
Dietary Fibre Intake in Relation to Asthma, Rhinitis and Lung Function Impairment—A Systematic Review of Observational Studies



Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Search Strategy
2.5. Study Selection
2.6. Data Extraction
2.7. Risk of Bias in Individual Studies
2.8. Presentation/Synthesis of Results
2.9. Risk of Bias across Studies
3. Results
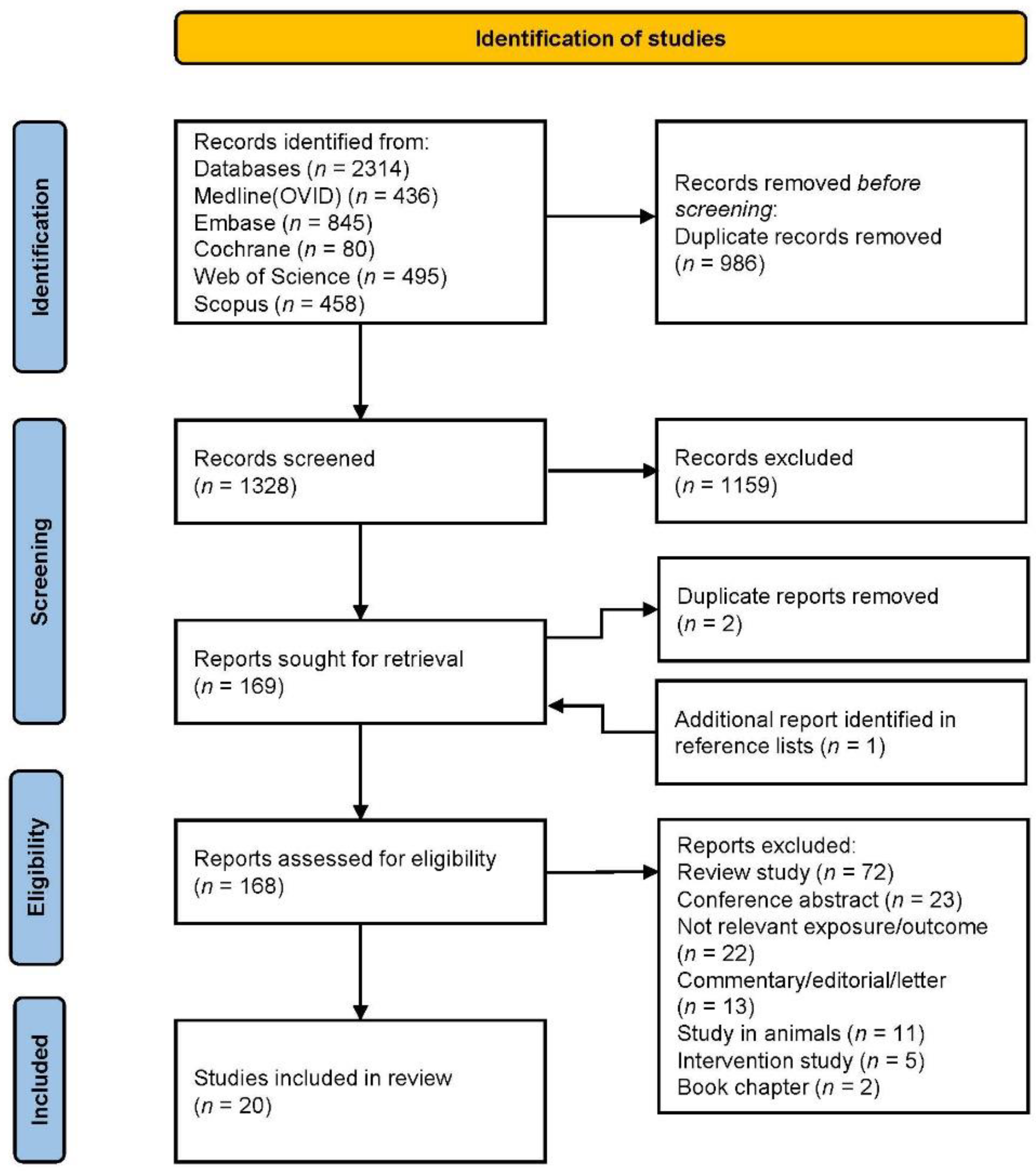
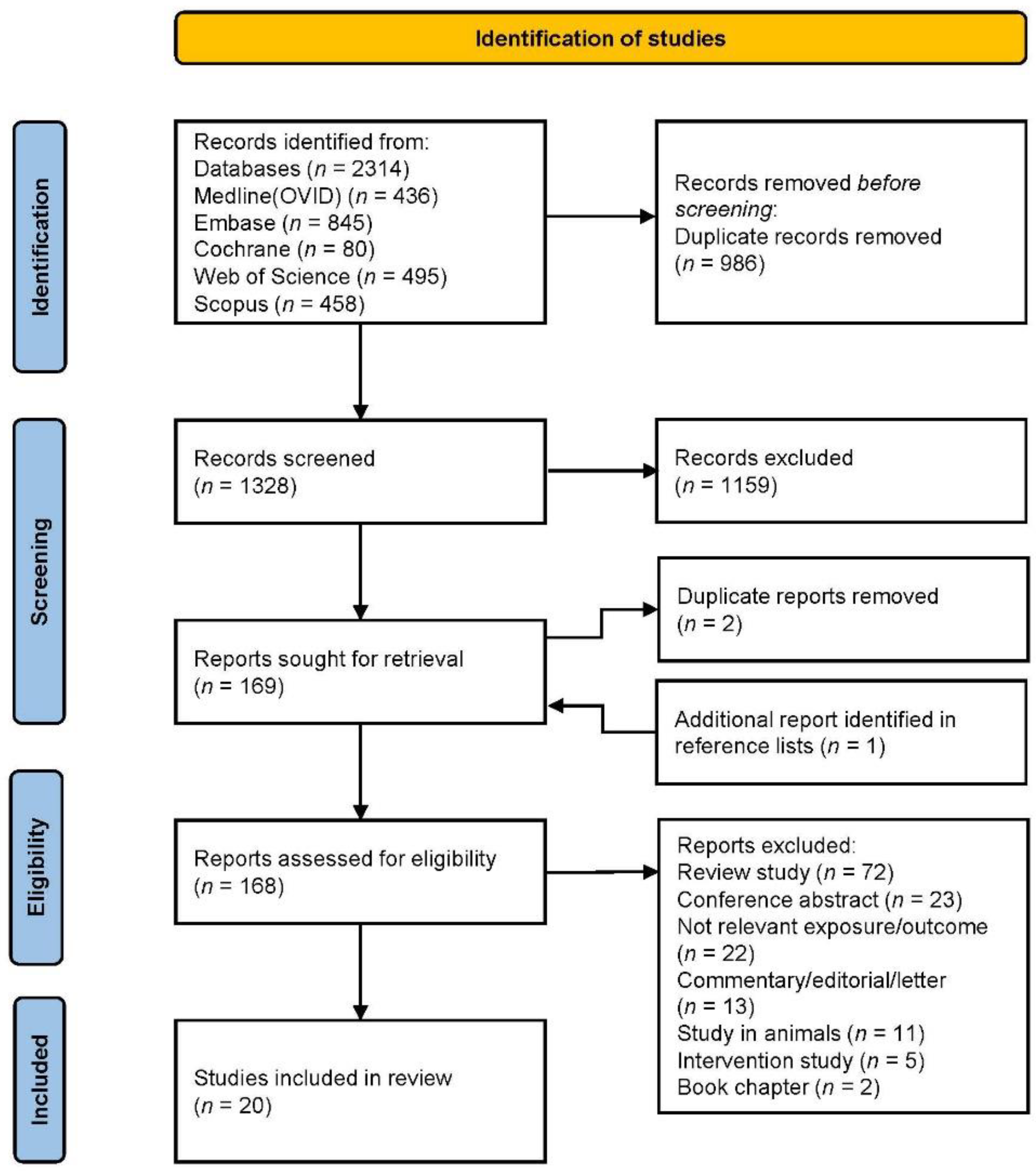
3.1. Study Selection
3.2. Study Characteristics
3.3. Results of Individual Studies
3.3.1. Maternal Fibre Intake during Pregnancy
3.3.2. Fibre Intake during Childhood
3.3.3. Fibre Intake during Adulthood
Asthma, Rhinitis and Related Symptoms
COPD and Related Symptoms
Lung Function
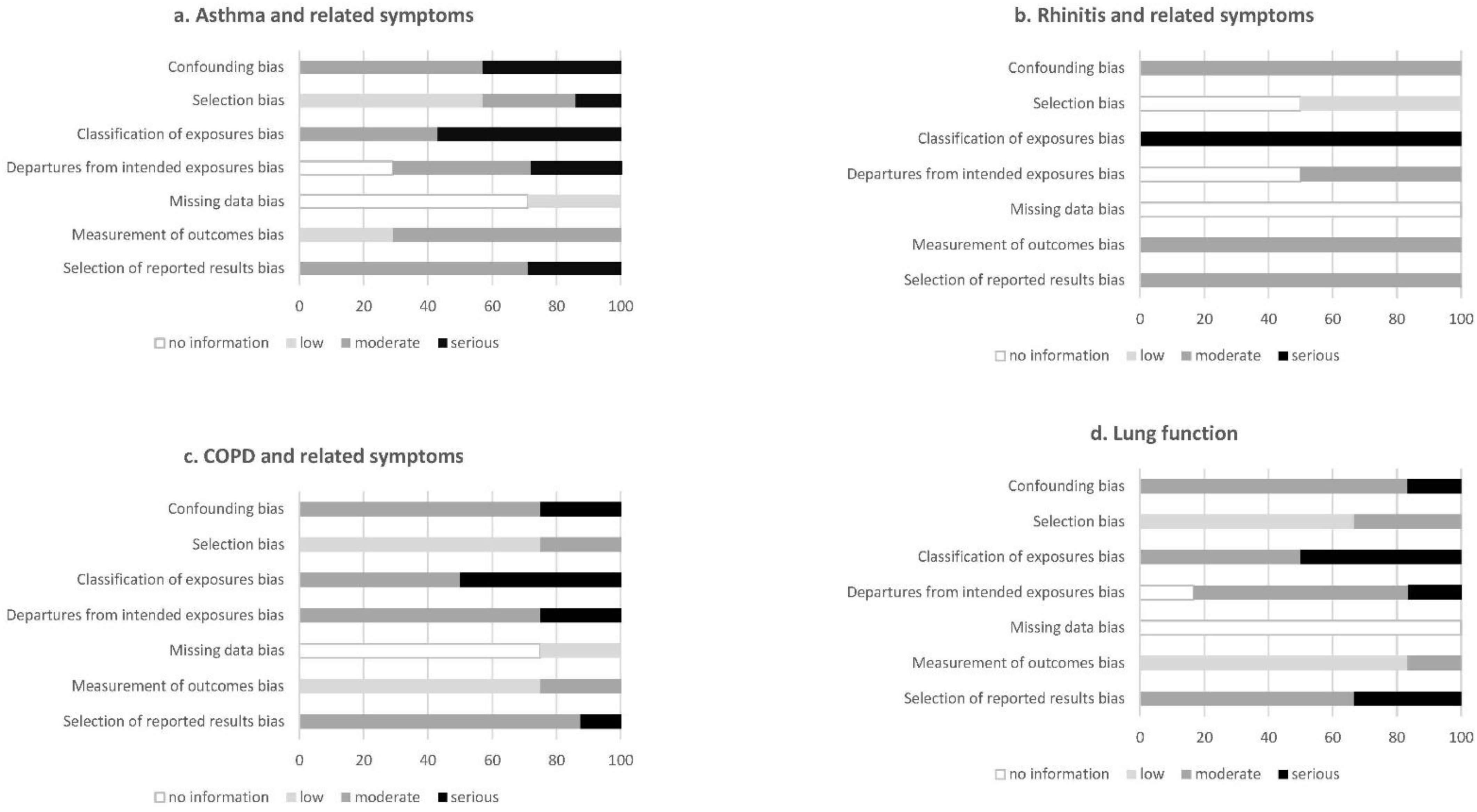
3.4. Quality of Studies
3.4.1. Asthma and Related Symptoms
3.4.2. Rhinitis and Related Symptoms
3.4.3. COPD and Related Symptoms
3.4.4. Lung Function
3.5. Strength of the Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Veronese, N.; Solmi, M.; Caruso, M.G.; Giannelli, G.; Osella, A.R.; Evangelou, E.; Maggi, S.; Fontana, L.; Stubbs, B.; Tzoulaki, I. Dietary fiber and health outcomes: An umbrella review of systematic reviews and meta-analyses. Am. J. Clin. Nutr. 2018, 107, 436–444. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.; Subar, A.; Hollenbeck, A.; Schatzkin, A. Dietary fiber intake and mortality in the NIH-AARP diet and health study. Arch. Intern. Med. 2011, 171, 1061–1068. [Google Scholar] [CrossRef] [Green Version]
- Chuang, S.-C.; Norat, T.; Murphy, N.; Olsen, A.; Tjonneland, A.; Overvad, K.; Boutron-Ruault, M.C.; Perquier, F.; Dartois, L.; Kaaks, R.; et al. Fiber intake and total and cause-specific mortality in the European Prospective Investigation into Cancer and Nutrition cohort. Am. J. Clin. Nutr. 2012, 96, 164–174. [Google Scholar] [CrossRef]
- Dreher, M. Whole Fruits and Fruit Fiber Emerging Health Effects. Nutrients 2018, 10, 1833. [Google Scholar] [CrossRef] [Green Version]
- Global Asthma Network. The Global Asthma Report; Auckland, New Zealand, 2018; Available online: http://globalasthmareport.org/ (accessed on 8 September 2021).
- Melén, E.; Guerra, S.; Hallberg, J.; Jarvis, D.; Stanojevic, S. Linking COPD epidemiology with pediatric asthma care: Implications for the patient and the physician. Pediatr. Allergy Immunol. 2019, 30, 589–597. [Google Scholar] [CrossRef]
- Ballardini, N.; Kull, I.; Lind, T.; Hallner, E.; Almqvist, C.; Ostblom, E.; Melén, E.; Pershagen, G.; Lilja, G.; Bergström, A.; et al. Development and comorbidity of eczema, asthma and rhinitis to age 12: Data from the BAMSE birth cohort. Allergy 2012, 67, 537–544. [Google Scholar] [CrossRef] [Green Version]
- Gibson, G.; Loddenkemper, R.; Sibille, Y.; Lundbäck, B. Childhood Asthma. European Lung White Book, 2nd ed.; European Respiratory Society: Sheffield, UK, 2013; pp. 126–137. [Google Scholar]
- McKenzie, C.; Tan, J.; Macia, L.; Mackay, C.R. The nutrition-gut microbiome-physiology axis and allergic diseases. Immunol. Rev. 2017, 278, 277–295. [Google Scholar] [CrossRef]
- Alwarith, J.; Kahleova, H.; Crosby, L.; Brooks, A.; Brandon, L.; Levin, S.M.; Barnard, N.D. The role of nutrition in asthma prevention and treatment. Nutr. Rev. 2020, 78, 928–938. [Google Scholar] [CrossRef] [Green Version]
- Palafox-Carlos, H.; Ayala-Zavala, J.; González-Aguilar, G. The role of dietary fiber in the bioaccessibility and bioavailability of fruit and vegetable antioxidants. J. Food Sci. 2011, 76, R6–R15. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372n71. [Google Scholar] [CrossRef]
- Nutrition Evidence Systematic Review. Risk of Bias for Nutrition Observational Studies (RoB-NObs) Tool. 2019. Available online: https://nesr.usda.gov/sites/default/files/2019-07/RiskOfBiasForNutritionObservationalStudies-RoB-NObs.pdf (accessed on 8 September 2021).
- World Cancer Research Fund, American Institute for Cancer Research. Judging the evidence. In Continuous Update Project Report; World Cancer Research Fund: London, UK, 2018. [Google Scholar]
- Arnesen, E.K.; Christensen, J.J.; Andersen, R.; Eneroth, H.; Erkkola, M.; Høyer, A.; Lemming, E.W.; Meltzer, H.M.; Þórhallsson, I.; Þórsdóttir, I.; et al. The Nordic Nutrition Recommendations 2022—Handbook for qualified systematic reviews. Food Nutr. Res. 2020, 64. [Google Scholar] [CrossRef]
- Pretorius, R.A.; Bodinier, M.; Prescott, S.L.; Palmer, D.J. Maternal Fiber Dietary Intakes during Pregnancy and Infant Allergic Disease. Nutrients 2019, 11, 1767. [Google Scholar] [CrossRef] [Green Version]
- Wood, L.G.; Lagleva, M.; Shah, S.; Berthon, B.S.; Galbraith, S.; Henry, R.; Kepreotes, H.; Gibson, P.G. Dietary changes in migrant adolescents with increasing length of stay in Australia and associated risk of wheeze—A retrospective, cross sectional study. BMC Pediatr. 2015, 15, 102. [Google Scholar] [CrossRef] [Green Version]
- Vaccaro, J.A.; Niego, J.; Huffman, F.G. Dietary factors, body weight, and screen time in U.S. children with and without asthma. J. Child. Health Care 2016, 45, 22–38. [Google Scholar] [CrossRef] [Green Version]
- Saeed, M.A.; Gribben, K.C.; Alam, M.; Lyden, E.R.; Hanson, C.K.; LeVan, T.D. Association of Dietary Fiber on Asthma, Respiratory Symptoms, and Inflammation in the Adult National Health and Nutrition Examination Survey Population. Ann. Am. Thorac. Soc. 2020, 17, 1062–1068. [Google Scholar] [CrossRef]
- Lee, H.; Lee, K.; Son, S.; Kim, Y.-C.; Kwak, J.; Kim, H.; Lee, S.; Kim, T. Association of allergic diseases and related conditions with dietary fiber intake in Korean adults. Int. J. Environ. Res. Public Health 2021, 18, 1–10. [Google Scholar]
- Miyake, Y.; Sasaki, S.; Ohya, Y.; Miyamoto, S.; Matsunaga, I.; Yoshida, T.; Hirota, Y.; Oda, H. Dietary intake of seaweed and minerals and prevalence of allergic rhinitis in Japanese pregnant females: Baseline data from the Osaka Maternal and Child Health Study. Ann. Epidemiol. 2006, 16, 614–621. [Google Scholar] [CrossRef]
- Andrianasolo, R.M.; Hercberg, S.; Kesse-Guyot, E.; Druesne-Pecollo, N.; Touvier, M.; Galan, P.; Varraso, R. Association between dietary fibre intake and asthma (symptoms and control): Results from the French national e-cohort NutriNet-Sante. Br. J. Nutr. 2019, 122, 1040–1051. [Google Scholar] [CrossRef]
- Berthon, B.S.; Macdonald-Wicks, L.K.; Gibson, P.G.; Wood, L.G. Investigation of the association between dietary intake, disease severity and airway inflammation in asthma. Respirology 2013, 18, 447–454. [Google Scholar] [CrossRef] [Green Version]
- Kan, H.; Stevens, J.; Heiss, G.; Rose, K.M.; London, S.J. Dietary fiber, lung function, and chronic obstructive pulmonary disease in the atherosclerosis risk in communities study. Am. J. Epidemiol. 2008, 167, 570–578. [Google Scholar] [CrossRef] [Green Version]
- Hirayama, F.; Lee, A.H.; Binns, C.; Zhao, Y.; Hiramatsu, T.; Tanikawa, Y.; Nishimura, K.; Taniguchi, H. Do vegetables and fruits reduce the risk of chronic obstructive pulmonary disease? A case-control study in Japan. Prev. Med. 2009, 49, 184–189. [Google Scholar] [CrossRef]
- Butler, L.M.; Koh, W.-P.; Lee, H.-P.; Yu, M.C.; London, S.J. Dietary fiber and reduced cough with phlegm: A cohort study in Singapore. Am. J. Respir. Crit. Care Med. 2004, 170, 279–287. [Google Scholar] [CrossRef]
- Varraso, R.; Willett, W.C.; Camargo, C.A., Jr. Prospective study of dietary fiber and risk of chronic obstructive pulmonary disease among US women and men. Am. J. Epidemiol. 2010, 171, 776–784. [Google Scholar] [CrossRef] [Green Version]
- Kaluza, J.; Harris, H.; Wallin, A.; Linden, A.; Wolk, A. Dietary Fiber Intake and Risk of Chronic Obstructive Pulmonary Disease: A Prospective Cohort Study of Men. Epidemiology 2018, 29, 254–260. [Google Scholar] [CrossRef]
- Szmidt, M.K.; Kaluza, J.; Harris, H.R.; Linden, A.; Wolk, A. Long-term dietary fiber intake and risk of chronic obstructive pulmonary disease: A prospective cohort study of women. Eur. J. Nutr. 2020, 59, 1869–1879. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.; Choi, H.; Kim, J. Association between Dietary Nutrient Intake and Chronic Obstructive Pulmonary Disease Severity: A Nationwide Population-Based Representative Sample. COPD 2020, 17, 49–58. [Google Scholar] [CrossRef]
- Jung, Y.J.; Lee, S.H.; Chang, J.H.; Lee, H.S.; Kang, E.H.; Lee, S.W. The Impact of Changes in the Intake of Fiber and Antioxidants on the Development of Chronic Obstructive Pulmonary Disease. Nutrients 2021, 13, 580. [Google Scholar] [CrossRef]
- Hanson, C.; Lyden, E.; Rennard, S.; Mannino, D.M.; Rutten, E.P.A.; Hopkins, R.; Young, R. The Relationship between Dietary Fiber Intake and Lung Function in the National Health and Nutrition Examination Surveys. Ann. Am. Thorac. Soc. 2016, 13, 643–650. [Google Scholar] [CrossRef]
- Root, M.M.; Houser, S.M.; Anderson, J.J.B.; Dawson, H.R. Healthy Eating Index 2005 and selected macronutrients are correlated with improved lung function in humans. Nutr. Res. 2014, 34, 277–284. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.-A.; Joshi, P.; Kim, Y.; Kang, D.; Kim, W.J. The Association of Dietary Macronutrients with Lung Function in Healthy Adults Using the Ansan-Ansung Cohort Study. Nutrients 2020, 12, 2688. [Google Scholar] [CrossRef]
- Leng, S.; Picchi, M.A.; Tesfaigzi, Y.; Wu, G.; Gauderman, W.J.; Xu, F.; Gilliland, F.D.; Belinsky, S.A. Dietary nutrients associated with preservation of lung function in Hispanic and non-Hispanic white smokers from New Mexico. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 3171–3181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephen, A.M.; Champ, M.M.-J.; Cloran, S.J.; Fleith, M.; Van Lieshout, L.; Mejborn, H.; Burley, V.J. Dietary fibre in Europe: Current state of knowledge on definitions, sources, recommendations, intakes and relationships to health. Nutr. Res. Rev. 2017, 30, 149–190. [Google Scholar] [CrossRef]
- Edwards, C.; Xie, C.; Garcia, A. Dietary fibre and health in children and adolescents. Proc. Nutr. Soc. 2015, 73, 292–302. [Google Scholar] [CrossRef] [Green Version]
- Lee-Sarwar, K.A.; Kelly, R.S.; Lasky-Su, J.; Zeiger, R.S.; O’Connor, G.T.; Sandel, M.T.; Bacharier, L.B.; Beigelman, A.; Rifas-Shiman, S.L.; Carey, V.J.; et al. Fecal short-chain fatty acids in pregnancy and offspring asthma and allergic outcomes. J. Allergy Clin. Immunol. Pract. 2020, 8, 1100–1102.e13. [Google Scholar] [CrossRef] [PubMed]
- Roduit, C.; Frei, R.; Ferstl, R.; Loeliger, S.; Westermann, P.; Rhyner, C.; Schiavi, E.; Barcik, W.; Rodriguez-Perez, N.; Wawrzyniak, M.; et al. High levels of Butyrate and Propionate in early life are associated with protection against atopy. Allergy Eur. J. Allergy Clin. Immunol. 2018, 74, 799–809. [Google Scholar] [CrossRef] [PubMed]
- Thorburn, A.N.; McKenzie, C.I.; Shen, S.; Stanley, D.; Macia, L.; Mason, L.J.; Roberts, L.K.; Wong, C.; Shim, R.; Robert, R.; et al. Evidence that asthma is a developmental origin disease influenced by maternal diet and bacterial metabolites. Nat. Commun. 2015, 6, 7320. [Google Scholar] [CrossRef]
- Zhang, D.P.; Li, S.; Wang, N.; Tan, H.Y.; Zhang, Z.M.; Feng, Y.B. The Cross-Talk Between Gut Microbiota and Lungs in Common Lung Diseases. Front. Microbiol. 2020, 11, 301. [Google Scholar] [CrossRef] [PubMed]
- Vuillermin, P.J.; Macia, L.; Nanan, R.; Tang, M.L.K.; Collier, F.; Brix, S. The maternal microbiome during pregnancy and allergic disease in the offspring. Semin. Immunopathol. 2017, 39, 669–675. [Google Scholar] [CrossRef] [Green Version]
- Seyedrezazadeh, E.; Moghaddam, M.; Ansarin, K.; Vafa, M.; Sharma, S.; Kolahdooz, F. Fruit and vegetable intake and risk of wheezing and asthma: A systematic review and meta-analysis. Nutr. Rev. 2014, 72, 411–428. [Google Scholar] [CrossRef]
- Hosseini, B.; Berthon, B.; Wark, P.; Wood, L. Effects of Fruit and Vegetable Consumption on Risk of Asthma, Wheezing and Immune Responses: A Systematic Review and Meta-Analysis. Nutrients 2017, 9, 341. [Google Scholar] [CrossRef]
- Zhang, Y.; Lin, J.; Fu, W.; Liu, S.; Gong, C.; Dai, J. Mediterranean diet during pregnancy and childhood for asthma in children: A systematic review and meta-analysis of observational studies. Pediatr. Pulmonol. 2019, 54, 949–961. [Google Scholar] [CrossRef] [PubMed]
- Tabak, C.; Wijga, A.; de Meer, G.; Janssen, N.; Brunekreef, B.; Smit, H. Diet and asthma in Dutch school children (ISAAC-2). Thorax 2006, 61, 1048–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuchs, O.; Bahmer, T.; Rabe, K.; von Mutius, E. Asthma transition from childhood into adulthood. Lancet Respir. Med. 2017, 5, 224–234. [Google Scholar] [CrossRef]
- Koefoed, H.; Zwitserloot, A.; Vonk, J.; Koppelman, G. Asthma, bronchial hyperresponsiveness, allergy and lung function development until early adulthood: A systematic literature review. Pediatr. Allergy Immunol. 2021, 32, 1238–1254. [Google Scholar] [CrossRef]
- Roberts, G.; Xatzipsalti, M.; Borrego, L.M.; Custovic, A.; Halken, S.; Hellings, P.; Papadopoulos, N.; Rotiroti, G.; Scadding, G.; Timmermans, F.; et al. Paediatric rhinitis: Position paper of the European Academy of Allergy and Clinical Immunology. Allergy 2013, 68, 1102–1116. [Google Scholar] [CrossRef] [PubMed]
- Hellings, P.W.; Klimek, L.; Cingi, C.; Agache, I.; Akdis, C.; Bachert, C.; Bousquet, J.; Demoly, P.; Gevaert, P.; Hox, V.; et al. Non-allergic rhinitis: Position paper of the European Academy of Allergy and Clinical Immunology. Allergy 2017, 72, 1657–1665. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.Y.; Shi, L.; Pang, W.H.; Liu, W.W.; Li, J.F.; Wang, H.B.; Shi, G. Dietary Fiber Intake Regulates Intestinal Microflora and Inhibits Ovalbumin-Induced Allergic Airway Inflammation in a Mouse Model. PLoS ONE 2016, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatzi, L.; Apostolaki, G.; Bibakis, I.; Skypala, I.; Bibaki-Liakou, V.; Tzanakis, N.; Kogevinas, M.; Cullinan, P. Protective effect of fruits, vegetables and the Mediterranean diet on asthma and allergies among children in Crete. Thorax 2007, 62, 677–683. [Google Scholar] [CrossRef] [Green Version]
- Fonseca Wald, E.L.A.; van den Borst, B.; Gosker, H.R.; Schols, A.M.W.J. Dietary fibre and fatty acids in chronic obstructive pulmonary disease risk and progression: A systematic review. Respirology 2014, 19, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Seyedrezazadeh, E.; Pour Moghaddam, M.; Ansarin, K.; Jafarabadi, M.A.; Sharifi, A.; Sharma, S.; Kolahdooz, F. Dietary Factors and Risk of Chronic Obstructive Pulmonary Disease: A Systemic Review and Meta-Analysis. Tanaffos 2019, 18, 294–309. [Google Scholar]
- Young, R.P.; Hopkins, R.J.; Marsland, B. The Gut-Liver-Lung Axis. Modulation of the Innate Immune Response and Its Possible Role in Chronic Obstructive Pulmonary Disease. Am. J. Respir. Cell Mol. Biol. 2016, 54, 161–169. [Google Scholar] [CrossRef]
- Reynolds, A.; Mann, J.; Cummings, J.; Winter, N.; Mete, E.; Te Morenga, L. Carbohydrate quality and human health: A series of systematic reviews and meta-analyses. Lancet 2019, 393, 434–445. [Google Scholar] [CrossRef] [Green Version]
- Willett, W.C. Nutritional Epidemiology, 3rd ed.; Oxford University Press: Oxford UK, 2013. [Google Scholar]
- Lachat, C.; Hawwash, D.; Ocké, M.; Berg, C.; Forsum, E.; Hörnell, A.; Larsson, C.; Sonestedt, E.; Wirfält, E.; Åkesson, A.; et al. Strengthening the Reporting of Observational Studies in Epidemiology-Nutritional Epidemiology (STROBE-nut): An Extension of the STROBE Statement. PLoS Med. 2016, 13, e1002036. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Author, Year, Country, Cohort | Study Design | Sample Size | Population | Exposure Assessment | Outcome Assessment | Follow-Up | Statistical Methods | Effect Measures | Covariates |
|---|---|---|---|---|---|---|---|---|---|
| Maternal fibre intake during pregnancy | |||||||||
| Pretorius et al., 2019, Australia [16] | C | 639 mother–infant pairs | mothers aged ≥ 18 years, non-smokers, infants with family history of allergic disease | semi-quantitative 101-item FFQ at 36–40 weeks’ gestation assessing intake over one month | parent reported and doctor diagnosed wheeze | 12 months | logistic regression, multinomial logistic regression | total fibre (g/day), median 23.8 OR (95% CI) 0.99 (0.99–1.00) parent reported wheeze OR (95% CI) 0.98 (0.94–1.01) doctor diagnosed wheeze | maternal age, education, ethnicity, child’s gender, birth weight, gestational age at birth, pet ownership, maternal parity, delivery mode |
| Fibre intake during childhood | |||||||||
| Wood et al., 2015, Australia [17] | CS | 144 | adolescents aged 12–18 years | interviewer administered 107-item FFQ | ISAAC video questionnaire, spirometry | - | logistic regression | total fibre (g/day) OR (95% CI) 1.0 (1.0–1.0) self-reported wheeze | age, sex, length of time in Australia |
| Vaccaro et al., 2016, US, NHANES [18] | CS | 4133 | children aged 2–11 years | 24 h dietary recall | self-reported asthma | - | logistic regression | energy adjusted fibre, median 6.7 g/1000 kcal Q1 vs. Q4 OR (95% CI) 1.31 (0.88–1.96), p-trend 0.034 ever asthma, Q1 vs. Q4 OR (95% CI) 1.38 (0.87–2.20), p-trend 0.027 current asthma | age, gender, second-hand smoke exposure, income |
| Fibre intake during adulthood | |||||||||
| Asthma, rhinitis and related symptoms | |||||||||
| Saeed et al., 2020, US, NHANES [19] | CS | 13,147 | adults aged 20–79 years (mean age 46 years) | two-interviewer-administered 24 h recalls | self-reported asthma, wheeze, cough, phlegm production, blood CRP | - | logistic regression, multinomial logistic regression | total fibre Q1 vs. Q4 (<10.5 vs. >21.2 g/day) OR (95% CI) 1.4 (1.0–1.8), p-trend 0.092 asthma, OR (95% CI) 1.3 (1.0–1.6), p-trend 0.017 wheeze, OR (95% CI) 1.7 (1.2–2.3), p-trend 0.0003 cough, OR (95% CI) 1.4 (1.1–2.0), p-trend 0.011 phlegm | age, race/ethnicity, sex, smoking status, BMI, poverty index ratio, total energy intake |
| Lee et al., 2021, South Korea, Korean NHANES [20] | CS | 10,479 | adults aged 19 years and older (mean age 51 years) | 63-item FFQ | self-reported asthma, self-reported rhinitis plus nasal endoscopy, serum IgE and specific IgE levels | - | logistic regression | total fibre Q4 vs. Q1 OR (95% CI) 0.66 (0.48–0.91), p-trend < 0.001 asthma, OR (95% CI) 0.95 (0.77–1.17), p-trend < 0.001 allergic rhinitis | age, sex, household income, residency, alcohol consumption, smoking status, BMI, physical activity, other nutrients |
| Miyake et al., 2006, Japan, Osaka Maternal and Child Health Study [21] | CS | 1002 | pregnant women | 147-item questionnaire assessing intake over one month | allergic rhinitis drug treatment during the previous 12 months | - | logistic regression | energy adjusted fibre (g/day) Q4 (14.7) vs. Q1 (8.2) OR (95% CI) 1.14 (0.66–2.00), p-trend 0.80 | age, gestation, parity, cigarette smoking, passive smoking, indoor domestic pets, family history of asthma, eczema, rhinitis, family income, education, mite allergen level in house dust, changes in diet in the previous month, season of data collection, BMI |
| Andrianasolo et al., 2019, France, NutriNet-Sante Study [22] | CS | 26,640 women and 8740 men | adults aged 18 years and older (mean age 53 years in women, 59 years in men) | three self-administered web-based 24 h dietary records | self-reported asthma symptom score, asthma control test | - | binomial negative regression, logistic regression | total fibre Q5 vs. Q1 (28.6 vs. 13.8 g/day in women, 30.5 vs. 12.7 g/day in men) asthma symptom score OR (95% CI) 0.73 (0.67–0.79), p-trend < 0.001 in women and OR (95% CI) 0.63 (0.55–0.73), p-trend < 0.001 in men | age, educational level, smoking status, pack-years of smoking, BMI, physical activity, total energy intake, allergic rhinitis, family history of asthma |
| Berthon et al., 2013, Australia [23] | CC | 137 cases with asthma (of which 64 with severe persistent asthma), 65 controls | adults aged 18 years and older (mean age 53 years) | 186-item semi-quantitative FFQ | asthma severity, lung function (eNO, spirometry, sputum cells) | - | logistic and linear regression | energy adjusted fibre (mean cases 32 g/day, controls 37 g/day) severe persistent asthma OR (95% CI) 0.94 (0.90–0.99) Coefficients for dietary fibre intake in asthmatics FEV1 0.02 L, FVC 0.02 L, FEV1/FVC 0.002, airway % eosinophils −0.36, % neutrophils 0.26 | age, gender, BMI, total energy |
| COPD and related symptoms | |||||||||
| Kan et al., 2008, US, ARIC study [24] | CS | 11,897 | adults aged 44–66 years | interviewer-administered 66-item semi-quantitative FFQ | spirometry, COPD based on self-reported symptoms or spirometry | 3 years | linear regression, logistic regression | total fibre (g/day) Q5 (26.7) vs. Q1 (9.5) OR (95% CI) COPD prevalence 0.85 (0.68–1.05), p-trend 0.044 Coefficients (95% CI) FEV1 60.2 mL (27.7–92.7), p-trend < 0.001, FVC 55.2 mL (18.2–92.3), p-trend 0.001, FEV1/FVC 0.4 (−0.1–0.9), p-trend 0.040, % predicted FEV1 1.8 (0.8–2.9), p-trend < 0.001, % predicted FVC 1.4 (0.4–2.4), p-trend 0.001 | BMI, age, ethnicity, gender, study centre, smoking status, pack-years, occupation, education, diabetes status, residence-based traffic density, total energy intake, glycaemic index, micronutrients from both food and supplements, and cured meat |
| Hirayama et al., 2009, Japan [25] | CC | 278 cases with COPD, 340 controls | adults aged 50–75 years (mean age 66 years) | 138-item FFQ assessing intake over the previous five years | spirometry diagnosed COPD within the past four years | - | unconditional logistic regression | total fibre (g/day) Q4 (≥16.08) vs. Q1 (≤8.84) OR (95% CI) 0.49 (0.26–0.95), p-trend 0.160 | age, gender, BMI, education level, life-long physical activity involvement, smoking status, smoking pack-years, alcohol drinking, intake of fish, red meat and chicken, total energy intake |
| Butler et al., 2004, Singapore, Singapore Chinese Health Study [26] | C | 49,140 | adults aged 45–74 years of Chinese origin | 165-item quantitative FFQ | self-reported incident cough with phlegm | 5.3 years | unconditional logistic regression | Q4 (11.6) vs. Q1 (4.7) OR (95% CI) non-starch polysaccharides (g) 0.61 (0.47–0.78), p-trend 0.001, fruit 0.67 (0.52–0.87), p-trend 0.006, grain 1.12 (0.80–1.56), p-trend 0.301, vegetable 0.92 (0.70–1.21), p-trend 0.504, soy isoflavones 0.67 (0.53–0.86), p-trend 0.001 | age, sex, dialect group, total energy intake, smoking status, age of smoking initiation, amount smoked |
| Varraso et al., 2010, US, Nurses’ Health Study, Health Professionals Follow-up Study [27] | C | 111,580 | female nurses aged 30–55 years, men health professionals 40–75 years, no history of asthma or COPD | FFQs administered in 1984, 1986, 1990, 1994 and 1998 in NHS and in 1986, 1990 and 1994 in HPFS | self-reported COPD defined by doctor diagnosis of chronic bronchitis or emphysema and diagnostic test | 16 and 12 years | Cox proportional hazard regression models | total fibre Q5 (28.4) vs. Q1 (11.2) RR (95% CI) 0.67 (0.50–0.90), p-trend 0.03 | age, sex, smoking status, pack-years, pack-years2, energy intake, BMI, US region, physician visits, physical activity, diabetes, intakes of omega-3 (foods and supplements), cured meat, (glycaemic index, carotenoids, vitamins C, D, E) |
| Kaluza et al., 2018, Sweden, Cohort of Swedish Men [28] | C | 45,058 | men aged 45–79 years, no history of COPD | 96-item FFQ | incident COPD cases through linkage with registry data | 13.1 years | Cox proportional hazard regression models | total fibre (g/day) Q5 (≥36.8) vs. Q1 (<23.7) HR (95% CI) 0.62 (0.53–0.71), p-trend < 0.001 | age, education, BMI, total physical activity, smoking status, pack-years of smoking, alcohol intake, energy intake |
| Szmidt et al., 2020, Sweden, Swedish Mammography Cohort [29] | C | 35,339 | women aged on average 62 years, no history of COPD | 67-tem FFQ in 1987, 96-item FFQ in 1997 (baseline) | incident COPD cases through linkage with registry data | 11.5 years | Cox proportional hazard regression models | long-term total fibre (g/day) Q5 (≥26.5) vs. Q1 (<17.6) HR (95% CI) 0.70 (0.59–0.83), p-trend < 0.001 | age, education, BMI, walking/cycling, smoking status, pack-years of smoking, alcohol, energy intake |
| Kim et al., 2019, South Korea, Korean NHANES [30] | CS | 702 | COPD adults aged ≥ 40 years | 24 h dietary recall | COPD severity defined by spirometry | - | linear regression | mean (SE) total fibre (g/day) severity men 20.9 (1.7), women 18.3 (1.8) | sex, age, residential area, educational level, household income, smoking status, height |
| Jung et al., 2021, Korea [31] | C | 1439 | adults aged on average 53 years | 117-item FFQ assessing intake over the previous three months, in 2012 and 2017 | incident COPD cases defined by spirometry | 5 years | logistic regression | decrease in total fibre (g/day) Q4 vs. Q1 decrease in total fibre, proportion of new airflow limitation cases 5.85% vs. 1.39% | age, sex, smoking history, baseline FEV1/FVC |
| Lung function | |||||||||
| Hanson et al., 2016, US, NHANES [32] | CS | 1921 | adults aged 40–79 years (mean age 53 years) | two-interviewer administered 24 h recalls | spirometry | - | regression analyses | total fibre (g/day) Q4 (<10.75) vs. Q1 (>17.5) Coefficients FEV1 82 mL, FVC 129 mL, % predicted FEV1 2.4, % predicted FVC 2.8 | age, sex, smoking status, height, BMI, socioeconomic status, total energy intake, CRP, vitamin E, a-carotene, b-carotene, b-cryptoxanthin, lycopene, lutein plus zeaxanthin, vitamin C and cured meat |
| Root et al., 2014, US, ARIC study [33] | C | 12,532 | adults aged on average 54 years | interviewer-administered semi-quantitative FFQ | spirometry | 3 years | linear regression | Coefficients per increase in one quintile of total fibre FEV1 NS, FVC NS, %FEV1 0.201, p-trend ≤ 0.05, FEV1/FVC 0.129, p-trend ≤ 0.01 | age, sex, ethnicity, education, total caloric intake, physical activity, current smoking, cigarette years, height, BMI, and interaction term black ethnicity × BMI |
| Lee et al., 2020, Korea, Ansan-Ansung cohort [34] | C | 5880 | non-COPD adults median age 50 years | 103-item FFQ | spirometry (% difference of predicted FEV1 between baseline and follow-up) | 4 years | logistic regression | Q5 (≥8.9) vs. Q1 (≤4.4 g/day) decreased vs. unchanged/improved OR (95% CI) 0.83 (0.61–1.12), p-trend 0.080 in men, 1.14 (0.86–1.51), p-trend 0.345 in women | age, education, household income, job, BMI, waist circumference, waist-to-hip ratio, smoking, alcohol, exercise, marriage status, history of asthma and tuberculosis, energy intake |
| Leng et al., 2017, US, Lovelace Smokers cohort (LSC), Veteran Smokers cohort (VSC) [35] | C | 1829 in LSC, 508 in VSC | adult smokers aged 40–74 years (mean age 57 in LSC, 62 in VSC) | semi-quantitative 150-item FFQ | spirometry | 5.3 years | linear mixed effects model with a subject-specific random intercept, linear regression | total fibre (g/day), mean 10.5 Coefficients (SE) FEV1 LSC 80.9 mL (20.3), VSC 97.8 mL (41.8), FEV1/FVC% LSC 1.075 (0.403), VSC 2.018 (0.761) | age, sex, ethnicity, smoking history, BMI, educational level, height, total caloric intake, time since enrolment, baseline FEV1 in decline analysis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sdona, E.; Georgakou, A.V.; Ekström, S.; Bergström, A. Dietary Fibre Intake in Relation to Asthma, Rhinitis and Lung Function Impairment—A Systematic Review of Observational Studies. Nutrients 2021, 13, 3594. https://doi.org/10.3390/nu13103594
Sdona E, Georgakou AV, Ekström S, Bergström A. Dietary Fibre Intake in Relation to Asthma, Rhinitis and Lung Function Impairment—A Systematic Review of Observational Studies. Nutrients. 2021; 13(10):3594. https://doi.org/10.3390/nu13103594
Chicago/Turabian StyleSdona, Emmanouela, Athina Vasiliki Georgakou, Sandra Ekström, and Anna Bergström. 2021. "Dietary Fibre Intake in Relation to Asthma, Rhinitis and Lung Function Impairment—A Systematic Review of Observational Studies" Nutrients 13, no. 10: 3594. https://doi.org/10.3390/nu13103594
APA StyleSdona, E., Georgakou, A. V., Ekström, S., & Bergström, A. (2021). Dietary Fibre Intake in Relation to Asthma, Rhinitis and Lung Function Impairment—A Systematic Review of Observational Studies. Nutrients, 13(10), 3594. https://doi.org/10.3390/nu13103594