The Frequency and Context of Snacking among Children: An Objective Analysis Using Wearable Cameras


 , and
, and
Abstract
1. Introduction
- Identify rates of total, discretionary and healthful snacking among children per day.
- Determine the context of snacking episodes relating to food group, eating location, source, time of consumption, social contact and screen use.
- Examine the association between sociodemographic characteristics (gender, ethnicity and household socioeconomic deprivation) and body mass index (BMI) and total, discretionary and healthful snacking rates.
2. Materials and Methods
2.1. The Kids’Cam Project
2.2. Methods for Coding Snacking Behaviour
2.3. Contextual Factors
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Snacking Frequency and Snacking Food Choices
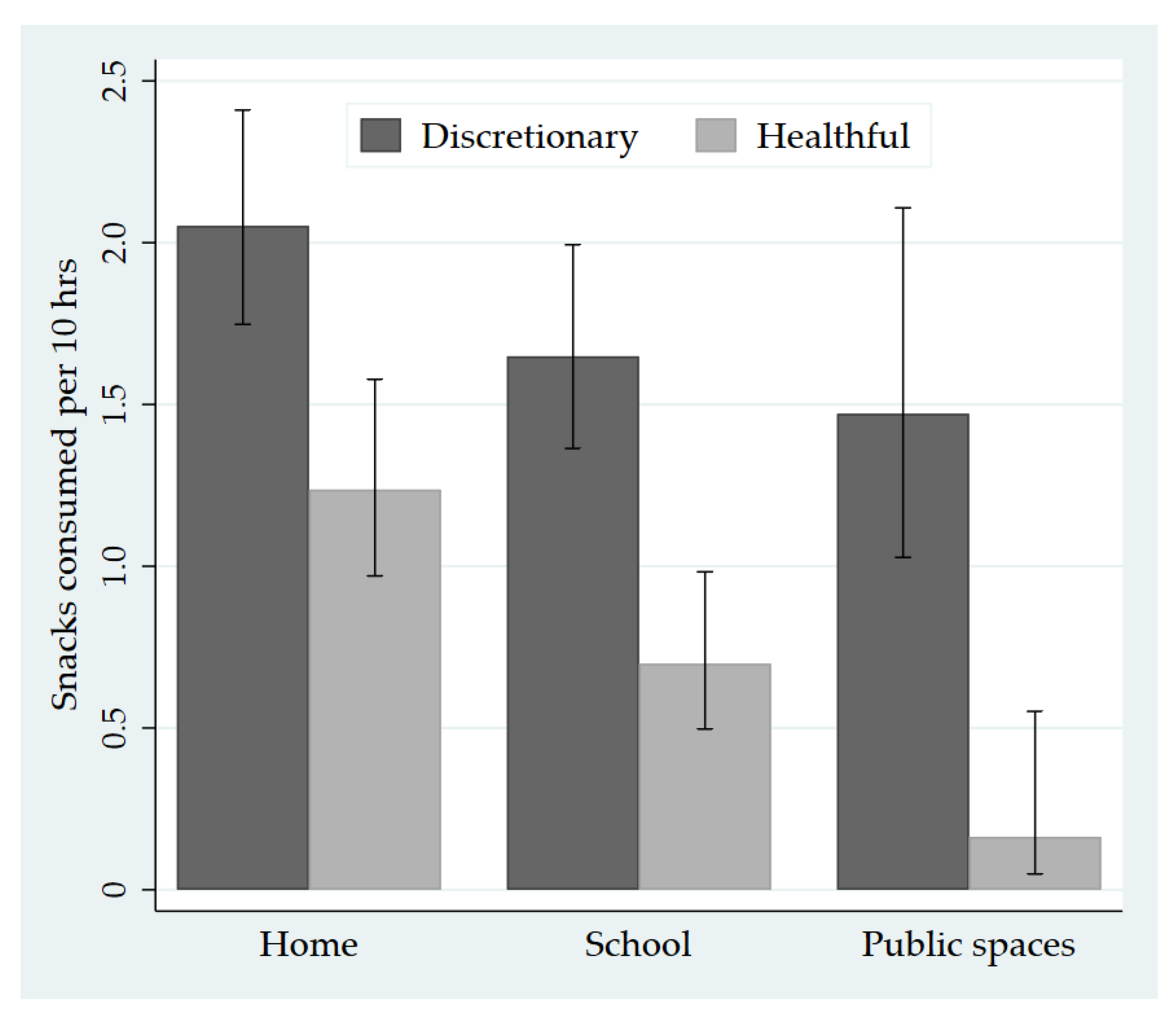
3.3. Eating Location
3.4. Sources of Snacks
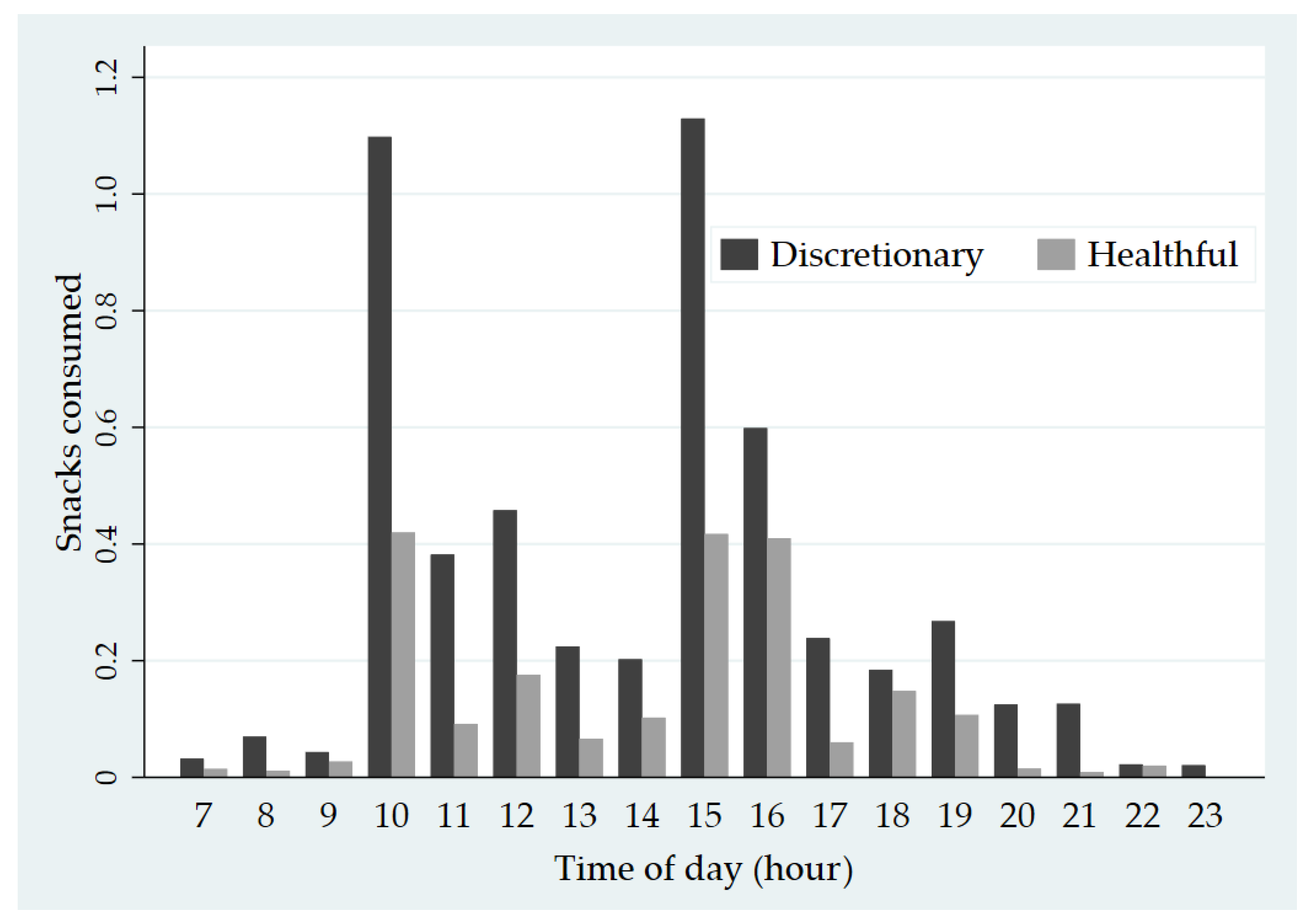
3.5. Timing
3.6. Screen Use and Social Contact
3.7. Differences in Snacking Episodes by Sociodemographic Characteristics and BMI
3.8. Sensitivity Analysis
4. Discussion
Study Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hess, J.M.; Jonnalagadda, S.S.; Slavin, J.L. What Is a Snack, Why Do We Snack, and How Can We Choose Better Snacks? A Review of the Definitions of Snacking, Motivations to Snack, Contributions to Dietary Intake, and Recommendations for Improvement. Adv. Nutr. 2016, 7, 466–475. [Google Scholar] [CrossRef] [PubMed]
- Njike, V.Y.; Smith, T.M.; Shuval, O.; Shuval, K.; Edshteyn, I.; Kalantari, V.; Yaroch, A.L. Snack Food, Satiety, and Weight. Adv. Nutr. 2016, 7, 866–878. [Google Scholar] [CrossRef] [PubMed]
- Leech, R.M.; Worsley, A.; Timperio, A.; McNaughton, S.A. Understanding meal patterns: Definitions, methodology and impact on nutrient intake and diet quality. Nutr. Res. Rev. 2015, 28, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Van der Horst, K.; Jacquier, E.F.; Afeiche, M.C.; Eldridge, A.L. Snacking Patterns in Children: A Comparison between Australia, China, Mexico, and the US. Nutrients 2018, 10, 198. [Google Scholar] [CrossRef]
- Veatupu, L.; Puloka, V.; Smith, M.; McKerchar, C.; Signal, L. Me’akai in Tonga: Exploring the Nature and Context of the Food Tongan Children Eat in Ha’apai Using Wearable Cameras. Int. J. Environ. Res. Public Health 2019, 16, 1681. [Google Scholar] [CrossRef]
- Potter, M.; Vlassopoulos, A.; Lehmann, U. Snacking Recommendations Worldwide: A Scoping Review. Adv. Nutr. 2018, 9, 86–98. [Google Scholar] [CrossRef]
- Johnson, B.J.; Bell, L.K.; Zarnowiecki, D.; Rangan, A.M.; Golley, R.K. Contribution of Discretionary Foods and Drinks to Australian Children’s Intake of Energy, Saturated Fat, Added Sugars and Salt. Children 2017, 4, 104. [Google Scholar] [CrossRef]
- Bellisle, F. Meals and snacking, diet quality and energy balance. Physiol. Behav. 2014, 134, 38–43. [Google Scholar] [CrossRef]
- Wouters, E.J.; Larsen, J.K.; Kremers, S.P.; Dagnelie, P.C.; Geenen, R. Peer influence on snacking behavior in adolescence. Appetite 2010, 55, 11–17. [Google Scholar] [CrossRef]
- Duffey, K.J.; Rivera, J.A.; Popkin, B.M. Snacking is prevalent in Mexico. J. Nutr. 2014, 144, 1843–1849. [Google Scholar] [CrossRef]
- Wansink, B.; Kim, J. Bad popcorn in big buckets: Portion size can influence intake as much as taste. J. Nutr. Educ. Behav. 2005, 37, 242–245. [Google Scholar] [CrossRef]
- Zenk, S.N.; Horoi, I.; McDonald, A.; Corte, C.; Riley, B.; Odoms-Young, A.M. Ecological momentary assessment of environmental and personal factors and snack food intake in African American women. Appetite 2014, 83, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, G.M.; Méjean, C.; Kesse-Guyot, E.; Andreeva, V.A.; Bellisle, F.; Hercberg, S.; Péneau, S. The associations between emotional eating and consumption of energy-dense snack foods are modified by sex and depressive symptomatology. J. Nutr. 2014, 144, 1264–1273. [Google Scholar] [CrossRef] [PubMed]
- Blaine, R.E.; Kachurak, A.; Davison, K.K.; Klabunde, R.; Fisher, J.O. Food parenting and child snacking: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 146. [Google Scholar] [CrossRef] [PubMed]
- Van Ansem, W.J.; Schrijvers, C.T.; Rodenburg, G.; van de Mheen, D. Children’s snack consumption: Role of parents, peers and child snack-purchasing behaviour. Results from the INPACT study. Eur. J. Public Health 2015, 25, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Micha, R.; Karageorgou, D.; Bakogianni, I.; Trichia, E.; Whitsel, L.P.; Story, M.; Penalvo, J.L.; Mozaffarian, D. Effectiveness of school food environment policies on children’s dietary behaviors: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0194555. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, M.; Cash, S.B.; Yeh, C.H.; Landwehr, S.C.; McAlister, A.R. Children’s purchase behavior in the snack market: Can branding or lower prices motivate healthier choices? Appetite 2017, 117, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.; Kelly, B.; Yeatman, H.; Boyland, E. Food Marketing Influences Children’s Attitudes, Preferences and Consumption: A Systematic Critical Review. Nutrients 2019, 11, 875. [Google Scholar] [CrossRef]
- Xin, J.; Zhao, L.; Wu, T.; Zhang, L.; Li, Y.; Xue, H.; Xiao, Q.; Wang, R.; Xu, P.; Visscher, T.; et al. Association between access to convenience stores and childhood obesity: A systematic review. Obes. Rev. 2019. [Google Scholar] [CrossRef]
- Stok, F.M.; de Vet, E.; de Ridder, D.T.; de Wit, J.B. The potential of peer social norms to shape food intake in adolescents and young adults: A systematic review of effects and moderators. Health Psychol. Rev. 2016, 10, 326–340. [Google Scholar] [CrossRef]
- Gemming, L.; Mhurchu, C.N. Dietary under-reporting: What foods and which meals are typically under-reported? Eur. J. Clin. Nutr. 2016, 70, 640–641. [Google Scholar] [CrossRef] [PubMed]
- O’Toole, C.; Gage, R.; McKerchar, C.; Puloka, V.; McLean, R.; Signal, L. Is snacking the new eating norm for New Zealand children? An urgent call for research. N. Z. Med. J. 2020, 133, 131–132. [Google Scholar] [PubMed]
- Ministry of Health. NZ Food NZ Children: Key Results of the 2002 National Children’s Nutrition Survey; Ministry of Health: Wellington, New Zealand, 2003.
- Regan, A.; Parnell, W.; Gray, A.; Wilson, N. New Zealand children’s dietary intakes during school hours. Nutr. Diet. 2008, 65, 205–210. [Google Scholar] [CrossRef]
- Rockell, J.E.; Parnell, W.R.; Wilson, N.C.; Skidmore, P.M.; Regan, A. Nutrients and foods consumed by New Zealand children on schooldays and non-schooldays. Public Health Nutr. 2011, 14, 203–208. [Google Scholar] [CrossRef]
- Chee, L. The Role of “Snacks” in the Diets of 5-Year Old Children in Dunedin, New Zealand; University of Otago: Dunedin, New Zealand, 2016. [Google Scholar]
- Ministry of Health. New Zealand Health Survey—Annual Data Explorer. 2019. Available online: https://minhealthnz.shinyapps.io/nz-health-survey-2018-19-annual-data-explorer/_w_ab5b87da/#!/home (accessed on 2 April 2020).
- Ministry of Health. Household Food Insecurity Among Children: New Zealand Health Survey: Summary of Findings; Ministry of Health: Wellington, New Zealand, 2019.
- Gemming, L.; Rush, E.; Maddison, R.; Doherty, A.; Gant, N.; Utter, J.; Mhurchu, C.N. Wearable cameras can reduce dietary under-reporting: Doubly labelled water validation of a camera-assisted 24 h recall. Br. J. Nutr. 2015, 113, 284–291. [Google Scholar] [CrossRef]
- O’Loughlin, G.; Cullen, S.J.; McGoldrick, A.; O’Connor, S.; Blain, R.; O’Malley, S.; Warrington, G.D. Using a wearable camera to increase the accuracy of dietary analysis. Am. J. Prev. Med. 2013, 44, 297–301. [Google Scholar] [CrossRef]
- Smith, M.; Stanley, J.; Signal, L.; Barr, M.; Chambers, T.; Balina, A.; Mhurchu, C.N.; Wilson, N. Children’s healthy and unhealthy beverage availability, purchase and consumption: A wearable camera study. Appetite 2019, 133, 240–251. [Google Scholar] [CrossRef]
- Davies, A.; Chan, V.; Bauman, A.; Signal, L.; Hosking, C.; Gemming, L.; Allman-Farinelli, M. Using wearable cameras to monitor eating and drinking behaviours during transport journeys. Eur. J. Nutr. 2020, 1–11. [Google Scholar] [CrossRef]
- Signal, L.N.; Smith, M.B.; Barr, M.; Stanley, J.; Chambers, T.J.; Zhou, J.; Duane, A.; Jenkin, G.L.; Pearson, A.L.; Gurrin, C.; et al. Kids’Cam: An Objective Methodology to Study the World in Which Children Live. Am. J. Prev. Med. 2017, 53, 89–95. [Google Scholar] [CrossRef]
- Signal, L.N.; Stanley, J.; Smith, M.; Barr, M.B.; Chambers, T.J.; Zhou, J.; Duane, A.; Gurrin, C.; Smeaton, A.F.; McKerchar, C.; et al. Children’s everyday exposure to food marketing: An objective analysis using wearable cameras. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 137. [Google Scholar] [CrossRef]
- Ministry of Health. Food and Nutrition Guidelines for Healthy Children and Young People (Aged 2–18 Years): A Background Paper—Revised February 2015; Ministry of Health: Wellington, New Zealand, 2012.
- Gardner, W.; Mulvey, E.P.; Shaw, E.C. Regression analyses of counts and rates: Poisson, overdispersed Poisson, and negative binomial models. Psychol. Bull. 1995, 118, 392–404. [Google Scholar] [CrossRef] [PubMed]
- Chambers, T.; Stanley, J.; Signal, L.; Pearson, A.L.; Smith, M.; Barr, M.; Ni Mhurchu, C. Quantifying the Nature and Extent of Children’s Real-time Exposure to Alcohol Marketing in Their Everyday Lives Using Wearable Cameras: Children’s Exposure via a Range of Media in a Range of Key Places. Alcohol Alcohol. 2018, 53, 626–633. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.; Chambers, T.; Abbott, M.; Signal, L. High Stakes: Children’s Exposure to Gambling and Gambling Marketing Using Wearable Cameras. Int. J. Ment. Health Addict. 2020, 18, 1025–1047. [Google Scholar] [CrossRef]
- Watkins, L.; Aitken, R.; Gage, R.; Smith, M.B.; Chambers, T.J.; Barr, M.; Stanley, J.; Signal, L.N. Capturing the Commercial World of Children: The Feasibility of Wearable Cameras to Assess Marketing Exposure. J. Consum. Aff. 2018, 53, 1396–1420. [Google Scholar] [CrossRef]
- Salmond, C.; Crampton, P.; King, P.; Waldegrave, C. NZiDep: A New Zealand index of socioeconomic deprivation for individuals. Soc. Sci. Med. 2006, 62, 1474–1485. [Google Scholar] [CrossRef]
- Murakami, K.; Livingstone, M.B. Associations between meal and snack frequency and diet quality and adiposity measures in British adults: Findings from the National Diet and Nutrition Survey. Public Health Nutr. 2016, 19, 1624–1634. [Google Scholar] [CrossRef]
- McKerchar, C.; Smith, M.; Gage, R.; Williman, J.; Abel, G.; Lacey, C.; Mhurchu, C.N.; Signal, L. Kids in a Candy Store: An Objective Analysis of Children’s Interactions with Food in Convenience Stores. Nutrients 2020, 12, 2143. [Google Scholar] [CrossRef]
- Vandevijvere, S.; Mackay, S.; D’Souza, E.; Swinburn, B. How Healthy Are New Zealand Food Environments? A Comprehensive Assessment 2014–2017; The University of Auckland: Auckland, New Zealand, 2018. [Google Scholar]
- Mozaffarian, D.; Angell, S.Y.; Lang, T.; Rivera, J.A. Role of government policy in nutrition—barriers to and opportunities for healthier eating. BMJ 2018, 361, k2426. [Google Scholar] [CrossRef]
- World Health Organization. Taking Action on Childhood Obesity; World Health Organization: Geneva, Sweden, 2018. [Google Scholar]
- Blundell-Birtill, P.; Hetherington, M.M. Determinants of Portion Size in Children and Adolescents: Insights from the UK National Diet and Nutrition Survey Rolling Programme (2008–2016). Nutrients 2019, 11, 2957. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Sociodemographic Variable and Group | n | % |
|---|---|---|
| Total | 158 | 100 |
| Gender | ||
| Female | 83 | 52.5 |
| Male | 75 | 47.5 |
| Ethnicity | ||
| NZ European | 65 | 41.1 |
| Māori | 58 | 36.7 |
| Pacific | 35 | 22.2 |
| Household socioeconomic deprivation | ||
| Lower (NZiDep 1–3) | 104 | 68 |
| Higher (NZiDep 4–5) | 49 | 32 |
| Age (years) | ||
| 11 | 13 | 8.2 |
| 12 | 115 | 72.8 |
| 13 | 24 | 15.2 |
| 14 | 1 | 0.6 |
| Mean (SD) | 12.6 (0.5) | |
| BMI | ||
| Not overweight (BMI = 16.0–24.9) | 90 | 57.3 |
| Overweight (BMI values ≥25.0) | 69 | 42.3 |
| Total Snacks | Discretionary Snacks | Healthful Snacks | ||||
|---|---|---|---|---|---|---|
| Mean Rate (95%CI) | % of Category | Mean Rate (95%CI) | % of Category | Mean Rate (95%CI) | % of Category | |
| Total snacking episodes | 8.2 (7.4, 9.1) | 100 | 5.2 (4.6, 5.9) | 100 | 2.1 (1.8, 2.5) | 100 |
| Food group | ||||||
| Confectionary | 1.3 (1.1, 1.5) | 15.5 | 1.3 (1.1, 1.5) | 24.5 | - | - |
| Snack foods | 1.2 (0.9, 1.6) | 14.4 | 1.2 (0.9, 1.6) | 22.8 | - | - |
| Cookies/cakes | 1.0 (0.8, 1.4) | 12.4 | 1.0 (0.8, 1.4) | 19.6 | - | - |
| Sugary drinks/juices | 1.0 (0.8, 1.2) | 12.1 | 1.0 (0.8, 1.2) | 19.1 | - | - |
| Fruit | 0.8 (0.6, 0.9) | 9.2 | - | - | 0.8 (0.6, 0.9) | 36.0 |
| Breads/cereals | 0.8 (0.6, 1.0) | 9.2 | - | - | 0.8 (0.6, 1.0) | 35.9 |
| Iced confectionary | 0.3 (0.2, 0.4) | 3.9 | 0.3 (0.2, 0.4) | 6.1 | - | - |
| Milk products (healthful) | 0.3 (0.2, 0.6) | 3.7 | - | - | 0.3 (0.2, 0.6) | 14.5 |
| Fast food (savoury only) | 0.2 (0.1, 0.3) | 2.0 | 0.2 (0.1, 0.3) | 3.2 | - | - |
| Vegetables | 0.1 (0.1, 0.2) | 1.2 | - | - | 0.1 (0.1, 0.2) | 4.7 |
| Processed meat | 0.1 (0.0, 0.2) | 1.1 | 0.1 (0.0, 0.2) | 1.7 | - | - |
| Savoury bakery items | 0.1 (0.0, 0.1) | 0.6 | 0.1 (0.0, 0.1) | 1.0 | - | - |
| Diet drinks | 0.1 (0.0, 0.1) | 0.6 | 0.1 (0.0, 0.1) | 0.9 | - | - |
| Nuts | 0.1 (0.0, 0.2) | 0.5 | - | - | 0.1 (0.0, 0.2) | 1.8 |
| Meat and alternatives | 0.1 (0.0, 0.1) | 0.4 | - | - | 0.1 (0.0, 0.1) | 1.7 |
| Milk products (discretionary) | 0.1 (0.0, 0.1) | 0.3 | 0.1 (0.0, 0.1) | 0.4 | - | - |
| Mixed dishes (healthful) | 0.1 (0.1, 0.2) | 0.2 | - | - | 0.1 (0.1, 0.2) | 4.9 |
| Mixed dishes (discretionary) | 0.1 (0.0, 0.3) | 0.1 | 0.1 (0.0, 0.3) | 1.6 | - | - |
| Eating location | ||||||
| Home | 3.9 (3.2, 4.5) | 47.5 | 2.1 (1.7, 2.4) | 39.5 | 1.2 (1.0, 1.6) | 58.7 |
| School | 2.6 (2.2, 3.1) | 31.7 | 1.6 (1.4, 2.0) | 31.8 | 0.7 (0.5, 1.0) | 33.2 |
| Public spaces | 1.8 (1.2, 2.8) | 21.9 | 1.5 (1.0, 2.1) | 28.3 | 0.1 (0.0, 0.6) | 7.8 |
| -Recreation/sport | 0.2 (0.1, 0.4) | 2.4 | 0.1 (0.1, 0.3) | 2.7 | 0.0 (0.0, 0.0) | 0.4 |
| -Food outlets | 0.3 (0.1, 0.7) | 3.7 | 0.2 (0.1, 0.4) | 3.2 | 0.0 (0.0, 0.1) | 1.1 |
| -Retail | 0.1 (0.0, 0.2) | 1.2 | 0.1 (0.0, 0.2) | 1.0 | 0.0 (0.0, 0.0) | 0.2 |
| -Other public places | 1.3 (0.8, 2.0) | 15.8 | 1.1 (0.7, 1.7) | 21.1 | 0.1 (0.0, 0.4) | 6.0 |
| Snack food source | ||||||
| Home | 5.6 (4.8, 6.6) | 68.9 | 3.2 (2.7, 3.9) | 62.6 | 1.7 (1.4, 2.1) | 81.7 |
| Food outlets | 1.0 (0.6, 1.7) | 12.8 | 0.9 (0.5, 1.4) | 16.8 | 0.1 (0.0, 0.2) | 3.0 |
| Unknown | 0.4 (0.3, 0.6) | 5.0 | 0.3 (0.2, 0.5) | 6.2 | 0.0 (0.0, 0.1) | 1.3 |
| School | 0.4 (0.2, 0.9) | 4.8 | 0.2 (0.1, 0.5) | 3.9 | 0.2 (0.1, 0.5) | 9.3 |
| Other child | 0.3 (0.2, 0.6) | 3.8 | 0.2 (0.1, 0.4) | 4.3 | 0.1 (0.0, 1.4) | 2.6 |
| Community venue | 0.2 (0.0, 1.0) | 2.5 | 0.2 (0.0, 1.0) | 3.5 | 0.0 (0.0, 0.1) | 0.5 |
| Adult | 0.1 (0.0, 0.3) | 1.3 | 0.1 (0.0, 0.2) | 1.1 | 0.0 (0.0, 0.3) | 1.7 |
| Retail | 0.1 (0.0, 0.5) | 0.8 | 0.1 (0.0, 4.7) | 1.3 | 0 | 0 |
| Recreation/sport | 0.0, 0.0, 0.1) | 0.1 | 0.0 (0.0, 0.1) | 0.2 | 0 | 0 |
| Time of day | ||||||
| Morning (06:00–11.59) | 2.4 (2.0, 3.0) | 29.7 | 1.6 (1.3, 1.9) | 30.9 | 0.6 (0.4, 0.9) | 28.2 |
| Afternoon (12:00–17.59.) | 4.6 (3.9, 5.4) | 55.9 | 2.8 (2.3, 3.5) | 54.9 | 1.2 (1.0, 1.5) | 58.2 |
| Evening (18:00–23.59) | 1.2 (0.8, 1.7) | 14.0 | 0.7 (0.5, 1.0) | 14.2 | 0.3 (0.1, 0.7) | 13.6 |
| Social contact | ||||||
| None | 2.0 (1.4, 2.8) | 24.5 | 1.2 (0.1, 1.8) | 22.7 | 0.6 (0.4, 0.9) | 28.2 |
| Children | 3.6 (2.8, 4.6) | 44.1 | 2.4 (1.8, 3.1) | 46.0 | 0.9 (0.7, 1.8) | 43.9 |
| Adults | 1.2 (1.0, 1.5) | 15.1 | 0.8 (0.5, 1.2) | 15.0 | 0.3 (0.2, 0.4) | 12.4 |
| Children and adults | 1.3 (0.7, 2.5) | 16.4 | 0.8 (0.5, 1.3) | 16.3 | 0.3 (0.1, 0.7) | 15.5 |
| Screen use | ||||||
| No screen | 6.3 (5.6, 6.9) | 76.0 | 3.9 (3.6, 4.3) | 75.9 | 1.6 (1.3, 1.9) | 74.9 |
| Screen use | 2.0 (1.5, 2.6) | 24.0 | 1.2 (1.0, 1.6) | 24.1 | 0.5 (0.3, 0.8) | 25.1 |
| All Snacks | Healthful Snacks | Discretionary Snacks | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristic | Mean Rate (95%CI) | Crude Rate ratio (RR) (95%CI) | Adjusted RR (95%CI) 1 | Mean Rate (95%CI) | Crude RR (95%CI) | Adjusted RR (95%CI) 1 | Mean Rate (95%CI) | Crude RR (95%CI) | Adjusted RR (95%CI) 1 |
| Gender | |||||||||
| Female (ref) | 9.2 (8.2, 10.0) | 1 | 1 | 2.5 (2.0, 3.0) | 1 | 1 | 5.8 (5.2, 6.5) | 1 | 1 |
| Male | 7.2 (6.4, 8.1) | 0.79 (0.68, 0.91) | 0.80 (0.70, 0.90) | 1.7 (1.3, 2.2) | 0.70 (0.49, 1.00) | 0.71 (0.55, 0.92) | 4.6 (3.8, 5.5) | 0.79 (0.65, 0.96) | 0.80 (0.66, 0.97) |
| Ethnicity | |||||||||
| NZE (ref) | 8.5 (7.4, 9.8) | 1 | 1 | 2.4 (1.9, 3.0) | 1 | 1 | 5.1 (4.3, 6.1) | 1 | 1 |
| Māori | 7.2 (5.8, 9.0) | 0.85 (0.65, 1.11) | 0.80 (0.63, 1.00) | 1.5 (0.9, 2.5) | 0.62 (0.36, 1.08) | 0.54 (0.35, 0.82) | 5.2 (4.2, 6.4) | 1.01 (0.78, 1.32) | 0.96 (0.74, 1.25) |
| Pacific | 8.0 (6.8, 9.3) | 0.94 (0.76, 1.15) | 0.95 (0.80, 1.13) | 1.4 (0.8, 2.3) | 0.57 (0.33, 0.99) | 0.58 (0.36, 0.94) | 5.5 (4.9, 6.2) | 1.08 (0.88, 1.32) | 1.05 (0.88, 1.24) |
| BMI | |||||||||
| Not overweight (ref) | 8.6 (7.3, 10.0) | 1 | 1 | 2.3 (1.8, 2.8) | 1 | 1 | 5.2 (4.3, 6.3) | 1 | 1 |
| Overweight/obese | 7.3 (6.6, 8.4) | 0.85 (0.67, 1.09) | 0.87 (0.69, 1.08) | 1.5 (1.2, 2.0) | 0.68 (0.49, 0.94) | 0.75 (0.53, 1.06) | 5.1 (4.4, 5.9) | 0.98 (0.74, 1.30) | 0.95 (0.73, 1.25) |
| NZiDep | |||||||||
| Lower deprivation (ref) | 7.9 (7.1, 8.8) | 1 | 1 | 2.0 (1.6, 2.4) | 1 | 1 | 5.0 (4.4, 5.7) | 1 | 1 |
| Higher deprivation | 9.0 (7.0, 11.6) | 1.13 (0.86, 1.49) | 1.19 (0.81, 1.10) | 2.5 (1.6, 4.2) | 1.30 (0.73, 2.33) | 1.48 (0.91, 2.43) | 5.9 (4.7, 7.4) | 1.18 (0.91, 1.54) | 1.16 (0.85, 1.59) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gage, R.; Girling-Butcher, M.; Joe, E.; Smith, M.; Ni Mhurchu, C.; McKerchar, C.; Puloka, V.; McLean, R.; Signal, L. The Frequency and Context of Snacking among Children: An Objective Analysis Using Wearable Cameras. Nutrients 2021, 13, 103. https://doi.org/10.3390/nu13010103
Gage R, Girling-Butcher M, Joe E, Smith M, Ni Mhurchu C, McKerchar C, Puloka V, McLean R, Signal L. The Frequency and Context of Snacking among Children: An Objective Analysis Using Wearable Cameras. Nutrients. 2021; 13(1):103. https://doi.org/10.3390/nu13010103
Chicago/Turabian StyleGage, Ryan, Martin Girling-Butcher, Ester Joe, Moira Smith, Cliona Ni Mhurchu, Christina McKerchar, Viliami Puloka, Rachael McLean, and Louise Signal. 2021. "The Frequency and Context of Snacking among Children: An Objective Analysis Using Wearable Cameras" Nutrients 13, no. 1: 103. https://doi.org/10.3390/nu13010103
APA StyleGage, R., Girling-Butcher, M., Joe, E., Smith, M., Ni Mhurchu, C., McKerchar, C., Puloka, V., McLean, R., & Signal, L. (2021). The Frequency and Context of Snacking among Children: An Objective Analysis Using Wearable Cameras. Nutrients, 13(1), 103. https://doi.org/10.3390/nu13010103