
Breastfeeding Practices and Determinant Factors of Exclusive Breastfeeding among Mothers of Children Aged 0–23 Months in Northwestern Romania


 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
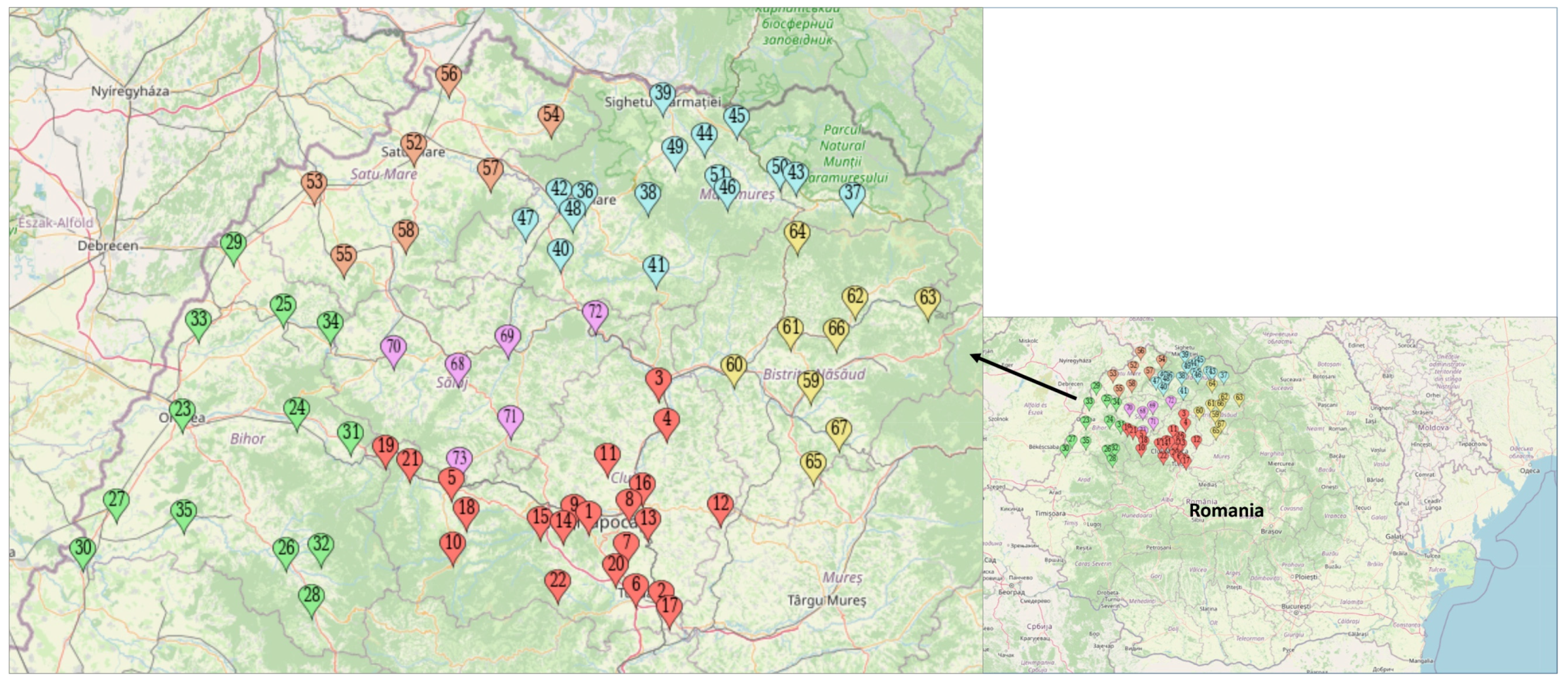
2.1. Study Area
2.2. Participants and Data Collection
2.3. Study Instrument
- Exclusive breastfeeding under 6 months (EBF): the proportion of infants 0–5 months of age who were fed exclusively with breast milk in the last 24 h;
- Continued breastfeeding at 1 year: the proportion of children 12–15 months of age who were fed breast milk in the last 24 h;
- Continued breastfeeding at 2 years: the proportion of children 20–23 months of age who were fed breast milk in the last 24 h;
- Children ever breastfed: the proportion of children born in the last 24 months who were ever breastfed.
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Characteristics of the Participants
3.2. Breastfeeding Practices
3.3. Determinants of Exclusive Breastfeeding
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Wang, Y.; Shan, C.; Zhang, Y.; Ding, L.; Wen, J.; Tian, Y. Early recognition of the preference for exclusive breastfeeding in current China: A prediction model based on decision trees. Sci. Rep. 2020, 10, 6720. [Google Scholar] [CrossRef] [Green Version]
- Ogbo, F.A.; Ezeh, O.K.; Khanlari, S.; Naz, S.; Senanayake, P.; Ahmed, K.Y.; McKenzie, A.; Ogunsiji, O.; Agho, K.; Page, A.; et al. Determinants of exclusive breastfeeding cessation in the early postnatal period among culturally and linguistically diverse (CALD) Australian mothers. Nutrients 2019, 11, 1611. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Yi, D.Y. Components of human breast milk: From macronutrient to microbiome and microRNA. Clin. Exp. Pediatr. 2020, 63, 301–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Victora, C.G.; Bahl, R.; Barros, A.J.D.; França, G.V.A.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C. Lancet Breastfeeding Series Group. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [Green Version]
- Rito, A.I.; Buoncristiano, M.; Spinelli, A.; Salanave, B.; Kunešová, M.; Hejgaard, T.; García Solano, M.; Fijałkowska, A.; Sturua, L.; Hyska, J.; et al. Association between characteristics at birth, breastfeeding and obesity in 22 countries: The WHO European Childhood Obesity Surveillance Initiative—COSI 2015/2017. Obes. Facts 2019, 12, 226–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheshmeh, S.; Nachvak, S.M.; Rezvani, N.; Saber, A. Effects of breastfeeding and formula feeding on the expression level of FTO, CPT1A and PPAR-α genes in healthy infants. Diabetes Metab. Syndr. Obes. 2020, 13, 2227–2237. [Google Scholar] [CrossRef] [PubMed]
- Chiriță Emandi, A.; Puiu, M.; Gafencu, M.; Pienar, C. Overweight and obesity in school age children in western Romania. Rev. Med. Chir. Soc. Med. Naț. Iași 2013, 117, 36–45. [Google Scholar]
- Barbu, C.G.; Teleman, M.D.; Albu, A.I.; Sîrbu, A.E.; Martin, S.C.; Băncescu, A.; Fica, S.V. Obesity and eating behaviors in school children and adolescents—Data from a cross sectional study from Bucharest, Romania. BMC Public Health 2015, 15, 206. [Google Scholar] [CrossRef] [Green Version]
- Bagci Bosi, A.T.; Eriksen, K.G.; Sobko, T.; Wijnhoven, T.M.; Breda, J. Breastfeeding practices and policies in WHO European Region Member States. Public Health Nutr. 2016, 19, 753–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miron, V.D.; Bar, G.; Filimon, C.; Gaidamut, V.A.; Craiu, M. Monitoring of excess body weight in children in the emergency department of a tertiary pediatric hospital in Bucharest, Romania. Maedica 2021, 16, 389–393. [Google Scholar]
- WHO. Global Strategy for Infant and Young Child Feeding; World Health Organization: Geneva, Switzerland, 2003; Available online: https://www.who.int/publications/i/item/9241562218 (accessed on 30 August 2021).
- Zakarija-Grković, I.; Cattaneo, A.; Bettinelli, M.E.; Pilato, C.; Vassallo, C.; Borg Buontempo, M.; Gray, H.; Meynell, C.; Wise, P.; Harutyunyan, S.; et al. Are our babies off to a healthy start? The state of implementation of the Global strategy for infant and young child feeding in Europe. Int. Breastfeed. J. 2020, 15, 51. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Nutrition Monitoring Framework: Operational Guidance for Tracking Progress in Meeting Targets for 2025; World Health Organization: Geneva, Switzerland, 2017; Available online: https://www.who.int/publications/i/item/9789241513609 (accessed on 30 August 2021).
- Romanian Ministry of Health; World Bank; UNFPA; USAID; UNICEF. Reproductive Health Survey: Romania. 2004. Available online: https://www.insmc.ro/wp-content/uploads/2021/01/studiul_sanatati_reproducerii.pdf (accessed on 31 August 2021).
- Nanu, M.I.; Moldovanu, F.; Stativă, E.; Stoicescu, S. Evaluating the Effectiveness of Interventions Included in National Nutrition Programs for Children under 2 Years of Age. Available online: https://www.insmc.ro/wp-content/uploads/2021/01/Nutritie-sub-2-ani-raport-final-studiu.pdf (accessed on 31 August 2021).
- Rollins, N.C.; Bhandari, N.; Hajeebhoy, N.; Horton, S.; Lutter, C.K.; Martines, J.C.; Piwoz, E.G.; Richter, L.M.; Victora, C.G.; Lancet Breastfeeding Series Group. Why invest, and what it will take to improve breastfeeding practices? Lancet 2016, 387, 491–504. [Google Scholar] [CrossRef]
- Iliodromiti, Z.; Zografaki, I.; Papamichail, D.; Stavrou, T.; Gaki, E.; Ekizoglou, C.; Nteka, E.; Mavrika, P.; Zidropoulos, S.; Panagiotopoulos, T.; et al. Increase of breast-feeding in the past decade in Greece, but still low uptake: Cross-sectional studies in 2007 and 2017. Public Health Nutr. 2020, 23, 961–970. [Google Scholar] [CrossRef] [PubMed]
- Inano, H.; Kameya, M.; Sasano, K.; Matsumura, K.; Tsuchida, A.; Hamazaki, K.; Inadera, H.; Hasegawa, T. Japan Environment and Children’s Study (JECS) Group. Factors influencing exclusive breastfeeding rates until 6 months postpartum: The Japan Environment and Children’s Study. Sci. Rep. 2021, 11, 6841. [Google Scholar] [CrossRef] [PubMed]
- Romanian North-West Regional Development Agency. Northwestern Regional Development Plan 2021–2027. Available online: https://www.nord-vest.ro/wp-content/uploads/2021/02/PDR-NV-2021-2027-versiunea-feb-2021.pdf (accessed on 6 November 2021).
- National Institute for Statistics Romania. TEMPO-Online Database. Available online: http://statistici.insse.ro:8077/tempo-online/#/pages/tables/insse-table (accessed on 6 November 2021).
- National Institute for Statistics Romania. The 2011 Census of the Population and Housing in Romania. Available online: http://www.recensamantromania.ro/rezultate-2/ (accessed on 6 November 2021).
- Cozma-Petruţ, A.; Badiu-Tişa, I.; Stanciu, O.; Filip, L.; Banc, R.; Gavrilaş, L.; Ciobârcă, D.; Hegheş, S.C.; Miere, D. Determinants of early initiation of breastfeeding among mothers of children aged less than 24 months in northwestern Romania. Nutrients 2019, 11, 2988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO; UNICEF; USAID; AED; UCDAVIS; IFPRI. Indicators for Assessing Infant and Young Child Feeding Practices. Part II: Measurement. Geneva: World Health Organization. 2010. Available online: https://apps.who.int/nutrition/publications/infantfeeding/9789241599290/en/index.html (accessed on 7 September 2021).
- World Breastfeeding Trends Initiative Country Reports. Available online: https://www.worldbreastfeedingtrends.org/wbti-country-report.php (accessed on 21 September 2021).
- Grgurić, J.; Zakarija-Grković, I.; Pavičić Bošnjak, A.; Stanojević, M. A multifaceted approach to revitalizing the Baby-Friendly Hospital Initiative in Croatia. J. Hum. Lact. 2016, 32, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Rangelova, L.; Duleva, V. Current breastfeeding practices in Bulgaria. In Proceedings of the Nutrition Society 2020, 79, OCE2—13th European Nutrition Conference, FENS 2019, 15–18 October 2019, Malnutrition in an Obese World: European Perspectives, Dublin-Ireland; Cambridge University Press: Cambridge, UK, 2020. [Google Scholar] [CrossRef]
- Courtois, F.; Péneau, S.; Salanave, B.; Andreeva, V.A.; Roland-Cachera, M.F.; Touvier, M.; Galan, P.; Hercberg, S.; Fezeu, L.K. Trends in breastfeeding practices and mothers’ experience in the French NutriNet-Santé cohort. Int. Breastfeed. J. 2021, 16, 50. [Google Scholar] [CrossRef]
- Oakley, L.L.; Kurinczuk, J.J.; Renfrew, M.J.; Quigley, M.A. Breastfeeding in England: Time trends 2005–2006 to 2012–2013 and inequalities by area profile. Matern. Child Nutr. 2016, 12, 440–451. [Google Scholar] [CrossRef]
- Papoutsou, S.; Savva, S.C.; Hunsberger, M.; Jilani, H.; Michels, N.; Ahrens, W.; Tornaritis, M.; Veidebaum, T.; Molnár, D.; Siani, A.; et al. IDEFICS consortium. Timing of solid food introduction and association with later childhood overweight and obesity: The IDEFICS study. Matern. Child Nutr. 2018, 14, e12471. [Google Scholar] [CrossRef] [Green Version]
- Pluymen, L.P.M.; Wijga, A.H.; Gehring, U.; Koppelman, G.H.; Smit, H.A.; van Rossem, L. Early introduction of complementary foods and childhood overweight in breastfed and formula-fed infants in the Netherlands: The PIAMA birth cohort study. Eur. J. Nutr. 2018, 57, 1985–1993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, G.; Coulthard, H. Early eating behaviours and food acceptance revisited: Breastfeeding and introduction of complementary foods as predictive of food acceptance. Curr. Obes. Rep. 2016, 5, 113–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, K.M.; Li, M.; Zhu, B.; Liang, F.; Shao, J.; Zhang, Y.; Ji, C.; Zhao, Z.; Kaciroti, N.; Lozoff, B. Breastfeeding, mixed, or formula feeding at 9 months of age and the prevalence of iron deficiency and iron deficiency anemia in two cohorts of infants in China. J. Pediatr. 2017, 181, 56–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stativa, E.; Rus, A.V.; Stanescu, A.; Pennings, J.S.; Parris, S.R.; Wenyika, R. Prevalence and predictors of anaemia in Romanian infants 6–23 months old. J. Public Health. 2016, 38, e72–e81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krebs, N.F. Food based complementary feeding strategies for breastfed infants: What’s the evidence that it matters? Nutr. Today. 2014, 49, 271–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadjiona, V.; Middleton, N.; Kouta, C.; Hadjigeorgiou, E.; Lambrinou, E.; Kolokotroni, O. Cyprus mothers’ breastfeeding self-efficacy and their perceptions about the implementation of the ‘10 steps’ in the first 48hours after birth. Midwifery 2016, 36, 43–52. [Google Scholar] [CrossRef]
- Daglas, M.; Petoussi, V.; Dionysiou, G.; Athanassakis, I. Do maternity hospital practices support Greek mothers’ decision to breastfeed? Clin. Exp. Obstet. Gynecol. 2010, 37, 43–48. [Google Scholar]
- Ragusa, R.; Giorgianni, G.; Marranzano, M.; Cacciola, S.; La Rosa, V.L.; Giarratana, A.; Altadonna, V.; Guardabasso, V. Breastfeeding in hospitals: Factors influencing maternal choice in Italy. Int. J. Environ. Res. Public Health 2020, 17, 3575. [Google Scholar] [CrossRef] [PubMed]
- Coman, E.; Diaconu, A.; Mesesan Schmitz, L.; Repanovici, A.; Baritz, M.; Coman, C.; Fotea, S. Patient satisfaction with private recovery services and importance of physician behavior during COVID time. Healthcare 2021, 9, 928. [Google Scholar] [CrossRef]
- Romanian Private Maternity Hospital “Queen Maria”. Available online: https://www.reginamaria.ro/lc-maternitate-cluj?gclid=CjwKCAjw8KmLBhB8EiwAQbqNoDNeqUAZxpq6J9sIjmv6MoIfOKkQS6gQkbjpuCKsY0ofpJTt-9L8IRoCS4UQAvD_BwE (accessed on 27 September 2021).
- Ragusa, R.; Marranzano, M.; La Rosa, V.L.; Giorgianni, G.; Commodari, E.; Quattrocchi, R.; Cacciola, S.; Guardabasso, V. Factors influencing uptake of breastfeeding: The role of early promotion in the maternity hospital. Int. J. Environ. Res. Public Health 2021, 18, 4783. [Google Scholar] [CrossRef]
- Mirkovic, K.R.; Perrine, C.G.; Scanlon, K.S. Paid maternity leave and breastfeeding outcomes. Birth 2016, 43, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, F.R.; Buccini, G.D.S.; Venâncio, S.I.; da Costa, T.H.M. Influence of maternity leave on exclusive breastfeeding. J. Pediatr. 2017, 93, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Steurer, L.M. Maternity leave length and workplace policies’ impact on the sustainment of breastfeeding: Global perspectives. Public Health Nurs. 2017, 34, 286–294. [Google Scholar] [CrossRef] [PubMed]
- de Lauzon-Guillain, B.; Thierry, X.; Bois, C.; Bournez, M.; Davisse-Paturet, C.; Dufourg, M.N.; Kersuzan, C.; Ksiazek, E.; Nicklaus, S.; Vicaire, H.; et al. Maternity or parental leave and breastfeeding duration: Results from the ELFE cohort. Matern. Child Nutr. 2019, 15, e12872. [Google Scholar] [CrossRef] [PubMed]
- Macht, A.; Popescu, R. Romania Country note. In International Review of Leave Policies and Research 2020; Koslowski, A., Blum, S., Dobrotić, I., Kaufman, G., Moss, P., Eds.; Deposit_Hagen: Hagen, Germany, 2020; Available online: https://ub-deposit.fernuni-hagen.de/servlets/MCRFileNodeServlet/mir_derivate_00002067/Koslowski_et_al_Leave_Policies_2020.pdf (accessed on 27 September 2021).
- Romanian National Center for Health Assessment and Promotion. Available online: https://insp.gov.ro/sites/cnepss/resurse-imc-alimentatia-la-san/ (accessed on 1 October 2021).
- National Institute of Public Health. Prevention Guide. Volume 6. Problems of Nutrition, Growth and Development in Children: Nutrition between 0–2 Years, Growth and Development Disorders. Available online: https://cnsmf.ro/ghidpreventie/GhidPreventie_Vol6.pdf (accessed on 1 October 2021).
- SAMAS Association—Health for Mothers and Infants. About the Activity of the Association. Available online: https://www.programsamas.ro/sanatatea-lui-incepe-cu-laptele-tau/ (accessed on 1 October 2021).
- UNICEF; Babeș-Bolyai University Cluj-Napoca, Romania. College of Political, Administrative and Communication Sciences. Department of Public Health. Action Lines to Promote Breastfeeding in Romania—Policy Brief. Available online: https://www.unicef.org/romania/media/4431/file/Policy%20Brief%20-%20engl.pdf (accessed on 4 November 2021).
- Mulol, H.; Coutsoudis, A. Limitations of maternal recall for measuring exclusive breastfeeding rates in South African mothers. Int. Breastfeed. J. 2018, 13, 19. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Frequency | Percent |
|---|---|---|
| Sociodemographic Characteristics | ||
| Maternal age (years) | ||
| <18 | 31 | 2.2 |
| 18–24 | 184 | 13.2 |
| 25–34 | 940 | 67.2 |
| ≥35 | 244 | 17.4 |
| Place of residence | ||
| Urban | 1027 | 73.4 |
| Rural | 372 | 26.6 |
| Marital status | ||
| Married/Living with a partner | 1382 | 98.8 |
| Single/Divorced/Widowed | 17 | 1.2 |
| Education | ||
| ≤Secondary school | 118 | 8.4 |
| Completed high school or equivalent | 304 | 21.7 |
| Bachelor’s degree or higher | 977 | 69.9 |
| Occupation | ||
| Employed | 1231 | 88.0 |
| Unemployed | 168 | 12.0 |
| Family financial wellbeing # | ||
| Poor | 235 | 16.8 |
| Fair | 301 | 21.5 |
| Good | 309 | 22.1 |
| Very good | 172 | 12.3 |
| Excellent | 180 | 12.9 |
| Parity | ||
| Primiparous | 833 | 59.5 |
| Multiparous | 566 | 40.5 |
| Child gender | ||
| Female | 683 | 48.8 |
| Male | 716 | 51.2 |
| Child age at interview (months) | ||
| 0–5 | 377 | 26.9 |
| 6–11 | 405 | 29.0 |
| 12–23 | 617 | 44.1 |
| Duration of parental leave | ||
| Less than 22 months from childbirth | 268 | 19.2 |
| 22 months or more from childbirth | 1131 | 80.8 |
| Pre/perinatal characteristics | ||
| Gestational age at delivery (weeks) | ||
| <37 | 170 | 12.1 |
| ≥37 | 1229 | 87.9 |
| Birth weight (grams) | ||
| <2500 | 69 | 4.9 |
| 2500–4199 | 1280 | 91.5 |
| ≥4200 | 50 | 3.6 |
| Mode of delivery | ||
| Vaginal delivery | 678 | 48.5 |
| Caesarean section | 721 | 51.5 |
| Place of delivery | ||
| Public hospital | 1021 | 73.0 |
| Private hospital | 378 | 27.0 |
| Skin-to-skin contact the first hour after birth | ||
| Yes | 303 | 21.7 |
| No | 1096 | 78.3 |
| Initiation of breastfeeding the first hour after birth | ||
| Yes | 340 | 24.3 |
| No | 1059 | 75.7 |
| Prenatal birth and infant care classes | ||
| Yes | 401 | 28.7 |
| No | 998 | 71.3 |
| Breastfeeding education during prenatal visits | ||
| Yes | 699 | 50.0 |
| No | 700 | 50.0 |
| Postnatal breastfeeding education | ||
| Yes | 1053 | 75.3 |
| No | 346 | 24.7 |
| Breastfeeding Practice | Frequency | Percent |
|---|---|---|
| Exclusive breastfeeding under 6 months (EBF) (n = 379) | 177 | 46.7 |
| Continued breastfeeding at 1 year (n = 203) | 110 | 54.2 |
| Continued breastfeeding at 2 years (n = 221) | 67 | 30.3 |
| Children ever breastfed (n = 1399) | 1339 | 95.7 |
| Characteristics | Unadjusted OR (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value |
|---|---|---|---|---|
| Sociodemographic Characteristics | ||||
| Maternal age (years) | ||||
| <18 | 2.70 (1.07, 6.80) | 0.035 * | 2.81 (0.98, 8.06) | 0.055 |
| 18–24 | 1.00 | |||
| 25–34 | 1.19 (0.73, 1.95) | 0.487 | 1.17 (0.68, 2.02) | 0.570 |
| ≥35 | 0.81 (0.43, 1.51) | 0.503 | 0.87 (0.43, 1.76) | 0.704 |
| Place of residence | ||||
| Urban | 1.00 | |||
| Rural | 1.07 (0.75, 1.52) | 0.725 | ||
| Education | ||||
| ≤Secondary school | 1.89 (1.01, 3.54) | 0.046 * | 1.46 (0.71, 3.01) | 0.306 |
| Completed high school or equivalent | 1.00 | |||
| Bachelor’s degree or higher | 1.51 (0.98, 2.33) | 0.059 | 1.34 (0.82, 2.21) | 0.243 |
| Occupation | ||||
| Employed | 1.00 | |||
| Unemployed | 1.17 (0.74, 1.87) | 0.497 | ||
| Family financial wellbeing | ||||
| Poor | 1.00 | |||
| Fair | 0.60 (0.37, 0.99) | 0.044 * | 0.63 (0.37, 1.08) | 0.094 |
| Good | 0.70 (0.44, 1.14) | 0.150 | 0.72 (0.41, 1.25) | 0.236 |
| Very good | 0.99 (0.59, 1.67) | 0.966 | 0.95 (0.52, 1.77) | 0.880 |
| Excellent | 0.58 (0.32, 1.03) | 0.064 | 0.57 (0.29, 1.14) | 0.110 |
| Parity | ||||
| Primiparous | 1.00 | |||
| Multiparous | 1.22 (0.89, 1.67) | 0.226 | ||
| Child gender | ||||
| Female | 1.10 (0.80, 1.50) | 0.564 | ||
| Male | 1.00 | |||
| Duration of parental leave | ||||
| Less than 22 months from childbirth | 1.00 | 1.00 | ||
| 22 months or more from childbirth | 5.71 (2.77, 11.76) | 0.000 ** | 7.90 (3.43, 18.22) | 0.000 ** |
| Pre/perinatal characteristics | ||||
| Gestational age at delivery (weeks) | ||||
| <37 | 1.00 | |||
| ≥37 | 1.35 (0.79, 2.28) | 0.269 | ||
| Birth weight (grams) | ||||
| <2500 | 0.53 (0.21, 1.34) | 0.181 | ||
| 2500–4199 | 1.00 | |||
| ≥4200 | 1.30 (0.60, 2.81) | 0.511 | ||
| Mode of delivery | ||||
| Vaginal delivery | 1.37 (1.00, 1.89) | 0.050 * | 1.27 (0.87, 1.87) | 0.218 |
| Caesarean section | 1.00 | 1.00 | ||
| Place of delivery | ||||
| Public hospital | 1.00 | 1.00 | ||
| Private hospital | 1.55 (1.11, 2.16) | 0.011 * | 1.62 (1.06, 2.48) | 0.026 * |
| Skin-to-skin contact the first hour after birth | ||||
| Yes | 1.72 (1.21, 2.43) | 0.002 * | 1.45 (0.94, 2.24) | 0.094 |
| No | 1.00 | 1.00 | ||
| Initiation of breastfeeding the first hour after birth | ||||
| Yes | 1.53 (1.08, 2.16) | 0.015 * | 1.14 (0.70, 1.87) | 0.601 |
| No | 1.00 | 1.00 | ||
| Prenatal birth and infant care classes | - | |||
| Yes | 1.11 (0.79, 1.56) | 0.561 | - | |
| No | 1.00 | - | ||
| Breastfeeding education during prenatal visits | ||||
| Yes | 1.15 (0.84, 1.58) | 0.371 | - | |
| No | 1.00 | - | ||
| Postnatal breastfeeding education | ||||
| Yes | 1.00 | - | ||
| No | 1.12 (0.78, 1.60) | 0.548 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cozma-Petruţ, A.; Filip, L.; Banc, R.; Mîrza, O.; Gavrilaş, L.; Ciobârcă, D.; Badiu-Tişa, I.; Hegheş, S.C.; Popa, C.O.; Miere, D. Breastfeeding Practices and Determinant Factors of Exclusive Breastfeeding among Mothers of Children Aged 0–23 Months in Northwestern Romania. Nutrients 2021, 13, 3998. https://doi.org/10.3390/nu13113998
Cozma-Petruţ A, Filip L, Banc R, Mîrza O, Gavrilaş L, Ciobârcă D, Badiu-Tişa I, Hegheş SC, Popa CO, Miere D. Breastfeeding Practices and Determinant Factors of Exclusive Breastfeeding among Mothers of Children Aged 0–23 Months in Northwestern Romania. Nutrients. 2021; 13(11):3998. https://doi.org/10.3390/nu13113998
Chicago/Turabian StyleCozma-Petruţ, Anamaria, Lorena Filip, Roxana Banc, Oana Mîrza, Laura Gavrilaş, Daniela Ciobârcă, Ioana Badiu-Tişa, Simona Codruţa Hegheş, Cristian Olimpiu Popa, and Doina Miere. 2021. "Breastfeeding Practices and Determinant Factors of Exclusive Breastfeeding among Mothers of Children Aged 0–23 Months in Northwestern Romania" Nutrients 13, no. 11: 3998. https://doi.org/10.3390/nu13113998
APA StyleCozma-Petruţ, A., Filip, L., Banc, R., Mîrza, O., Gavrilaş, L., Ciobârcă, D., Badiu-Tişa, I., Hegheş, S. C., Popa, C. O., & Miere, D. (2021). Breastfeeding Practices and Determinant Factors of Exclusive Breastfeeding among Mothers of Children Aged 0–23 Months in Northwestern Romania. Nutrients, 13(11), 3998. https://doi.org/10.3390/nu13113998