
COVID-19 Mortality Risk Correlates Inversely with Vitamin D3 Status, and a Mortality Rate Close to Zero Could Theoretically Be Achieved at 50 ng/mL 25(OH)D3: Results of a Systematic Review and Meta-Analysis


Abstract
:1. Introduction
- Vitamin D3 reduces the severity of cytokine release syndrome (CRS). This “cytokine storm” causes multiple organ damage and is therefore the main cause of death in the late stage of SARS-CoV-2 infection. The systemic inflammatory response due to viral infection is attenuated by promoting the differentiation of regulatory T cells [98,99,100,101].
2. Methods
2.1. Search Strategy and Selection Criteria
2.2. Data Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xue, K.S. Coexisting with the Coronavirus. New Yorker. 2021. Available online: https://www.newyorker.com/science/annals-of-medicine/coexisting-with-the-coronavirus (accessed on 20 August 2021).
- Can We Predict the Limits of SARS-CoV-2 Variants and Their Phenotypic Consequences? 2021. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1007566/S1335_Long_term_evolution_of_SARS-CoV-2.pdf (accessed on 27 August 2021).
- Denison, M.R.; Graham, R.L.; Donaldson, E.F.; Eckerle, L.D.; Baric, R.S. Coronaviruses. RNA Biol. Inf. UK Ltd. 2011, 8, 270. [Google Scholar] [CrossRef] [Green Version]
- Dawood, A.A. Mutated COVID-19 may foretell a great risk for mankind in the future. New Microbes New Infect. Elsevier BV 2020, 35, 673. [Google Scholar] [CrossRef] [PubMed]
- Harvey, W.T.; Carabelli, A.M.; Jackson, B.; Gupta, R.K.; Thomson, E.C.; Harrison, E.M. SARS-CoV-2 variants, spike mutations and immune escape. Nat. Rev. Microbiol 2021, 19, 409. [Google Scholar] [CrossRef] [PubMed]
- Williams, T.C.; Burgers, W.A. SARS-CoV-2 evolution and vaccines: Cause for concern? Lancet Respir. Med. 2021, 9, 333. [Google Scholar] [CrossRef]
- Karim, S.S.A. Vaccines and SARS-CoV-2 variants: The urgent need for a correlate of protection. Lancet 2021, 397, 1263. [Google Scholar] [CrossRef]
- Starr, T.N.; Greaney, A.J.; Addetia, A.; Hannon, W.W.; Choudhary, M.C.; Dingens, A.S. Prospective mapping of viral mutations that escape antibodies used to treat COVID-Science (80-). Am. Assoc. Adv. Sci. 2021, 371, 850. [Google Scholar] [CrossRef]
- Brown, C.M.; Vostok, J.; Johnson, H.; Burns, M.; Gharpure, R.; Sami, S. Outbreak of SARS-CoV-2 Infections, Including COVID-19 Vaccine Breakthrough Infections, Associated with Large Public Gatherings—Barnstable County, Massachusetts, July MMWR. Morb. Mortal. Wkly Rep. 2021, 70, 1059. [Google Scholar] [CrossRef] [PubMed]
- Rella, S.A.; Kulikova, Y.A.; Dermitzakis, E.T.; Kondrashov, F.A. Rates of SARS-CoV-2 transmission and vaccination impact the fate of vaccine-resistant strains. Sci. Rep. 2021, 38, 950253. [Google Scholar] [CrossRef]
- Rella, S.A.; Kulikova, Y.A.; Dermitzakis, E.T.; Kondrashov, F.A. SARS-CoV-2 transmission, vaccination rate and the fate of resistant strains. Cold Spring Harb. Lab. 2021, 11, 1383. [Google Scholar] [CrossRef]
- Iddir, M.; Brito, A.; Dingeo, G.; Campo, S.S.F.; Samouda, H.; Frano, M.R. Strengthening the Immune System and Reducing Inflammation and Oxidative Stress through Diet and Nutrition: Considerations during the COVID-19 Crisis. Nutrients 2020, 12, 1562. [Google Scholar] [CrossRef]
- Holick, M.F.; Chen, T.C. Vitamin D deficiency: A worldwide problem with health consequences. Am. J. Clin. Nutr. 2008, 87, 1080S–1086S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manson, J.E.; Bassuk, S.S. Commentary. Eliminating vitamin D deficiency during the COVID-19 pandemic: A call to action. Metabolism 2020, 112, 154322. [Google Scholar] [CrossRef]
- Palacios, C.; Gonzalez, L. Is vitamin D deficiency a major global public health problem? J. Steroid Biochem. Mol. Biol. 2014, 144, 138. [Google Scholar] [CrossRef] [Green Version]
- Forrest, K.Y.Z.; Stuhldreher, W.L. Prevalence and correlates of vitamin D deficiency in US adults. Nutr. Res. 2011, 31, 48. [Google Scholar] [CrossRef] [PubMed]
- Tangpricha, V.; Pearce, E.N.; Chen, T.C.; Holick, M.F. Vitamin D insufficiency among free-living healthy young adults. Am. J. Med. 2002, 112, 659. [Google Scholar] [CrossRef] [Green Version]
- Honardoost, M.; Ghavideldarestani, M.; Khamseh, M.E. Role of vitamin D in pathogenesis and severity of COVID-19 infection. Arch. Physiol. Biochem. 2020, 1, 1792505. [Google Scholar] [CrossRef]
- Lips, P.; Cashman, K.D.; Lamberg-Allardt, C.; Bischoff-Ferrari, H.A.; Obermayer-Pietsch, B.; Bianchi, M.L. Current vitamin D status in European and Middle East countries and strategies to prevent vitamin D deficiency: A position statement of the European Calcified Tissue Society. Eur. J. Endocrinol. 2019, 180, P23. [Google Scholar] [CrossRef] [Green Version]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Berisha, A.T. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef]
- Biesalski, H.K. Vitamin D deficiency and co-morbidities in COVID-19 patients–A fatal relationship? NFLs J. 2020, 20, 10. [Google Scholar] [CrossRef]
- Gloth, F.M. Vitamin D Deficiency in Homebound Elderly Persons. JAMA J. Am. Med. Assoc. 1995, 274, 7027. [Google Scholar] [CrossRef]
- Giménez, V.M.M.; Inserra, F.; Ferder, L.; García, J.; Manucha, W. Vitamin D deficiency in African Americans is associated with a high risk of severe disease and mortality by SARS-CoV-J Hum Hypertens. Springer Sci. Bus. Media LLC 2020, 35, 378. [Google Scholar] [CrossRef]
- Berry, D.J.; Hesketh, K.; Power, C.; Hyppönen, E. Vitamin D status has a linear association with seasonal infections and lung function in British adults. Br. J. Nutr. 2011, 106, 1433–1440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohlmeier, M. Avoidance of vitamin D deficiency to slow the COVID-19 pandemic. BMJ Nutr. Prev. Health 2020, 3, 67. [Google Scholar] [CrossRef]
- Rhodes, J.M.; Subramanian, S.; Laird, E.; Kenny, R.A. Editorial: Low population mortality from COVID-19 in countries south of latitude 35 degrees North supports vitamin D as a factor determining severity. Aliment. Pharmacol. Ther. 2020, 51, 1434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abhimanyu, A.; Coussens, A.K. The role of UV radiation and vitamin D in the seasonality and outcomes of infectious disease. Photochem. Photobiol. Sci. 2017, 16, 314. [Google Scholar] [CrossRef]
- Zhang, M.; Shen, F.; Petryk, A.; Tang, J.; Chen, X.; Sergi, C. English Disease: Historical Notes on Rickets, the Bone Lung Link and Child Neglect Issues. Nutrients 2016, 8, 722. [Google Scholar] [CrossRef] [Green Version]
- Rajakumar, K. Vitamin D Cod-liver oil, sunlight, and rickets: A historical perspective. Pediatrics Am. Acad. Pediatrics 2003, 112, e132–e135. [Google Scholar] [CrossRef] [Green Version]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K. The 2011 Report on Dietary Reference Intakes for Calcium and Vitamin D from the Institute of Medicine: What Clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53. [Google Scholar] [CrossRef]
- DeLuca, H.F. History of the discovery of vitamin D and its active metabolites. Bonekey Rep. 2014, 3, 119. [Google Scholar] [CrossRef] [Green Version]
- Prietl, B.; Treiber, G.; Pieber, T.R.; Amrein, K. Vitamin D and immune function. Nutrients 2013, 5, 2502–2521. [Google Scholar] [CrossRef]
- Kongsbak, M.; Levring, T.B.; Geisler, C.; von Essen, M.R. The Vitamin D Receptor and T Cell Function. Front. Immunol. 2013, 14, 148. [Google Scholar] [CrossRef] [Green Version]
- Hewison, M. An update on vitamin D and human immunity. Clin. Endocrinol. 2012, 76, 315. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. Mass Med. Soc. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Battault, S.; Whiting, S.J.; Peltier, S.L.; Sadrin, S.; Gerber, G.; Maixent, J.M. Vitamin D metabolism, functions and needs: From science to health claims. Eur. J. Nutr. 2013, 52, 429–441. [Google Scholar] [CrossRef]
- Christakos, S.; Hewison, M.; Gardner, D.G.; Wagner, C.L.; Sergeev, I.N.; Rutten, E. Vitamin D: Beyond bone. Ann. N. Y. Acad. Sci. 2013, 1287, 45. [Google Scholar] [CrossRef] [PubMed]
- Charoenngam, N.; Holick, M.F. Immunologic Effects of Vitamin D on Human Health and Disease. Nutrients 2020, 12, 2097. [Google Scholar] [CrossRef]
- Carlberg, C. Vitamin D Signaling in the Context of Innate Immunity: Focus on Human Monocytes. Front. Immunol. 2019, 12, 2211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, W.B.; Anouti FAl Moukayed, M. Targeted 25-hydroxyvitamin D concentration measurements and vitamin D3 supplementation can have important patient and public health benefits. Eur. J. Clin. Nutr. 2020, 74, 366. [Google Scholar] [CrossRef]
- Feldman, D.; Krishnan, A.V.; Swami, S.; Giovannucci, E.; Feldman, B.J. The role of vitamin D in reducing cancer risk and progression. Nat. Rev. Cancer 2014, 14, 342. [Google Scholar] [CrossRef]
- Jeon, S.-M.; Shin, E.-A. Exploring vitamin D metabolism and function in cancer. Exp. Mol. Med. 2018, 50, 389. [Google Scholar] [CrossRef] [Green Version]
- Berridge, M.J. Vitamin D deficiency and diabetes. Biochem. J. 2017, 474, 1321. [Google Scholar] [CrossRef] [PubMed]
- Martineau, A.R.; Jolliffe, D.A.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Dubnov-Raz, G. Vitamin D supplementation to prevent acute respiratory infections: Individual participant data meta-analysis. Health Technol. Assess. 2019, 23, 23020. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, D.; Yin, K. Vitamin D and inflammatory diseases. J. Inflamm Res. 2014, 12, 63898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, C.E.; Ntambi, J.M. Multiple Sclerosis: Lipids, Lymphocytes, and Vitamin D. Immunometabolism 2020, 10, 19. [Google Scholar] [CrossRef]
- Hewison, M.; Gacad, M.A.; Lemire, J.; Adams, J.S. Vitamin D as a cytokine and hematopoetic factor. Rev. Endocr. Metab. Disord. 2001, 2, 217–227. [Google Scholar] [CrossRef]
- Adams, J.S.; Hewison, M. Update in vitamin D. J. Clin. Endocrinol. Metab. 2010, 95, 471–478. [Google Scholar] [CrossRef] [Green Version]
- Sassi, F.; Tamone, C.; D’Amelio, P. Vitamin D: Nutrient, Hormone, and Immunomodulator. Nutrients 2018, 10, 1656. [Google Scholar] [CrossRef] [Green Version]
- Baeke, F.; Takiishi, T.; Korf, H.; Gysemans, C.; Mathieu, C. Vitamin D: Modulator of the immune system. Curr. Opin. Pharm. 2010, 10, 482. [Google Scholar] [CrossRef]
- Chun, R.F.; Liu, P.T.; Modlin, R.L.; Adams, J.S.; Hewison, M. Impact of vitamin D on immune function: Lessons learned from genome-wide analysis. Front. Physiol. 2014, 11, 151. [Google Scholar] [CrossRef] [Green Version]
- Hansdottir, S.; Monick, M.M.; Hinde, S.L.; Lovan, N.; Look, D.C.; Hunninghake, G.W. Respiratory Epithelial Cells Convert Inactive Vitamin D to Its Active Form: Potential Effects on Host Defense. J. Immunol. 2008, 181, 7090. [Google Scholar] [CrossRef] [Green Version]
- Adams, J.S.; Hewison, M. Unexpected actions of vitamin D: New perspectives on the regulation of innate and adaptive immunity. Nat. Clin. Pract. Endocrinol. Metab. 2008, 4, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chambers, E.S.; Hawrylowicz, C.M. The Impact of Vitamin D on Regulatory T Cells. Curr. Allergy Asthma. Rep. 2010, 11, 29. [Google Scholar] [CrossRef] [PubMed]
- Bishop, E.L.; Ismailova, A.; Dimeloe, S.; Hewison, M.; White, J.H. Vitamin D and Immune Regulation: Antibacterial, Antiviral, Anti-Inflammatory. JBMR Plus 2020, 10, 405. [Google Scholar] [CrossRef]
- Gruber Bzura, B.M. Vitamin D and Influenza—Prevention or Therapy? Int. J. Mol. Sci. 2018, 19, 2419. [Google Scholar] [CrossRef] [Green Version]
- Lowe, K.E.; Maiyar, A.C.; Norman, A.W. Vitamin D-Mediated Gene Expression. 1992. Available online: https://pubmed.ncbi.nlm.nih.gov/1543898/ (accessed on 20 August 2021).
- de Haan, K.; Groeneveld, A.B.J.; de Geus, H.R.H.; Egal, M.; Struijs, A. Vitamin D deficiency as a risk factor for infection, sepsis and mortality in the critically ill: Systematic review and meta-analysis. Crit. Care 2014, 66, 6604. [Google Scholar] [CrossRef] [Green Version]
- Braun, A.; Chang, D.; Mahadevappa, K.; Gibbons, F.K.; Liu, Y.; Giovannucci, E. Association of low serum 25-hydroxyvitamin D levels and mortality in the critically ill. Crit. Care Med. 2011, 39, 671. [Google Scholar] [CrossRef] [Green Version]
- Autier, P.; Boniol, M.; Pizot, C.; Mullie, P. Vitamin D status and ill health: A systematic review. Lancet Diabetes Endocrinol. 2014, 2, 76. [Google Scholar] [CrossRef]
- Zhou, Y.-F.; Luo, B.-A.; Qin, L.-L. The association between vitamin D deficiency and community-acquired pneumonia. Medicine 2019, 98, e17252. [Google Scholar] [CrossRef]
- Goodall, E.C.; Granados, A.C.; Luinstra, K.; Pullenayegum, E.; Coleman, B.L.; Loeb, M. Vitamin D3 and gargling for the prevention of upper respiratory tract infections: A randomized controlled trial. BMC Infect. Dis. 2014, 11, 14273. [Google Scholar] [CrossRef] [Green Version]
- Vanherwegen, A.-S.; Gysemans, C.; Mathieu, C. Regulation of Immune Function by Vitamin D and Its Use in Diseases of Immunity. Endocrinol. Metab. Clin. N. Am. 2017, 46, 1061. [Google Scholar] [CrossRef]
- Greiller, C.; Martineau, A. Modulation of the Immune Response to Respiratory Viruses by Vitamin D. Nutrients 2015, 7, 4240–4270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zdrenghea, M.T.; Makrinioti, H.; Bagacean, C.; Bush, A.; Johnston, S.L.; Stanciu, L.A. Vitamin D modulation of innate immune responses to respiratory viral infections. Rev. Med. Virol. 2016, 27, e1909. [Google Scholar] [CrossRef] [PubMed]
- Sabetta, J.R.; DePetrillo, P.; Cipriani, R.J.; Smardin, J.; Burns, L.A.; Landry, M.L. Serum 25-hydroxyvitamin d and the incidence of acute viral respiratory tract infections in healthy adults. PLoS ONE 2010, 5, e11088. [Google Scholar] [CrossRef]
- Ingham, T.R.; Jones, B.; Camargo, C.A.; Kirman, J.; Dowell, A.C.; Crane, J. Association of vitamin D deficiency with severity of acute respiratory infection: A case-control study in New Zealand children Eur Respir. J. Eur. Respir. Soc. 2014, 44, 124. [Google Scholar]
- FGunville, C.; MMourani, P.; AGinde, A. The role of vitamin D in prevention and treatment of infection. Inflamm. Allergy-Drug Targets 2013, 12, 239–245. [Google Scholar] [CrossRef]
- Khoo, A.L.; Chai, L.; Koenen, H.; Joosten, I.; Netea, M.; van der Ven, A. Translating the role of vitamin D3in infectious diseases. Crit. Rev. Microbiol. 2012, 38, 122. [Google Scholar] [CrossRef]
- Taha, R.; Abureesh, S.; Alghamdi, S.; Hassan, R.Y.; Cheikh, M.M.; Bagabir, R.A. The Relationship Between Vitamin D and Infections Including COVID-19: Any Hopes? Int. J. Gen. Med. 2021, 14, 3849. [Google Scholar] [CrossRef] [PubMed]
- Martineau, A.R.; Jolliffe, D.A.; Hooper, R.L.; Greenberg, L.; Aloia, J.F.; Bergman, P. Vitamin D supplementation to prevent acute respiratory tract infections: Systematic review and meta-analysis of individual participant data. BMJ 2017, 65, 6583. [Google Scholar] [CrossRef] [Green Version]
- Dancer, R.C.A.; Parekh, D.; Lax, S.; D’Souza, V.; Zheng, S.; Bassford, C.R. Vitamin D deficiency contributes directly to the acute respiratory distress syndrome (ARDS). Thorax BMJ 2015, 70, 617. [Google Scholar] [CrossRef] [Green Version]
- Thickett, D.R.; Moromizato, T.; Litonjua, A.A.; Amrein, K.; Quraishi, S.A.; Lee-Sarwar, K.A. Association between prehospital vitamin D status and incident acute respiratory failure in critically ill patients: A retrospective cohort study. BMJ Open Respir. Res. 2015, 2, e74. [Google Scholar] [CrossRef] [Green Version]
- Cantorna, M.T.; Mahon, B.D. D-hormone and the immune system. J. Rheumatol. Suppl. 2005, 76, 11–20. [Google Scholar]
- Antico, A.; Tampoia, M.; Tozzoli, R.; Bizzaro, N. Can supplementation with vitamin D reduce the risk or modify the course of autoimmune diseases? A systematic review of the literature. Autoimmun. Rev. 2012, 12, 127. [Google Scholar] [CrossRef]
- Michigami, T. Rickets/Osteomalacia. Consensus on Vitamin D Deficiency and Insufficiency in Children. Clin. Calcium 2018, 28, 1307–1311. [Google Scholar]
- Grant, W.; Lahore, H.; McDonnell, S.; Baggerly, C.; French, C.; Aliano, J. Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veugelers, P.; Ekwaru, J. A Statistical Error in the Estimation of the Recommended Dietary Allowance for Vitamin D. Nutrients 2014, 6, 4472–4475. [Google Scholar] [CrossRef] [PubMed]
- Papadimitriou, D.T. The Big Vitamin D Mistake. J. Prev. Med. Public Health 2017, 50, 278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Ballegooijen, A.J.; Pilz, S.; Tomaschitz, A.; Grübler, M.R.; Verheyen, N. The Synergistic Interplay between Vitamins D and K for Bone and Cardiovascular Health: A Narrative Review. Int. J. Endocrinol. 2017, 2017, 4376. [Google Scholar] [CrossRef]
- Maresz, K. Proper calcium use: Vitamin K2 as a promoter of bone and cardiovascular health. Integr. Med. A Clin. J. InnoVision Media 2015, 14, 34. [Google Scholar]
- Mandatori, D.; Pelusi, L.; Schiavone, V.; Pipino, C.; Pietro NDi Pandolfi, A. The Dual Role of Vitamin K2 in “Bone-Vascular Crosstalk”: Opposite Effects on Bone Loss and Vascular Calcification. Nutrients 2021, 13, 1222. [Google Scholar] [CrossRef]
- Quesada-Gomez, J.M.; Entrenas-Castillo, M.; Bouillon, R. Vitamin D receptor stimulation to reduce acute respiratory distress syndrome (ARDS) in patients with coronavirus SARS-CoV-2 infections. J. Steroid. Biochem. Mol. Biol. 2020, 202, 105719. [Google Scholar] [CrossRef]
- Mercola, J.; Grant, W.B.; Wagner, C.L. Evidence Regarding Vitamin D and Risk of COVID-19 and Its Severity. Nutrients 2020, 12, 3361. [Google Scholar] [CrossRef] [PubMed]
- Giménez, V.M.M.; Inserra, F.; Tajer, C.D.; Mariani, J.; Ferder, L.; Reiter, R.J. Lungs as target of COVID-19 infection: Protective common molecular mechanisms of vitamin D and melatonin as a new potential synergistic treatment. Life Sci. 2020, 254, 117808. [Google Scholar] [CrossRef]
- Imai, Y.; Kuba, K.; Penninger, J.M. Angiotensin-converting enzyme 2 in acute respiratory distress syndrome. Cell Mol. Life Sci. 2007, 64, 2006. [Google Scholar] [CrossRef]
- Simko, F.; Hrenak, J.; Adamcova, M.; Paulis, L. Renin-Angiotensin-Aldosterone System: Friend or Foe-The Matter of Balance. Insight on History, Therapeutic Implications and {COVID}-19 Interactions. Int. J. Mol. Sci. 2021, 22, 3217. [Google Scholar] [CrossRef] [PubMed]
- Zwart, S.R.; Smith, S.M. Vitamin D and COVID-19: Lessons from Spaceflight Analogs. J. Nutr. 2020, 150, 2624. [Google Scholar] [CrossRef] [PubMed]
- Pouya, F.D.; Rasmi, Y.; Nemati, M.; Asl, E.R. Vitamin D Double-edged Sword Against COVID. Int. J. Infect. 2021, 12, 43. [Google Scholar] [CrossRef]
- Li, Y.C.; Qiao, G.; Uskokovic, M.; Xiang, W.; Zheng, W.; Kong, J. Vitamin D: A negative endocrine regulator of the renin-angiotensin system and blood pressure. J. Steroid. Biochem. Mol. Biol. 2004, 89–90, 387. [Google Scholar] [CrossRef]
- Mahdavi, A.M. A brief review of interplay between vitamin D and angiotensin-converting enzyme 2: Implications for a potential treatment for COVID. Rev. Med. Virol. 2020, 12, 2119. [Google Scholar] [CrossRef]
- Getachew, B.; Tizabi, Y. Vitamin D and COVID-19: Role of ACE2, age, gender, and ethnicity. J. Med. Virol. 2021, 93, 5285. [Google Scholar] [CrossRef]
- de Borst, M.H.; Vervloet, M.G.; ter Wee, P.M.; Navis, G. Cross Talk Between the Renin-Angiotensin-Aldosterone System and Vitamin D-FGF-23-klotho in Chronic Kidney Disease: Figure. J. Am. Soc. Nephrol. 2011, 22, 1603. [Google Scholar] [CrossRef] [Green Version]
- Aygun, H. Vitamin D can prevent COVID-19 infection-induced multiple organ damage. Naunyn Schmiedebergs Arch. Pharmacol. 2020, 393, 1157–1160. [Google Scholar] [CrossRef] [PubMed]
- Malaguarnera, L. Vitamin D3 as Potential Treatment Adjuncts for COVID. Nutrients 2020, 12, 3512. [Google Scholar] [CrossRef] [PubMed]
- Schleithoff, S.S.; Zittermann, A.; Tenderich, G.; Berthold, H.K.; Stehle, P.; Koerfer, R. Vitamin D supplementation improves cytokine profiles in patients with congestive heart failure: A double-blind, randomized, placebo-controlled trial. Am. J. Clin. Nutr. 2006, 83, 754. [Google Scholar] [CrossRef]
- Palmer, M.T.; Lee, Y.K.; Maynard, C.L.; Oliver, J.R.; Bikle, D.D.; Jetten, A.M. Lineage-specific effects of 1, 25-dihydroxyvitamin D3 on the development of effector CD4 T cells. J. Biol Chem. 2011, 286, 997–1004. [Google Scholar] [CrossRef] [Green Version]
- Lemire, J.M.; Archer, D.C.; Beck, L.; Spiegelberg, H.L. Immunosuppressive actions of 1, 25-dihydroxyvitamin D3: Preferential inhibition of Th1 functions. J. Nutr. 1995, 125, 1704S–1708S. [Google Scholar] [PubMed]
- Boonstra, A.; Barrat, F.J.; Crain, C.; Heath, V.L.; Savelkoul, H.F.J.; O’Garra, A. 1$α$, 25-Dihydroxyvitamin D3 has a direct effect on naive CD4+ T cells to enhance the development of Th2 cells. J. Immunol. Am. Assoc. Immnol. 2001, 167, 4974–4980. [Google Scholar] [CrossRef] [Green Version]
- Jeffery, L.E.; Burke, F.; Mura, M.; Zheng, Y.; Qureshi, O.S.; Hewison, M. 1,25-Dihydroxyvitamin D3 and IL-2 Combine to Inhibit T Cell Production of Inflammatory Cytokines and Promote Development of Regulatory T Cells Expressing CTLA-4 and FoxP3. J. Immunol. 2009, 183, 5458. [Google Scholar] [CrossRef] [Green Version]
- Daneshkhah, A.; Agrawal, V.; Eshein, A.; Subramanian, H.; Roy, H.K.; Backman, V. Evidence for possible association of vitamin D status with cytokine storm and unregulated inflammation in COVID-19 patients. Aging Clin. Exp. Res. 2020, 32, 2141–2158. [Google Scholar] [CrossRef]
- Herr, C.; Shaykhiev, R.; Bals, R. The role of cathelicidin and defensins in pulmonary inflammatory diseases. Expert Opin. Biol. 2007, 7, 1449. [Google Scholar] [CrossRef]
- Shahmiri, M.; Enciso, M.; Adda, C.G.; Smith, B.J.; Perugini, M.A.; Mechler, A. Membrane core-specific antimicrobial action of cathelicidin LL-37 peptide switches between pore and nanofibre formation. Sci. Rep. 2016, 6, 38184. [Google Scholar] [CrossRef] [Green Version]
- Liu, P.T.; Stenger, S.; Li, H.; Wenzel, L.; Tan, B.H.; Krutzik, S.R. Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response. Science (80-). Am. Assoc. Adv. Sci. 2006, 311, 1770–1773. [Google Scholar]
- Gombart, A.F.; Borregaard, N.; Koeffler, H.P. Human cathelicidin antimicrobial peptide (CAMP) gene is a direct target of the vitamin D receptor and is strongly up-regulated in myeloid cells by 1,25-dihydroxyvitamin D. FASEB J. 2005, 19, 1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beard, J.A.; Bearden, A.; Striker, R. Vitamin D and the anti-viral state. J. Clin. Virol. 2011, 50, 194. [Google Scholar] [CrossRef] [PubMed]
- Barlow, P.G.; Findlay, E.G.; Currie, S.M.; Davidson, D.J. Antiviral potential of cathelicidins. Future Microbiol. 2014, 9, 55. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; McCullough, P.A.; Tecson, K.M. Vitamin D deficiency in association with endothelial dysfunction: Implications for patients with COVID. Rev. Cardiovasc. Med. 2020, 21, 131. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-H.; Meza, C.A.; Clarke, H.; Kim, J.-S.; Hickner, R.C. Vitamin D and Endothelial Function. Nutrients 2020, 12, 575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sengupta, T.; Majumder, R.; Majumder, S. Role of vitamin D in treating COVID-19-associated coagulopathy: Problems and perspectives. Mol. Cell Biochem. 2021, 476, 2421–2427. [Google Scholar] [CrossRef]
- Mohammad, S.; Mishra, A.; Ashraf, M.Z. Emerging role of vitamin D and its associated molecules in pathways related to pathogenesis of thrombosis. Biomolecules 2019, 9, 649. [Google Scholar] [CrossRef] [Green Version]
- Levi, M.; Thachil, J.; Iba, T.; Levy, J.H. Coagulation abnormalities and thrombosis in patients with COVID. Lancet Haematol. 2020, 7, e438–e440. [Google Scholar] [CrossRef]
- Abrishami, A.; Dalili, N.; Torbati, P.M.; Asgari, R.; Arab-Ahmadi, M.; Behnam, B. Possible association of vitamin D status with lung involvement and outcome in patients with COVID-19: A retrospective study. Eur. J. Nutr. 2021, 60, 2249–2257. [Google Scholar] [CrossRef]
- Smet, D.; Smet, K.; Herroelen, P.; Gryspeerdt, S.; Martens, G.A. Serum 25(OH)D Level on Hospital Admission Associated With COVID-19 Stage and Mortality. Am. J. Clin. Pathol. 2020, 155, 381. [Google Scholar] [CrossRef]
- Vanegas-Cedillo, P.E.; Bello-Chavolla, O.Y.; Ramirez-Pedraza, N.; Encinas, B.R.; Carrión, C.I.P.; Ávila, M.I.J. Serum Vitamin D levels are associated with increased COVID-19 severity and mortality independent of visceral adiposity. Cold Spring Harb. Lab. 2021, 12, 3490. [Google Scholar] [CrossRef]
- Carpagnano, G.E.; Lecce VDi Quaranta, V.N.; Zito, A.; Buonamico, E.; Capozza, E. Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID. J. Endocrinol. Investig. 2020, 44, 765. [Google Scholar] [CrossRef] [PubMed]
- Pizzini, A.; Aichner, M.; Sahanic, S.; Böhm, A.; Egger, A.; Hoermann, G. Impact of Vitamin D Deficiency on COVID-19—A Prospective Analysis from the CovILD Registry. Nutrients 2020, 12, 2775. [Google Scholar] [CrossRef] [PubMed]
- Lau, F.H.; Majumder, R.; Torabi, R.; Saeg, F.; Hoffman, R.; Cirillo, J.D. Vitamin D insufficiency is prevalent in severe COVID-19. Cold Spring Harb. Lab. 2020, 11, 5838. [Google Scholar] [CrossRef]
- Luo, X.; Liao, Q.; Shen, Y.; Li, H.; Cheng, L. Vitamin D Deficiency Is Associated with COVID-19 Incidence and Disease Severity in Chinese People. J. Nutr. 2020, 151, 98. [Google Scholar] [CrossRef] [PubMed]
- Vassiliou, A.G.; Jahaj, E.; Pratikaki, M.; Keskinidou, C.; Detsika, M.; Grigoriou, E.; Psarra, K.; Orfanos, S.E.; Tsirogianni, A. Vitamin D deficiency correlates with a reduced number of natural killer cells in intensive care unit (ICU) and non-ICU patients with COVID-19 pneumonia. Hell. J. Cardiol. 2020, 11, 241. [Google Scholar]
- Meltzer, D.O.; Best, T.J.; Zhang, H.; Vokes, T.; Arora, V.; Solway, J. Association of Vitamin D Status and Other Clinical Characteristics with COVID-19 Test Results. JAMA Netw. Open 2020, 3, e19722. [Google Scholar] [CrossRef]
- Kaufman, H.W.; Niles, J.K.; Kroll, M.H.; Bi, C.; Holick, M.F. SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels. PLoS ONE 2020, 15, 1252. [Google Scholar] [CrossRef]
- Merzon, E.; Tworowski, D.; Gorohovski, A.; Vinker, S.; Cohen, A.G.; Green, I. Low plasma 25(OH) vitamin D level is associated with increased risk of COVID-19 infection: An Israeli population-based study. FEBS J. 2020, 287, 3693. [Google Scholar] [CrossRef]
- D’Avolio, A.; Avataneo, V.; Manca, A.; Cusato, J.; Nicolò ADe Lucchini, R. 25-Hydroxyvitamin D Concentrations Are Lower in Patients with Positive PCR for SARS-CoV. Nutrients 2020, 12, 1359. [Google Scholar] [CrossRef] [PubMed]
- Radujkovic, A.; Hippchen, T.; Tiwari-Heckler, S.; Dreher, S.; Boxberger, M.; Merle, U. Vitamin D Deficiency and Outcome of COVID-19 Patients. Nutrients 2020, 12, 2757. [Google Scholar] [CrossRef]
- Gavioli, E.M.; Miyashita, H.; Hassaneen, O.; Siau, E. An Evaluation of Serum 25-Hydroxy Vitamin D Levels in Patients with COVID-19 in New York City. J. Am. Coll. Nutr. 2021, 1, 9626. [Google Scholar] [CrossRef]
- Szeto, B.; Zucker, J.E.; LaSota, E.D.; Rubin, M.R.; Walker, M.D.; Yin, M.T. Vitamin D Status and COVID-19 Clinical Outcomes in Hospitalized Patients. Endocr. Res. 2020, 46, 66. [Google Scholar] [CrossRef] [PubMed]
- Ohaegbulam, K.C.; Swalih, M.; Patel, P.; Smith, M.A.; Perrin, R. Vitamin D supplementation in COVID-19 patients: A clinical case series. Am. J. Ther. 2020, 11, e485. [Google Scholar] [CrossRef]
- Rastogi, A.; Bhansali, A.; Khare, N.; Suri, V.; Yaddanapudi, N.; Sachdeva, N. Short term, high-dose vitamin D supplementation for COVID-19 disease: A randomised, placebo-controlled, study (SHADE study). Postgrad. Med. J. 2020, 2020, 139065. [Google Scholar] [CrossRef]
- Annweiler, G.; Corvaisier, M.; Gautier, J.; Dubée, V.; Legrand, E.; Sacco, G. Vitamin D Supplementation Associated to Better Survival in Hospitalized Frail Elderly COVID-19 Patients: The GERIA-COVID Quasi-Experimental Study. Nutrients 2020, 12, 3377. [Google Scholar] [CrossRef] [PubMed]
- Han, J.E.; Jones, J.L.; Tangpricha, V.; Brown, M.A.; Hao, L.; Hebbar, G. High dose vitamin D administration in ventilated intensive care unit patients: A pilot double blind randomized controlled trial. J. Clin. Transl. Endocrinol. 2016, 4, 59. [Google Scholar] [CrossRef] [Green Version]
- Panagiotou, G.; Tee, S.A.; Ihsan, Y.; Athar, W.; Marchitelli, G.; Kelly, D. Low serum 25-hydroxyvitamin D (25[OH]D) levels in patients hospitalized with COVID-19 are associated with greater disease severity. Clin. Endocrinol. 2020, 93, 508. [Google Scholar] [CrossRef]
- Castillo, M.E.; Costa, L.M.E.; Barrios, J.M.V.; Díaz, J.F.A.; Miranda, J.L.; Bouillon, R. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. J. Steroid. Biochem. Mol. Biol. 2020, 203, 105751. [Google Scholar] [CrossRef]
- Annweiler, C.; Hanotte, B.; de l’Eprevier, C.G.; Sabatier, J.-M.; Lafaie, L.; Célarier, T. Vitamin D and survival in COVID-19 patients: A quasi-experimental study. J. Steroid. Biochem. Mol. Biol. 2020, 204, 105771. [Google Scholar] [CrossRef]
- Zemb, P.; Bergman, P.; Camargo, C.A.; Cavalier, E.; Cormier, C.; Courbebaisse, M. Vitamin D deficiency and the COVID-19 pandemic. J. Glob. Antimicrob. Resist. 2020, 22, 133. [Google Scholar] [CrossRef] [PubMed]
- Laird, E.; Rhodes, J.; Kenny, R.A. Vitamin D and inflammation: Potential implications for severity of COVID-19. Ir. Med. J. 2020, 113, 81. [Google Scholar] [PubMed]
- McCartney, D.M.; O’Shea, P.M.; Faul, J.L.; Healy, M.J.; Byrne, G.; Griffin, T.P. Vitamin D and SARS-CoV-2 infection—evolution of evidence supporting clinical practice and policy development. Ir. J. Med. Sci. 2020, 190, 1253. [Google Scholar] [CrossRef]
- Benskin, L.L. A Basic Review of the Preliminary Evidence That COVID-19 Risk and Severity Is Increased in Vitamin D Deficiency. Front. Public Health 2020, 11, 513. [Google Scholar] [CrossRef]
- Silva, M.C.; Furlanetto, T.W. Does serum 25-hydroxyvitamin D decrease during acute-phase response? A systematic review. Nutr. Res. 2015, 35, 91. [Google Scholar] [CrossRef]
- Annweiler, C.; Cao, Z.; Sabatier, J.-M. Point of view: Should COVID-19 patients be supplemented with vitamin D? Maturitas 2020, 140, 24. [Google Scholar] [CrossRef]
- Antonelli, M.; Kushner, I. Low Serum Levels of 25-hydroxyvitamin D Accompany Severe COVID-19 because it is a Negative Acute Phase Reactant. Am. J. Med. Sci. 2021, 14, 2546. [Google Scholar]
- Ahmad, A.; Heumann, C.; Ali, R.; Oliver, T. Mean Vitamin D levels in 19 European Countries & COVID-19 Mortality over 10 months. Cold Spring Harb. Lab. 2021, 11, 361. [Google Scholar] [CrossRef]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Porcher, S. Response2covid19, a dataset of governments’ responses to COVID-19 all around the world. Sci. Data 2020, 11, 757. [Google Scholar] [CrossRef]
- Ilie, P.C.; Stefanescu, S.; Smith, L. The role of Vitamin D in the prevention of coronavirus disease 2019 infection and mortality. Aging Clin. Exp. Res. 2020, 32, 1195. [Google Scholar] [CrossRef] [PubMed]
- Pal, R.; Banerjee, M.; Bhadada, S.K.; Shetty, A.J.; Singh, B.; Vyas, A. Vitamin D supplementation and clinical outcomes in COVID-19: A systematic review and meta-analysis. J. Endocrinol. Investig. 2021, 14, 618. [Google Scholar] [CrossRef]
- Nikniaz, L.; Akbarzadeh, M.A.; Hosseinifard, H.; Hosseini, M.-S. The impact of vitamin D supplementation on mortality rate and clinical outcomes of COVID-19 patients: A systematic review and meta-analysis. Cold Spring Harb. Lab. 2021, 11, 219. [Google Scholar] [CrossRef]
- Hariyanto, T.I.; Intan, D.; Hananto, J.E.; Harapan, H.; Kurniawan, A. Vitamin D supplementation and Covid-19 outcomes: A systematic review, meta-analysis and meta-regression. Rev. Med. Virol. 2021, 11, 2269. [Google Scholar] [CrossRef]
- Kazemi, A.; Mohammadi, V.; Aghababaee, S.K.; Golzarand, M.; Clark, C.C.T.; Babajafari, S. Association of Vitamin D Status with SARS-CoV-2 Infection or COVID-19 Severity: A Systematic Review and Meta-analysis. Adv. Nutr. 2021, 10, 12. [Google Scholar] [CrossRef]
- Munshi, R.; Hussein, M.H.; Toraih, E.A.; Elshazli, R.M.; Jardak, C.; Sultana, N. Vitamin D insufficiency as a potential culprit in critical COVID-19 patients. J. Med. Virol. 2020, 93, 733. [Google Scholar] [CrossRef]
- Crafa, A.; Cannarella, R.; Condorelli, R.A.; Mongioì, L.M.; Barbagallo, F.; Aversa, A. Influence of 25-hydroxy-cholecalciferol levels on SARS-CoV-2 infection~and COVID-19 severity: A systematic review and meta-analysis. EClinicalMedicine 2021, 37, 124. [Google Scholar] [CrossRef]
- Teshome, A.; Adane, A.; Girma, B.; Mekonnen, Z.A. The Impact of Vitamin D Level on {COVID}-19 Infection: Systematic Review and Meta-Analysis. Front. Public Health 2021, 11, 559. [Google Scholar] [CrossRef]
- CADTH. CADTH COVID-19 Search Strings. 2020. Available online: https://covid.cadth.ca/literature-searching-tools/cadth-covid-19-search-strings/ (accessed on 13 April 2020).
- COVID-19 Risk Estimator. Available online: https://github.com/TheEconomist/covid-19-risk-estimator (accessed on 30 July 2021).
- Ricci, A.; Pagliuca, A.; D’Ascanio, M.; Innammorato, M.; De Vitis, C.; Mancini, R. Circulating Vitamin D levels status and clinical prognostic indices in COVID-19 patients. Respir. Res. 2021, 22, 166. [Google Scholar] [CrossRef]
- Bennouar, S.; Cherif, A.B.; Kessira, A.; Bennouar, D.E.; Abdi, S. Vitamin D Deficiency and Low Serum Calcium as Predictors of Poor Prognosis in Patients with Severe COVID. J. Am. Coll. Nutr. 2020, 40, 104. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 11, 372. [Google Scholar]
- Haddaway, N.R.; McGuinness, L.A. PRISMA2020: R package and ShinyApp for producing PRISMA 2020 compliant flow diagrams (Version 0.0.1). Zenodo 2020, 11, 835. [Google Scholar] [CrossRef]
- Angelidi, A.M.; Belanger, M.J.; Lorinsky, M.K.; Karamanis, D.; Chamorro-Pareja, N.; Ognibene, J. Vitamin D Status is Associated With In-hospital Mortality and Mechanical Ventilation: A Cohort of COVID-19 Hospitalized Patients. Mayo Clin. Proc. 2021, 11, 1145. [Google Scholar] [CrossRef]
- Charoenngam, N.; Shirvani, A.; Reddy, N.; Vodopivec, D.M.; Apovian, C.M.; Holick, M.F. Association of Vitamin D Status With Hospital Morbidity and Mortality in Adult Hospitalized COVID-19 Patients With COVID. Endocr. Pract. 2021, 11, 145. Available online: http://www.ncbi.nlm.nih.gov/pubmed/33705975 (accessed on 27 March 2021).
- Susianti, H.; Wahono, C.S.; Rahman, P.A.; Pratama, M.Z.; Wulanda, I.A.; Hartanti, K.D. Low Levels of Vitamin D were Associated with Coagulopathy Among Hospitalized Coronavirus Disease-19 (COVID-19) Patients: A Single-Centered Study in Indonesia. J. Med. Biochem. 2021, 11, 1–10. [Google Scholar]
- IDF. IDF Diabetes Atlas, 9th Edition 2019. 2019. Available online: https://www.diabetesatlas.org/en/ (accessed on 3 August 2021).
- UN. Population Interpolated by Single Age and Single Year. 2019. Available online: https://population.un.org/wpp/Download/Standard/CSV/ (accessed on 10 April 2021).
- Butt, A.A.; Nafady-Hego, H.; Chemaitelly, H.; Abou-Samra, A.-B.; Khal AAl Coyle, P.V. Outcomes Among Patients with Breakthrough SARS-CoV-2 Infection After Vaccination. Int. J. Infect. Dis. 2021, 110, 353. [Google Scholar] [CrossRef]
- Birhane, M.; Bressler, S.; Chang, G.; Clark, T.; Dorough, L.; Fischer, M. COVID-19 Vaccine Breakthrough Infections Reported to CDC–United States, January 1–April 30. MMWR Morb. Mortal. Wkly Rep. 2021, 70, 792. [Google Scholar] [CrossRef]
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J. Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis. J. Infect. 2020, 81, e16. [Google Scholar] [CrossRef]
- Murdaca, G.; Tonacci, A.; Negrini, S.; Greco, M.; Borro, M.; Puppo, F. Emerging role of vitamin D in autoimmune diseases: An update on evidence and therapeutic implications. Autoimmun. Rev. 2019, 18, 2350. [Google Scholar] [CrossRef]
- Yang, C.-Y.; Leung, P.S.C.; Adamopoulos, I.E.; Gershwin, M.E. The Implication of Vitamin D and Autoimmunity: A Comprehensive Review. Clin. Rev. Allergy Immunol. 2013, 45, 217. [Google Scholar] [CrossRef]
- Stanhope, K.L. Sugar consumption, metabolic disease and obesity: The state of the controversy. Crit. Rev. Clin. Lab. Sci. 2015, 53, 52. [Google Scholar] [CrossRef]
- Sekine, T.; Perez-Potti, A.; Rivera-Ballesteros, O.; Strålin, K.; Gorin, J.-B.; Olsson, A. Robust T Cell Immunity in Convalescent Individuals with Asymptomatic or Mild COVID-19. Cell 2020, 183, 158–168. [Google Scholar] [CrossRef]
- Worldometer, F.A.Q. Worldometer. 2021. Available online: https://www.worldometers.info/faq/ (accessed on 23 August 2021).
- Reis, B.Z.; Fernandes, A.L.; Sales, L.P.; Santos, M.D.; Dos~Santos, C.C.; Pinto, A.J. Influence of vitamin D status on hospital length of stay and prognosis in hospitalized patients with moderate to severe COVID-19: A multicenter prospective cohort study. Am. J. Clin. Nutr. 2021, 114, 598. [Google Scholar] [CrossRef]
- Zhang, Y.; Leung, D.Y.M.; Richers, B.N.; Liu, Y.; Remigio, L.K.; Riches, D.W. Vitamin D inhibits monocyte/macrophage proinflammatory cytokine production by targeting MAPK phosphatase. J. Immunol. Am. Assoc. Immnol. 2012, 188, 2127–2135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luxwolda, M.F.; Kuipers, R.S.; Kema, I.P.; Dijck-Brouwer, D.A.J.; Muskiet, F.A.J. Traditionally living populations in East Africa have a mean serum 25-hydroxyvitamin D concentration of 115 nmol/L. Br. J. Nutr. 2012, 108, 1557–1561. [Google Scholar] [CrossRef] [Green Version]
- Afshar, P.; Ghaffaripour, M.; Sajjadi, H. Suggested Role of Vitamin D Supplementation in COVID-19 Severity. 2020. Available online: http://www.jocms.org/index.php/jcms/article/view/822 (accessed on 20 August 2021).
- Vukić, M.; Neme, A.; Seuter, S.; Saksa, N.; De Mello, V.D.F.; Nurmi, T. Relevance of vitamin D receptor target genes for monitoring the vitamin D responsiveness of primary human cells. PLoS ONE 2015, 10, e0124339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Mendel, J.; Borsche, L. COVID-19 mortality risk correlates inversely with vitamin D3 status, mortality close to zero could theoretically be achieved at 50 ng/ml 25(OH)D3: Results of a systematic review and meta-analysis. Harv. Dataverse 2020, 11, 147. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source | Search Strategy | Time Frame |
|---|---|---|
| PubMed | COVID-19 Search String from [153] AND (“vitamin d” or “d3” or “25(OH)D” or “25-hydroxyvitamin D”) | 1 November 2019–27 March 2021 |
| https://c19vitamind.com (accessed on 27 March 2021) | Restriction to category “Levels” | 1 November 2019–27 March 2021 |
| Author | Reference | Cohort | No. of Patients | Laboratory Results Recorded Pre-/Post-Infection | Mortality | Vitamin D Level [ng/mL] |
|---|---|---|---|---|---|---|
| Ahmad et al., 2021 | [142] | 19 European countries | 448,785,546 | Up to 10 months in advance | Refer to source study | |
| Angelidi et al., 2021 | [159] | <30 ng/mL | 79 | Within 1 day after admission | 25.30% | NR a Median (IQR): 28 ng/mL (16.80–39.00 ng/mL) |
| ≥30 ng/mL | 65 | 9.20% | ||||
| Charoenngam et al., 2021 | [160] | <20 ng/mL | 96 | Up to 1 year in advance | 14.58% | NR a |
| 20–30 ng/mL | 91 | 16.48% | ||||
| ≥30 ng/mL | 100 | 12.00% | ||||
| Gavioli et al., 2021 | [126] | Deficient | 177 | Up to 3 months in advance | 29.00% | 14.00 31.00 |
| Sufficient | 260 | 31.00% | ||||
| Susianti et al., 2021 | [161] | <49.92 nmol/L | 42 | Within 1 day after admission | 45.00% | 8.00 28.40 |
| ≥49.92 nmol/L | 8 | 42.00% | ||||
| Szeto et al., 2021 | [127] | <20 ng/mL | 35 | Up to 12 months in advance | 23.00% | 16.00 32.00 |
| ≥20 ng/mL | 58 | 24.00% | ||||
| Vanegas-Cedillo et al., 2021 | [115] | ≤20 ng/mL | 251 | Within 1 day after admission | 23.50% | NR a Mean ± SD 21.78 ± 9.01 ng/ml |
| >20 ng/mL | 300 | 19.00% | ||||
| Vassiliou, 2020 | [120] | ≤19.9 ng/mL | 32 | Within 1 day after admission | 25.00% | NR a |
| 20–29.9 ng/mL | 7 | 14.30% | ||||
| Method | Reference | Resulting Pearson Correlation CMR~D3 |
|---|---|---|
| None | – | r(17) = −0.4154, p = 0.0770 |
| Two most extreme outliers removed | – | r(15) = −0.3471, p = 0.1722 |
| Rigidity of public health measures | [144] | r(17) = −0.4662, p = 0.0442 |
| Sex/age distribution, diabetes | [162,163] | r(17) = −0.5113, p = 0.0253 |
| Expected SARS-COV-2 positive rate for given D3 level | [122] | r(17) = −0.5997, p = 0.0066 |
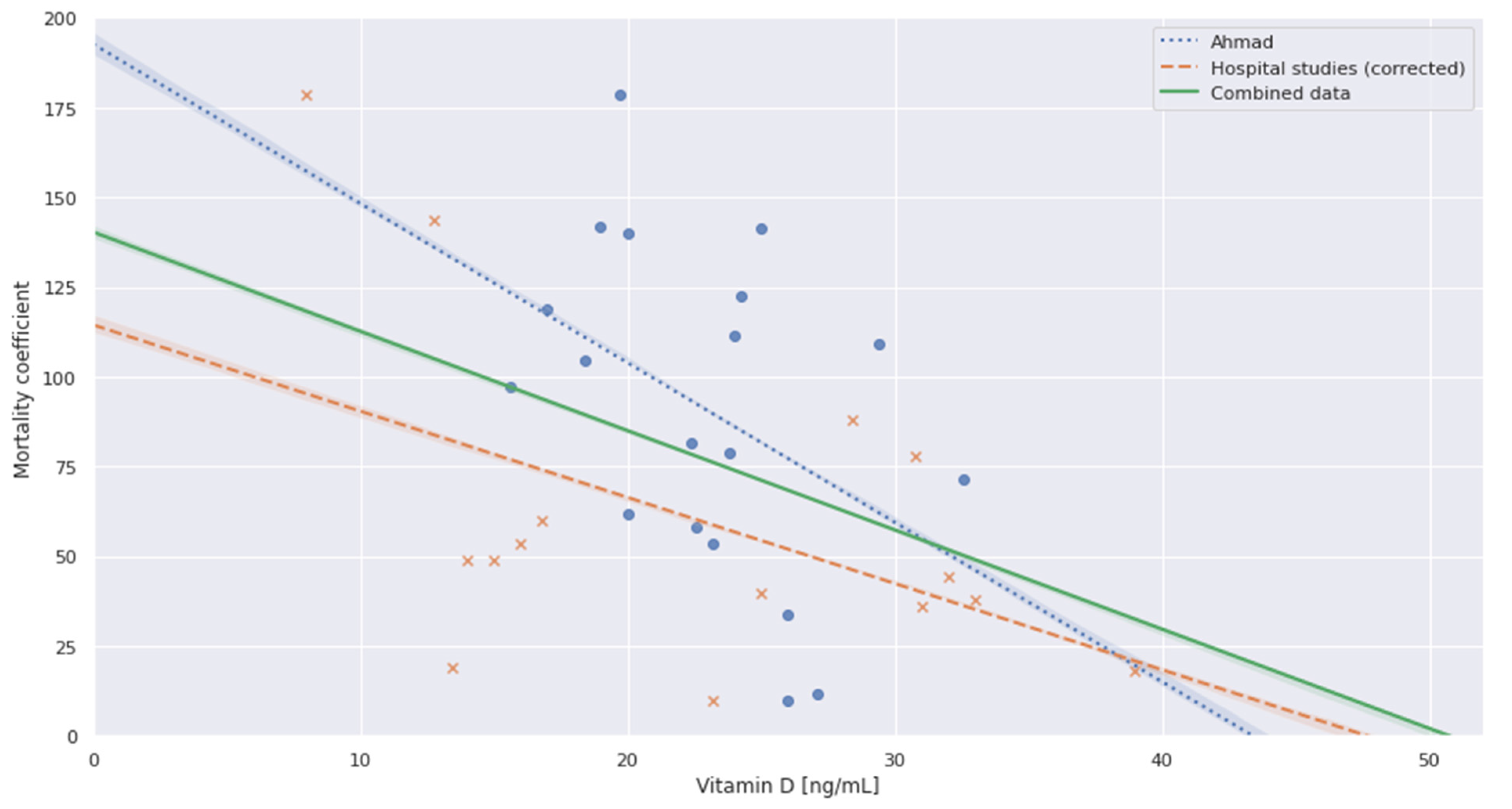
| Ahmad | Hospital Studies (Corrected) | Combined | |
|---|---|---|---|
| Pearson correlation (Mortality~Vit D) | r(17) = −0.4154, p = 0.0770 | r(13) = −0.4886, p = 0.0646 | r(32) = −0.3989, p = 0.0194 |
| Spearman correlation (Mortality~Vit D) | rs = −0.4300, p = 0.0661, N = 19 | rs = −0.469, p = 0.0786, N = 15 | rs = −0.3698, p = 0.03136, N = 34 |
| Ahmad | Hospital Studies (Corrected) | Combined | |
|---|---|---|---|
| Intercept | 192.6788 | 114.4156 | 140.2880 |
| Coefficient | −4.4408 | −2.4015 | −2.7654 |
| R2 | 0.173 | 0.239 | 0.159 |
| Adj. R2 | 0.124 | 0.180 | 0.133 |
| Prob (F-Statistic) | 0.0770 | 0.0646 | 0.0194 |
| AIC | 1980.7 | 1560.5 | 3560.8 |
| BIC | 2000.6 | 1580.0 | 3590.8 |
| Prob (Omnibus) | 0.342 | 0.568 | 0.436 |
| Durbin-Watson | 10.238 | 10.514 | 10.217 |
| Prob (Jarque-Bera) | 0.591 | 0.662 | 0.572 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borsche, L.; Glauner, B.; von Mendel, J. COVID-19 Mortality Risk Correlates Inversely with Vitamin D3 Status, and a Mortality Rate Close to Zero Could Theoretically Be Achieved at 50 ng/mL 25(OH)D3: Results of a Systematic Review and Meta-Analysis. Nutrients 2021, 13, 3596. https://doi.org/10.3390/nu13103596
Borsche L, Glauner B, von Mendel J. COVID-19 Mortality Risk Correlates Inversely with Vitamin D3 Status, and a Mortality Rate Close to Zero Could Theoretically Be Achieved at 50 ng/mL 25(OH)D3: Results of a Systematic Review and Meta-Analysis. Nutrients. 2021; 13(10):3596. https://doi.org/10.3390/nu13103596
Chicago/Turabian StyleBorsche, Lorenz, Bernd Glauner, and Julian von Mendel. 2021. "COVID-19 Mortality Risk Correlates Inversely with Vitamin D3 Status, and a Mortality Rate Close to Zero Could Theoretically Be Achieved at 50 ng/mL 25(OH)D3: Results of a Systematic Review and Meta-Analysis" Nutrients 13, no. 10: 3596. https://doi.org/10.3390/nu13103596
APA StyleBorsche, L., Glauner, B., & von Mendel, J. (2021). COVID-19 Mortality Risk Correlates Inversely with Vitamin D3 Status, and a Mortality Rate Close to Zero Could Theoretically Be Achieved at 50 ng/mL 25(OH)D3: Results of a Systematic Review and Meta-Analysis. Nutrients, 13(10), 3596. https://doi.org/10.3390/nu13103596