Daily Intake and Serum Levels of Copper, Selenium and Zinc According to Glucose Metabolism: Cross-Sectional and Comparative Study

 and
and
Abstract
1. Introduction
2. Materials and Methods
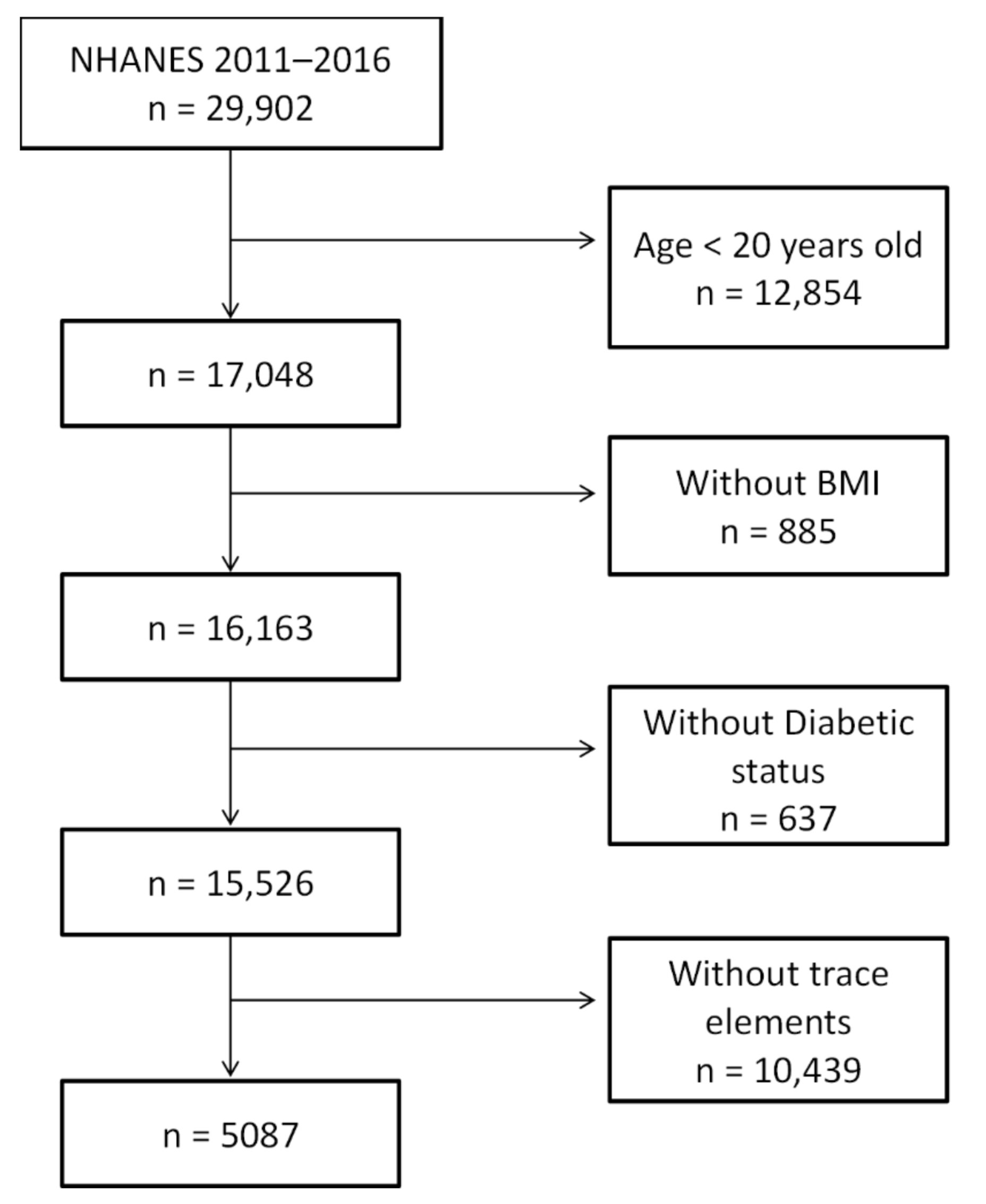
2.1. Study Subjects
2.2. Definition of Glucose Tolerance States
2.3. Laboratory Methods
2.4. Other Measures
2.5. Statistical Analysis
3. Results
3.1. Surveyed Subjects
3.2. Prevalence of Copper, Selenium, and Zinc Deficiency and Excess
3.3. Trace Element Intake and Serum Trace Element Concentration
3.4. Copper
3.5. Selenium
3.6. Zinc
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nordberg, M.; Nordberg, G.F. Trace element research-historical and future aspects. J. Trace Elem. Med. Biol. 2016, 38, 46–52. [Google Scholar] [CrossRef]
- Tako, E. Dietary Trace Minerals. Nutrients 2019, 11, 2823. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Zhu, W.; Wang, W.; Li, R.; Hou, S.; Wang, D.; Yang, L. Selenium in soil and endemic diseases in China. Sci. Total Environ. 2002, 284, 227–235. [Google Scholar] [CrossRef]
- Oh, C.-K.; Moon, Y. Dietary and Sentinel Factors Leading to Hemochromatosis. Nutrients 2019, 11, 1047. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, K.; Bawazeer, N.; Joy, S.S. Variation in Macro and Trace Elements in Progression of Type 2 Diabetes. Sci. World J. 2014, 2014, 461591. [Google Scholar] [CrossRef]
- Dubey, P.; Thakur, V.; Chattopadhyay, M. Role of Minerals and Trace Elements in Diabetes and Insulin Resistance. Nutrients 2020, 12, 1864. [Google Scholar] [CrossRef]
- Chabosseau, P.; Rutter, G.A. Zinc and diabetes. Arch. Biochem. Biophys. 2016, 611, 79–85. [Google Scholar] [CrossRef]
- Qiu, Q.; Zhang, F.; Zhu, W.; Wu, J.; Liang, M. Copper in Diabetes Mellitus: A Meta-Analysis and Systematic Review of Plasma and Serum Studies. Biol. Trace Elem. Res. 2017, 177, 53–63. [Google Scholar] [CrossRef]
- Vinceti, M.; Filippini, T.; Rothman, K.J. Selenium exposure and the risk of type 2 diabetes: A systematic review and meta-analysis. Eur. J. Epidemiol. 2018, 33, 789–810. [Google Scholar] [CrossRef]
- Rodríguez-Pérez, C.; Gómez-Peña, C.; Pérez-Carrascosa, F.M.; Vrhovnik, P.; Echeverría, R.; Salcedo-Bellido, I.; Mustieles, V.; Željka, F.; Arrebola, J.P. Trace elements concentration in adipose tissue and the risk of incident type 2 diabetes in a prospective adult cohort. Environ. Pollut. 2021, 286, 117496. [Google Scholar] [CrossRef]
- Sonkar, S.K.; Parmar, K.S.; Ahmad, M.K.; Sonkar, G.K.; Gautam, M. An observational study to estimate the level of essential trace elements and its implications in type 2 diabetes mellitus patients. J. Fam. Med. Prim. Care 2021, 10, 2594–2599. [Google Scholar] [CrossRef] [PubMed]
- Grădinaru, D.; Margină, D.; Ungurianu, A.; Nițulescu, G.; Pena, C.M.; Ionescu-Tîrgoviște, C.; Miulescu, R.D. Zinc status, insulin resistance and glycoxidative stress in elderly subjects with type 2 diabetes mellitus. Exp. Ther. Med. 2021, 22, 1–6. [Google Scholar] [CrossRef]
- Israt, S.; Nessa, A.; Rahman, H.H.; Sharmin, A.; Akter, N.; Dipa, M.I.; Firoz, S.; Saki, S.A. Correlation between Fasting Serum Glucose and Serum Zinc Level in Patients with Type-2 Diabetes Mellitus. Mymensingh Med. J. 2021, 30, 950–953. [Google Scholar]
- Urbano, T.; Filippini, T.; Lasagni, D.; De Luca, T.; Grill, P.; Sucato, S.; Polledri, E.; Noumbi, G.D.; Malavolti, M.; Santachiara, A.; et al. Association of Urinary and Dietary Selenium and of Serum Selenium Species with Serum Alanine Aminotransferase in a Healthy Italian Population. Antioxidants 2021, 10, 1516. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 43, S14–S31. [CrossRef]
- Tietz, N.W. Textbook of Clinical Chemistry, 3rd ed.; W.B. Saunders Co.: Philadelphia, PA, USA, 1999. [Google Scholar]
- Niskar, A.S.; Paschal, D.C.; Kieszak, S.M.; Flegal, K.M.; Bowman, B.; Gunter, E.W.; Pirkle, J.L.; Rubin, C.; Sampson, E.J.; McGeehin, M. Serum Selenium Levels in the US Population: Third National Health and Nutrition Examination Survey, 1988–1994. Biol. Trace Elem. Res. 2003, 91, 1–10. [Google Scholar] [CrossRef]
- Li, J.; Li, X.; Gathirua-Mwangi, W.; Song, Y. Prevalence and trends in dietary supplement use among US adults with diabetes: The National Health and Nutrition Examination Surveys, 1999–2014. BMJ Open Diabetes Res. Care 2020, 8, e000925. [Google Scholar] [CrossRef]
- Archer, E.; Pavela, G.; Lavie, C.J. The Inadmissibility of What We Eat in America and NHANES Dietary Data in Nutrition and Obesity Research and the Scientific Formulation of National Dietary Guidelines. Mayo Clin. Proc. 2015, 90, 911–926. [Google Scholar] [CrossRef]
- Archer, E.; Hand, G.A.; Blair, S.N. Validity of U.S. Nutritional Surveillance: National Health and Nutrition Examination Survey Caloric Energy Intake Data, 1971–2010. PLoS ONE 2013, 8, e76632. [Google Scholar] [CrossRef]
- Boulet, A.; Vest, K.; Maynard, M.K.; Gammon, M.G.; Russell, A.; Mathews, A.T.; Cole, S.E.; Zhu, X.; Phillips, C.B.; Kwong, J.Q.; et al. The mammalian phosphate carrier SLC25A3 is a mitochondrial copper transporter required for cytochrome c oxidase biogenesis. J. Biol. Chem. 2018, 293, 1887–1896. [Google Scholar] [CrossRef]
- Robinett, N.G.; Peterson, R.L.; Culotta, V.C. Eukaryotic copper-only superoxide dismutases (SODs): A new class of SOD enzymes and SOD-like protein domains. J. Biol. Chem. 2018, 293, 4636–4643. [Google Scholar] [CrossRef]
- Rehman, K.; Akash, M.S.H. Mechanism of Generation of Oxidative Stress and Pathophysiology of Type 2 Diabetes Mellitus: How Are They Interlinked? J. Cell. Biochem. 2017, 118, 3577–3585. [Google Scholar] [CrossRef]
- Weksler-Zangen, S.; Raz, I.; Lenzen, S.; Jörns, A.; Ehrenfeld, S.; Amir, G.; Oprescu, A.; Yagil, Y.; Yagil, C.; Zangen, D.H.; et al. Impaired Glucose-Stimulated Insulin Secretion Is Coupled With Exocrine Pancreatic Lesions in the Cohen Diabetic Rat. Diabetes 2007, 57, 279–287. [Google Scholar] [CrossRef][Green Version]
- Logan, J.; Harveyson, K.; Wisdom, G.; Hughes, A.; Archbold, G. Hereditary caeruloplasmin deficiency, dementia and diabetes mellitus. QJM 1994, 87, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Yonekawa, M.; Okabe, T.; Asamoto, Y.; Ohta, M. A Case of Hereditary Ceruloplasmin Deficiency with Iron Deposition in the Brain Associated with Chorea, Dementia, Diabetes mellitus and Retinal Pigmentation: Administration of Fresh-Frozen Human Plasma. Eur. Neurol. 1999, 42, 157–162. [Google Scholar] [CrossRef]
- Kato, T.; Daimon, M.; Kawanami, T.; Ikezawa, Y.; Sasaki, H.; Maeda, K. Islet changes in hereditary ceruloplasmin deficiency. Hum. Pathol. 1997, 28, 499–502. [Google Scholar] [CrossRef]
- Kapoor, N.; Shetty, S.; Thomas, N.; Paul, T.V. Wilson′s disease: An endocrine revelation. Indian J. Endocrinol. Metab. 2014, 18, 855–857. [Google Scholar] [CrossRef] [PubMed]
- Johansen, K.; Gregersen, G. Glucose intolerance in Wilson’s disease. Normalization after treatment with penicillamine. Arch. Intern. Med. 1972, 129, 587–590. [Google Scholar] [CrossRef]
- Tanaka, A.; Kaneto, H.; Miyatsuka, T.; Yamamoto, K.; Yoshiuchi, K.; Yamasaki, Y.; Shimomura, I.; Matsuoka, T.-A.; Matsuhisa, M. Role of Copper Ion in the Pathogenesis of Type 2 Diabetes. Endocr. J. 2009, 56, 699–706. [Google Scholar] [CrossRef]
- Eshak, E.S.; Iso, H.; Maruyama, K.; Muraki, I.; Tamakoshi, A. Associations between dietary intakes of iron, copper and zinc with risk of type 2 diabetes mellitus: A large population-based prospective cohort study. Clin. Nutr. 2018, 37, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Rayman, M.P. Selenium and human health. Lancet 2012, 379, 1256–1268. [Google Scholar] [CrossRef]
- Mueller, A.S.; Pallauf, J.; Rafael, J. The chemical form of selenium affects insulinomimetic properties of the trace element: Investigations in type II diabetic dbdb mice. J. Nutr. Biochem. 2003, 14, 637–647. [Google Scholar] [CrossRef]
- Becker, D.J.; Reul, B.; Ozcelikay, A.T.; Buchet, J.-P.; Henquin, J.-C.; Brichard, S.M. Oral selenate improves glucose homeostasis and partly reverses abnormal expression of liver glycolytic and gluconeogenic enzymes in diabetic rats. Diabetologia 1996, 39, 3–11. [Google Scholar] [CrossRef]
- Wang, X.-L.; Yang, T.-B.; Wei, J.; Lei, G.-H.; Zeng, C. Association between serum selenium level and type 2 diabetes mellitus: A non-linear dose–response meta-analysis of observational studies. Nutr. J. 2015, 15, 1–9. [Google Scholar] [CrossRef]
- Stranges, S.; Marshall, J.R.; Natarajan, R.; Donahue, R.P.; Trevisan, M.; Combs, G.F.; Cappuccio, F.P.; Ceriello, A.; Reid, M.E. Effects of long-term selenium supplementation on the incidence of type 2 diabetes: A randomized trial. Ann. Intern. Med. 2007, 147, 217–223. [Google Scholar] [CrossRef]
- Cherasse, Y.; Urade, Y. Dietary Zinc Acts as a Sleep Modulator. Int. J. Mol. Sci. 2017, 18, 2334. [Google Scholar] [CrossRef]
- Davidson, H.W.; Wenzlau, J.M.; O’Brien, R.M. Zinc transporter 8 (ZnT8) and β cell function. Trends Endocrinol. Metab. 2014, 25, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Flannick, J.; Thorleifsson, G.; Beer, N.L.; Jacobs, S.B.R.; Grarup, N.; Burtt, N.P.; Mahajan, A.; Fuchsberger, C.; Atzmon, G.; Benediktsson, R.; et al. Loss-of-function mutations in SLC30A8 protect against type 2 diabetes. Nat. Genet. 2014, 46, 357–363. [Google Scholar] [CrossRef]
- Williams, C.L.; Long, A.E. What has zinc transporter 8 autoimmunity taught us about type 1 diabetes? Diabetology 2019, 62, 1969–1976. [Google Scholar] [CrossRef] [PubMed]
- Fukunaka, A.; Fujitani, Y. Role of Zinc Homeostasis in the Pathogenesis of Diabetes and Obesity. Int. J. Mol. Sci. 2018, 19, 476. [Google Scholar] [CrossRef] [PubMed]
- El Dib, R.; Gameiro, O.L.F.; Ogata, M.S.P.; Módolo, N.S.P.; Braz, L.G.; Jorge, E.; Junior, P.D.N.; Beletate, V.; Nascimento, P.D. Zinc supplementation for the prevention of type 2 diabetes mellitus in adults with insulin resistance. Cochrane Database Syst. Rev. 2015, 5, CD005525. [Google Scholar] [CrossRef]
- King, J.C.; Brown, K.H.; Gibson, R.S.; Krebs, N.F.; Lowe, N.M.; Siekmann, J.H.; Raiten, D.J. Biomarkers of Nutrition for Development (BOND)—Zinc Review. J. Nutr. 2015, 146, 858S–885S. [Google Scholar] [CrossRef]
- Bullard, K.M.; Cowie, C.C.; Lessem, S.E.; Saydah, S.H.; Menke, A.; Geiss, L.S.; Orchard, T.; Rolka, D.B.; Imperatore, G. Prevalence of Diagnosed Diabetes in Adults by Diabetes Type—United States, 2016. MMWR. Morb. Mortal. Wkly. Rep. 2018, 67, 359–361. [Google Scholar] [CrossRef]
- A Mulhern, S.; Raveche, E.S.; Smith, H.R.; Lal, R.B. Dietary copper deficiency and autoimmunity in the NZB mouse. Am. J. Clin. Nutr. 1987, 46, 1035–1039. [Google Scholar] [CrossRef]
- Ruggeri, R.M.; D’Ascola, A.; Vicchio, T.M.; Campo, S.; Gianì, F.; Giovinazzo, S.; Frasca, F.; Cannavò, S.; Campennì, A.; Trimarchi, F. Selenium exerts protective effects against oxidative stress and cell damage in human thyrocytes and fibroblasts. Endocrine 2020, 68, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Wessels, I.; Rink, L. Micronutrients in autoimmune diseases: Possible therapeutic benefits of zinc and vitamin D. J. Nutr. Biochem. 2020, 77, 108240. [Google Scholar] [CrossRef]
- Alghobashy, A.A.; Alkholy, U.M.; A Talat, M.; Abdalmonem, N.; Zaki, A.; Ahmed, I.A.; Mohamed, R.H. Trace elements and oxidative stress in children with type 1 diabetes mellitus. Diabetes Metab. Syndr. Obes. Targets Ther. 2018, 11, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Squitti, R.; Negrouk, V.; Perera, M.; Llabre, M.M.; Ricordi, C.; Rongioletti, M.C.A.; Mendez, A.J. Serum copper profile in patients with type 1 diabetes in comparison to other metals. J. Trace Elem. Med. Biol. 2019, 56, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Rungby, J. Zinc, zinc transporters and diabetes. Diabetologia 2010, 53, 1549–1551. [Google Scholar] [CrossRef]
- Hayes, D.P. Nutritional hormesis. Eur. J. Clin. Nutr. 2007, 61, 147–159. [Google Scholar] [CrossRef]


{kind=link}
| All Subjects | Normal Glucose Tolerance | Abnormal Glucose Tolerance | Diabetes Mellitus | p | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | 5087 | 2452 | 1575 | 1060 | |||||||||
| Age (year) | 49 | ± | 18 | 42 | ± | 16 | 53 | ± | 17 | 60 | ± | 14 | <0.0001 |
| Gender (female) | 2578 | 50.68% | 1332 | 54.32% | 751 | 47.68% | 495 | 46.70% | <0.0001 | ||||
| Body mass index (kg/m2) | 29.16 | ± | 7.07 | 27.46 | ± | 6.26 | 29.78 | ± | 7.06 | 32.17 | ± | 7.69 | <0.0001 |
| Current smoker | 986 | 19.38% | 477 | 19.45% | 333 | 21.14% | 176 | 16.60% | 0.02 | ||||
| Current alcohol consumption | 3691 | 72.56% | 1876 | 76.51% | 1099 | 69.78% | 716 | 67.55% | <0.0001 | ||||
| Family history of diabetes | 2061 | 40.52% | 842 | 34.34% | 566 | 35.94% | 653 | 61.60% | <0.0001 | ||||
| Racial/ethnic group | <0.0001 | ||||||||||||
| Mexican Americans | 692 | 13.60% | 289 | 11.79% | 220 | 13.97% | 183 | 17.26% | |||||
| Other Hispanics | 560 | 11.01% | 240 | 9.79% | 188 | 11.94% | 132 | 12.45% | |||||
| Non-Hispanic whites | 1950 | 38.33% | 1052 | 42.90% | 551 | 34.98% | 347 | 32.74% | |||||
| Non-Hispanic blacks | 1092 | 21.47% | 468 | 19.09% | 371 | 23.56% | 253 | 23.87% | |||||
| Others | 793 | 15.59% | 403 | 16.44% | 245 | 15.56% | 145 | 13.68% | |||||
| Established diabetes | 848 | 16.67% | 848 | 80.00% | |||||||||
| Years of diabetes | 12 | ± | 11 | 12 | ± | 11 | |||||||
| Serum copper (ug/dL) | 120.1 | ± | 30.7 | 118.6 | ± | 32.7 | 121.0 | ± | 28.5 | 122.3 | ± | 28.9 | 0.002 |
| Serum selenium (ug/L) | 129.5 | ± | 18.4 | 127.9 | ± | 17.5 | 129.6 | ± | 18.4 | 133.4 | ± | 19.8 | <0.0001 |
| Serum zinc (ug/dL) | 81.5 | ± | 15.3 | 79.9 | ± | 15.3 | 83.2 | ± | 15.2 | 82.6 | ± | 15.0 | <0.0001 |
| Daily Dietary Intake | Daily Supplement | Daily Total Intake | |||||
|---|---|---|---|---|---|---|---|
| Mean | 95%CI | Mean | 95%CI | Mean | 95%CI | ||
| Copper (mg/day) | Normal glucose tolerance | 0.68 | 0.66–0.70 | 1.24 | 1.12–1.36 | 1.06 | 1.01–1.10 |
| Abnormal glucose tolerance | 0.66 | 0.63–0.68 | 1.28 | 1.12–1.44 | 1.07 | 1.01–1.14 | |
| Diabetes mellitus | 0.69 | 0.66–0.73 | 0.94 | 0.73–1.14 | 1.02 | 0.93–1.11 | |
| p * | NS | 0.02 | NS | ||||
| Selenium (mcg/day) | Normal glucose tolerance | 60.29 | 59.02–61.56 | 62.34 | 55.80–68.88 | 79.93 | 77.20–82.66 |
| Abnormal glucose tolerance | 61.64 | 59.85–63.42 | 66.46 | 57.26–75.65 | 82.64 | 78.80–86.48 | |
| Diabetes mellitus | 60.35 | 57.97–62.74 | 62.00 | 50.34–73.66 | 82.03 | 76.91–87.16 | |
| p * | NS | NS | NS | ||||
| Zinc (mg/day) | Normal glucose tolerance | 6.01 | 5.86–6.17 | 13.57 | 12.61–14.53 | 11.00 | 10.52–11.48 |
| Abnormal glucose tolerance | 5.96 | 5.74–6.18 | 14.82 | 13.47–16.17 | 11.44 | 10.76–12.12 | |
| Diabetes mellitus | 5.96 | 5.67–6.25 | 14.31 | 12.51–16.11 | 11.25 | 10.34–12.15 | |
| p * | NS | NS | NS | ||||
| Unweighted | Weighted | ||||
|---|---|---|---|---|---|
| Total | n | % | % | 95% CI | |
| Cu < 20 μg/dL | 5087 | 0 | - | - | - |
| Cu > 302 μg/dL | 5087 | 1 | 0.02% | 0.02% | 0.02–0.02 - |
| Se < 95 μg/L | 5087 | 74 | 1.45% | 1.46% | 1.46–1.46 - |
| Se > 165 μg/L | 5087 | 159 | 3.13% | 3.02% | 3.02–3.02 |
| Zn < 70 μg/dL | 5087 | 1143 | 22.47% | 21.15% | 21.15–21.16 |
| Zn > 120 μg/dL | 5087 | 68 | 1.34% | 1.50% | 1.50–1.50 |
| Serum Cu Concentration | Serum Se Concentration | Serum Zn Concentration | ||||
|---|---|---|---|---|---|---|
| r | p | r | p | r | p | |
| Daily dietary intake | −0.0904 | <0.0001 | 0.0300 | 0.03 | 0.0466 | 0.0009 |
| Daily supplement | 0.0055 | NS | 0.1337 | <0.0001 | 0.1353 | <0.0001 |
| Daily total intake | −0.0349 | 0.01 | 0.1216 | <0.0001 | 0.1426 | <0.0001 |
| Trace Element | Glucose Tolerance Status | Unweighted | Weighted | ||||
|---|---|---|---|---|---|---|---|
| Total | Taking Supplement | Taking Supplement | p | ||||
| N | n | % | % | 95% CI | |||
| Copper | Normal glucose tolerance | 2452 | 636 | 25.94% | 29.21% | 29.20–29.22 | <0.0001 |
| Abnormal glucose tolerance | 1575 | 443 | 28.13% | 32.80% | 32.79–32.81 | ||
| Diabetes mellitus | 1060 | 276 | 26.04% | 31.54% | 31.52–31.55 | ||
| Selenium | Normal glucose tolerance | 2452 | 619 | 25.24% | 29.01% | 29.00–29.02 | <0.0001 |
| Abnormal glucose tolerance | 1575 | 430 | 27.30% | 31.78% | 31.77–31.79 | ||
| Diabetes mellitus | 1060 | 275 | 25.94% | 30.88% | 30.87–30.90 | ||
| Zinc | Normal glucose tolerance | 2452 | 778 | 31.73% | 34.60% | 34.59–34.60 | <0.0001 |
| Abnormal glucose tolerance | 1575 | 495 | 31.43% | 37.08% | 37.07–37.09 | ||
| Diabetes mellitus | 1060 | 302 | 28.49% | 33.90% | 33.89–33.92 | ||
| Normal Glucose Tolerance | Abnormal Glucose Tolerance | Diabetes Mellitus | p | ||
|---|---|---|---|---|---|
| n | 2452 | 1575 | 1060 | ||
| (a) Copper (μg/dL) | |||||
| Model 1 | Weighted mean | 117.83 | 119.63 | 119.68 | NS |
| 95% CI | (116.69–118.96) | (118.08–121.19) | (117.63–121.74) | ||
| Model 2 | Weighted mean | 117.71 | 120.28 | 118.93 | 0.02 |
| 95% CI | (116.67–118.76) | (118.89–121.66) | (117.01–120.85) | ||
| Model 3 | Weighted mean | 117.86 | 120.07 | 118.81 | 0.05 |
| 95% CI | (116.81–118.91) | (118.68–121.45) | (116.87–120.75) | ||
| (b) Selenium (μg/L) | |||||
| Model 1 | Weighted mean | 128.91 | 130.32 | 132.92 | <0.0001 |
| 95% CI | (128.22–129.60) | (129.38–131.27) | (131.67–134.17) | ||
| Model 2 | Weighted mean | 129.16 | 130.02 | 132.62 | <0.0001 |
| 95% CI | (128.44–129.88) | (129.07–130.97) | (131.30–133.93) | ||
| Model 3 | Weighted mean | 129.01 | 130.17 | 132.85 | <0.0001 |
| 95% CI | (128.29–129.72) | (129.23–131.12) | (131.53–134.18) | ||
| (c) Zinc (μg/dL) | |||||
| Model 1 | Weighted mean | 80.22 | 84.94 | 82.84 | <0.0001 |
| 95% CI | (79.66–80.79) | (84.16–85.71) | (81.82–83.87) | ||
| Model 2 | Weighted mean | 79.84 | 85.14 | 83.76 | <0.0001 |
| 95% CI | (79.25–80.43) | (84.36–85.91) | (82.68–84.84) | ||
| Model 3 | Weighted mean | 79.82 | 85.08 | 83.93 | <0.0001 |
| 95% CI | (79.23–80.40) | (84.30–85.85) | (82.85–85.01) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pattan, V.; Chang Villacreses, M.M.; Karnchanasorn, R.; Chiu, K.C.; Samoa, R. Daily Intake and Serum Levels of Copper, Selenium and Zinc According to Glucose Metabolism: Cross-Sectional and Comparative Study. Nutrients 2021, 13, 4044. https://doi.org/10.3390/nu13114044
Pattan V, Chang Villacreses MM, Karnchanasorn R, Chiu KC, Samoa R. Daily Intake and Serum Levels of Copper, Selenium and Zinc According to Glucose Metabolism: Cross-Sectional and Comparative Study. Nutrients. 2021; 13(11):4044. https://doi.org/10.3390/nu13114044
Chicago/Turabian StylePattan, Vishwanath, Maria Mercedes Chang Villacreses, Rudruidee Karnchanasorn, Ken C. Chiu, and Raynald Samoa. 2021. "Daily Intake and Serum Levels of Copper, Selenium and Zinc According to Glucose Metabolism: Cross-Sectional and Comparative Study" Nutrients 13, no. 11: 4044. https://doi.org/10.3390/nu13114044
APA StylePattan, V., Chang Villacreses, M. M., Karnchanasorn, R., Chiu, K. C., & Samoa, R. (2021). Daily Intake and Serum Levels of Copper, Selenium and Zinc According to Glucose Metabolism: Cross-Sectional and Comparative Study. Nutrients, 13(11), 4044. https://doi.org/10.3390/nu13114044