
Dietary Protein Intake Dynamics in Elderly Chinese from 1991 to 2018

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Dietary Intake Measurement
2.3. Dietary Estimation and Food Sources of Protein
2.4. Measurement of Sociodemographic Characteristics
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Trends in Dietary Protein Intake Distribution
3.3. Assessment of Dietary Protein Intake Level in the Study Participants
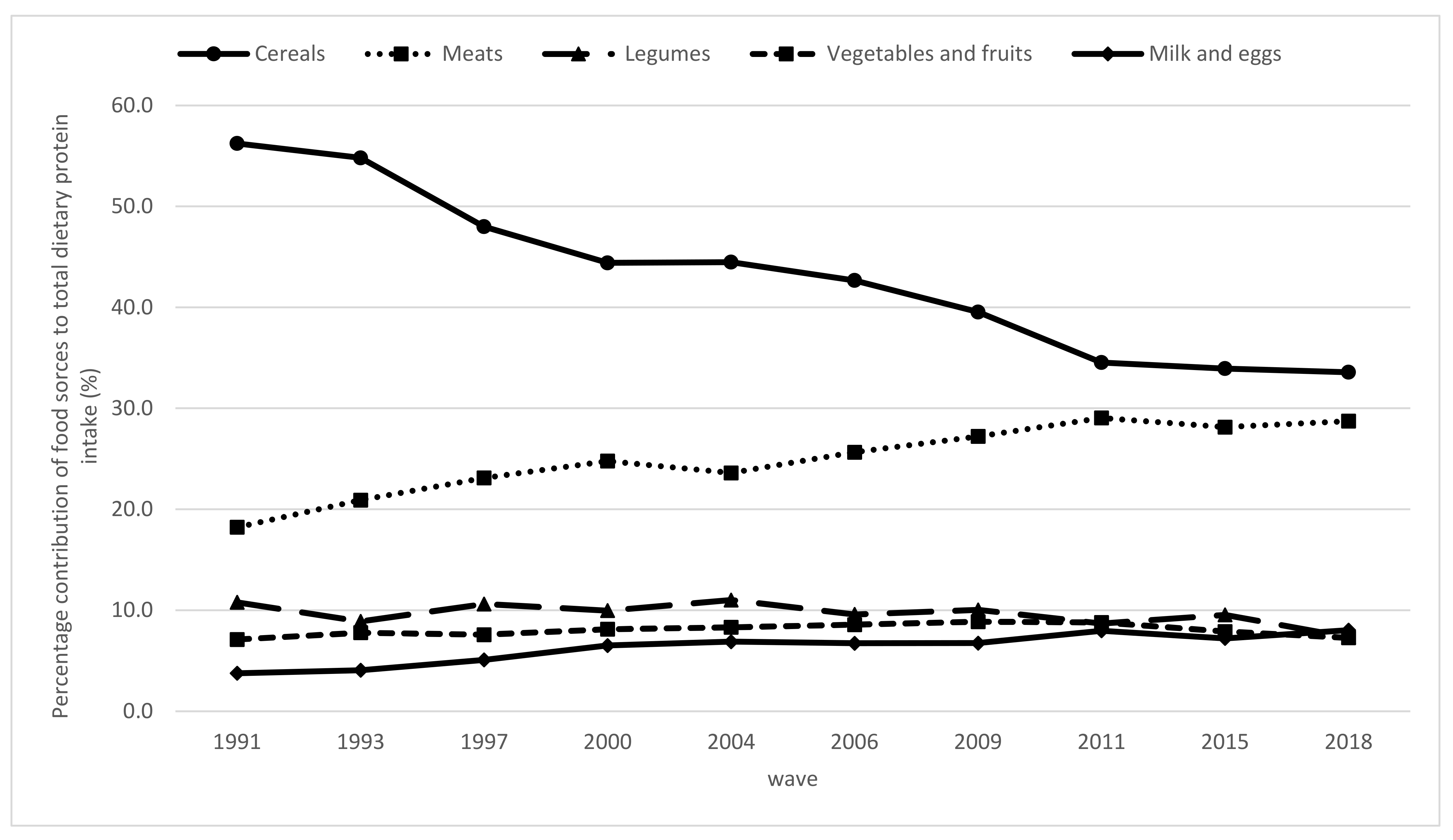
3.4. Contribution Percentages of Food Sources to the Total Dietary Protein Intake
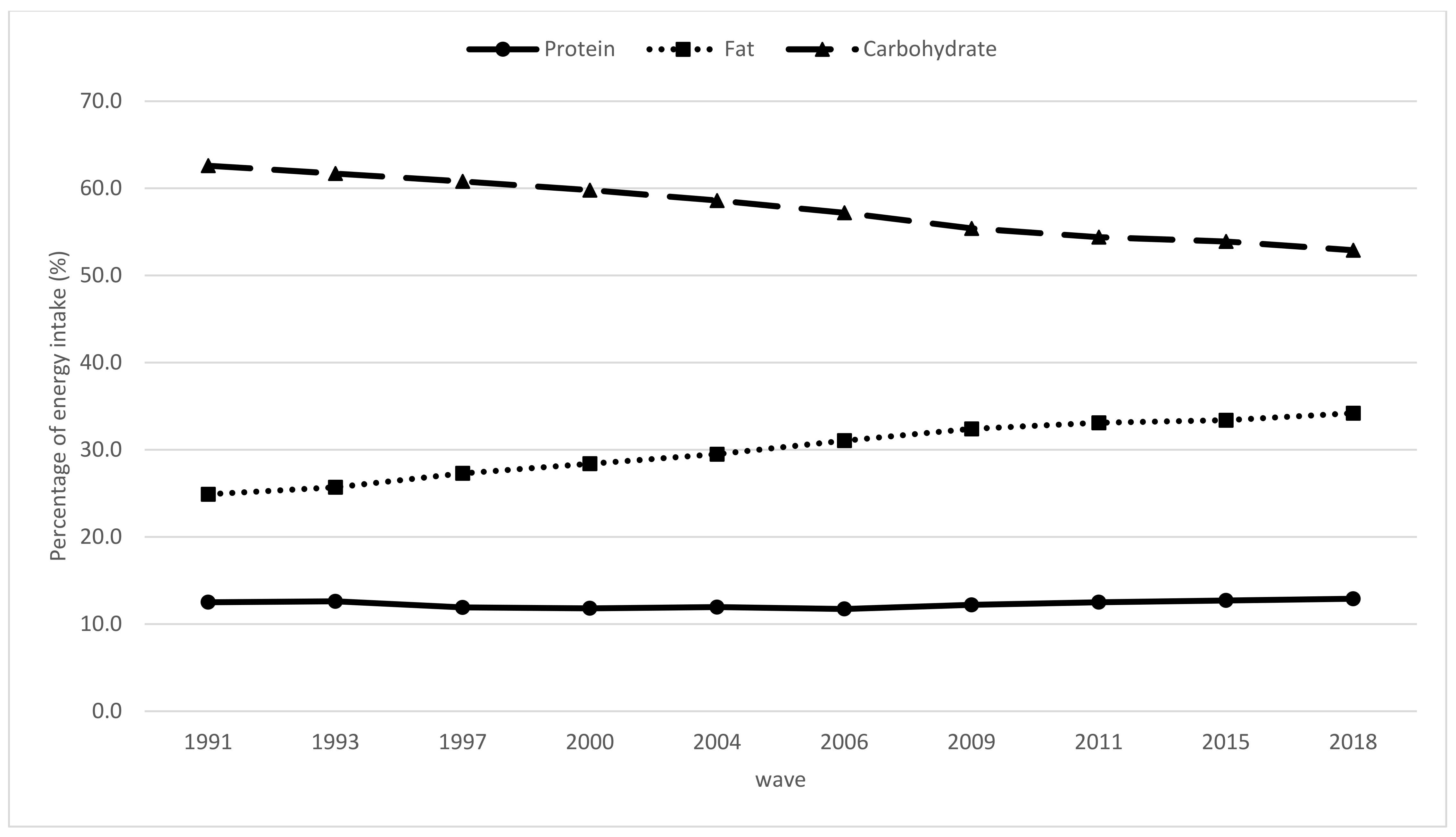
3.5. Energy from Carbohydrates, Proteins, and Fats
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Decade of Healthy Ageing: Baseline Report. Summary; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. World Report on Ageing and Health 2015; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Phillips, D.R.; Feng, Z. Challenges for the Aging Family in the People’s Republic of China. Can. J. Aging 2015, 34, 290–304. [Google Scholar] [CrossRef] [Green Version]
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznariç, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leidy, H.J.; Clifton, P.M.; Astrup, A.; Wycherley, T.P.; Westerterp-Plantenga, M.S.; Luscombe-Marsh, N.D.; Woods, S.C.; Mattes, R.D. The role of protein in weight loss and maintenance. Am. J. Clin. Nutr. 2015, 101, 1320–1329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.E.; O’Connor, L.E.; Sands, L.P.; Slebodnik, M.B.; Campbell, W.W. Effects of dietary protein intake on body composition changes after weight loss in older adults: A systematic review and meta-analysis. Nutr. Rev. 2016, 74, 210–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Draganidis, D.; Karagounis, L.G.; Athanailidis, I.; Chatzinikolaou, A.; Jamurtas, A.Z.; Fatouros, I.G. Inflammaging and Skeletal Muscle: Can Protein Intake Make a Difference? J. Nutr. 2016, 146, 1940–1952. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, J.; Ellison, R.C.; Singer, M.R.; Bradlee, M.L.; Kalesan, B.; Holick, M.F.; Moore, L.L. Dietary Protein and Preservation of Physical Functioning Among Middle-Aged and Older Adults in the Framingham Offspring Study. Am. J. Epidemiol. 2018, 187, 1411–1419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jäger, R.; Kerksick, C.M.; Campbell, B.I.; Cribb, P.J.; Wells, S.D.; Skwiat, T.M.; Purpura, M.; Ziegenfuss, T.N.; Ferrando, A.A.; Arent, S.M.; et al. International Society of Sports Nutrition Position Stand: Protein and exercise. J. Int. Soc. Sports Nutr. 2017, 14, 20. [Google Scholar] [CrossRef] [Green Version]
- Zhao, J.; Su, C.; Wang, H.; Wang, Z.; Wang, Y.; Zhang, B. Secular Trends in Energy and Macronutrient Intakes and Distribution among Adult Females (1991–2015): Results from the China Health and Nutrition Survey. Nutrients 2018, 10, 115. [Google Scholar] [CrossRef] [Green Version]
- Su, C.; Zhao, J.; Wu, Y.; Wang, H.; Wang, Z.; Wang, Y.; Zhang, B. Temporal Trends in Dietary Macronutrient Intakes among Adults in Rural China from 1991 to 2011: Findings from the CHNS. Nutrients 2017, 9, 227. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.; Sayer, A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Xu, X.; Byles, J.E.; Shi, Z.; Hall, J.J. Evaluation of older Chinese people’s macronutrient intake status: Results from the China Health and Nutrition Survey. Br. J. Nutr. 2015, 113, 159–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landi, F.; Calvani, R.; Tosato, M.; Martone, A.M.; Ortolani, E.; Savera, G.; D’Angelo, E.; Sisto, A.; Marzetti, E. Protein Intake and Muscle Health in Old Age: From Biological Plausibility to Clinical Evidence. Nutrients 2016, 8, 295. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wang, Z.; Du, W.; Huang, F.; Jiang, H.; Bai, J.; Zhang, X.; Zhang, B.; Wang, H. Twenty-Five-Year Trends in Dietary Patterns among Chinese Adults from 1991 to 2015. Nutrients 2021, 13, 1327. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Li, Y.; Yang, X.; Hemler, E.C.; Fang, Y.; Zhao, L.; Zhang, J.; Yang, Z.; Wang, Z.; He, L.; et al. The dietary transition and its association with cardiometabolic mortality among Chinese adults, 1982–2012: A cross-sectional population-based study. Lancet Diabetes Endocrinol. 2019, 7, 540–548. [Google Scholar] [CrossRef]
- Popkin, B.M.; Du, S.; Zhai, F.; Zhang, B. Cohort Profile: The China Health and Nutrition Survey--monitoring and understanding socio-economic and health change in China, 1989–2011. Int. J. Epidemiol. 2010, 39, 1435–1440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhai, F.Y.; Du, S.F.; Wang, Z.H.; Zhang, J.G.; Du, W.W.; Popkin, B.M. Dynamics of the Chinese diet and the role of urbanicity, 1991–2011. Obes. Rev. 2014, 15 (Suppl. 1), 16–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shan, Z.; Rehm, C.D.; Rogers, G.; Ruan, M.; Wang, D.D.; Hu, F.B.; Mozaffarian, D.; Zhang, F.F.; Bhupathiraju, S.N. Trends in Dietary Carbohydrate, Protein, and Fat Intake and Diet Quality Among US Adults, 1999–2016. JAMA 2019, 322, 1178–1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lonnie, M.; Hooker, E.; Brunstrom, J.M.; Corfe, B.M.; Green, M.A.; Watson, A.W.; Williams, E.A.; Stevenson, E.J.; Penson, S.; Johnstone, A.M. Protein for Life: Review of Optimal Protein Intake, Sustainable Dietary Sources and the Effect on Appetite in Ageing Adults. Nutrients 2018, 10, 360. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, C.L.P.; Dionne, I.J.; Prado, C.M. Are Canadian protein and physical activity guidelines optimal for sarcopenia prevention in older adults? Appl. Physiol. Nutr. Metab. 2018, 43, 1215–1223. [Google Scholar] [CrossRef]
- Baum, J.I.; Kim, I.-Y.; Wolfe, R.R. Protein Consumption and the Elderly: What Is the Optimal Level of Intake? Nutrients 2016, 8, 359. [Google Scholar] [CrossRef] [Green Version]
- Park, H.A. Adequacy of Protein Intake among Korean Elderly: An Analysis of the 2013–2014 Korea National Health and Nutrition Examination Survey Data. Korean J. Fam. Med. 2018, 39, 130–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berryman, C.E.; Lieberman, H.R.; Fulgoni, V.L., III; Pasiakos, S.M. Protein intake trends and conformity with the Dietary Reference Intakes in the United States: Analysis of the National Health and Nutrition Examination Survey, 2001–2014. Am. J. Clin. Nutr. 2018, 108, 405–413. [Google Scholar] [CrossRef]
- Jiang, L.; Shen, J.; Zhao, Y.; Li, J.; Liu, S.; Liu, Y.; Wang, H.; Su, C.; Zhuang, X.; Chen, N.; et al. Trans fatty acid intake among Chinese population: A longitudinal study from 1991 to 2011. Lipids Health Dis. 2020, 19, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Song, P.K.; Zhao, L.Y.; Sun, Y.; Yu, K.; Yin, J.; Pang, S.J.; Liu, Z.; Man, Q.Q.; He, L.; et al. Malnutrition in Relation with Dietary, Geographical, and Socioeconomic Factors among Older Chinese. Biomed. Environ. Sci. 2021, 34, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.H.; Zhai, F.Y.; Wang, H.J.; Zhang, J.G.; Du, W.W.; Su, C.; Zhang, J.; Jiang, H.R.; Zhang, B. Secular trends in meat and seafood consumption patterns among Chinese adults, 1991–2011. Eur. J. Clin. Nutr. 2015, 69, 227–233. [Google Scholar] [CrossRef]
- Sandhu, H.S.; Arora, A.; Sarker, S.I.; Shah, B.; Sivendra, A.; Winsor, E.S.; Luthra, A. Pandemic prevention and unsustainable animal-based consumption. Bull. World Health Organ. 2021, 99, 603–605. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Wave | 1991 | 1993 | 1997 | 2000 | 2004 | 2006 | 2009 | 2011 | 2015 | 2018 | p Value b |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample size (n) | 1334 | 1372 | 1588 | 1893 | 2144 | 2359 | 2662 | 3655 | 4994 | 5870 | |
| Age group (years) | |||||||||||
| 60–69 | 855 (64.1) | 890 (64.9) | 999 (62.9) | 1169 (61.8) | 1245 (58.1) | 1344 (57.0) | 1523 (57.2) | 2208 (60.4) | 3180 (63.7) | 3655 (62.3) | <0.0001 |
| 70– | 479 (35.9) | 482 (35.1) | 589 (37.1) | 724 (38.2) | 899 (41.9) | 1015 (43.0) | 1139 (42.8) | 1447 (39.6) | 1814 (36.3) | 2215 (37.7) | |
| Gender | |||||||||||
| Male | 633 (47.5) | 646 (47.1) | 732 (46.1) | 883 (46.6) | 1012 (47.2) | 1100 (46.6) | 1252 (47.0) | 1733 (47.4) | 2355 (47.2) | 2748 (46.8) | 0.99 |
| Female | 701 (52.5) | 726 (52.9) | 856 (53.9) | 1010 (53.4) | 1132 (52.8) | 1259 (53.4) | 1410 (53.0) | 1922 (52.6) | 2639 (52.8) | 3122 (53.2) | |
| Education level | |||||||||||
| Primary/illiterate | 1176 (90.6) | 1142 (88) | 1235 (85.2) | 1369 (79.7) | 1604 (75.4) | 1709 (73.2) | 1905 (72.1) | 2289 (62.9) | 2798 (56.3) | 2842 (49.9) | <0.0001 |
| Middle school and above | 122 (9.4) | 155 (12) | 215 (14.8) | 348 (20.3) | 524 (24.6) | 625 (26.8) | 738 (27.9) | 1350 (37.1) | 2173 (43.7) | 2850 (50.1) | |
| Yearly income level | |||||||||||
| Low | 441 (33.3) | 453 (33.3) | 520 (33.3) | 610 (33.3) | 709 (33.4) | 773 (33.3) | 872 (33.3) | 1202 (33.3) | 1625 (33.3) | 1723 (33.4) | 1.00 |
| Middle | 443 (33.4) | 454 (33.4) | 520 (33.3) | 611 (33.4) | 707 (33.3) | 776 (33.4) | 872 (33.3) | 1202 (33.3) | 1624 (33.3) | 1719 (33.3) | |
| High | 442 (33.3) | 453 (33.3) | 520 (33.3) | 610 (33.3) | 709 (33.4) | 773 (33.3) | 872 (33.3) | 1202 (33.3) | 1625 (33.3) | 1722 (33.3) | |
| Residence area | |||||||||||
| City | 366 (27.4) | 343 (25) | 414 (26.1) | 461 (24.4) | 548 (25.6) | 605 (25.6) | 652 (24.5) | 1253 (34.3) | 1895 (37.9) | 2377 (40.5) | <0.0001 |
| Suburb | 453 (34) | 483 (35.2) | 589 (37.1) | 620 (32.8) | 649 (30.3) | 717 (30.4) | 835 (31.4) | 915 (25) | 1014 (20.3) | 1165 (19.8) | |
| Town | 420 (31.5) | 431 (31.4) | 495 (31.2) | 530 (28) | 583 (27.2) | 631 (26.7) | 710 (26.7) | 982 (26.9) | 1516 (30.4) | 1677 (28.6) | |
| Village | 95 (7.1) | 115 (8.4) | 90 (5.7) | 282 (14.9) | 364 (17) | 406 (17.2) | 465 (17.5) | 505 (13.8) | 569 (11.4) | 651 (11.1) |
| Wave | 1991 | 1993 | 1997 | 2000 | 2004 | 2006 | 2009 | 2011 | 2015 | 2018 | Per-Year Change (β ± SE) | p Value for Linear Trend b |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample size (n) | 1334 | 1372 | 1588 | 1893 | 2144 | 2359 | 2662 | 3655 | 4994 | 5870 | ||
| Age group (years) | ||||||||||||
| 60–69 | 66.1 (30.6) | 64.3 (28.0) | 63.2 (29.6) | 59.8 (28.0) | 62.6 (31.8) | 61.6 (30.7) | 61.1 (28.9) | 56.0 (28.0) | 58.8 (31.5) | 59.8 (31.0) | −0.033 ± 0.0002 | <0.0001 |
| 70– | 57.4 (30.3) | 57.0 (27.2) | 54.1 (28.6) | 54.2 (27.2) | 54.6 (31.0) | 53.1 (30.2) | 51.9 (25.2) | 50.3 (26.6) | 52.2 (30.7) | 54.6 (31.2) | −0.029 ± 0.0001 | <0.0001 |
| p value for interaction c | 0.03 | |||||||||||
| Gender | ||||||||||||
| Male | 68.5 (33.2) | 67.0 (29.8) | 65.4 (30.7) | 62.9 (30.9) | 65.0 (31.9) | 62.7 (32.6) | 63.3 (30.6) | 58.6 (28.3) | 60.9 (32.1) | 62.8 (33.1) | −0.034 ± 0.0002 | <0.0001 |
| Female | 58.3 (28.5) | 57.9 (25.2) | 56.1 (27.2) | 54.0 (24.8) | 54.9 (29.3) | 54.2 (29.8) | 52.8 (24.3) | 49.7 (24.2) | 51.8 (29.0) | 53.9 (29.3) | −0.030 ± 0.0002 | <0.0001 |
| p value for interaction c | 0.88 | |||||||||||
| Education level | ||||||||||||
| Primary/illiterate | 62.5 (29.9) | 61.3 (28.1) | 58.7 (28.4) | 55.0 (26.3) | 57.6 (30.0) | 55.1 (30.9) | 54.8 (25.9) | 50.5 (25.6) | 51.6 (28.3) | 53.3 (29.9) | −0.030 ± 0.0000 | <0.0001 |
| Middle school and above | 72.3 (35.9) | 71.1 (33.9) | 71.1 (28.9) | 68.2 (27.0) | 68.1 (37.6) | 64.7 (31.3) | 63.9 (30.7) | 59.8 (28.0) | 62.6 (32.0) | 62.8 (31.9) | −0.036 ± 0.0002 | <0.0001 |
| p value for interaction c | 0.04 | |||||||||||
| Yearly income level | ||||||||||||
| Low | 58.2 (30.7) | 56.7 (27.5) | 58.3 (31.5) | 54.1 (27.8) | 56.0 (29.8) | 52.5 (32.4) | 52.2 (25.7) | 49.2 (25.4) | 50.3 (27.9) | 51.5 (29.4) | −0.029 ± 0.0001 | <0.0001 |
| Middle | 60.5 (29.6) | 61.4 (27.8) | 58.6 (27.1) | 55.8 (27.9) | 59.0 (30.6) | 57.5 (29.6) | 58.7 (26.6) | 53.7 (24.8) | 56.3 (29.5) | 57.5 (30.7) | −0.032 ± 0.0002 | <0.0001 |
| High | 71.1 (30.5) | 66.6 (28.5) | 63.4 (28.9) | 62.0 (28.3) | 63.6 (32.3) | 63.2 (31.5) | 60.4 (29.7) | 59.5 (29.4) | 64.1 (33.0) | 63.5 (31.6) | −0.035 ± 0.0002 | <0.0001 |
| p value for interaction c | 0.44 | |||||||||||
| Area | ||||||||||||
| City | 68.3 (31.5) | 62.7 (25.7) | 65.1 (28.8) | 63.2 (31.3) | 64.5 (34.2) | 66.9 (31.1) | 62.5 (33.3) | 59.5 (31.1) | 63.1 (32.9) | 63.4 (33.5) | −0.035 ± 0.0002 | <0.0001 |
| Suburb | 62.9 (31.5) | 60.7 (30.3) | 57.3 (30.1) | 57.5 (26.9) | 58.8 (32.1) | 57.8 (31.6) | 56.1 (25.3) | 52.6 (25.9) | 54.8 (28.8) | 59.1 (29.5) | −0.031 ± 0.0001 | <0.0001 |
| Town | 58.2 (25.2) | 58.8 (27.3) | 60.0 (28.0) | 55.0 (24.6) | 56.5 (27.0) | 50.0 (23.9) | 53.2 (26.7) | 49.0 (22.9) | 51.9 (28.0) | 51.5 (29.0) | −0.029 ± 0.0001 | <0.0001 |
| Village | 82.5 (34.2) | 72.8 (40.0) | 55.6 (24.8) | 56.8 (27.3) | 56.5 (31.0) | 62.1 (36.1) | 57.4 (24.3) | 53.3 (26.7) | 51.5 (28.8) | 52.4 (29.9) | −0.033 ± 0.0003 | <0.0001 |
| p value for interaction c | <0.0001 | |||||||||||
| Total | 63.3 (30.7) | 61.5 (28.7) | 60.0 (29.1) | 57.5 (27.3) | 59.5 (31.1) | 57.8 (31.9) | 57.2 (27.2) | 53.7 (27.3) | 56.5 (31.1) | 57.8 (31.2) | −0.032 ± 0.0001 | <0.0001 |
| Wave | 1991 | 1993 | 1997 | 2000 | 2004 | 2006 | 2009 | 2011 | 2015 | 2018 | Per-Year Change (β ± SE) | p Value for Linear Trend b |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total subjects | 475 (35.6) | 478 (34.8) | 633 (39.9) | 810 (42.8) | 879 (41.0) | 1025 (43.5) | 1176 (44.2) | 1894 (51.8) | 2362 (47.3) | 2581 (44.0) | 0.024 ± 0.0017 | <0.0001 |
| Age group (years) | ||||||||||||
| 60–69 | 258 (30.2) | 269 (30.2) | 330 (33.0) | 450 (38.5) | 439 (35.3) | 498 (37.1) | 548 (36.0) | 1028 (46.6) | 1378 (43.3) | 1473 (40.3) | 0.027 ± 0.0022 | <0.0001 |
| 70– | 217 (45.3) | 209 (43.4) | 303 (51.4) | 360 (49.7) | 440 (48.9) | 527 (51.9) | 628 (55.1) | 866 (59.8) | 984 (54.2) | 1108 (50.0) | 0.021 ± 0.0027 | <0.0001 |
| p value for interaction c | 0.0033 | |||||||||||
| Gender | ||||||||||||
| Male | 225 (35.5) | 246 (38.1) | 301 (41.1) | 395 (44.7) | 428 (42.3) | 500 (45.5) | 561 (44.8) | 922 (53.2) | 1131 (48.0) | 1243 (45.2) | 0.022 ± 0.0024 | <0.0001 |
| Female | 250 (35.7) | 232 (32.0) | 332 (38.8) | 415 (41.1) | 451 (39.8) | 525 (41.7) | 615 (43.6) | 972 (50.6) | 1231 (46.6) | 1338 (42.9) | 0.027 ± 0.0023 | <0.0001 |
| p value for interaction c | 0.4367 | |||||||||||
| Education level | ||||||||||||
| Primary/illiterate | 423 (36.0) | 393 (34.4) | 511 (41.4) | 640 (46.7) | 689 (43.0) | 790 (46.2) | 903 (47.4) | 1311 (57.3) | 1510 (54.0) | 1431 (50.4) | 0.025 ± 0.0019 | <0.0001 |
| Middle school and above | 33 (27.0) | 48 (31.0) | 54 (25.1) | 91 (26.1) | 182 (34.7) | 225 (36.0) | 264 (35.8) | 574 (42.5) | 844 (38.8) | 1047 (36.7) | 0.024 ± 0.0036 | <0.0001 |
| p value for interaction c | 0.0054 | |||||||||||
| Yearly income level | ||||||||||||
| Low | 196 (44.4) | 196 (43.3) | 229 (44.0) | 307 (50.3) | 333 (47.0) | 400 (51.7) | 469 (53.8) | 741 (61.6) | 945 (58.2) | 955 (55.4) | 0.026 ± 0.0028 | <0.0001 |
| Middle | 173 (39.1) | 156 (34.4) | 227 (43.7) | 279 (45.7) | 292 (41.3) | 339 (43.7) | 352 (40.4) | 633 (52.7) | 791 (48.7) | 761 (44.3) | 0.019 ± 0.0029 | <0.0001 |
| High | 103 (23.3) | 122 (26.9) | 168 (32.3) | 197 (32.3) | 244 (34.4) | 268 (34.7) | 325 (37.3) | 493 (41.0) | 563 (34.6) | 580 (33.7) | 0.029 ± 0.0031 | <0.0001 |
| p value for interaction c | 0.9920 | |||||||||||
| Area | ||||||||||||
| City | 105 (28.7) | 97 (28.3) | 126 (30.4) | 148 (32.1) | 180 (32.8) | 173 (28.6) | 222 (34.0) | 513 (40.9) | 682 (36.0) | 814 (34.2) | 0.021 ± 0.0032 | <0.0001 |
| Suburb | 172 (38.0) | 193 (40.0) | 263 (44.7) | 268 (43.2) | 264 (40.7) | 323 (45.0) | 381 (45.6) | 496 (54.2) | 505 (49.8) | 477 (40.9) | 0.014 ± 0.0030 | <0.0001 |
| Town | 184 (43.8) | 159 (36.9) | 200 (40.4) | 258 (48.7) | 261 (44.8) | 367 (58.2) | 368 (51.8) | 622 (63.3) | 852 (56.2) | 932 (55.6) | 0.029 ± 0.0030 | <0.0001 |
| Village | 14 (14.7) | 29 (25.2) | 44 (48.9) | 136 (48.2) | 174 (47.8) | 162 (39.9) | 205 (44.1) | 263 (52.1) | 323 (56.8) | 358 (55.0) | 0.051 ± 0.0055 | <0.0001 |
| p value for interaction c | <0.0001 |
| Wave | 1991 | 1993 | 1997 | 2000 | 2004 | 2006 | 2009 | 2011 | 2015 | 2018 | Per-Year Change (β ± SE) | p Value for Linear Trend b |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total subjects | 756 (56.7) | 750 (54.7) | 815 (51.3) | 894 (47.2) | 1068 (49.8) | 1121 (47.5) | 1221 (45.9) | 1411 (38.6) | 2203 (44.1) | 2775 (47.3) | −0.023 ± 0.0017 | <0.0001 |
| Age group (years) | ||||||||||||
| 60–69 | 536 (62.7) | 530 (59.6) | 573 (57.4) | 603 (51.6) | 685 (55.0) | 715 (53.2) | 809 (53.1) | 952 (43.1) | 1524 (47.9) | 1849 (50.6) | −0.025 ± 0.0021 | <0.0001 |
| 70– | 220 (45.9) | 220 (45.6) | 242 (41.1) | 291 (40.2) | 383 (42.6) | 406 (40.0) | 412 (36.2) | 459 (31.7) | 679 (37.4) | 926 (41.8) | −0.021 ± 0.0027 | <0.0001 |
| p value for interaction c | 0.0277 | |||||||||||
| Gender | ||||||||||||
| Male | 362 (57.2) | 343 (53.1) | 374 (51.1) | 411 (46.5) | 505 (49.9) | 515 (46.8) | 591 (47.2) | 664 (38.3) | 1024 (43.5) | 1274 (46.4) | −0.023 ± 0.0024 | <0.0001 |
| Female | 394 (56.2) | 394 (56.2) | 394 (56.2) | 394 (56.2) | 394 (56.2) | 394 (56.2) | 394 (56.2) | 394 (56.2) | 394 (56.2) | 394 (56.2) | −0.025 ± 0.0022 | <0.0001 |
| p value for interaction c | 0.7966 | |||||||||||
| Education level | ||||||||||||
| Primary/illiterate | 662 (56.3) | 629 (55.1) | 615 (49.8) | 591 (43.2) | 768 (47.9) | 760 (44.5) | 814 (42.7) | 764 (33.4) | 1046 (37.4) | 1162 (40.9) | −0.024 ± 0.0019 | <0.0001 |
| Middle school and above | 81 (66.4) | 94 (60.6) | 142 (66.0) | 229 (65.8) | 294 (56.1) | 349 (55.8) | 402 (54.5) | 642 (47.6) | 1144 (52.6) | 1558 (54.7) | −0.022 ± 0.0035 | <0.0001 |
| p value for interaction c | 0.0386 | |||||||||||
| Yearly income level | ||||||||||||
| Low | 212 (48.1) | 207 (45.7) | 250 (48.1) | 243 (39.8) | 314 (44.3) | 311 (40.2) | 323 (37.0) | 361 (30.0) | 544 (33.5) | 632 (36.7) | −0.024 ± 0.0028 | <0.0001 |
| Middle | 230 (51.9) | 249 (54.8) | 246 (47.3) | 271 (44.4) | 348 (49.2) | 357 (46.0) | 430 (49.3) | 439 (36.5) | 694 (42.7) | 800 (46.5) | −0.018 ± 0.0028 | <0.0001 |
| High | 309 (69.9) | 288 (63.6) | 306 (58.8) | 348 (57.0) | 398 (56.1) | 435 (56.3) | 455 (52.2) | 591 (49.2) | 919 (56.6) | 990 (57.5) | −0.027 ± 0.0030 | <0.0001 |
| p value for interaction c | 0.8876 | |||||||||||
| Area | ||||||||||||
| City | 238 (65.0) | 206 (60.1) | 256 (61.8) | 270 (58.6) | 322 (58.8) | 370 (61.2) | 367 (56.3) | 621 (49.6) | 1035 (54.6) | 1345 (56.6) | −0.022 ± 0.0031 | <0.0001 |
| Suburb | 254 (56.1) | 245 (50.7) | 278 (47.2) | 282 (45.5) | 326 (50.2) | 340 (47.4) | 379 (45.4) | 331 (36.2) | 421 (41.5) | 585 (50.2) | −0.016 ± 0.0030 | <0.0001 |
| Town | 188 (44.8) | 216 (50.1) | 247 (49.9) | 216 (40.8) | 257 (44.1) | 193 (30.6) | 269 (37.9) | 268 (27.3) | 542 (35.8) | 602 (35.9) | −0.027 ± 0.0030 | <0.0001 |
| Village | 76 (80.0) | 83 (72.2) | 34 (37.8) | 126 (44.7) | 163 (44.8) | 218 (53.7) | 206 (44.3) | 191 (37.8) | 205 (36.0) | 243 (37.3) | −0.053 ± 0.0055 | <0.0001 |
| p value for interaction c | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ouyang, Y.; Tan, T.; Song, X.; Huang, F.; Zhang, B.; Ding, G.; Wang, H. Dietary Protein Intake Dynamics in Elderly Chinese from 1991 to 2018. Nutrients 2021, 13, 3806. https://doi.org/10.3390/nu13113806
Ouyang Y, Tan T, Song X, Huang F, Zhang B, Ding G, Wang H. Dietary Protein Intake Dynamics in Elderly Chinese from 1991 to 2018. Nutrients. 2021; 13(11):3806. https://doi.org/10.3390/nu13113806
Chicago/Turabian StyleOuyang, Yifei, Tingyi Tan, Xiaoyun Song, Feifei Huang, Bing Zhang, Gangqiang Ding, and Huijun Wang. 2021. "Dietary Protein Intake Dynamics in Elderly Chinese from 1991 to 2018" Nutrients 13, no. 11: 3806. https://doi.org/10.3390/nu13113806
APA StyleOuyang, Y., Tan, T., Song, X., Huang, F., Zhang, B., Ding, G., & Wang, H. (2021). Dietary Protein Intake Dynamics in Elderly Chinese from 1991 to 2018. Nutrients, 13(11), 3806. https://doi.org/10.3390/nu13113806