

The Effect of Daily Methylsulfonylmethane (MSM) Consumption on High-Density Lipoprotein Cholesterol in Healthy Overweight and Obese Adults: A Randomized Controlled Trial

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Approval
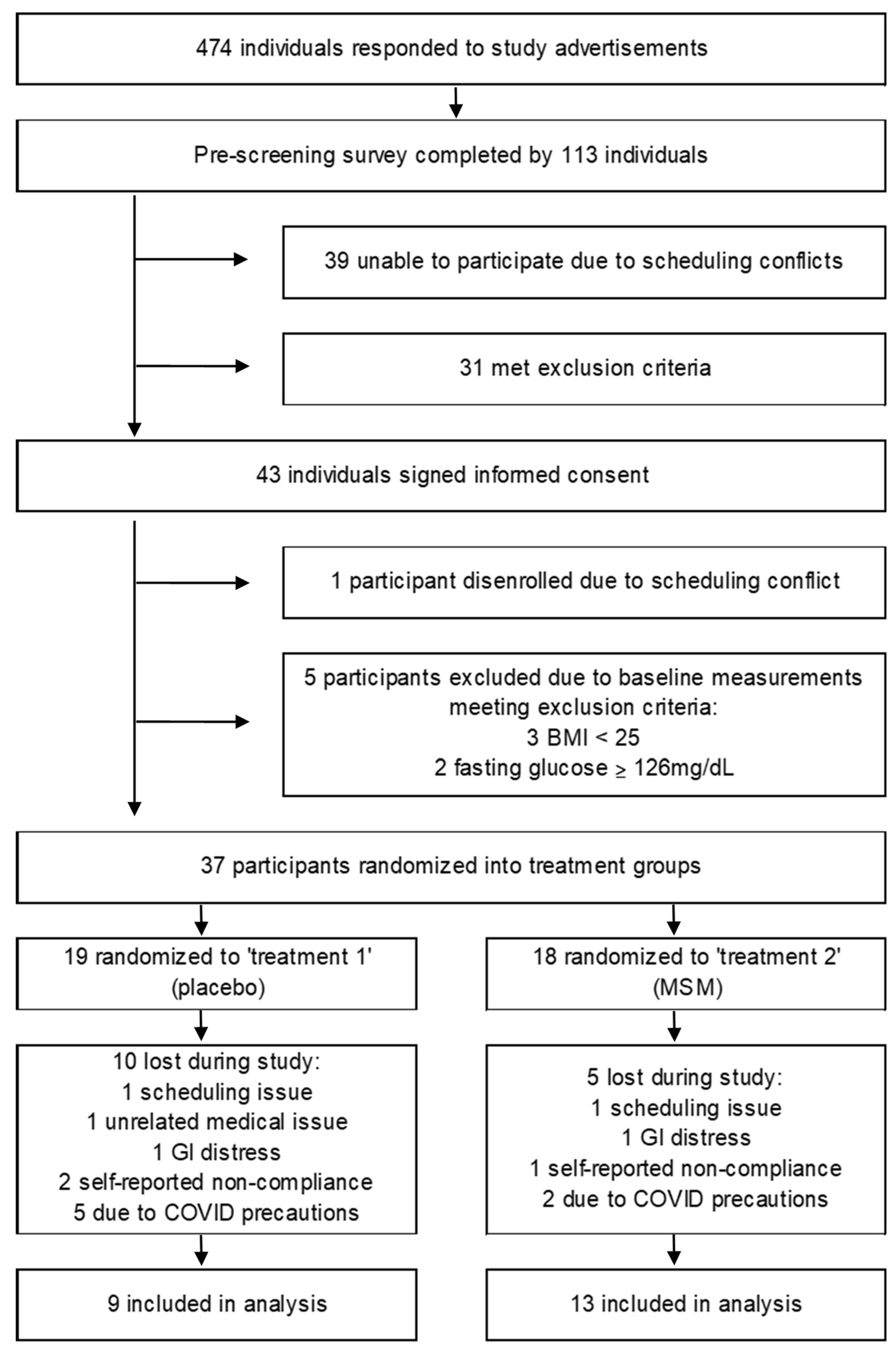
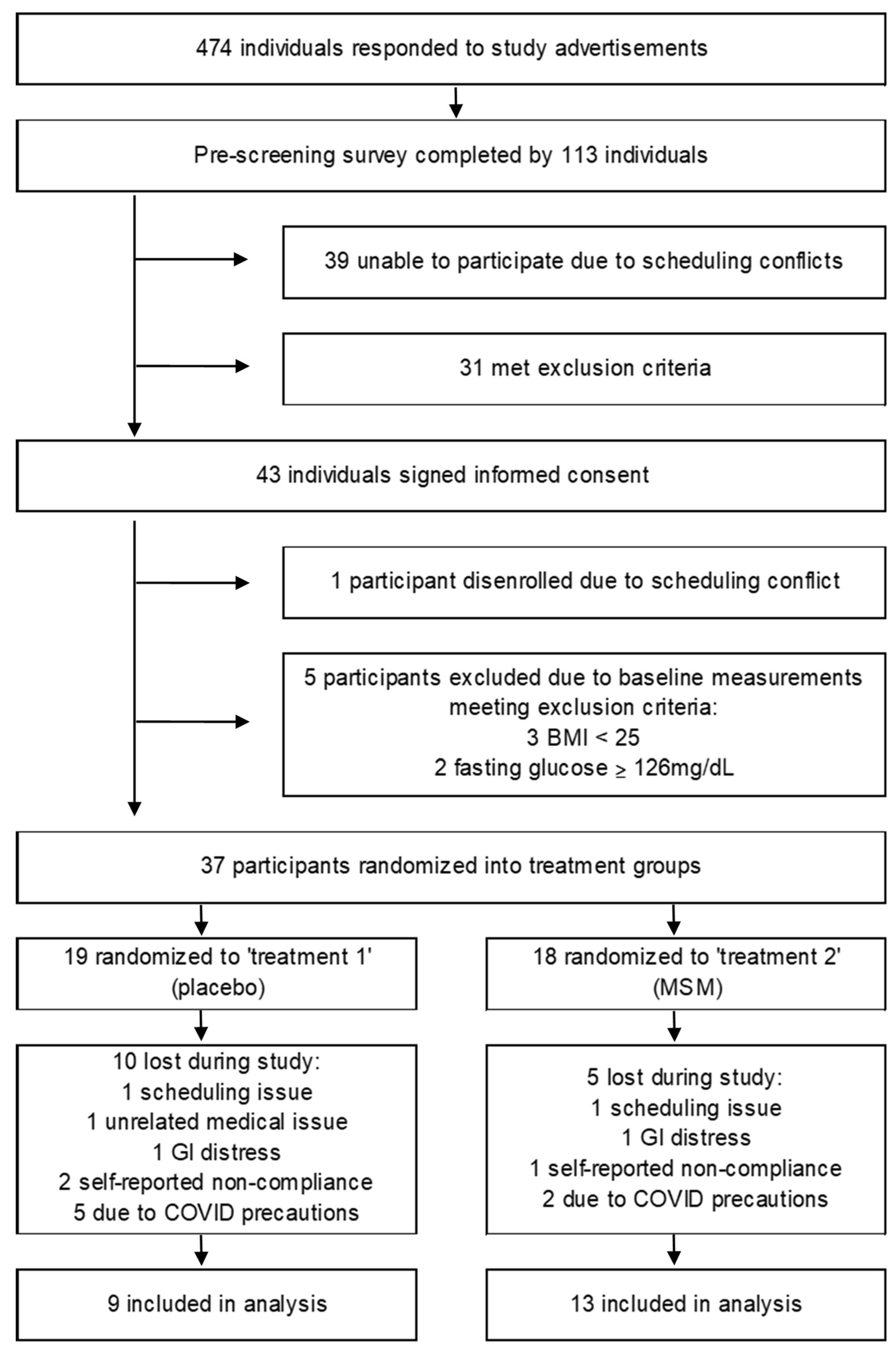
2.2. Participant Recruitment
2.3. Study Design
2.4. Physical Activity
2.5. Dietary Intake
2.6. Anthropometric Measures
2.7. Metabolic Rate and Blood Pressure
2.8. Blood Measures
2.9. Statistics
3. Results
3.1. Physical Activity and Diet
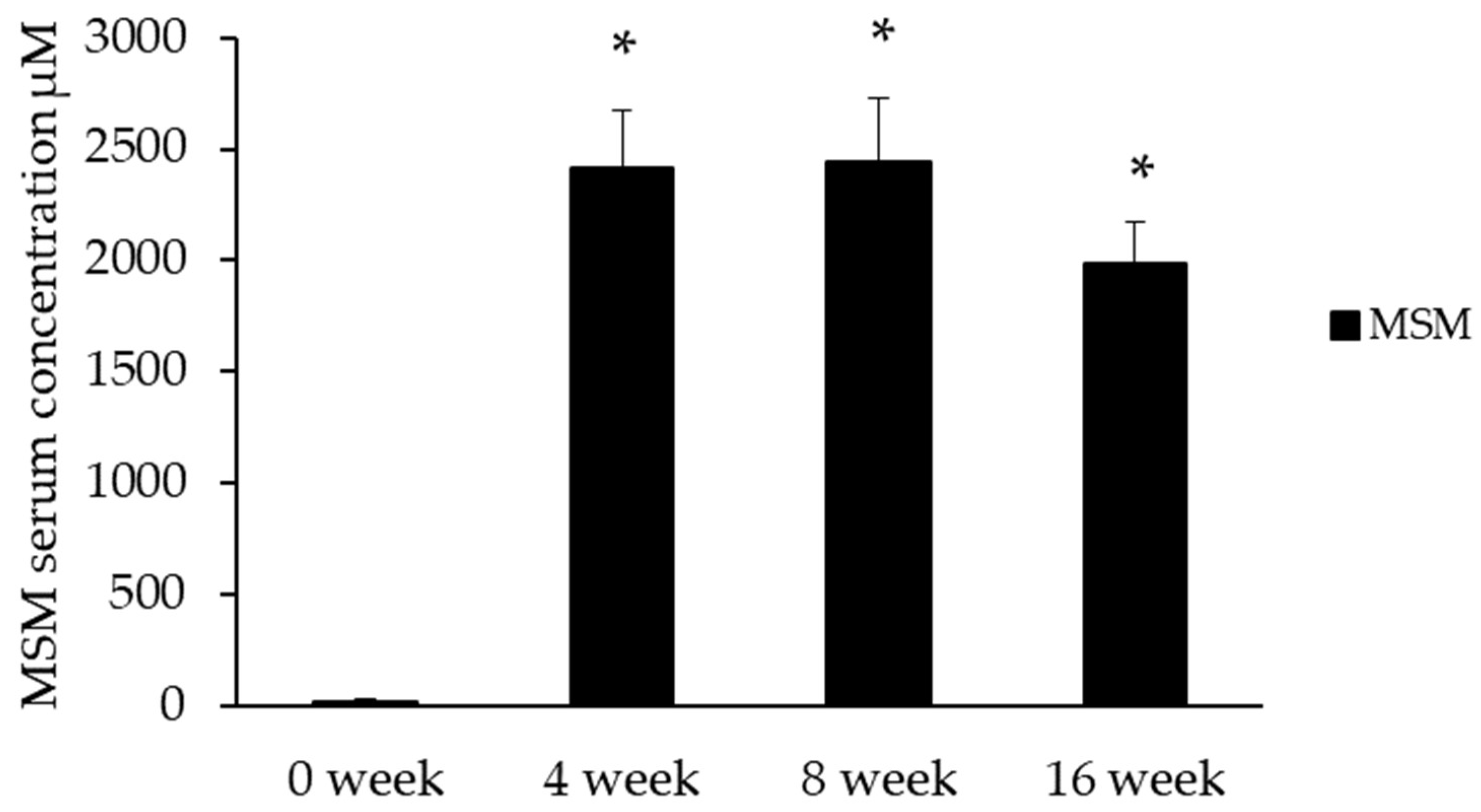
3.2. Serum Methylsulfonylmethane
3.3. Anthropometric, Metabolic Measures
3.4. Measures of Inflammation, Oxidative Status, and Cardiac Fibrosis
4. Discussion
4.1. Physical Activity and Diet
4.2. Serum MSM
4.3. Markers of Cardiometabolic Health
4.4. Markers of Inflammation and Oxidative Status
4.5. Cardiac Fibrosis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Ogden, C.L.; Flegal, K.M. Prevalence of Obesity Among Adults and Youth: United States, 2011–2014. NCHS Data Brief 2015, 131, 1–8. [Google Scholar]
- Fève, B.; Bastard, J.-P. The Role of Interleukins in Insulin Resistance and Type 2 Diabetes Mellitus. Nat. Rev. Endocrinol. 2009, 5, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Katz, R.; Jenny, N.S.; Zakai, N.A.; LeWinter, M.M.; Barzilay, J.I.; Cushman, M. Metabolic Syndrome, Inflammation, and Incident Heart Failure in the Elderly: The Cardiovascular Health Study. Circ. Heart Fail. 2008, 1, 242–248. [Google Scholar] [CrossRef] [Green Version]
- Savini, I.; Catani, M.V.; Evangelista, D.; Gasperi, V.; Avigliano, L. Obesity-Associated Oxidative Stress: Strategies Finalized to Improve Redox State. Int. J. Mol. Sci. 2013, 14, 10497–10538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, L.; Ellims, A.H.; Beale, A.L.; Taylor, A.J.; Murphy, A.; Dart, A.M. Systemic Inflammation Is Associated with Myocardial Fibrosis, Diastolic Dysfunction, and Cardiac Hypertrophy in Patients with Hypertrophic Cardiomyopathy. Am. J. Transl. Res. 2017, 9, 5063–5073. [Google Scholar] [PubMed]
- Bahrami, H.; Bluemke, D.A.; Kronmal, R.; Bertoni, A.G.; Lloyd-Jones, D.M.; Shahar, E.; Szklo, M.; Lima, J.A.C. Novel Metabolic Risk Factors for Incident Heart Failure and Their Relationship with Obesity: The MESA (Multi-Ethnic Study of Atherosclerosis) Study. J. Am. Coll. Cardiol. 2008, 51, 1775–1783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Visser, M.; Bouter, L.M.; McQuillan, G.M.; Wener, M.H.; Harris, T.B. Elevated C-Reactive Protein Levels in Overweight and Obese Adults. JAMA 1999, 282, 2131–2135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wee, C.C.; Mukamal, K.J.; Huang, A.; Davis, R.B.; McCarthy, E.P.; Mittleman, M.A. Obesity and C-Reactive Protein Levels among White, Black, and Hispanic US Adults. Obesity 2008, 16, 875–880. [Google Scholar] [CrossRef]
- Eckel, N.; Meidtner, K.; Kalle-Uhlmann, T.; Stefan, N.; Schulze, M.B. Metabolically Healthy Obesity and Cardiovascular Events: A Systematic Review and Meta-Analysis. Eur. J. Prev. Cardiol. 2016, 23, 956–966. [Google Scholar] [CrossRef]
- Bell, J.A.; Kivimaki, M.; Hamer, M. Metabolically Healthy Obesity and Risk of Incident Type 2 Diabetes: A Meta-Analysis of Prospective Cohort Studies. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2014, 15, 504–515. [Google Scholar] [CrossRef] [Green Version]
- Bañuls, C.; Rovira-Llopis, S.; Lopez-Domenech, S.; Diaz-Morales, N.; Blas-Garcia, A.; Veses, S.; Morillas, C.; Victor, V.M.; Rocha, M.; Hernandez-Mijares, A. Oxidative and Endoplasmic Reticulum Stress Is Impaired in Leukocytes from Metabolically Unhealthy vs Healthy Obese Individuals. Int. J. Obes. 2017, 41, 1556–1563. [Google Scholar] [CrossRef] [PubMed]
- Esser, N.; L’homme, L.; De Roover, A.; Kohnen, L.; Scheen, A.J.; Moutschen, M.; Piette, J.; Legrand-Poels, S.; Paquot, N. Obesity Phenotype Is Related to NLRP3 Inflammasome Activity and Immunological Profile of Visceral Adipose Tissue. Diabetologia 2013, 56, 2487–2497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Opio, J.; Croker, E.; Odongo, G.S.; Attia, J.; Wynne, K.; McEvoy, M. Metabolically Healthy Overweight/Obesity Are Associated with Increased Risk of Cardiovascular Disease in Adults, Even in the Absence of Metabolic Risk Factors: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. Obes. Rev. 2020, 21, e13127. [Google Scholar] [CrossRef] [PubMed]
- Bogers, R.P.; Bemelmans, W.J.E.; Hoogenveen, R.T.; Boshuizen, H.C.; Woodward, M.; Knekt, P.; van Dam, R.M.; Hu, F.B.; Visscher, T.L.S.; Menotti, A.; et al. Association of Overweight with Increased Risk of Coronary Heart Disease Partly Independent of Blood Pressure and Cholesterol Levels: A Meta-Analysis of 21 Cohort Studies Including More Than 300,000 Persons. Arch. Intern. Med. 2007, 167, 1720–1728. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the Metabolic Syndrome: A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; And International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [Green Version]
- Franz, M.J.; Boucher, J.L.; Rutten-Ramos, S.; VanWormer, J.J. Lifestyle Weight-Loss Intervention Outcomes in Overweight and Obese Adults with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. J. Acad. Nutr. Diet. 2015, 115, 1447–1463. [Google Scholar] [CrossRef] [PubMed]
- Stefan, N.; Häring, H.-U.; Schulze, M.B. Metabolically Healthy Obesity: The Low-Hanging Fruit in Obesity Treatment? Lancet Diabetes Endocrinol. 2018, 6, 249–258. [Google Scholar] [CrossRef]
- Nakhostin-Roohi, B.; Barmaki, S.; Khoshkhahesh, F.; Bohlooli, S. Effect of Chronic Supplementation with Methylsulfonylmethane on Oxidative Stress Following Acute Exercise in Untrained Healthy Men. J. Pharm. Pharmacol. 2011, 63, 1290–1294. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.H.; Kim, D.H.; Lim, H.; Baek, D.-Y.; Shin, H.-K.; Kim, J.-K. The Anti-Inflammatory Effects of Methylsulfonylmethane on Lipopolysaccharide-Induced Inflammatory Responses in Murine Macrophages. Biol. Pharm. Bull. 2009, 32, 651–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, H.; Kim, J.; Lee, M.-J.; Kim, Y.J.; Cho, Y.-W.; Lee, G.-S. Methylsulfonylmethane Inhibits NLRP3 Inflammasome Activation. Cytokine 2015, 71, 223–231. [Google Scholar] [CrossRef]
- Miller, L.E. Methylsulfonylmethane Decreases Inflammatory Response to Tumor Necrosis Factor-α in Cardiac Cells. Am. J. Cardiovasc. Dis. 2018, 8, 31–38. [Google Scholar] [PubMed]
- Bertoni, A.G.; Burke, G.L.; Owusu, J.A.; Carnethon, M.R.; Vaidya, D.; Barr, R.G.; Jenny, N.S.; Ouyang, P.; Rotter, J.I. Inflammation and the Incidence of Type 2 Diabetes: The Multi-Ethnic Study of Atherosclerosis (MESA). Diabetes Care 2010, 33, 804–810. [Google Scholar] [CrossRef] [Green Version]
- Sousa-Lima, I.; Park, S.-Y.; Chung, M.; Jung, H.J.; Kang, M.-C.; Gaspar, J.M.; Seo, J.A.; Macedo, M.P.; Park, K.S.; Mantzoros, C.; et al. Methylsulfonylmethane (MSM), an Organosulfur Compound, Is Effective against Obesity-Induced Metabolic Disorders in Mice. Metabolism 2016, 65, 1508–1521. [Google Scholar] [CrossRef]
- Rubenstein, J.H.; Morgenstern, H.; Kellenberg, J.; Kalish, T.; Donovan, J.; Inadomi, J.; McConnell, D.; Stojanovska, J.; Schoenfeld, P. Validation of a New Physical Activity Questionnaire for a Sedentary Population. Dig. Dis. Sci. 2011, 56, 2678–2687. [Google Scholar] [CrossRef] [PubMed]
- Subar, A.F.; Kirkpatrick, S.I.; Mittl, B.; Zimmerman, T.P.; Thompson, F.E.; Bingley, C.; Willis, G.; Islam, N.G.; Baranowski, T.; McNutt, S.; et al. The Automated Self-Administered 24-Hour Dietary Recall (ASA24): A Resource for Researchers, Clinicians, and Educators from the National Cancer Institute. J. Acad. Nutr. Diet. 2012, 112, 1134–1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and β-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, T.M.; Levy, J.C.; Matthews, D.R. Use and Abuse of HOMA Modeling. Diabetes Care 2004, 27, 1487–1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, L.; Ma, D.; Bloomer, R.; Butawan, M.; Smith, W.A.; Yates, C.R. Development and Application of an LC-MS/MS Method for Determining Methylsulfonylmethane (MSM) Levels in Human Plasma. J Nutr Food Sci. 2020, 10, 773. [Google Scholar]
- Luo, X.; Chae, M.; Krishnakumar, R.; Danko, C.G.; Kraus, W. Dynamic Reorganization of the AC16 Cardiomyocyte Transcriptome in Response to TNFα Signaling Revealed by Integrated Genomic Analyses. BMC Genom. 2014, 15, 155. [Google Scholar] [CrossRef] [Green Version]
- Gordon, D.J.; Probstfield, J.L.; Garrison, R.J.; Neaton, J.D.; Castelli, W.P.; Knoke, J.D.; Jacobs, D.R.; Bangdiwala, S.; Tyroler, H.A. High-Density Lipoprotein Cholesterol and Cardiovascular Disease. Four Prospective American Studies. Circulation 1989, 79, 8–15. [Google Scholar] [CrossRef] [Green Version]
- Pirillo, A.; Catapano, A.L.; Norata, G.D. Biological Consequences of Dysfunctional HDL. Curr. Med. Chem. 2019, 26, 1644–1664. [Google Scholar] [CrossRef] [PubMed]
- van der Merwe, M.; Bloomer, R.J. The Influence of Methylsulfonylmethane on Inflammation-Associated Cytokine Release before and Following Strenuous Exercise. J. Sports Med. 2016, 2016, 7498359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morishima, A.; Ohkubo, N.; Maeda, N.; Miki, T.; Mitsuda, N. NFkappaB Regulates Plasma Apolipoprotein A-I and High Density Lipoprotein Cholesterol through Inhibition of Peroxisome Proliferator-Activated Receptor Alpha. J. Biol. Chem. 2003, 278, 38188–38193. [Google Scholar] [CrossRef] [Green Version]
- Puzianowska-Kuźnicka, M.; Owczarz, M.; Wieczorowska-Tobis, K.; Nadrowski, P.; Chudek, J.; Slusarczyk, P.; Skalska, A.; Jonas, M.; Franek, E.; Mossakowska, M. Interleukin-6 and C-Reactive Protein, Successful Aging, and Mortality: The PolSenior Study. Immun. Ageing 2016, 13, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barmaki, S.; Bohlooli, S.; Khoshkhahesh, F.; Nakhostin-Roohi, B. Effect of Methylsulfonylmethane Supplementation on Exercise—Induced Muscle Damage and Total Antioxidant Capacity. J. Sports Med. Phys. Fitness 2012, 52, 170–174. [Google Scholar] [PubMed]
- Nakhostin-Roohi, B.; Niknam, Z.; Vaezi, N.; Mohammadi, S.; Bohlooli, S. Effect of Single Dose Administration of Methylsulfonylmethane on Oxidative Stress Following Acute Exhaustive Exercise. Iran J. Pharm. Res. 2013, 12, 845–853. [Google Scholar]
- Gupta, S.; Young, D.; Maitra, R.K.; Gupta, A.; Popovic, Z.B.; Yong, S.L.; Mahajan, A.; Wang, Q.; Sen, S. Prevention of Cardiac Hypertrophy and Heart Failure by Silencing of NF-KappaB. J. Mol. Biol. 2008, 375, 637–649. [Google Scholar] [CrossRef] [Green Version]
- Zhong, P.; Wu, L.; Qian, Y.; Fang, Q.; Liang, D.; Wang, J.; Zeng, C.; Wang, Y.; Liang, G. Blockage of ROS and NF-ΚB-Mediated Inflammation by a New Chalcone L6H9 Protects Cardiomyocytes from Hyperglycemia-Induced Injuries. Biochim. Biophys. Acta 2015, 1852, 1230–1241. [Google Scholar] [CrossRef] [Green Version]
- Rubiś, P.; Wiśniowska-Smiałek, S.; Wypasek, E.; Rudnicka-Sosin, L.; Hlawaty, M.; Leśniak-Sobelga, A.; Kostkiewicz, M.; Podolec, P. 12-Month Patterns of Serum Markers of Collagen Synthesis, Transforming Growth Factor and Connective Tissue Growth Factor Are Similar in New-Onset and Chronic Dilated Cardiomyopathy in Patients Both with and without Cardiac Fibrosis. Cytokine 2017, 96, 217–227. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Placebo | MSM | p Value |
|---|---|---|---|
| n (sex) | 6 (female) 3 (male) | 9 (female) 4 (male) | |
| age | 40.7 ± 4.0 | 43.7 ± 3.9 | 0.605 |
| BMI (kg/m2) | 34 ± 2.3 | 31.5 ± 1.1 | 0.593 |
| % body fat | 41.2 ± 3.3 | 39.8 ± 2.0 | 0.708 |
| RMR (kcals/day) | 1650.0 ± 218.3 | 1596.9 ± 109.3 | 0.814 |
| PA (kcals/kg/week) | 290.5 ± 29.2 | 299.6 ± 24.3 | 0.789 |
| Dietary intake (kcals/day) | 2069.1 ± 174.4 | 2206.0 ± 134.3 | 0.54 |
| Fat (g/day) | 78.9 ± 6.5 | 102.2 ± 6.5 | 0.031 * |
| Protein (g/day) | 82.6 ± 11.0 | 97.8 ± 10.2 | 0.263 |
| Carbohydrate (g/day) | 258.0 ± 43.5 | 231.5 ± 25.4 | 0.583 |
| Variable | Group | Baseline | 4 Week | 8 Week | 16 Week | p Value |
|---|---|---|---|---|---|---|
| glucose (mg/dL) | placebo | 92.3 ± 4.1 | 93.8 ± 3.7 | 92.9 ± 3.9 | 94.4 ± 3.2 | 0.656 |
| MSM | 92.5 ± 3.0 | 95.0 ± 2.8 | 93.8 ± 2.9 | 93.2 ± 2.5 | ||
| insulin (uUI/mL) | placebo | 19.6 ± 3.6 | 18.2 ± 4.4 | 17.4 ± 5.4 | 20.6 ± 5.8 | 0.097 |
| MSM | 18.5 ± 2.6 | 18.3 ± 1.7 | 14.7 ± 1.5 | 17.9 ± 1.6 | ||
| HOMA-IR | placebo | 4.5 ± 0.8 | 4.2 ± 1.1 | 4.0 ± 1.3 | 4.8 ± 1.4 | 0.260 |
| MSM | 4.2 ± 0.6 | 4.3 ± 0.4 | 3.9 ± 0.5 | 4.1 ± 0.4 | ||
| Total Cholesterol (mg/dL) | placebo | 188.3 ± 11.5 | 194.3 ± 8.0 | 200 ± 9.4 | 186.9 ± 9.3 | 0.099 |
| MSM | 172.2 ± 10.3 | 179.0 ± 8.4 | 181.2 ± 8.0 | 176.4 ± 8.3 | ||
| TGs (mg/dL) | placebo | 165.0 ± 36.0 | 121.1 ± 13.8 | 156.4 ± 35.7 | 162.1 ± 26.2 | 0.515 |
| MSM | 112.5 ± 11.4 | 110.7 ± 9.6 | 112.1 ± 12.8 | 131.6 ± 18.3 | ||
| LDL (mg/dL) | placebo | 118.6 ± 9.2 | 123.9 ± 6.5 | 127.6 ± 9.7 | 109.7 ± 10.2 | 0.126 |
| MSM | 102.0 ± 8.5 | 106.2 ± 7.3 | 107.4 ± 5.6 | 100.2 ± 6.3 | ||
| VLDL (mg/dL) | placebo | 27.8 ± 3.4 | 24.4 ± 2.7 | 27.1 ± 1.4 | 29.2 ± 5.2 | 0.235 |
| MSM | 22.5 ± 2.3 | 22.2 ± 1.9 | 21.6 ± 2.6 | 24.4 ± 3.6 | ||
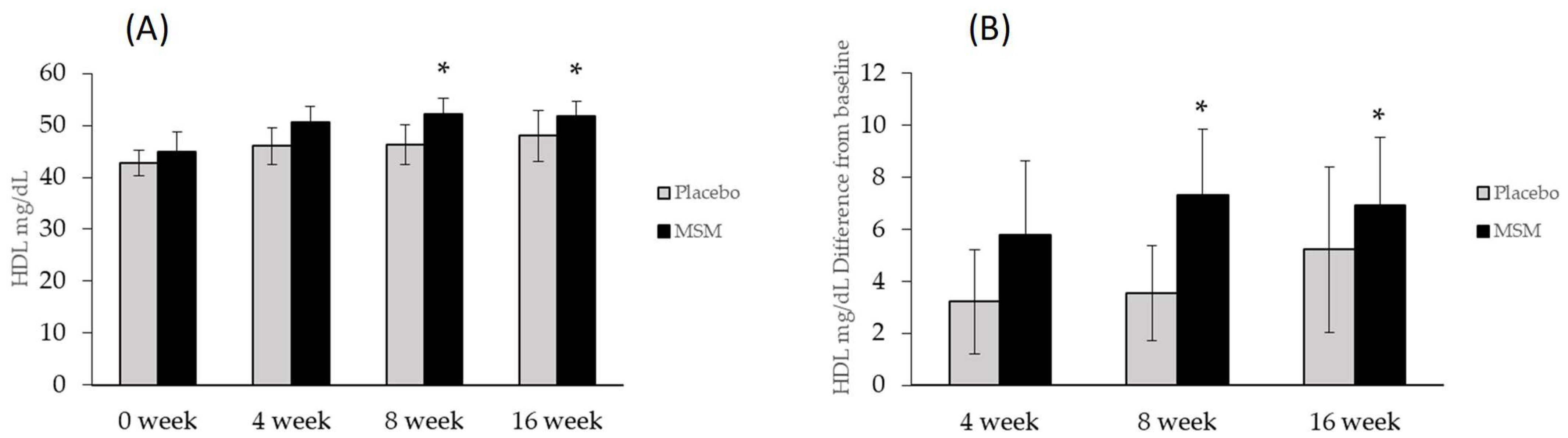
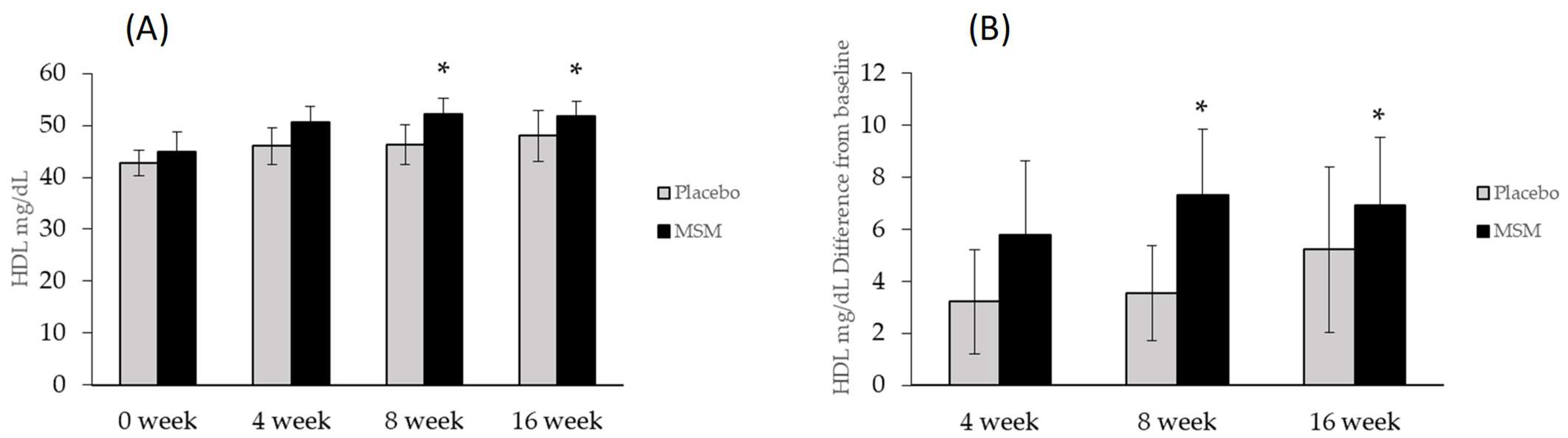
| HDL (mg/dL) | placebo | 42.7 ± 2.5 | 46.0 ± 3.8 | 46.3 ± 3.8 | 48.0 ± 4.9 | 0.003 |
| MSM | 44.9 ± 3.7 | 50.7 ± 3.0 | * 52.2 ± 2.9 | * 51.8 ± 2.8 | ||
| SBP (mmHg) | placebo | 123.5 ± 5.2 | 118.1 ± 5.2 | 119.3 ± 5.4 | 114.9 ± 3.1 | 0.625 |
| MSM | 127.3 ± 4.6 | 120.3 ± 5.2 | 119.7 ± 4.0 | 121.6 ± 4.8 | ||
| DBP (mmHg) | placebo | 84.8 ± 4.5 | 77.6 ± 3.5 | 79.8 ± 3.0 | 78.2 ± 2.6 | 0.967 |
| MSM | 80.7 ± 3.1 | 81.3 ± 4.0 | 77.6 ± 3.5 | 80.1 ± 3.3 |
| Variable | Group | Baseline | 4 Week | 8 Week | 16 Week | p Value |
|---|---|---|---|---|---|---|
| TAC | placebo | 6.06 ± 0.58 | 6.49 ± 0.78 | 6.30 ± 0.74 | 6.44 ± 0.91 | 0.583 |
| MSM | 6.37 ± 0.58 | 6.49 ± 0.61 | 6.75 ± 0.66 | 6.75 ± 0.60 | ||
| TNF-α | placebo | 6.46 ± 1.08 | 6.63 ± 1.07 | 6.72 ± 1.07 | 6.84 ± 1.08 | 0.498 |
| MSM | 7.84 ± 1.06 | 7.76 ± 1.00 | 7.63 ± 0.98 | 8.04 ± 1.13 | ||
| IL-6 | placebo | 1.75 ± 0.43 | 2.33 ± 0.59 | 2.17 ± 0.71 | 2.29 ± 0.66 | 0.319 |
| MSM | 1.79 ± 0.60 | 2.07 ± 0.67 | 1.76 ± 0.62 | 1.68 ± 0.57 | ||
| 4-HNE | placebo | 91.24 ± 20.91 | 96.63 ± 22.14 | 87.77 ± 21.5 | 85.75 ± 26.62 | 0.574 |
| MSM | 50.90 ± 6.58 | 55.01 ± 7.37 | 55.61 ± 8.51 | 49.88 ± 7.54 | ||
| PINP | placebo | 437.38 ± 98.32 | _ | _ | 363.27 ± 51.39 | 0.297 |
| MSM | 432.74 ± 77.78 | _ | _ | 460.38 ± 64.39 | ||
| PIIINP | placebo | 0.446 ± 0.130 | _ | _ | 0.680 ± 0.293 | 0.308 |
| MSM | 0.305 ± 0.077 | _ | _ | 0.533 ± 0.120 | ||
| PINP/PIIINP | placebo | 3691.512 ± 2714.35 | _ | _ | 2369.616 ± 945.108 | 0.311 |
| MSM | 1727.916 ± 601.482 | _ | _ | 899.000 ± 187.634 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miller, L.; Thompson, K.; Pavlenco, C.; Mettu, V.S.; Haverkamp, H.; Skaufel, S.; Basit, A.; Prasad, B.; Larsen, J. The Effect of Daily Methylsulfonylmethane (MSM) Consumption on High-Density Lipoprotein Cholesterol in Healthy Overweight and Obese Adults: A Randomized Controlled Trial. Nutrients 2021, 13, 3620. https://doi.org/10.3390/nu13103620
Miller L, Thompson K, Pavlenco C, Mettu VS, Haverkamp H, Skaufel S, Basit A, Prasad B, Larsen J. The Effect of Daily Methylsulfonylmethane (MSM) Consumption on High-Density Lipoprotein Cholesterol in Healthy Overweight and Obese Adults: A Randomized Controlled Trial. Nutrients. 2021; 13(10):3620. https://doi.org/10.3390/nu13103620
Chicago/Turabian StyleMiller, Lindsey, Kari Thompson, Carolina Pavlenco, Vijaya Saradhi Mettu, Hans Haverkamp, Samantha Skaufel, Abdul Basit, Bhagwat Prasad, and Julie Larsen. 2021. "The Effect of Daily Methylsulfonylmethane (MSM) Consumption on High-Density Lipoprotein Cholesterol in Healthy Overweight and Obese Adults: A Randomized Controlled Trial" Nutrients 13, no. 10: 3620. https://doi.org/10.3390/nu13103620
APA StyleMiller, L., Thompson, K., Pavlenco, C., Mettu, V. S., Haverkamp, H., Skaufel, S., Basit, A., Prasad, B., & Larsen, J. (2021). The Effect of Daily Methylsulfonylmethane (MSM) Consumption on High-Density Lipoprotein Cholesterol in Healthy Overweight and Obese Adults: A Randomized Controlled Trial. Nutrients, 13(10), 3620. https://doi.org/10.3390/nu13103620