
The Effect of Weight-Loss Interventions on Cervical and Chin Subcutaneous Fat Depots; the CENTRAL Randomized Controlled Trial

 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
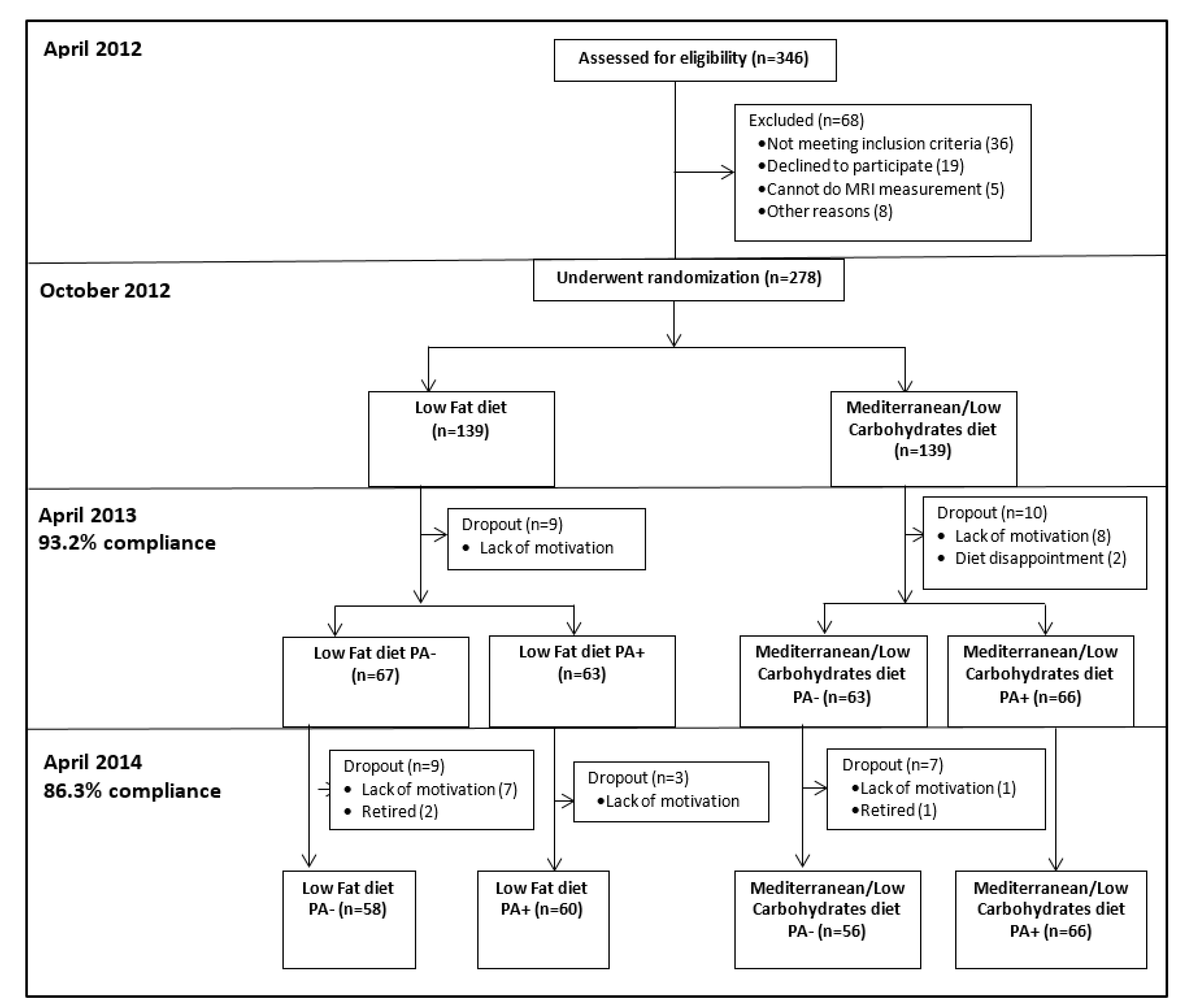
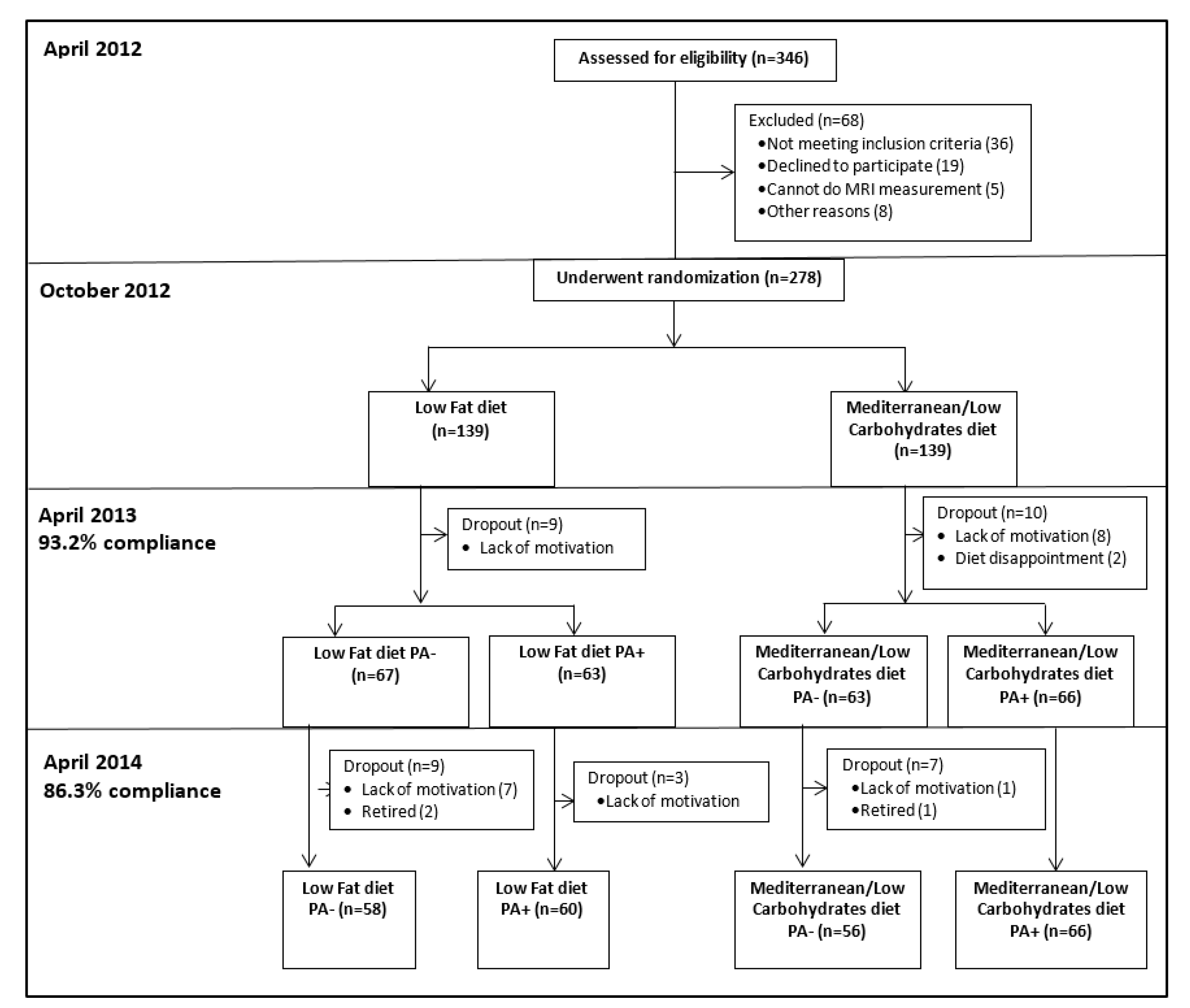
2.1. Eligibility and Study Design
2.2. Outcomes
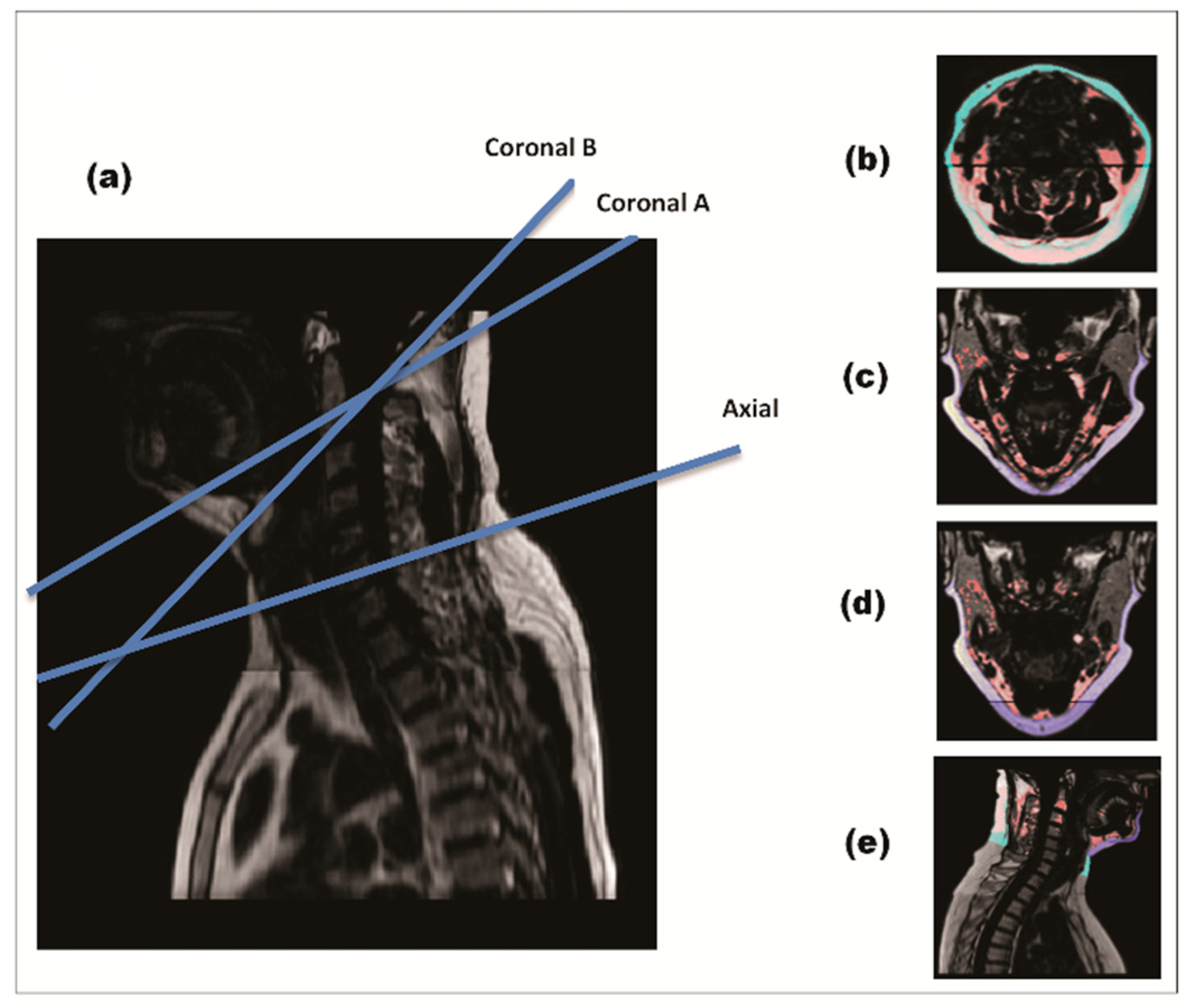
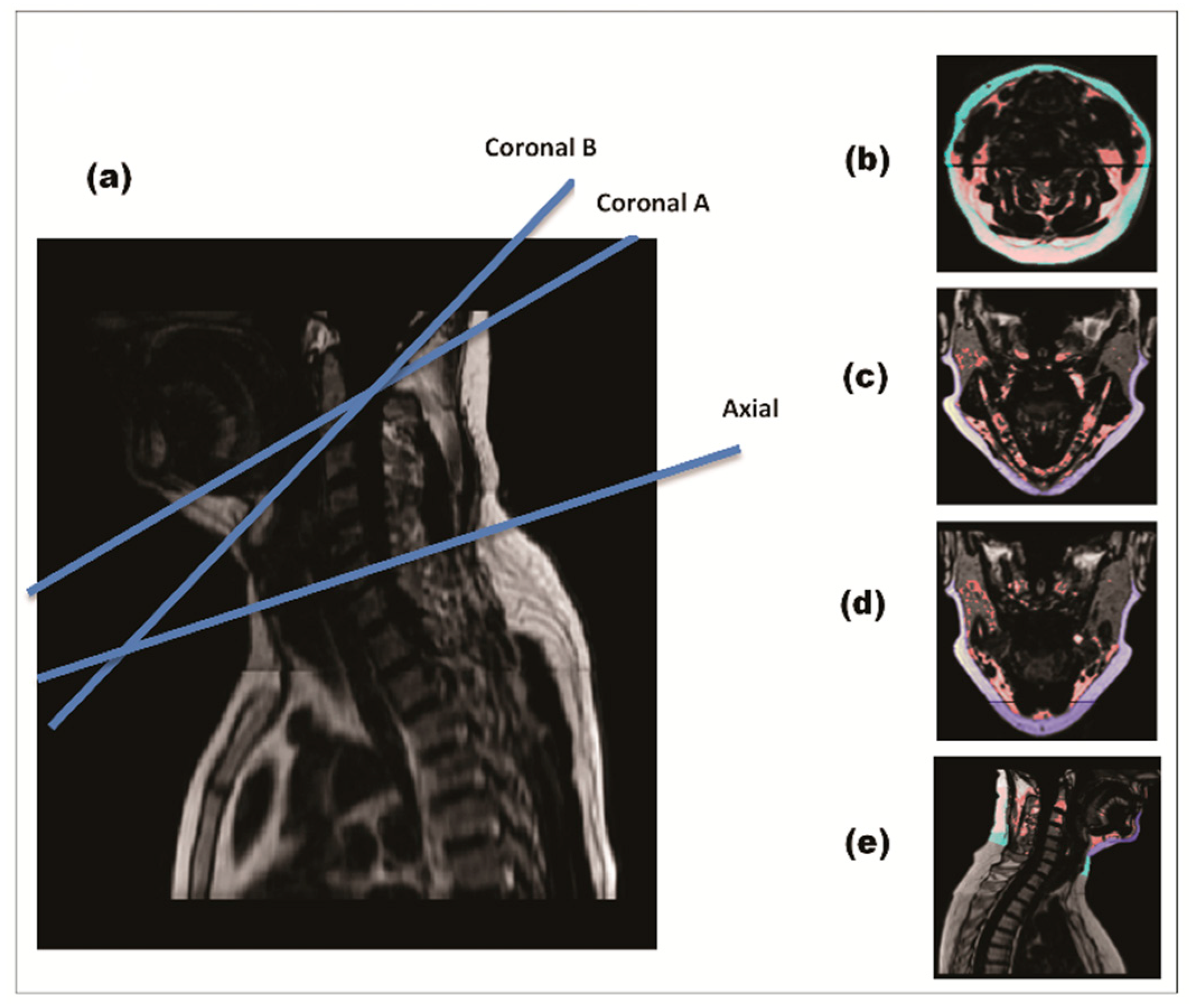
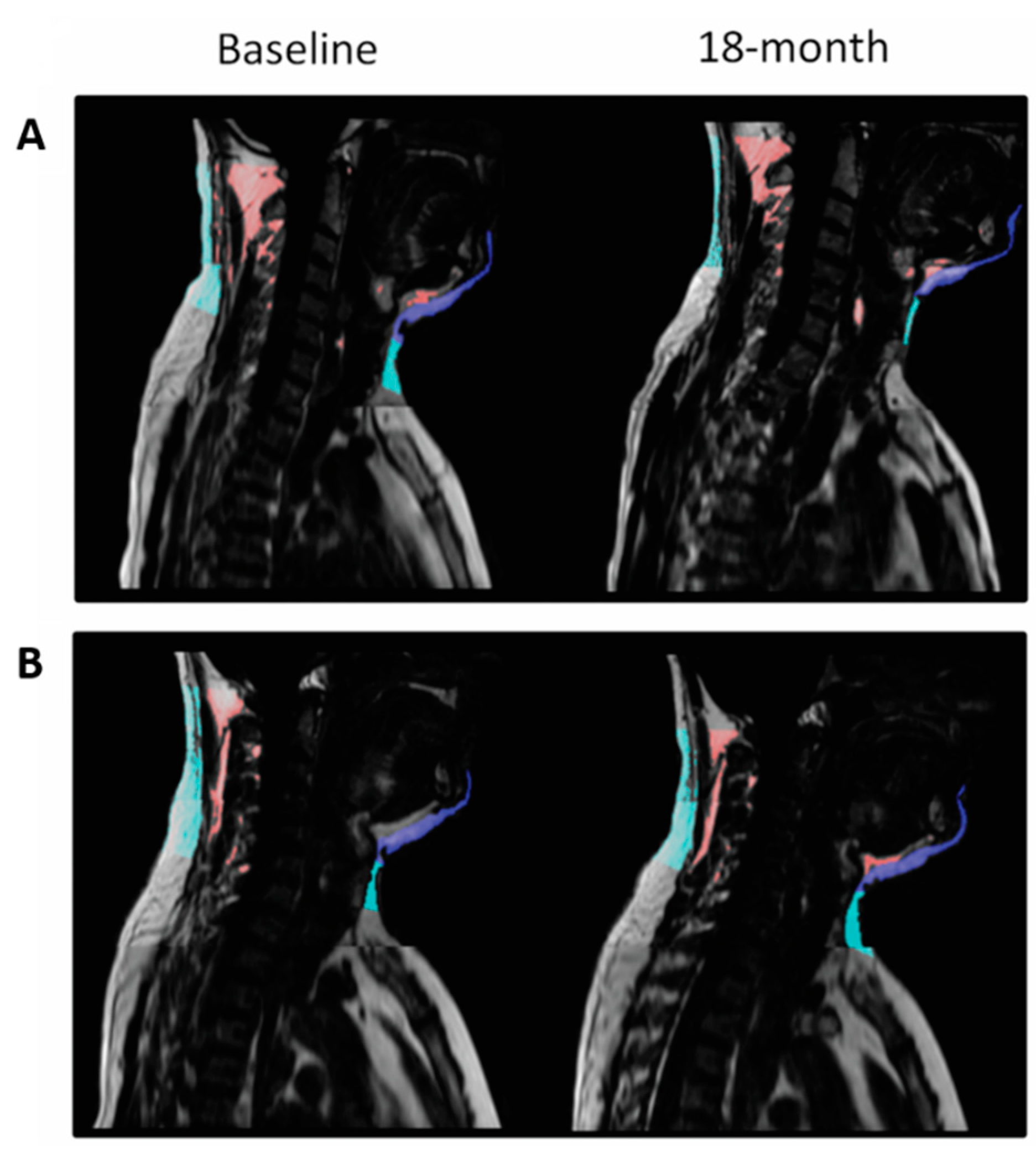
2.2.1. Magnetic Resonance Imaging
2.2.2. Clinical and Anthropometric Outcomes
2.2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
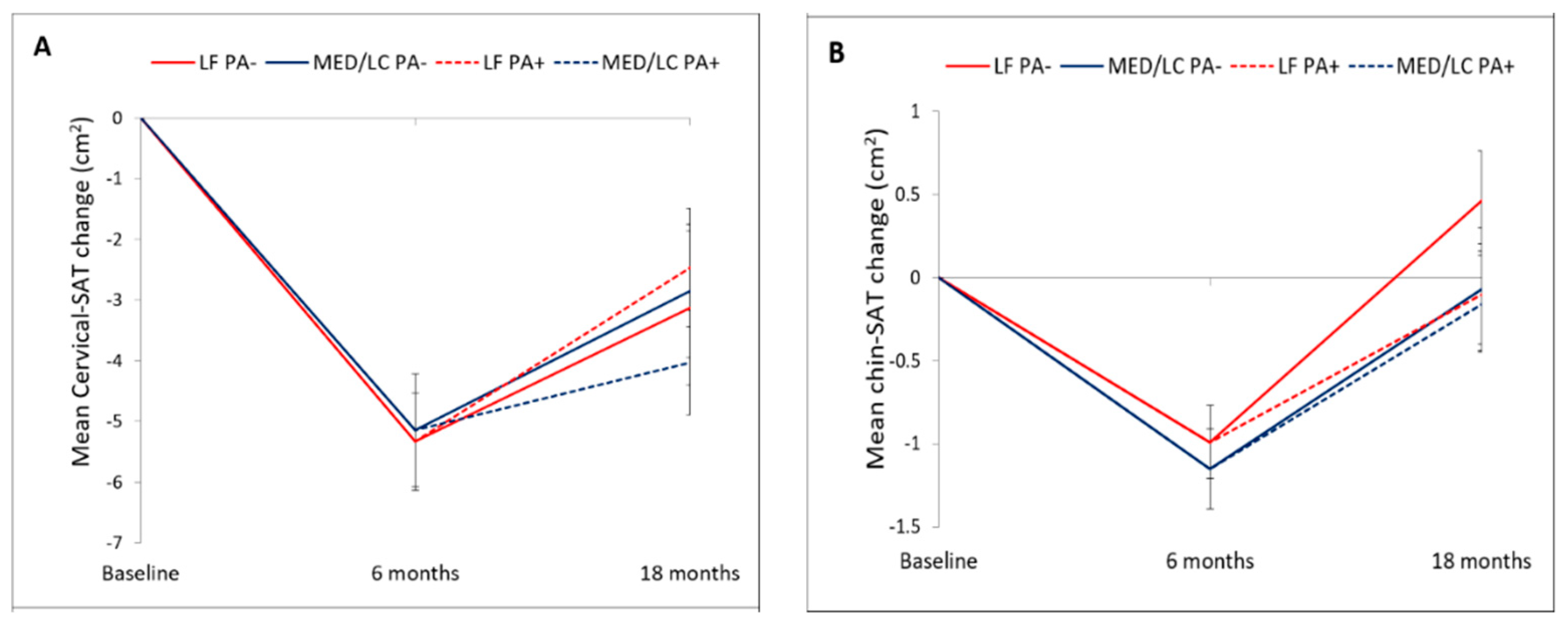
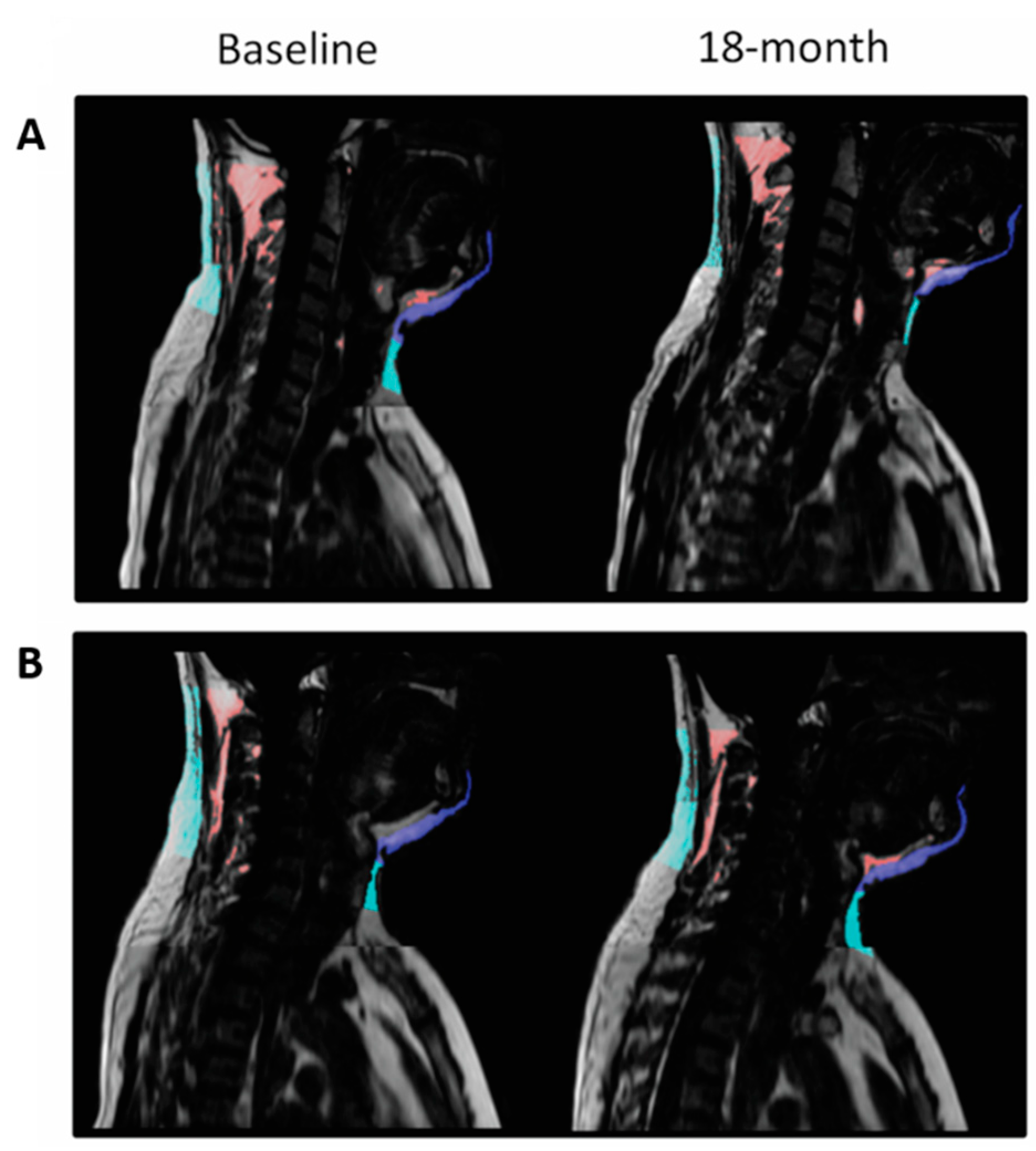
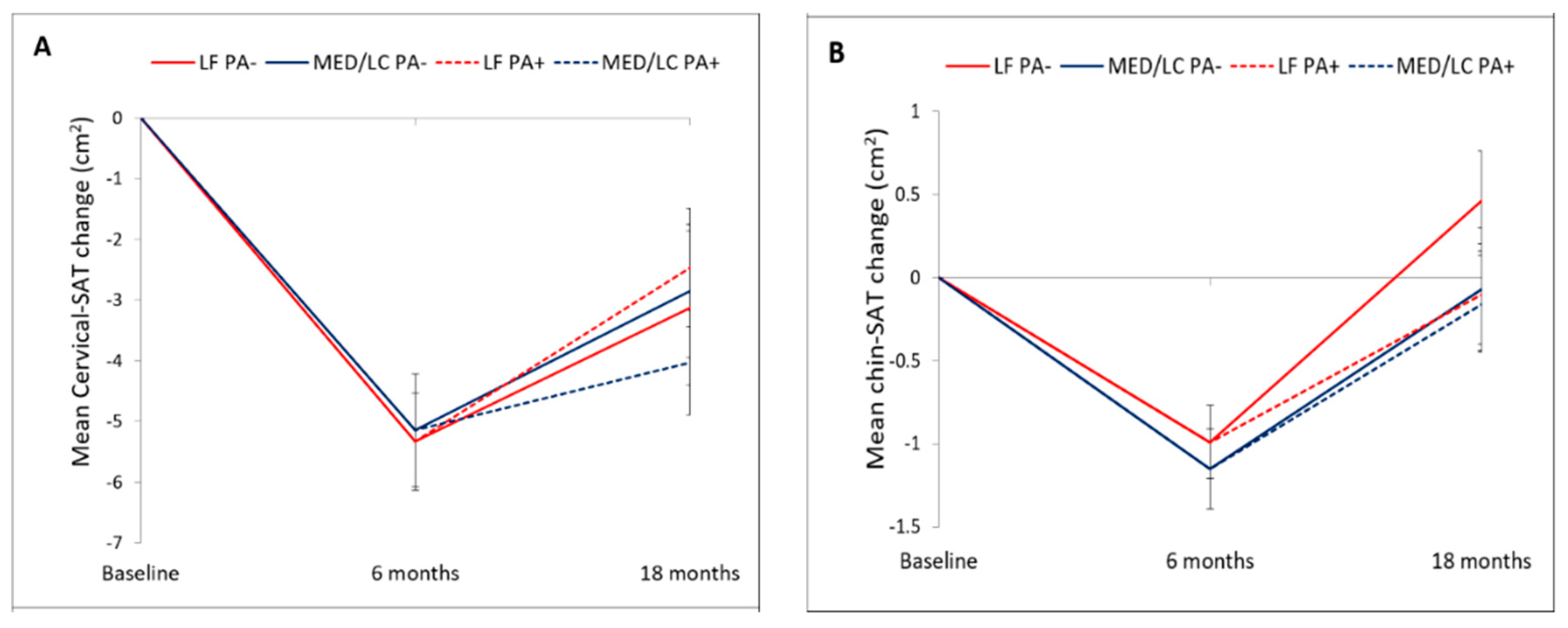
3.2. Changes in Cervical and Chin SATs during the Lifestyle Intervention
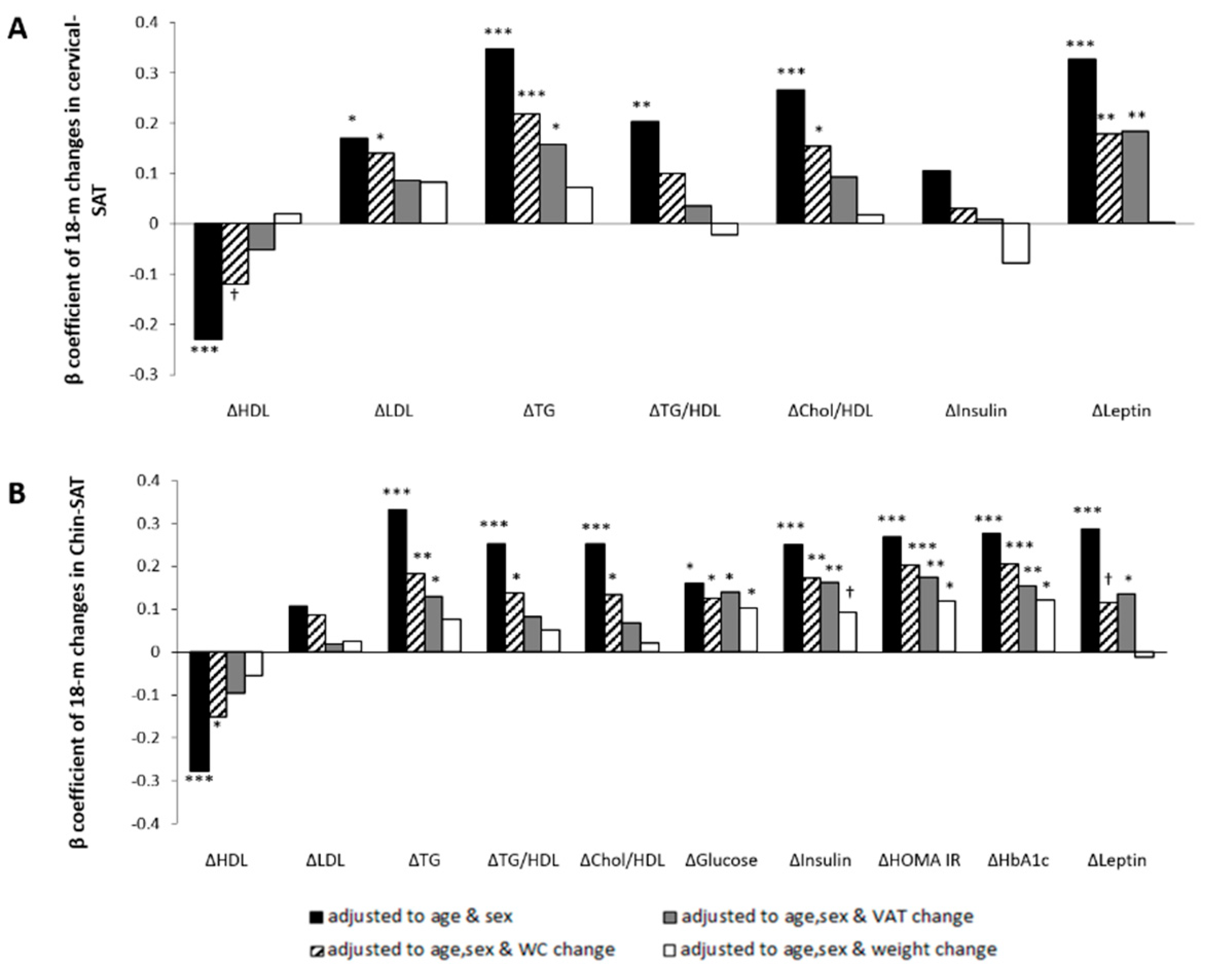
3.3. Association between 18-Month Changes in Cervical-SAT with Changes in Anthropometric Measurements and Body Fat Depots
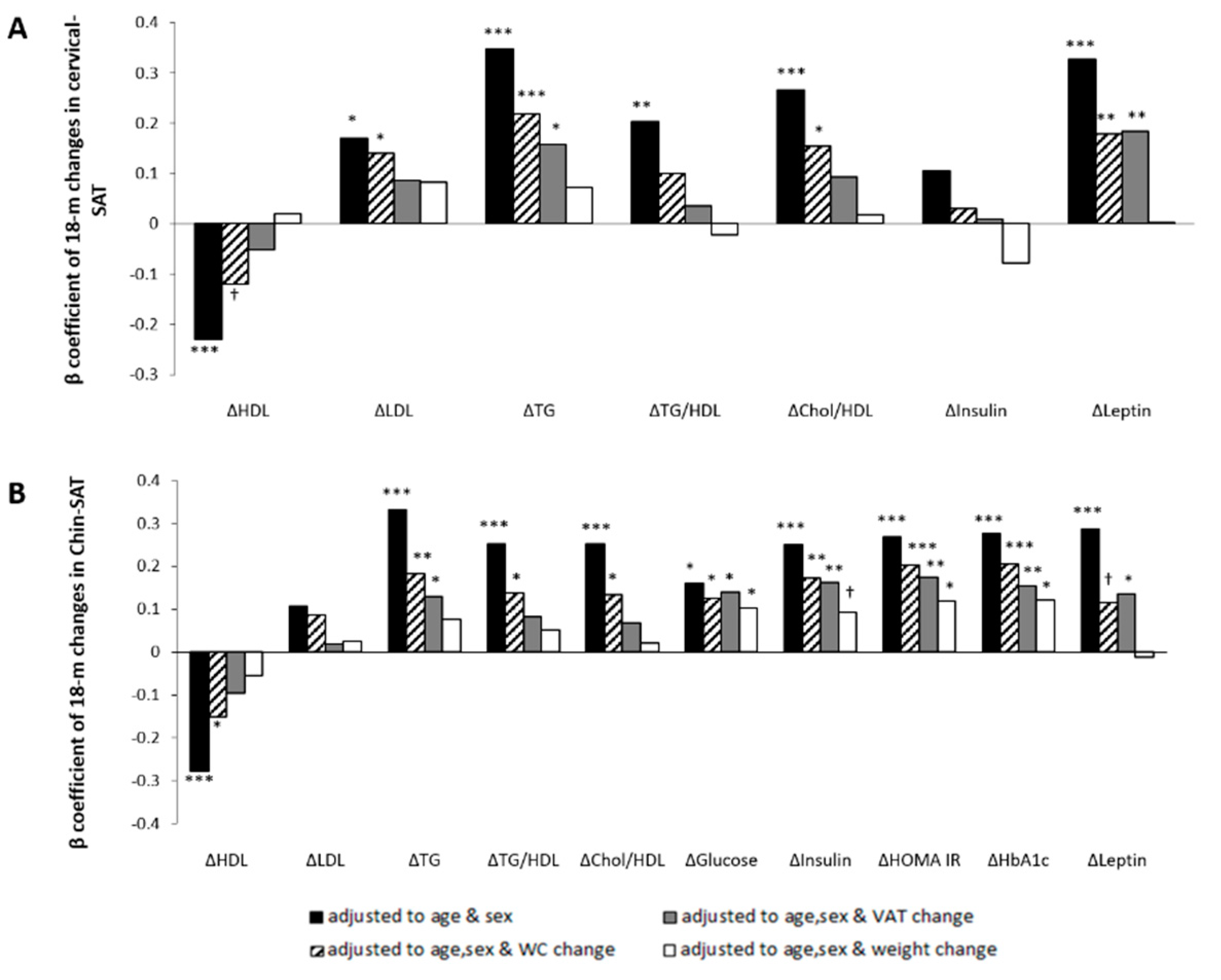
3.4. Association between 18-Month Changes in Chin-SAT with Changes in Cardiometabolic Profile
3.5. Associations between 18-Month Changes in Cervical-SAT with Changes in Cardiometabolic Profile
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Torriani, M.; Gill, C.M.; Daley, S.; Oliveira, A.L.; Azevedo, D.C.; Bredella, M.A. Compartmental neck fat accumulation and its relation to cardiovascular risk and metabolic syndrome. Am. J. Clin. Nutr. 2014, 100, 1244–1251. [Google Scholar] [CrossRef] [Green Version]
- Fox, C.S.; Massaro, J.M.; Hoffmann, U.; Pou, K.M.; Maurovich-Horvat, P.; Liu, C.-Y.; Vasan, R.S.; Murabito, J.M.; Meigs, J.B.; Cupples, L.A.; et al. Abdominal Visceral and Subcutaneous Adipose Tissue Compartments. Circulation 2007, 116, 39–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porter, S.A.; Massaro, J.M.; Hoffmann, U.; Vasan, R.S.; O’Donnel, C.J.; Fox, C.S. Abdominal Subcutaneous Adipose Tissue: A Protective Fat Depot? Diabetes Care 2009, 32, 1068–1075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLaughlin, T.; Lamendola, C.; Liu, A.; Abbasi, F. Preferential Fat Deposition in Subcutaneous Versus Visceral Depots Is Associated with Insulin Sensitivity. J. Clin. Endocrinol. Metab. 2011, 96, E1756–E1760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garg, A. Regional Adiposity and Insulin Resistance. J. Clin. Endocrinol. Metab. 2004, 89, 4206–4210. [Google Scholar] [CrossRef] [Green Version]
- Kelley, D.E.; Thaete, F.L.; Troost, F.; Huwe, T.; Goodpaster, B.H. Subdivisions of subcutaneous abdominal adipose tissue and insulin resistance. Am. J. Physiol. Metab. 2000, 278, E941–E948. [Google Scholar] [CrossRef] [PubMed]
- Golan, R.; Shelef, I.; Rudich, A.; Gepner, Y.; Shemesh, E.; Chassidim, Y.; Harman-Boehm, I.; Henkin, Y.; Schwarzfuchs, D.; Ben Avraham, S.; et al. Abdominal Superficial Subcutaneous Fat: A putative distinct protective fat subdepot in type 2 diabetes. Diabetes Care 2012, 35, 640–647. [Google Scholar] [CrossRef] [Green Version]
- Jensen, M.D. Role of Body Fat Distribution and the Metabolic Complications of Obesity. J. Clin. Endocrinol. Metab. 2008, 93, s57–s63. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.J.; Pedley, A.; Therkelsen, K.E.; Hoffmann, U.; Massaro, J.M.; Levy, D.; Long, M.T. Upper Body Subcutaneous Fat Is Associated with Cardiometabolic Risk Factors. Am. J. Med. 2017, 130, 958–966. [Google Scholar] [CrossRef] [Green Version]
- Lê, K.-A.; Mahurkar, S.; Alderete, T.L.; Hasson, R.E.; Adam, T.C.; Kim, J.S.; Beale, E.; Xie, C.; Greenberg, A.S.; Allayee, H.; et al. Subcutaneous adipose tissue macrophage infiltration is associated with hepatic and visceral fat deposition, hyperinsulinemia, and stimulation of NF-κB stress pathway. Diabetes 2011, 60, 2802–2809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, S.; Guo, Z.; Johnson, C.M.; Hensrud, D.D.; Jensen, M.D. Splanchnic lipolysis in human obesity. J. Clin. Investig. 2004, 113, 1582–1588. [Google Scholar] [CrossRef] [Green Version]
- Preis, S.R.; Massaro, J.M.; Hoffmann, U.; D’Agostino, R.B.; Levy, D.; Robins, S.J.; Meigs, J.B.; Vasan, R.S.; O’Donnell, C.J.; Fox, C.S. Neck Circumference as a Novel Measure of Cardiometabolic Risk: The Framingham Heart Study. J. Clin. Endocrinol. Metab. 2010, 95, 3701–3710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallianou, N.G.; Evangelopoulos, A.A.; Bountziouka, V.; Vogiatzakis, E.D.; Bonou, M.S.; Barbetseas, J.; Avgerinos, P.C.; Panagiotakos, D.B. Neck circumference is correlated with triglycerides and inversely related with HDL cholesterol beyond BMI and waist circumference. Diabetes Metab. Res. Rev. 2013, 29, 90–97. [Google Scholar] [CrossRef]
- Stabe, C.; Vasques, A.C.J.; Lima, M.M.O.; Tambascia, M.A.; Pareja, J.C.; Yamanaka, A.; Geloneze, B. Neck circumference as a simple tool for identifying the metabolic syndrome and insulin resistance: Results from the Brazilian Metabolic Syndrome Study. Clin. Endocrinol. 2013, 78, 874–881. [Google Scholar] [CrossRef]
- Misra, A.; Jaiswal, A.; Shakti, D.; Wasir, J.; Vikram, N.K.; Pandey, R.M.; Kondal, D.; Bhushan, B. Novel phenotypic markers and screening score for the metabolic syndrome in adult Asian Indians. Diabetes Res. Clin. Pract. 2008, 79, e1–e5. [Google Scholar] [CrossRef] [PubMed]
- Mallon, P.W.G.; Wand, H.; Law, M.; Miller, J.; Cooper, D.A.; Carr, A.; HIV Lipodystrophy Case Definition Study; Australian Lipodystrophy Prevalence Survey Investigators. Buffalo hump seen in HIV-associated lipodystrophy is associated with hyperinsulinemia but not dyslipidemia. J. Acquir. Immune Defic. Syndr. 2005, 38, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.; Meigs, J.B. Links Between Ectopic Fat and Vascular Disease in Humans. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1820–1826. [Google Scholar] [CrossRef] [Green Version]
- Rosenquist, K.J.; Therkelsen, K.E.; Massaro, J.M.; Hoffmann, U.; Fox, C.S. Development and Reproducibility of a Computed Tomography–Based Measurement for Upper Body Subcutaneous Neck Fat. J. Am. Heart Assoc. 2014, 3, e000979. [Google Scholar] [CrossRef] [Green Version]
- Thamer, C.; Machann, J.; Staiger, H.; Müssig, K.; Schwenzer, N.; Ludescher, B.; Machicao, F.; Claussen, C.; Fritsche, A.; Schick, F.; et al. Interscapular Fat Is Strongly Associated with Insulin Resistance. J. Clin. Endocrinol. Metab. 2010, 95, 4736–4742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haque, W.A.; Oral, E.A.; Dietz, K.; Bowcock, A.M.; Agarwal, A.K.; Garg, A. Risk factors for diabetes in familial partial lipodystrophy, Dunnigan variety. Diabetes Care 2003, 26, 1350–1355. [Google Scholar] [CrossRef] [Green Version]
- Alam, I.; Lewis, K.; Stephens, J.W.; Baxter, J.N. Obesity, metabolic syndrome and sleep apnoea: All pro-inflammatory states. Obes. Rev. 2007, 8, 119–127. [Google Scholar] [CrossRef]
- Gepner, Y.; Shelef, I.; Schwarzfuchs, D.; Zelicha, H.; Tene, L.; Yaskolka Meir, A.; Tsaban, G.; Cohen, N.; Bril, N.; Rein, M.; et al. Effect of Distinct Lifestyle Interventions on Mobilization of Fat Storage Pools: The CENTRAL MRI Randomized Controlled Trial. Circulation 2017, 137, 1143–1157. [Google Scholar] [CrossRef]
- Lichtenstein, A.H.; Lichtenstein, A.H.; Appel, L.J.; Brands, M.; Carnethon, M.; Daniels, S.; Franch, H.A.; Franklin, B.; Kris-Etherton, P.; Harris, W.S.; et al. Diet and Lifestyle Recommendations Revision 2006: A Scientific Statement From the American Heart Association Nutrition Committee. Circulation 2006, 114, 82–96. [Google Scholar] [CrossRef] [Green Version]
- Shai, I.; Schwarzfuchs, D.; Henkin, Y.; Shahar, D.R.; Witkow, S.; Greenberg, R.; Golan, R.; Fraser, D.; Bolotin, A.; Vardi, H.; et al. Weight loss with a low-carbohydrate, mediterranean, or low-fat diet. N. Engl. J. Med. 2008, 359, 229–241. [Google Scholar] [CrossRef] [Green Version]
- Tsaban, G.; Wolak, A.; Avni-Hassid, H.; Gepner, Y.; Shelef, I.; Henkin, Y.; Schwarzfuchs, D.; Cohen, N.; Bril, N.; Rein, M.; et al. Dynamics of intrapericardial and extrapericardial fat tissues during long-term, dietary-induced, moderate weight loss. Am. J. Clin. Nutr. 2017, 106, 984–995. [Google Scholar] [CrossRef] [Green Version]
- Gepner, Y.; Shelef, I.; Komy, O.; Cohen, N.; Schwarzfuchs, D.; Bril, N.; Rein, M.; Serfaty, D.; Kenigsbuch, S.; Zelicha, H.; et al. The beneficial effects of Mediterranean diet over low-fat diet may be mediated by decreasing hepatic fat content. J. Hepatol. 2019, 71, 379–388. [Google Scholar] [CrossRef] [Green Version]
- Mangge, H.; Almer, G.; Haj-Yahya, S.; Grandits, N.; Gasser, R.; Pilz, S.; Möller, R.; Horejsi, R. Nuchal thickness of subcutaneous adipose tissue is tightly associated with an increased LMW/total adiponectin ratio in obese juveniles. Atherosclerosis 2009, 203, 277–283. [Google Scholar] [CrossRef]
- Bhatt, S.P.; Misra, A.; Nigam, P.; Guleria, R.; Pasha, M.A.Q. Phenotype, Body Composition, and Prediction Equations (Indian Fatty Liver Index) for Non-Alcoholic Fatty Liver Disease in Non-Diabetic Asian Indians: A Case-Control Study. PLoS ONE 2015, 10, e0142260. [Google Scholar] [CrossRef] [Green Version]
- Orth, D.N. Cushing’s Syndrome. N. Engl. J. Med. 1995, 332, 791–803. [Google Scholar] [CrossRef]
- Roberge, C.; Carpentier, A.C.; Langlois, M.-F.; Baillargeon, J.-P.; Ardilouze, J.-L.; Maheux, P.; Gallo-Payet, N. Adrenocortical dysregulation as a major player in insulin resistance and onset of obesity. Am. J. Physiol. Metab. 2007, 293, E1465–E1478. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.; Misra, A.; Garg, A. Lipodystrophy in Human Immunodeficiency Virus-Infected Patients. J. Clin. Endocrinol. Metab. 2002, 11, 4845–4856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sierra-Johnson, J.; Johnson, B.D. Facial fat and its relationship to abdominal fat: A marker for insulin resistance? Med. Hypotheses 2004, 63, 783–786. [Google Scholar] [CrossRef] [PubMed]
- Cho, N.H.; Oh, T.J.; Kim, K.M.; Choi, S.H.; Lee, J.H.; Park, K.S.; Jang, H.C.; Kim, J.Y.; Lee, H.K.; Lim, S. Neck Circumference and Incidence of Diabetes Mellitus over 10 Years in the Korean Genome and Epidemiology Study (KoGES). Sci. Rep. 2016, 5, 18565. [Google Scholar] [CrossRef] [Green Version]
- Cizza, G.; de Jonge, L.; Piaggi, P.; Mattingly, M.; Zhao, X.; Lucassen, E.; Rother, K.I.; Sumner, A.E.; Csako, G.; NIDDK Sleep Extension Study. Neck Circumference Is a Predictor of Metabolic Syndrome and Obstructive Sleep Apnea in Short-Sleeping Obese Men and Women. Metab. Syndr. Relat. Disord. 2014, 12, 231–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nedergaard, J.; Cannon, B. How brown is brown fat? It depends where you look. Nat. Med. 2013, 19, 540–541. [Google Scholar] [CrossRef]
- Fenzl, A.; Kiefer, F.W. Brown adipose tissue and thermogenesis. Horm. Mol. Biol. Clin. Investig. 2014, 19, 25–37. [Google Scholar] [CrossRef]
- Bartelt, A.; Heeren, J. Adipose tissue browning and metabolic health. Nat. Rev. Endocrinol. 2014, 10, 24–36. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Low Tertile (n = 91) | Intermediate Tertile (n = 90) | Top Tertile (n = 92) | p-of-Trend | Entire (n = 273) | |
|---|---|---|---|---|---|
| BMI (Kg/m2) | |||||
| Men (n = 245) | 24.04–29.23 | 29.24–31.93 | 31.94–43.47 | ||
| Women (n = 28) | 24.06–27.02 | 27.03–31.72 | 31.73–42.28 | ||
| Chin-SAT (cm2) | 15.02 ± 2.96 | 17.58 ± 3.70 | 20.65 ± 4.95 | <0.001 | 17.75 ± 4.56 |
| Cervical-SAT (cm2) | 25.07 ± 7.18 | 32.83 ± 10.29 | 42.99 ± 12.63 | <0.001 | 33.45 ± 12.54 |
| Age (year) | 46.80 ± 9.82 | 48.82 ± 9.11 | 47.67 ± 8.88 | 0.492 | 47.76 ± 9.28 |
| Waist circumference (cm) | |||||
| Men | 100.3 ± 5.3 | 106.4 ± 4.8 | 116.4 ± 7.3 | <0.001 | 107.7 ± 8.9 |
| Women | 92.6 ± 6.4 | 96.2 ± 6.0 | 105.2 ± 12.5 | 0.004 | 98.3 ± 10.2 |
| Diastolic Blood Pressure (mmHg) | 78.42 ± 9.86 | 80.16 ± 9.79 | 83.45 ± 10.80 | 0.001 | 80.69 ± 10.34 |
| Systolic Blood Pressure (mmHg) | 122.13 ± 15.36 | 124.41 ± 14.71 | 129.11 ± 17.52 | 0.002 | 125.24 ± 16.13 |
| Blood biomarkers | |||||
| Fasting Plasma Glucose (mg/dL) | 105.71 ± 15.64 | 105.19 ± 16.31 | 110.68 ± 24.43 | 0.271 | 107.21 ± 19.34 |
| Serum Insulin (μU/mL) | 13.67 ± 7.25 | 16.13 ± 9.28 | 21.23 ± 12.19 | <0.001 | 17.05 ± 10.27 |
| HbA1c (%) | 5.47 ± 0.48 | 5.45 ± 0.40 | 5.70 ± 0.61 | 0.006 | 5.54 ± 0.52 |
| HOMA-IR | 3.62 ± 2.16 | 4.21 ± 2.75 | 5.93 ± 3.92 | <0.001 | 4.60 ± 3.18 |
| Serum LDL-cholesterol (mg/dL) | 120.04 ± 32.37 | 123.47 ± 30.39 | 121.82 ± 31.41 | 0.917 | 121.78 ± 31.32 |
| Serum HDL-cholesterol (mg/dL) | |||||
| Men | 42.12 ± 9.06 | 40.74 ± 9.26 | 41.98 ± 11.67 | 0.381 | 41.62 ± 10.04 |
| Women | 55.73 ± 16.23 | 61.18 ± 23.01 | 51.74 ± 6.95 | 0.933 | 56.05 ± 16.33 |
| Serum triglycerides (mg/dL) | 70.62 ± 41.58 | 73.44 ± 40.36 | 73.39 ± 42.35 | 0.723 | 72.48 ± 41.31 |
| Abdominal fat depots | |||||
| Superficial-SAT (cm2) | 106.1 ± 35.0 | 132.5 ± 47.0 | 186.0 ± 66.5 | <0.001 | 141.7 ± 61.0 |
| Deep-SAT (cm2) | 161.2 ± 45.5 | 209.0 ± 48.3 | 278.3 ± 71.7 | <0.001 | 216.4 ± 74.2 |
| VAT (cm2) | 141.5 ± 48.5 | 175.7 ± 60.5 | 209.1 ± 71.5 | <0.001 | 175.6 ± 66.8 |
| LF Diet | MED/LC Diet | p Value LF: MED/LC 1 | p Value LF ± PA: MED/ LC ± PA 2 | Entire Change | |||
|---|---|---|---|---|---|---|---|
| LF PA+ | LF PA− | MED/LC PA+ | MED/LC PA− | ||||
| 6 months | |||||||
| Chin-SAT | −1.0 cm2 ± 1.8 (−5.1% ± 9.7) *** | −1.1 cm2 ± 2.0 (−5.6 ± 11.5) *** | 0.574 (0.603) | NA | −1.1 cm2 ± 1.9 (−5.3% ± 10.7) *** | ||
| Cervical-SAT | −5.3 cm2 ± 6.4 (−13.8% ± 15.1) *** | −5.1 cm2 ± 7.8 (−12.3% ± 18.4) *** | 0.752 (0.603) | NA | −5.2 cm2 ± 7.2 (−13.1% ± 16.9) *** | ||
| 18 months | |||||||
| Chin-SAT | −0.1 cm2 ± 2.3 | 0.5 cm2 ± 2.1 | −0.2 cm2 ± 2.3 | −0.1 cm2 ± 2.4 | 0.428 | 0.390 | 0.0 cm2 ± 2.3 (0.8% ± 12.6) |
| (0.2% ± 12.2) | (2.9% ± 12.1) | (−0.1% ± 12.2) | (0.5% ± 14.5) | (0.477) | (0.623) | ||
| Cervical-SAT | −2.5 cm2 ± 7.3 | −3.1 cm2 ± 8.5 | −4.0 cm2 ± 6.6 | −2.8 cm2 ± 7.1 | 0.398 | 0.482 | −3.1 cm2 ± 7.3 |
| (−6.6% ± 20.0) ** | (−7.0% ± 20.0) ** | (−10.2% ± 17.0) *** | (−6.8% ± 18.2) ** | (0.437) | (0.706) | (−7.8% ± 18.7) *** | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsaban, G.; Bilitzky-Kopit, A.; Yaskolka Meir, A.; Zelicha, H.; Gepner, Y.; Shelef, I.; Orr, O.; Chassidim, Y.; Sarusi, B.; Ceglarek, U.; et al. The Effect of Weight-Loss Interventions on Cervical and Chin Subcutaneous Fat Depots; the CENTRAL Randomized Controlled Trial. Nutrients 2021, 13, 3827. https://doi.org/10.3390/nu13113827
Tsaban G, Bilitzky-Kopit A, Yaskolka Meir A, Zelicha H, Gepner Y, Shelef I, Orr O, Chassidim Y, Sarusi B, Ceglarek U, et al. The Effect of Weight-Loss Interventions on Cervical and Chin Subcutaneous Fat Depots; the CENTRAL Randomized Controlled Trial. Nutrients. 2021; 13(11):3827. https://doi.org/10.3390/nu13113827
Chicago/Turabian StyleTsaban, Gal, Avital Bilitzky-Kopit, Anat Yaskolka Meir, Hila Zelicha, Yftach Gepner, Ilan Shelef, Omri Orr, Yoash Chassidim, Benjamin Sarusi, Uta Ceglarek, and et al. 2021. "The Effect of Weight-Loss Interventions on Cervical and Chin Subcutaneous Fat Depots; the CENTRAL Randomized Controlled Trial" Nutrients 13, no. 11: 3827. https://doi.org/10.3390/nu13113827
APA StyleTsaban, G., Bilitzky-Kopit, A., Yaskolka Meir, A., Zelicha, H., Gepner, Y., Shelef, I., Orr, O., Chassidim, Y., Sarusi, B., Ceglarek, U., Stumvoll, M., Blüher, M., Stampfer, M. J., Shai, I., & Schwarzfuchs, D. (2021). The Effect of Weight-Loss Interventions on Cervical and Chin Subcutaneous Fat Depots; the CENTRAL Randomized Controlled Trial. Nutrients, 13(11), 3827. https://doi.org/10.3390/nu13113827