Henderson, J.M.T.; France, K.G.; Owens, J.L.; Blampied, N.M. Sleeping through the Night: The Consolidation of Self-regulated Sleep across the First Year of Life. Pediatrics 2010, 126, e1081–e1087. [Google Scholar] [CrossRef] [PubMed]
- Davis, K.F.; Parker, K.P.; Montgomery, G.L. Sleep in infants and young children: Part one: Normal sleep. J. Pediatr. Health Care 2004, 18, 65–71. [Google Scholar] [CrossRef]
- Dias, C.C.; Figueiredo, B.; Rocha, M.; Field, T. Reference values and changes in infant sleep-wake behaviour during the first 12 months of life: A systematic review. J. Sleep Res. 2018, 27, e12654. [Google Scholar] [CrossRef] [PubMed]
- Tham, E.K.; Schneider, N.; Broekman, B.F. Infant sleep and its relation with cognition and growth: A narrative review. Nat. Sci. Sleep 2017, ume 9, 135–149. [Google Scholar] [CrossRef]
- Seehagen, S.; Konrad, C.; Herbert, J.; Schneider, S. Timely sleep facilitates declarative memory consolidation in infants. Proc. Natl. Acad. Sci. USA 2015, 112, 1625–1629. [Google Scholar] [CrossRef]
- Friedrich, M.; Wilhelm, I.; Born, J.; Friederici, A.D. Generalization of word meanings during infant sleep. Nat. Commun. 2015, 6, 6004. [Google Scholar] [CrossRef] [PubMed]
- Taveras, E.M.; Rifas-Shiman, S.L.; Oken, E.; Gunderson, E.P.; Gillman, M.W. Short Sleep Duration in Infancy and Risk of Childhood Overweight. Arch. Pediatr. Adolesc. Med. 2008, 162, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Zuckerman, B.; Stevenson, J.; Bailey, V. Sleep Problems in Early-Childhood-Continuities, Predictive Factors, and Behavioral Correlates. Pediatrics 1987, 80, 664–671. [Google Scholar]
- Martin, J.; Hiscock, H.; Hardy, P.; Davey, B.; Wake, M. Adverse Associations of Infant and Child Sleep Problems and Parent Health: An Australian Population Study. Pediatrics 2007, 119, 947–955. [Google Scholar] [CrossRef]
- Bernier, A.; Carlson, S.M.; Bordeleau, S.; Carrier, J. Relations Between Physiological and Cognitive Regulatory Systems: Infant Sleep Regulation and Subsequent Executive Functioning. Child Dev. 2010, 81, 1739–1752. [Google Scholar] [CrossRef] [PubMed]
- Karraker, K.H.; Young, M. Night waking in 6-month-old infants and maternal depressive symptoms. J. Appl. Dev. Psychol. 2007, 28, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Hiscock, H.; Wake, M. Infant sleep problems and postnatal depression: A community-based study. Pediatrics 2001, 107, 1317–1322. [Google Scholar] [CrossRef] [PubMed]
- Teng, A.; Bartle, A.; Sadeh, A.; Mindell, J. Infant and toddler sleep in Australia and New Zealand. J. Paediatr. Child Health 2011, 48, 268–273. [Google Scholar] [CrossRef]
- Galbally, M.; Lewis, A.J.; McEgan, K.; Scalzo, K.; Islam, F.A. Breastfeeding and infant sleep patterns: An Australian population study. J. Paediatr. Child Health 2013, 49, E147–E152. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.; Harries, V. Infant Sleep and Night Feeding Patterns During Later Infancy: Association with Breastfeeding Frequency, Daytime Complementary Food Intake, and Infant Weight. Breastfeed. Med. 2015, 10, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Perkin, M.R.; Bahnson, H.T.; Logan, K.; Marrs, T.; Radulovic, S.; Craven, J.; Flohr, C.; Lack, G. Association of Early Introduction of Solids with Infant Sleep. JAMA Pediatr. 2018, 172, e180739. [Google Scholar] [CrossRef] [PubMed]
- Dias, C.C.; Figueiredo, B. Sleep-wake behaviour during the first 12 months of life and associated factors: A systematic review. Early Child Dev. Care 2020, 190, 2333–2365. [Google Scholar] [CrossRef]
- Demirci, J.R.; Braxter, B.J.; Chasens, E.R. Breastfeeding and short sleep duration in mothers and 6–11-month-old infants. Infant Behav. Dev. 2012, 35, 884–886. [Google Scholar] [CrossRef] [PubMed]
- Nevarez, M.D.; Rifas-Shiman, S.L.; Kleinman, K.; Gillman, M.W.; Taveras, E.M. Associations of Early Life Risk Factors with Infant Sleep Duration. Acad. Pediatr. 2010, 10, 187–193. [Google Scholar] [CrossRef]
- Alder, E.M.; Williams, F.L.R.; Anderson, A.S.; Forsyth, S.; Florey, C.D.V.; Van Der Velde, P. What influences the timing of the introduction of solid food to infants? Br. J. Nutr. 2004, 92, 527–531. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Clarivate. The EndNote Team EndNote, EndNote X9; Clarivate: Philadelphia, PA, USA, 2013. [Google Scholar]
- World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices Part 3: Country Profiles; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef]
- Butte, N.F.; Jensen, C.L.; Moon, J.K.; Glaze, D.G.; Frost, J.D. Sleep Organization and Energy Expenditure of Breast-Fed and Formula-Fed Infants. Pediatr. Res. 1992, 32, 514–519. [Google Scholar] [CrossRef] [PubMed]
- DeLeon, C.W.; Karraker, K.H. Intrinsic and extrinsic factors associated with night waking in 9-month-old infants. Infant Behav. Dev. 2007, 30, 596–605. [Google Scholar] [CrossRef]
- Kaley, F.; Reid, V.; Flynn, E. Investigating the biographic, social and temperamental correlates of young infants’ sleeping, crying and feeding routines. Infant Behav. Dev. 2012, 35, 596–605. [Google Scholar] [CrossRef] [PubMed]
- Lee, K. Crying and behavior pattern in breast- and formula-fed infants. Early Hum. Dev. 2000, 58, 133–140. [Google Scholar] [CrossRef]
- Quillin, S.I.M. Infant and mother sleep patterns during 4th postpartum week. Issues Compr. Pediatr. Nurs. 1997, 20, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Quillin, I.; Glenn, L.L. Interaction Between Feeding Method and Co-Sleeping on Maternal-Newborn Sleep. J. Obstet. Gynecol. Neonatal Nurs. 2004, 33, 580–588. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Li, S.X.; Jiang, Y.; Xu, X.; Spruyt, K.; Zhu, Q.; Tseng, C.-H.; Jiang, F. A Community-Based Study of Sleep and Cognitive Development in Infants and Toddlers. J. Clin. Sleep Med. 2018, 14, 977–984. [Google Scholar] [CrossRef] [PubMed]
- Wailoo, M.P.; Petersen, S.A.; Whitaker, H. Disturbed nights and 3-4 month old infants: The effects of feeding and thermal environment. Arch. Dis. Child. 1990, 65, 499–501. [Google Scholar] [CrossRef]
- Berger, P.K.; Lavner, J.A.; Smith, J.J.; Birch, L.L. Differences in early risk factors for obesity between African American formula-fed infants and White breastfed controls. Pilot Feasibility Stud. 2017, 3, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, B.; Dias, C.C.; Pinto, T.M.; Field, T. Exclusive breastfeeding at three months and infant sleep-wake behaviors at two weeks, three and six months. Infant Behav. Dev. 2017, 49, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.-N.; Wang, H.-S.; Chang, J.-J.; Wang, L.-H.; Liu, X.-C.; Jiang, J.-X.; An, L. Feeding methods, sleep arrangement, and infant sleep patterns: A Chinese population-based study. World J. Pediatr. 2016, 12, 66–75. [Google Scholar] [CrossRef]
- Tikotzky, L.; Sadeh, A.; Volkovich, E.; Manber, R.; Meiri, G.; Shahar, G. VII. infant sleep development from 3 to 6 months postpartum: Links with maternal sleep and paternal involvement. Monogr. Soc. Res. Child Dev. 2015, 80, 107–124. [Google Scholar] [CrossRef] [PubMed]
- Pennestri, M.-H.; Laganière, C.; Bouvette-Turcot, A.-A.; Pokhvisneva, I.; Steiner, M.; Meaney, M.J.; Gaudreau, H.; on behalf of the Mavan Research Team. Uninterrupted Infant Sleep, Development, and Maternal Mood. Pediatrics 2018, 142, e20174330. [Google Scholar] [CrossRef] [PubMed]
- Heinig, M.J.; Nommsen, L.A.; Peerson, J.M.; Lonnerdal, B.; Dewey, K.G. Intake and growth of breast-fed and formula-fed infants in relation to the timing of introduction of complementary foods: The DARLING study. Acta Paediatr. 1993, 82, 999–1006. [Google Scholar] [CrossRef]
- Rudzik, A.E.; Robinson-Smith, L.; Ball, H.L. Discrepancies in maternal reports of infant sleep vs. actigraphy by mode of feeding. Sleep Med. 2018, 49, 90–98. [Google Scholar] [CrossRef]
- Tikotzky, L.; Sadeh, A.; Glickman-Gavrieli, T. Infant Sleep and Paternal Involvement in Infant Caregiving During the First 6 Months of Life. J. Pediatr. Psychol. 2010, 36, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, M.; Shinohara, H.; Kodama, H. Assessment of nocturnal sleep architecture by actigraphy and one-channel electroencephalography in early infancy. Early Hum. Dev. 2015, 91, 519–526. [Google Scholar] [CrossRef]
- Morgan, J.B.; Lucas, A.; Fewtrell, M.S. Does weaning influence growth and health up to 18 months? Arch. Dis. Child. 2004, 89, 728–733. [Google Scholar] [CrossRef]
- Sadeh, A. A Brief Screening Questionnaire for Infant Sleep Problems: Validation and Findings for an Internet Sample. Pediatrics 2004, 113, e570–e577. [Google Scholar] [CrossRef] [PubMed]
- Touchette, É.; Petit, D.; Paquet, J.; Boivin, M.; Japel, C.; Tremblay, R.E.; Montplaisir, J.Y. Factors Associated with Fragmented Sleep at Night Across Early Childhood. Arch. Pediatr. Adolesc. Med. 2005, 159, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Lanting, C.; Huisman, M.; Boersma, E.; Touwen, B.; Fidler, V. Neurological differences between 9-year-old children fed breast-milk or formula-milk as babies. Lancet 1994, 344, 1319–1322. [Google Scholar] [CrossRef]
- Wolke, D.; Bilgin, A.; Samara, M. Systematic Review and Meta-Analysis: Fussing and Crying Durations and Prevalence of Colic in Infants. J. Pediatr. 2017, 185, 55–61.e4. [Google Scholar] [CrossRef] [PubMed]
- Kim, P.; Feldman, R.; Mayes, L.C.; Eicher, V.; Thompson, N.; Leckman, J.F.; Swain, J.E. Breastfeeding, brain activation to own infant cry, and maternal sensitivity. J. Child Psychol. Psychiatry 2011, 52, 907–915. [Google Scholar] [CrossRef]
- Gozal, D.; Dayyat, E.A.; Spruyt, K.; Molfese, D.L. Sleep estimates in children: Parental versus actigraphic assessments. Nat. Sci. Sleep 2011, 3, 115–123. [Google Scholar] [CrossRef]
- Galland, B.C.; Taylor, B.; Elder, D.E.; Herbison, P. Normal sleep patterns in infants and children: A systematic review of observational studies. Sleep Med. Rev. 2012, 16, 213–222. [Google Scholar] [CrossRef]
- Hall, W.A.; Eliva, S.; Emoynihan, M.; Esaunders, R. A Comparison of Actigraphy and Sleep Diaries for Infants’ Sleep Behavior. Front. Psychiatry 2015, 6, 19. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, M.; Iwata, S.; Iemura, A.; Yamashita, N.; Tomino, Y.; Anme, T.; Yamagata, Z.; Iwata, O.; Matsuishi, T. Utility of Subjective Sleep Assessment Tools for Healthy Preschool Children: A Comparative Study Between Sleep Logs, Questionnaires, and Actigraphy. J. Epidemiol. 2010, 20, 143–149. [Google Scholar] [CrossRef]
- Bauer, K.; Blunden, S. How Accurate is Subjective Reporting of Childhood Sleep Patterns? A Review of the Literature and Implications for Practice. Curr. Pediatr. Rev. 2008, 4, 132–142. [Google Scholar] [CrossRef]
- Sadeh, A. Evaluating Night Wakings in Sleep-Disturbed Infants: A Methodological Study of Parental Reports and Actigraphy. Sleep 1996, 19, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.; Wickwire, E.M.; Hirshkowitz, M.; Albert, S.; Avidan, A.; Daly, F.J.; Dauvilliers, Y.; Ferri, R.; Fung, C.; Gozal, D.; et al. National Sleep Foundation’s sleep quality recommendations: First report. Sleep Health 2017, 3, 6–19. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef]


{kind=link}
| Author, Year, Country | Sample Size | Design | Sleep Variables | Type of Milk Feeding 1 | Age of Introduction to Complementary Foods 1 | Infant Sleep Assessment 1 | Quality Rating 2 |
|---|---|---|---|---|---|---|---|
| Berger et al., 2017 (United States) [37] | 57 | Prospective cohort | 24 h sleep duration Night-time sleep Night-waking frequency | BF FF | X | BISQ | 6 |
| Brown et al., 2015 (United Kingdom) [19] | 756 | Cross-sectional | Night-waking frequency | BF +/− food FF +/− food | 8 to 32 weeks (mean 21.2 weeks) | Questionnaire | 5 |
| Butte et al., 1992 (United States) [29] | 20 | Cross-sectional | Sleep diary: 24 h sleep duration Night-time sleep EEG: Night-waking frequency Sleep onset latency | BF FF | X | 5 days sleep diary 1 night 3 EEG | 5 |
| DeLeon et al., 2007 (United States) [30] | 41 | Cross-sectional | Duration of night wakings Night-waking frequency Night-time sleep | BF +/− food FF +/− food | X | Questionnaire and sleep diary | 4 |
| Figueiredo et al., 2017 (Portugal) [38] | 148, 2 weeks 162, 3 months 123, 6 months | Prospective cohort | Night-time sleep Night-waking frequency Duration of night wakings Sleep onset latency Longest sleep period 24 h sleep duration | EBF BF FF | X | 24 h infant sleep chronogram | 5 |
| Heinig et al., 1993 (United States) [42] | 105 | Longitudinal study | 24 h sleep duration | BF +/− food FF +/− food | <26 weeks ≥26 weeks | Sleep record | 4 |
| Huang et al., 2016 (China) [39] | 524 | Prospective cohort | 24 h sleep % Night-waking frequency night-time sleep % Longest sleep period | BF +/− food FF +/− food | X | 3 and 7 days Sleep diary 4 | 4 |
| Kaley et al., 2012 (United Kingdom) [31] | 74 | Cross-sectional | Night-waking frequency Night-time sleep 24 h sleep duration | BF FF | X | 3–7 days sleep diary | 4 |
| Lee et al., 2000 (South Korea) [32] | 188 | Cross-sectional | 24 h sleep duration Longest sleep period 5 | EBF FF | X | Sleep diary | 4 |
| Mindell et al., 2012 (United States) [17] | 92 | Prospective Longitudinal | Night-waking frequency Longest sleep period Night-time sleep Sleep onset latency | BF +/− food FF +/− food | X | Expanded BISQ | 6 |
| Morgan et al., 2004 (United Kingdom) [46] | 1187, type of milk feeding 6 1196, introduction to complementary foods 6 | Combined RCT | 24 h sleep duration | BF FF | ≤12 weeks >12 weeks | Questionnaire | 5 |
| Nevarez et al., 2010 (United States) [23] | 1676, 6 months 1228, 12 months | Prospective cohort | 24 h sleep duration | BF +/− food FF +/− food | <4 months > 4 months | 1 night EEG Sleep questionnaire | 5 |
| Pennestri et al., 2018 (Canada) [41] | 388, 6 months 369, 12 months | Cohort study | Sleep through the night—6 h criterion Sleep through the night—8 h criterion | BF +/− food FF +/− food | X | Questionnaire | 4 |
| Quillin et al., 1997 (United States) [33] | 45 | Cross-sectional | Night-time sleep Night-waking frequency | BF FF | X | 6 days sleep activity record | 3 |
| Quillin et al., 2004 (United States) [34] | 33 | Cross-sectional | 24 h sleep duration Night-time sleep Night-waking frequency 7 | BF FF | X | 5 days sleep diary | 4 |
| Rudzik et al., 2018 (United Kingdom) [43] | 61 | Longitudinal | Night-time sleep Longest sleep period Night-waking frequency | EBF FF | X | 1 night actigraph 8 and sleep diary | 3 |
| Sun et al., 2018 (China) [35] | 590 | Cross-sectional | Night-waking frequency | BF +/− food FF +/− food | X | Chinese BISQ | 6 |
| Tikotzky et al., 2011 (Israel) [44] | 56 | Longitudinal observational | Night-waking frequency 24 h sleep duration | EBF BF FF | X | 4 days actigraph and sleep diary | 6 |
| Tikotzky et al., 2015 (Israel) [40] | 53 | Cohort | Night-waking frequency 9 Night-time sleep 9 | EBF BF FF | X | 5 days actigraph and sleep diary, BISQ | 5 |
| Wailoo et al., 1990 (United Kingdom) [36] | 87 | Cross-sectional | Night-waking frequency Longest sleep period | BF FF | X | 1 night sleep diary | 2 |
| Yoshida et al., 2015 (Japan) [45] | 27 | Longitudinal | Sleep through the night—6 h criterion Duration of night wakings | EBF FF | X | 2 days actigraph 2 days sleep timetable | 5 |
| 24 h Sleep Duration | |||||||
|---|---|---|---|---|---|---|---|
| Author, Year | Infant Age at Assessment/Assessment Frequency | ≤6 Months | >6 Months | 0–12 Months | Statistics 1 | Quality Rating 2 | |
| EBF vs FF 1 | BF vs. FF 1 | BF vs. FF 1 | BF vs. FF 1 | ||||
| Berger et al., 2017 [37] | 16 weeks | BF vs. FF mean ± SE (h) 12.95 ± 0.51 vs. 11.43 ± 0.53, p = 0.047 | t-test | 6 | |||
| Butte et al., 1992 [29] | 17 weeks | BF vs. FF mean ± SD (h) 13.2 ± 2.3 vs.13.3 ± 0.9, p > 0.05 | t-test Regression | 5 | |||
| Figueiredo et al., 2017 [38] | 2, 13, 26 weeks | EBF vs. FF mean ± SD (h) 2 weeks 13.43 ± 2.34 vs. 12.29 ± 2.27, p > 0.05 13 weeks 13.05 ± 1.87 vs. 12.87 ± 2.44, p > 0.05 26 weeks 12.37 ± 1.76 vs. 12.79 ± 1.05, p > 0.05 | BF vs. FF mean ± SD (h) 2 weeks 12.18 ± 3.02 vs. 12.29 ± 2.27, p > 0.05 13 weeks 12.41 ± 2.21 vs. 12.87 ± 2.44, p > 0.05 26 weeks 12.73 ± 1.48 vs. 12.79 ± 1.05, p > 0.05 | Multivariate Analyses of Chi MANCOVA 3 | 5 | ||
| Kaley et al., 2012 [31] | 4–10 weeks | BF vs. FF Total sleep not assoc. with feeding, p > 0.05 | Correlation ANOVA | 4 | |||
| Lee et al., 2000 [32] | 2–17 weeks | EBF vs. FF mean ± SD (min) 902.4 ± 119.1 vs. 854.8 ± 130.7, p < 0.01 | Unpaired t-test | 4 | |||
| Quillin et al., 2004 [34] | 4 weeks | BF vs. FF mean ± SD (h) 13.1 ± 1.4 vs. 14.4 ± 1.1, p = 0.006 | t-test | 4 | |||
| Tikotzky et al., 2011 [44] | 26 weeks | EBF vs. FF No assoc. between total sleep and EBF (r = 0.15, p > 0.05) | Spearman rho correlations | 6 | |||
| Nevarez et al., 2010 [23] | 26, 52 weeks 4 | BF +/− food vs. FF +/− food Bivariate 26 weeks β = 0.05 (95%CI: −0.14 to 0.24), p > 0.05 Multivariate 26 weeks β = −0.15 (95%CI: −0.37 to 0.07), p > 0.05 | BF +/− food vs. FF +/− food Bivariate 52 weeks β = 0.02 (95%CI: −0.17 to 0.20), p > 0.05 Multivariate 52 weeks is β = −0.17 (95%CI: −0.37 to 0.03), p > 0.05 | Bivariate Multivariate linear regression 5 | 5 | ||
| Heinig et al., 1993 [42] | 39 weeks | BF +/− food vs. FF +/− food 24 h sleep at 39 weeks greater in FF compared to BF grps, p < 0.05 | t-test | 4 | |||
| Morgan et al., 2004 [46] | 39 weeks 4 | BF +/− food vs. FF +/− food mean ± SE (h) 11.2 ± 0.1 vs. 11.4 ± 0.6, p = 0.01 6 | ANCOVA 7 | 5 | |||
| Huang et al., 2016 [39] | 0–34 weeks | BF +/− food vs. FF +/− food BF 2.1% lower (30 min less) 24 h sleep % than FF, p = 0.0009 | Multilevel mixed models | 4 | |||
| Total Night-Time Sleep | |||||||
| Author, Year | Infant Age at Assessment/Assessment Frequency | ≤6 Months | >6 Months | 0–12 Months | Statistics 1 | Quality Rating 2 | |
| EBF vs. FF 1 | BF vs. FF 1 | BF vs. FF 1 | BF vs. FF 1 | ||||
| Berger et al., 2017 [37] | 16 weeks | BF vs. FF mean ± SE (h) 9.50 ± 0.38 vs. 7.33 ± 0.39, p < 0.0001 | t-test | 6 | |||
| Butte et al., 1992 [29] | 17 weeks | BF vs. FF mean ± SD (h) 8.2 ± 1.6 vs. 9.9 ± 1.4, p < 0.04 | t-test Regression | 5 | |||
| Figueiredo et al., 2017 [38] | 2, 13, 26 weeks | EBF vs. FF mean ± SD (h) 2 weeks 7.08 ± 1.33 vs. 6.34 ± 1.21, p > 0.05 13 weeks 8.06 ± 1.30 vs. 8.27 ± 1.35, p > 0.05 26 weeks 8.29 ± 1.36 vs. 8.29 ± 1.07, p > 0.05 | BF vs. FF mean ± SD (h) 2 weeks 6.77 ± 1.55 vs. 6.34 ± 1.21, p > 0.05 13 weeks 8.12 ± 1.22 vs. 8.27 ± 1.35, p > 0.05 26 weeks 8.93 ± 1.21 vs. 8.29 ± 1.07, p > 0.05 | Multivariate Analyses of Chi MANCOVA 3 | 5 | ||
| Kaley et al., 2012 [31] | 4–10 weeks | BF vs. FF NTS duration not assoc. with feeding, p > 0.05 | Correlation ANOVA | 4 | |||
| Quillin et al., 1997 [33] | 4 weeks | BF vs. FF BF infants slept less at night than FF infants. F(1,39) = 4.925, p < 0.05 | ANOVA-two-way analysis of variance | 3 | |||
| Quillin et al., 2004 [34] | 4 weeks | BF vs. FF mean ± SD (h) 6.4 ±1.0 vs. 6.4 ± 0.8, p > 0.05 | t-test | 4 | |||
| Rudzik et al., 2018 [43] | 4,6,8,10,12,14,16, 18 weeks | EBF vs. FF Actigraph report No difference between grps for NTS at 2, 6, 8, 10, 12, 14, 16, 18 weeks, p > 0.05 | t-test | 3 | |||
| Yoshida et al., 2015 [45] | 13, 17 weeks | EBF vs. FF STN (6 h criterion): 33% vs. 67% | Multiple linear regression | 5 | |||
| Pennestri et al., 2018 [41] | 26, 52 weeks | BF +/− food vs. FF +/− food BF infants less likely to STN at 26 weeks (χ2 = 26.67, p < 0.0001) using 6 h criterion BF infants less likely to STN at 6 months (χ2 = 31.19, p < 0.0001) using 8 h criterion | BF +/− food vs. FF +/− food BF infants less likely to STN at 52 weeks (χ2 = 34.96, p < 0.0001) using 6 h criterion BF infants less likely to STN at 12 months (χ2 = 25.24, p < 0.0001) using 8 h criterion | Chi-squared | 4 | ||
| DeLeon et al., 2007 [30] | 39 weeks | BF +/− food vs. FF +/− food BF −ve correlated with total NTS (r = −0.42, p < 0.01) | Pearson’s correlation coefficient | 4 | |||
| Huang et al., 2016 [39] | 0–34 weeks | BF +/− food vs. FF +/− food No assoc. between NTS %, p > 0.05 | Multilevel mixed models | 4 | |||
| Mindell et al., 2012 [17] | 13–52 weeks 4 | BF +/− food vs. FF +/− food mean ± SD (h) 10.70 ± 1.03 vs. 10.30 ± 1.31, p = 0.146 | MANCOVA | 6 | |||
| Night-Waking Frequency | |||||||
| Author, Year | Infant Age at Assessment/Assessment Frequency | ≤6 Months | >6 Months | 0–12 Months | Statistics 1 | Quality Rating 2 | |
| EBF vs. FF 1 | BF vs. FF 1 | BF vs. FF 1 | BF vs. FF 1 | ||||
| Berger et al., 2017 [37] | 16 weeks | BF vs. FF No difference in no. of NW, p > 0.05 | t-test | 6 | |||
| Butte et al., 1992 [29] | 17 weeks | BF vs. FF mean ± SD (no.) 2.9 ± 1.8 vs. 2.7 ± 2.0, p > 0.05 | t-test Regression | 5 | |||
| Figueiredo et al., 2017 [38] | 2, 13, 26 weeks | EBF vs. FF mean ± SD (no.) 2 weeks 3.02 ± 0.83 vs. 2.96 ± 0.88, p > 0.05 13 weeks 2.19 ± 1.07 vs. 1.65 ± 1.17, p > 0.05 26 weeks 2.22 ± 1.01 vs. 1.53 ± 0.90, p < 0.01 | BF vs. FF mean ± SD (no.) 2 weeks 2.63 ± 0.67 vs. 2.96 ± 0.88, p > 0.05 13 weeks 2.18 ± 1.36 vs. 1.65 ± 1.17, p > 0.05 26 weeks 1.73 ± 0.94 vs. 1.53 ± 0.90, p > 0.05 | Multivariate Analyses of Chi MANCOVA 3 | 5 | ||
| Kaley et al., 2012 [31] | 4–10 weeks | BF vs. FF BF woke more freq. than FF, p < 0.05 | Correlation ANOVA | 4 | |||
| Quillin et al., 1997 [33] | 4 weeks | BF vs. FF BF infants had more awakenings F(1,39) = 12.231, p < 0.01 | ANOVA-two-way analysis of variance | 3 | |||
| Quillin et al., 2004 [34] | 4 weeks | BF vs. FF Mean ± SD (no.) 8 2.2 ± 0.8 vs. 2.0 ± 0.9, p > 0.05 | t-test | 4 | |||
| Rudzik et al., 2018 [43] | 4, 6, 8, 10, 12, 14, 16, 18 weeks | EBF vs. FF Actigraphy report EBF has 2.1 less NW at 16 weeks, p = 0.05 No difference between grps for number of NW at 4, 6, 8, 10, 12, 14, 18 weeks | t-test | 3 | |||
| Tikotzky et al., 2011 [44] | 26 weeks | EBF vs. FF EBF assoc. with more NW (Actigraph) (r = 0.32, p < 0.05) | Spearman rho correlations | 6 | |||
| Tikotzky et al., 2015 [40] | 26 weeks | EBF vs. FF Mean ± SD (no.) 9 2.53 ± 1.08 vs. 1.48 ± 0.96, p < 0.05 | Spearman CC | 5 | |||
| Wailoo et al., 1990 [36] | 13–17 weeks | BF vs. FF No difference in no. of NW, p > 0.05 | t-test | 2 | |||
| Brown et al., 2015 [19] | 26–52 weeks | BF +/− food vs. FF +/− food No difference in total NW F(1711) = 0.931, p = 0.335 | MANOVA 10 | 5 | |||
| DeLeon et al., 2007 [30] | 39 weeks | BF +/− food vs. FF +/− food BF +ve correlated with NW frequency (r = 0.48, p < 0.01) | Pearson’s correlation coefficient | 4 | |||
| Huang et al., 2016 [39] | 0–34 weeks | BF +/− food vs. FF +/− food BF no diff as compared to FF for NW, p = 0.0700 | Multilevel mixed models | 4 | |||
| Mindell et al., 2012 [17] | 13–52 weeks 4 | BF +/− food vs. FF +/− food mean ± SD (no.) 1.63 ± 1.24 vs. 0.94 ± 0.87, p = 0.003 | MANCOVA | 6 | |||
| Sun et al., 2018 [35] | 8–52 weeks | BF +/− food vs. FF +/− food Freq. NW assoc. with BF (v = 0.18, p = 0.002) | Chi-squared t-test | ||||
| Duration of Night Wakings | |||||||
| Author, Year | Infant Age at Assessment/ Assessment Frequency | ≤6 Months | >6 Months | 0–12 Months | Statistics 1 | Quality Rating 2 | |
| EBF vs. FF 1 | BF vs. FF 1 | BF vs. FF 1 | BF vs. FF 1 | ||||
| Figueiredo et al., 2017 [38] | 2, 13, 26 weeks | EBF vs. FF mean ± SD (h) 2 weeks 3.87 ± 1.13 vs. 4.38 ± 1.18, p > 0.05 13 weeks 3.03 ± 1.16 vs. 3.05 ± 1.20, p > 0.05 26 weeks 2.86 ± 1.01 vs. 2.87 ± 1.12, p > 0.05 | BF vs. FF mean ± SD (h) 2 weeks 4.00 ± 1.11 vs. 4.38 ± 1.18, p > 0.05 13 weeks 3.00 ± 1.16 vs. 3.05 ± 1.20, p > 0.05 26 weeks 2.14 ± 0.90 vs. 2.87 ± 1.12, p > 0.05 | Multivariate analyses of Chi MANCOVA 3 | 5 | ||
| Yoshida et al., 2015 [45] | 13, 17 weeks | EBF vs. FF EBF +ve correlated with wake time at night, p < 0.01 | Multiple linear regression | 5 | |||
| DeLeon et al., 2007 [30] | 39 weeks | BF +/− food vs. FF +/− food BF +ve correlated with duration of NW (r = 0.33, p < 0.05) | Pearson’s correlation coefficient | 4 | |||
| Longest Sleep Period | |||||||
| Author, Year | Infant Age at Assessment/ Assessment Frequency | ≤6 Months | >6 Months | 0–12 Months | Statistics 1 | Quality Rating 2 | |
| EBF vs. FF 1 | BF vs. FF 1 | BF vs. FF 1 | BF vs. FF 1 | ||||
| Figueiredo et al., 2017 [38] | 2, 13, 26 weeks | EBF vs. FF mean ± SD (h) 2 weeks 3.04 ± 1.00 vs. 2.82 ± 0.90, p > 0.05 13 weeks 5.26 ± 2.15 vs. 6.50 ± 2.44, p < 0.05 26 weeks 5.38 ± 2.45 vs. 6.76 ± 1.96, p < 0.05 | BF vs. FF mean ± SD (h) 2 weeks 3.38 ± 1.12 vs. 2.82 ± 0.90, p > 0.05 13 weeks 5.74 ± 2.31 vs. 6.50 ± 2.44, p > 0.05 26 weeks 6.98 ± 2.58 vs. 6.76 ± 1.96, p > 0.05 | Multivariate analyses of Chi MANCOVA 3 | 5 | ||
| Lee et al., 2000 [32] | 2–17 weeks | EBF vs. FF mean ± SD (min) 11 239.9 ± 102.7 vs. 274.1 ± 105.3, p < 0.01 | Unpaired t-test | 4 | |||
| Rudzik et al., 2018 [43] | 4, 6, 8, 10, 12, 14, 16, 18 weeks | EBF vs. FF Actigraph report EBF has 55 min-longer LSP at 18 weeks, p = 0.04 No difference between grps for LSP at 4, 6, 8, 10, 12, 14, 16 weeks | t-test | 3 | |||
| Wailoo et al., 1990 [36] | 13–17 weeks | BF vs. FF BF infants more likely to disturb parents within 4 h (χ2 = 5.9, DF 3, p < 0.01) | t-test | 2 | |||
| Huang et al., 2016 [39] | 0–34 weeks | BF +/− food vs. FF +/− food No assoc. between LSP p > 0.05 | Multilevel mixed models | 4 | |||
| Mindell et al., 2012 [17] | 13–52 weeks 4 | BF +/− food vs. FF +/− food mean ± SD (h) 7.06 ± 2.73 vs. 7.85 ± 2.75, p = 0.249 | MANCOVA | 6 | |||
| Sleep Onset Latency | |||||||
| Author, Year | Infant Age at Assessment/Assessment Frequency | ≤6 Months | >6 Months | 0–12 Months | Statistics 1 | Quality Rating 2 | |
| EBF vs. FF 1 | BF vs. FF 1 | BF vs. FF 1 | BF vs. FF 1 | ||||
| Butte et al., 1992 [29] | 17 weeks | BF vs. FF EEG: mean ± SD (min) 34.3 ± 41.6 vs. 4.0 ± 12.6, p < 0.05 | t-test Regression | 5 | |||
| Figueiredo et al., 2017 [38] | 2, 13, 26 weeks | EBF vs. FF mean ± SD (h) 2 weeks 0.33 ± 0.31 vs. 0.48 ± 0.40, p > 0.05 13 weeks 0.42 ± 0.45 vs. 0.42 ± 0.52, p > 0.05 26 weeks 0.39 ± 0.35 vs. 0.57 ± 0.72, p > 0.05 | BF vs. FF mean ± SD (h) 2 weeks 0.56 ± 0.75 vs. 0.48 ± 0.40, p > 0.05 13 weeks 0.44 ± 0.41 vs. 0.42 ± 0.52, p > 0.05 26 weeks 0.51 ± 0.31 vs. 0.57 ± 0.72, p > 0.05 | Multivariate analyses of Chi MANCOVA 3 | 5 | ||
| Tikotzky et al., 2011 [44] | 26 weeks | EBF vs. FF EBF assoc. with later sleep onset (r = 0.32, p < 0.05) | Spearman rho correlations | 6 | |||
| Mindell et al., 2012 [17] | 13–52 weeks 4 | BF +/− food vs. FF +/− food mean ± SD (h) 0.23 ± 0.15 vs. 0.30 ± 0.53, p = 0.427 | MANCOVA | 6 | |||
| 24 h Sleep Duration | ||||
|---|---|---|---|---|
| Author, Year | Infant Age at Assessment/Assessment Frequency | Sleep Outcomes on Introduction to Complementary Foods | Statistics 1 | Quality Rating 2 |
| Morgan et al., 2004 [46] | 9 months 3 | ≤12 weeks vs. >12 weeks mean ± SE (h) 11.4 ± 0.1 vs. 11.2 ± 0.1, p = 0.07 4 | ANCOVA 5 | 5 |
| Nevarez et al., 2010 [23] | 6, 12 months 3 | <4 months vs. ≥4 months Bivariate 6 months Β =−0.20 (95%CI: −0.47 to 0.07), p > 0.05 12 months Β = −0.38 (95%CI: −0.64 to −0.12), p < 0.05 Multivariate 6 months Β = −0.05 (95%CI: −0.35 to 0.24), p > 0.05 12 months Is β = −0.039 (95%CI: −0.67 to −0.11), p < 0.05 | Bivariate Multivariate linear regression 6 | 5 |
| Heinig et al., 1993 [42] | 9 months | <26 weeks vs. ≥26 weeks mean± SE (h) BF group:12.2 ± 1.1 vs. 12.1 ± 1.0, p > 0.05 FF group: No associations between age of solid food introduction and 24 h sleep duration | Regression | 4 |
| Night-Waking Frequency | ||||
| Author, Year | Infant Age at Assessment/Assessment Frequency | Sleep Outcomes on Introduction to Complementary Foods | Statistics 1 | Quality Rating 2 |
| Brown et al., (2015) [19] | 6–12 months | Outcomes: 8 to 32 weeks (mean 21.2 weeks) No associations between solid food introduction and NW (r = 0.06, p = 0.141) | Pearson’s CC | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, X.; Lovell, A.L.; Braakhuis, A.J.; Mithen, R.F.; Wall, C.R. Type of Milk Feeding and Introduction to Complementary Foods in Relation to Infant Sleep: A Systematic Review. Nutrients 2021, 13, 4105. https://doi.org/10.3390/nu13114105
Fu X, Lovell AL, Braakhuis AJ, Mithen RF, Wall CR. Type of Milk Feeding and Introduction to Complementary Foods in Relation to Infant Sleep: A Systematic Review. Nutrients. 2021; 13(11):4105. https://doi.org/10.3390/nu13114105
Chicago/Turabian StyleFu, Xiaoxi, Amy L. Lovell, Andrea J. Braakhuis, Richard F. Mithen, and Clare R. Wall. 2021. "Type of Milk Feeding and Introduction to Complementary Foods in Relation to Infant Sleep: A Systematic Review" Nutrients 13, no. 11: 4105. https://doi.org/10.3390/nu13114105
APA StyleFu, X., Lovell, A. L., Braakhuis, A. J., Mithen, R. F., & Wall, C. R. (2021). Type of Milk Feeding and Introduction to Complementary Foods in Relation to Infant Sleep: A Systematic Review. Nutrients, 13(11), 4105. https://doi.org/10.3390/nu13114105