Effects of the Preschool-Based Family-Involving DAGIS Intervention Program on Children’s Energy Balance-Related Behaviors and Self-Regulation Skills: A Clustered Randomized Controlled Trial

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
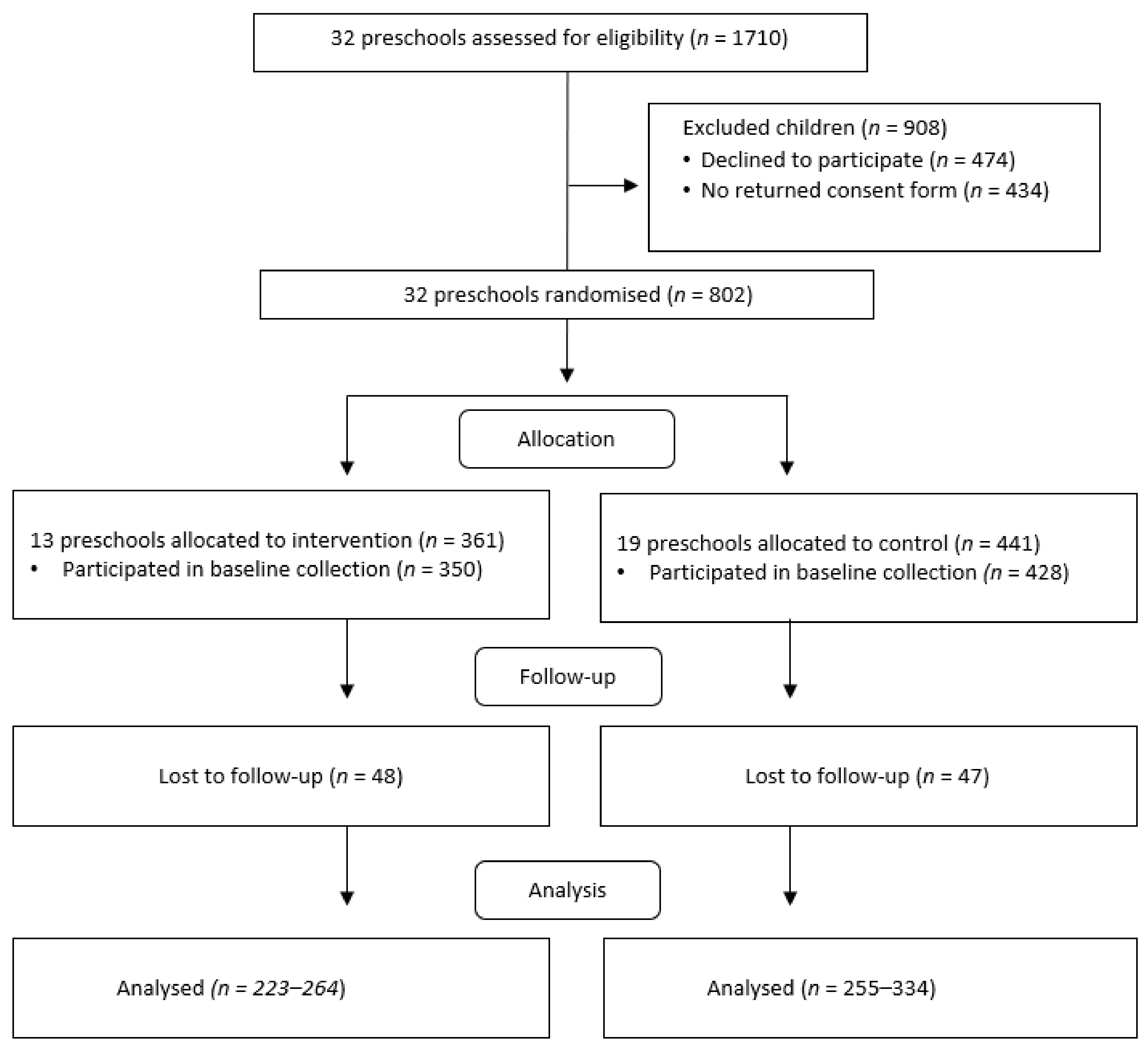
2.1. Recruitment
2.2. Ethical Issues
2.3. Data Collection and Measurements
2.3.1. Measurements
2.3.2. Parental Educational Level
2.3.3. Confounding Factors
2.4. Randomization, the Intervention, and the Program Content
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kremers, S.P.J.; de Bruijn, G.J.; Visscher, T.L.S.; van Mechelen, W.; de Vries, N.K.; Brug, J. Environmental Influences on Energy Balance-Related Behaviors: A Dual-Process View. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 1–10. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Report of the Comission on Ending Childhood Obesity; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Halfon, N.; Larson, K.; Slusser, W. Associations between Obesity and Comorbid Mental Health, Developmental, and Physical Health Conditions in a Nationally Representative Sample of US Children Aged 10 to 17. Acad. Pediatr. 2013, 13, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Methven, E.; Mcdowell, Z.C.; Hacking, B.; Alexander, D.; Stewart, L.; Kelnar, C.J.H. Health Consequences of Obesity. Arch. Dis. Child. 2003, 88, 748–752. [Google Scholar] [CrossRef] [PubMed]
- Mantziki, K.; Vassilopoulos, A.; Radulian, G.; Borys, J.-M.; Du Plessis, H.; Gregorio, M.J.; Graca, P.; De Henauw, S.; Handjiev, S.; Visscher, T. Inequities in Energy-Balance Related Behaviours and Family Environmental Determinants in European Children: Baseline Results of the Prospective EPHE Evaluation Study. BMC Public Health 2015, 15, 1203. [Google Scholar] [CrossRef]
- Fernandez-Alvira, J.; Mouratidou, T.; Bammann, K.; Hebestreit, A.; Barba, G.; Sieri, S.; Reisch, L.; Eiben, G.; Hadjigeorgiou, C.; Kovacs, E.; et al. Parental Education and Frequency of Food Consumption in European Children: The IDEFICS Study. Public Health Nutr. 2013, 16, 487–498. [Google Scholar] [CrossRef]
- Lehto, E.; Ray, C.; Vepsäläinen, H.; Korkalo, L.; Lehto, R.; Kaukonen, R.; Suhonen, E.; Nislin, M.; Nissinen, K.; Skaffari, E.; et al. Increased Health and Wellbeing in Preschools (DAGIS) Study—Differences in Children’s Energy Balance-Related Behaviors (EBRBs) and in Long-Term Stress by Parental Educational Level. Int. J. Environ. Res. Public Health 2018, 15, 2313. [Google Scholar] [CrossRef]
- Gubbels, J.S.; Van Kann, D.H.H.; de Vries, N.K.; Thijs, C.; Kremers, S.P.J. The next Step in Health Behavior Research: The Need for Ecological Moderation Analyses—An Application to Diet and Physical Activity at Childcare. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 52. [Google Scholar] [CrossRef]
- Gubbels, J.S.; Stessen, K.; Van De Kolk, I.; De Vries, N.K.; Thijs, C.; Kremers, S.P.J. Energy Balance-Related Parenting and Childcare Practices: The Importance of Meso-System Consistency. PLoS ONE 2018, 13, e0203689. [Google Scholar] [CrossRef]
- Määttä, S.; Lehto, R.; Nislin, M.; Ray, C.; Erkkola, M.; Sajaniemi, N.; Roos, E. Increased Health and Well-Being in Preschools (DAGIS): Rationale and Design for a Randomized Controlled Trial Health Behavior, Health Promotion and Society. BMC Public Health 2015, 15, 1–10. [Google Scholar] [CrossRef]
- Biddle, S.J.H.; Petrolini, I.; Pearson, N. Interventions Designed to Reduce Sedentary Behaviours in Young People: A Review of Reviews. Br. J. Sports Med. 2014, 48, 182–186. [Google Scholar] [CrossRef]
- Black, A.P.; D’Onise, K.; McDermott, R.; Vally, H.; O’Dea, K. How Effective Are Family-Based and Institutional Nutrition Interventions in Improving Children’s Diet and Health? A Systematic Review. BMC Public Health 2017, 17, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Pinket, A.S.; De Craemer, M.; Huybrechts, I.; De Bourdeaudhuij, I.; Deforche, B.; Cardon, G.; Androutsos, O.; Koletzko, B.; Moreno, L.A.; Socha, P.; et al. Multibehavioural Interventions with a Focus on Specific Energy Balance-Related Behaviours Can Affect Diet Quality in Preschoolers from Six European Countries: The Toybox-Study. Nutrients 2017, 9, 479. [Google Scholar] [CrossRef] [PubMed]
- Latomme, J.; Cardon, G.; De Bourdeaudhuij, I.; De Craemer, M.; Iotova, V.; Koletzko, B.; Socha, P.; Moreno, L.; Androutsos, O.; Manios, Y. Effect and Process Evaluation of a Kindergarten-Based, Family-Involved Intervention with a Randomized Cluster Design on Sedentary Behaviour in 4- to 6- Year Old European Preschool Children: The ToyBox-Study. PLoS ONE 2017, 12, e0172730. [Google Scholar] [CrossRef] [PubMed]
- Duncan, S.; Stewart, T.; McPhee, J.; Borotkanics, R.; Prendergast, K.; Zinn, C.; Meredith-Jones, K.; Taylor, R.; McLachlan, C.; Schofield, G. Efficacy of a Compulsory Homework Programme for Increasing Physical Activity and Improving Nutrition in Children: A Cluster Randomised Controlled Trial. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 80. [Google Scholar] [CrossRef] [PubMed]
- De Craemer, M.; De Decker, E.; Verloigne, M.; De Bourdeaudhuij, I.; Manios, Y.; Cardon, G. The Effect of a Cluster Randomised Control Trial on Objectively Measured Sedentary Time and Parental Reports of Time Spent in Sedentary Activities in Belgian Preschoolers: The ToyBox-Study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–17. [Google Scholar] [CrossRef]
- Marmot, M. Proportionate universalism. In The Health Gap—The Challenge of an Unequal World; Bloomsbury Publishing: London, UK, 2015; pp. 279–289. [Google Scholar]
- Wijtzes, A.I.; Van De Gaar, V.M.; Van Grieken, A.; De Kroon, M.L.A.; Mackenbach, J.P.; Van Lenthe, F.J.; Jansen, W.; Raat, H. Effectiveness of Interventions to Improve Lifestyle Behaviors among Socially Disadvantaged Children in Europe. Eur. J. Public Health 2017, 27, 240–247. [Google Scholar] [CrossRef]
- Love, R.E.; Adams, J.; van Sluijs, E.M.F. Equity Effects of Children’s Physical Activity Interventions: A Systematic Scoping Review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 134. [Google Scholar] [CrossRef]
- Downing, K.L.; Hnatiuk, J.A.; Hinkley, T.; Salmon, J.; Hesketh, K.D. Interventions to Reduce Sedentary Behaviour in 0–5-Year-Olds: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Br. J. Sports Med. 2018, 52, 314–321. [Google Scholar] [CrossRef]
- Aparicio, E.; Canals, J.; Arija, V.; De Henauw, S.; Michels, N. The Role of Emotion Regulation in Childhood Obesity: Implications for Prevention and Treatment. Nutr. Res. Rev. 2016, 29, 17–29. [Google Scholar] [CrossRef]
- Miller, A.L.; Lumeng, J.C. Pathways of Association from Stress to Obesity in Early Childhood. Obesity 2018, 26, 1117–1124. [Google Scholar] [CrossRef]
- Nigg, J.T. Annual Research Review: On the Relations among Self-Regulation, Self-Control, Executive Functioning, Effortful Control, Cognitive Control, Impulsivity, Risk-Taking, and Inhibition for Developmental Psychopathology. J. Child. Psychol. Psychiatry 2017, 58, 361–383. [Google Scholar] [CrossRef] [PubMed]
- Seeyave, D.M.; Coleman, S.; Appugliese, D.; Corwyn, R.F.; Bradley, R.H.; Davidson, N.S.; Kaciroti, N.; Lumeng, J.C. Ability to Delay Gratification at Age 4 Years and Risk of Overweight at Age 11 Years. Arch. Pediatr. Adolesc. Med. 2009, 163, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.; Matheson, B.E.; Kaye, W.H.; Boutelle, K.N. Neurocognitive Correlates of Obesity and Obesity-Related Behaviors in Children and Adolescents. Int. J. Obes. 2014, 38, 494–506. [Google Scholar] [CrossRef] [PubMed]
- Anderson, S.; Sacker, A.; Whitaker, R.; Kelly, Y. Self-Regulation and Household Routines at Age Three and Obesity at Age Eleven: Longitudinal Analysis of the UK Millennium Cohort Study. Int. J. Obes. 2017, 41, 1459–1466. [Google Scholar] [CrossRef]
- Lumeng, J.C.; Miller, A.L.; Horodynski, M.A.; Brophy-Herb, H.E.; Contreras, D.; Lee, H.; Sturza, J.; Kaciroti, N.; Peterson, K.E. Improving Self-Regulation for Obesity Prevention in Head Start: A Randomized Controlled Trial. Pediatrics 2017, 139, e20162047. [Google Scholar] [CrossRef]
- Ray, C.; Kaukonen, R.; Lehto, E.; Vepsäläinen, H.; Sajaniemi, N.; Erkkola, M.; Roos, E. Development of the DAGIS Intervention Study: A Preschool-Based Family-Involving Study Promoting Preschoolers’ Energy Balance-Related Behaviours and Self-Regulation Skills. BMC Public Health 2019, 19, 1670. [Google Scholar] [CrossRef]
- Eldredge, L.K.B.; Markham, C.M.; Ruiter, R.A.C.; Fernandez, M.E.; Parcel, G.S. Planning Health Promotion Programs—An Intervention Mapping Approach, 4th ed.; Jossey-Bass: San Fransisco, CA, USA, 2016. [Google Scholar]
- Säkkinen, S.; Kuoppala, T. Varhaiskasvatus 2017 (Children’s Day Care 2018); National Institute of Health and Welfare: Helsinki, Finland, 2018. Available online: http://urn.fi/URN:NBN:fi-fe2018100937865 (accessed on 24 August 2020).
- Korkalo, L.; Nissinen, K.; Skaffari, E.; Vepsäläinen, H.; Lehto, R.; Kaukonen, R.; Koivusilta, L.; Sajaniemi, N.; Roos, E.; Erkkola, M. The Contribution of Preschool Meals to the Diet of Finnish Preschoolers. Nutrients 2019, 11, 1531. [Google Scholar] [CrossRef]
- National Institute for Health and Welfare. The Welfare Compass for Monitoring Regional Welfare. Available online: https://www.hyvinvointikompassi.fi/en/web/hyvinvointikompassi/etusivu (accessed on 21 March 2019).
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef]
- Wen, L.; van der Ploeg, H.; Kite, J.; Cashmore, A.; Rissel, C. A Validation Study of Assessing Physical Activity and Sedentary Behavior in Children Aged 3 to 5 Years. Pediatr. Exerc. Sci. 2010, 22, 408–420. [Google Scholar] [CrossRef]
- Määttä, S.; Vepsäläinen, H.; Lehto, R.; Erkkola, M.; Roos, E.; Ray, C. Reproducibility of Preschool Personnel and Guardian Reports on Energy Balance-Related Behaviors and Their Correlates in Finnish Preschool Children. Children 2018, 5, 144. [Google Scholar] [CrossRef]
- Cliff, D.; Okely, A.; Smith, L.; McKeen, K. Relationships between Fundamental Movement Skills and Objectively Measured Physical Activity in Preschool Children. Pediatr. Exerc. Sci. 2009, 21, 436–449. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.; Catellier, D.; Gill, K.; McMurray, R. Calibration of Two Objective Measures of Physical Activity for Children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Korkalo, L.; Vepsäläinen, H.; Ray, C.; Skaffari, E.; Lehto, R.; Hauta-alus, H.; Nissinen, K.; Meinilä, J.; Erkkola, M.; Roos, E. Parents’ Reports of Preschoolers’ Diets: Relative Validity of a Food Frequency Questionnaire and Dietary Patterns. Nutrients 2019, 11, 159. [Google Scholar] [CrossRef] [PubMed]
- Maloney, J.E.; Lawlor, M.S.; Shonert-Reichl, K.A.; Whitehead, J. A universal, mindfulness-based social and emotional learning (SEL) Program designed to be implemented in schools by regular classroom teachers. In Handbook of Mindfulness in Education—Integrating Theory into Practice; Shonert-Reichl, K.A., Roeser, R.W., Eds.; Springer: New York, NY, USA, 2016; pp. 313–334. [Google Scholar]
- Carson, V.; Lee, E.Y.; Hesketh, K.D.; Hunter, S.; Kuzik, N.; Predy, M.; Rhodes, R.E.; Rinaldi, C.M.; Spence, J.C.; Hinkley, T. Physical Activity and Sedentary Behavior across Three Time-Points and Associations with Social Skills in Early Childhood. BMC Public Health 2019, 19, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Steene-Johannessen, J.; Hansen, B.; Dalene, K.; Kolle, E.; Northstone, K.; Møller, N.; Grøntved, A.; Wedderkopp, N.; Kriemler, S.; Page, A.; et al. Variations in Accelerometry Measured Physical Activity and Sedentary Time across Europe—Harmonized Analyses of 47,497 Children and Adolescents. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 38. [Google Scholar] [CrossRef] [PubMed]
- Brusseau, T.A. The Intricacies of Children’s Physical Activity. J. Hum. Kinet. 2015, 47, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Harrison, F.; Goodman, A.; van Sluijs, E.M.F.; Andersen, L.B.; Cardon, G.; Davey, R.; Janz, K.F.; Kriemler, S.; Molloy, L.; Page, A.S.; et al. Weather and Children’s Physical Activity; How and Why Do Relationships Vary between Countries? Int. J. Behav. Nutr. Phys. Act. 2017, 14, 74. [Google Scholar] [CrossRef]
- De Craemer, M.; Verloigne, M.; De Bourdeaudhuij, I.; Androutsos, O.; Iotova, V.; Moreno, L.; Koletzko, B.; Socha, P.; Manios, Y.; Cardon, G.; et al. Effect and Process Evaluation of a Kindergarten-Based, Family-Involved Cluster Randomised Controlled Trial in Six European Countries on Four- to Six-Year-Old Children’s Steps per Day: The ToyBox-Study. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 116. [Google Scholar] [CrossRef]
- Bellows, L.; Davies, P.; Anderson, J.; Kennedy, C. Effectiveness of a Physical Activity Intervention for Head Start Preschoolers: A Randomized Intervention Study. Am. J. Occup. Ther. 2013, 67, 28–36. [Google Scholar] [CrossRef]
- Reilly, J.; Kelly, L.; Montgomery, C.; Williamson, A.; Fisher, A.; McColl, J.; Lo Conte, R.; Paton, J.; Grant, S. Physical Activity to Prevent Obesity in Young Children: Cluster Randomised Controlled Trial. BMJ Open 2006, 333, 1041. [Google Scholar] [CrossRef]
- Buscemi, J.; Odoms-Young, A.; Stolley, M.R.; Schiffer, L.; Blumstein, L.; Clark, M.H.; Berbaum, M.L.; McCaffrey, J.; Braunschweig, C.; Fitzgibbon, M.L. Comparative Effectiveness Trial of an Obesity Prevention Intervention in EFNEP and SNAP-ED: Primary Outcomes. Nutrients 2019, 11, 1012. [Google Scholar] [CrossRef] [PubMed]
- Rios, L.M.; Serrano, M.M.; Aguilar, A.J.; Chacón, L.B.; Neria, C.R.; Monreal, L.A. Promoting Fruit, Vegetable and Simple Water Consumption among Mothers and Teachers of Preschool Children: An Intervention Mapping Initiative. Eval. Program Plann. 2019, 76, 101675. [Google Scholar] [CrossRef] [PubMed]
- Wolfenden, L.; Barnes, C.; Jones, J.; Finch, M.; Wyse, R.; Kingsland, M.; Tzelepis, F.; Grady, A.; Hodder, R.; Booth, D.; et al. Strategies to Improve the Implementation of Healthy Eating, Physical Activity and Obesity Prevention Policies, Practices or Programmes within Childcare Services. Cochrane Database Syst. Rev. 2020, 2, CD011779. [Google Scholar] [CrossRef] [PubMed]
- Steenbock, B.; Buck, C.; Zeeb, H.; Rach, S.; Pischke, C.R. Impact of the Intervention Program “JolinchenKids-Fit and Healthy in Daycare” on Energy Balance Related-Behaviors: Results of a Cluster Controlled Trial. BMC Pediatr. 2019, 19, 432. [Google Scholar] [CrossRef] [PubMed]
- Halle, T.G.; Darling-Churchill, K.E. Review of Measures of Social and Emotional Development. J. Appl. Dev. Psychol. 2016, 45, 8–18. [Google Scholar] [CrossRef]
- Prevo, L.; Kremers, S.; Jansen, M. Small Successes Make Big Wins: A Retrospective Case Study towards Community Engagement of Low-SES Families. Int. J. Environ. Res. Public Health 2020, 17, 612. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Control | Intervention | p-Value | ||||
|---|---|---|---|---|---|---|
| n | Mean ± SD * | n | Mean ± SD * | |||
| Child’s Age c | 441 | 5.24 ± 1.06 | 360 | 5.14 ± 1.04 | 0.060 a | |
| n | % | n | % | |||
| Child’s gender | girl | 203 | 46.0% | 172 | 47.8% | 0.496 b |
| boy | 238 | 54.0% | 188 | 52.2% | ||
| Parental educational level d | low | 116 | 29.9% | 109 | 35.4% | <0.001 b |
| middle | 169 | 43.6% | 143 | 46.4% | ||
| high | 103 | 26.5% | 56 | 18.2% | ||
| Municipality | Salo | 357 | 81.0% | 306 | 84.8% | 0.040 b |
| Riihimäki | 84 | 19.0% | 55 | 15.2% | ||
| EBRBs and SR Skills * | Baseline | Follow-Up | ||||||
|---|---|---|---|---|---|---|---|---|
| Control | Intervention | Control | Intervention | |||||
| n | Mean ± SD ** | n | Mean ± SD ** | n | Mean ± SD ** | n | Mean ± SD ** | |
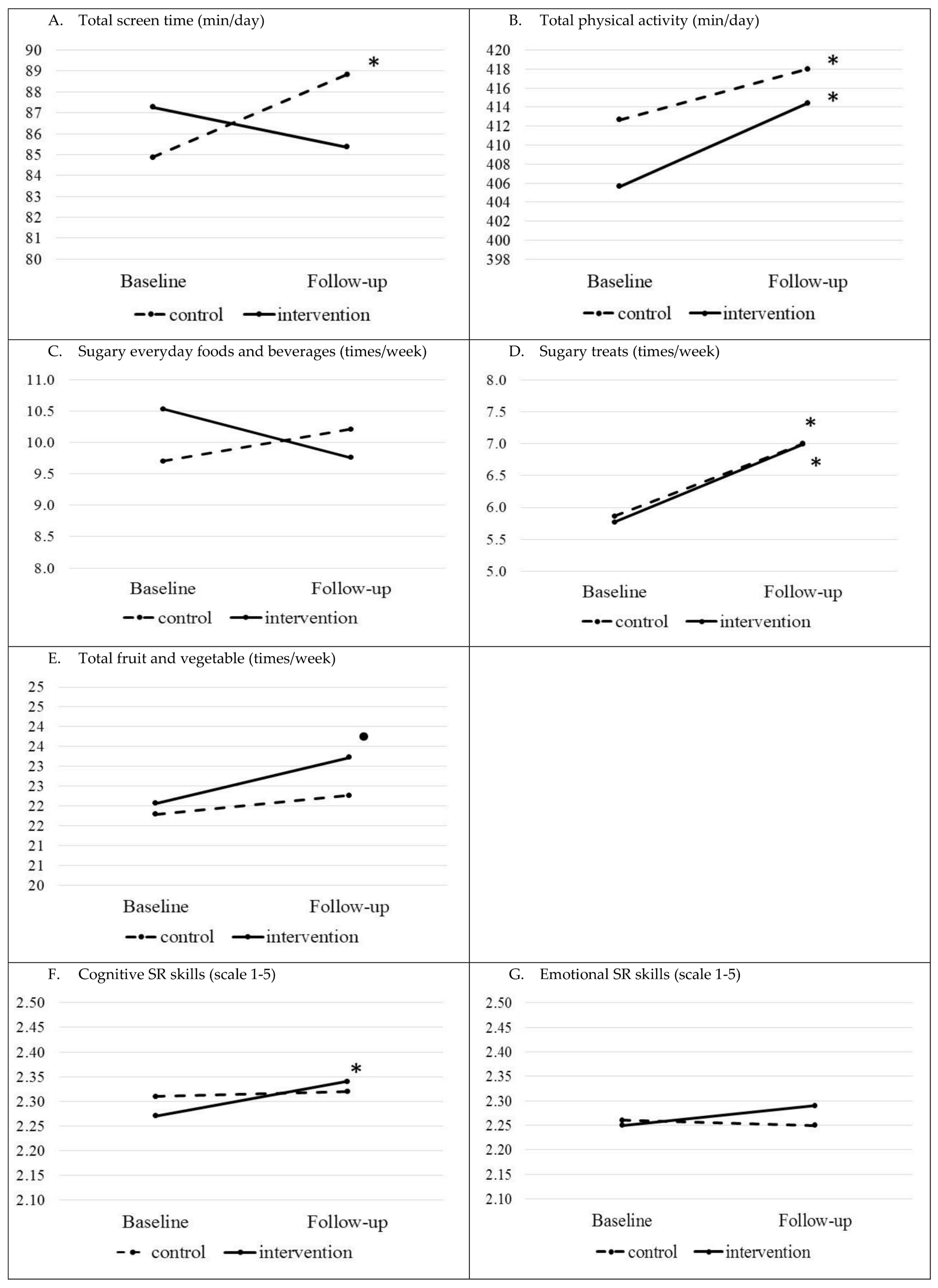
| Total screen time (min/day) | 370 | 84.87 ± 43.45 | 303 | 87.27 ± 44.06 | 325 | 88.84 ± 42.47 | 261 | 85.37 ± 41.34 |
| Total physical activity a (min/day) | 335 | 412.68 ± 48.40 | 282 | 405.66 ± 48.61 | 270 | 418.02 ± 45.34 | 210 | 414.42 ± 50.42 |
| Sugary everyday food and beverages (times/week) | 307 | 9.70 ± 6.89 | 293 | 10.53 ± 7.84 | 241 | 10.21± 8.96 | 200 | 9.76 ± 6.88 |
| Sugary treats (times/week) | 318 | 5.86 ± 3.99 | 299 | 5.77 ± 3.21 | 236 | 7.00 ± 5.34 | 192 | 6.99 ± 5.34 |
| Fruit and vegetables (times/week) | 323 | 21.79 ± 10.67 | 298 | 22.06 ± 13.12 | 258 | 22.26 ± 11.38 | 200 | 23.22 ± 13.39 |
| Cognitive SR skills (scale 1–3) | 383 | 2.31 ± 0.39 | 313 | 2.27 ± 0.43 | 324 | 2.32 ± 0.41 | 256 | 2.34 ± 0.43 |
| Emotional SR skills (scale 1–3) | 383 | 2.26 ± 0.51 | 313 | 2.25 ± 0.52 | 324 | 2.25 ± 0.51 | 256 | 2.29 ± 0.53 |
| General Linear Mixed Model c | Linear Mixed Models with Repeated Measures | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Children’s EBRBs and SR Skills | Comparison between Intervention and Control Group at Follow-Up c | Change between Follow-Up and Baseline in Control Group | Change between Follow-Up and Baseline in Intervention Group | ||||||
| (95% C.I.) | p-Value | diff F–B | (95% C.I.) | p-Value | diff F–B | (95% C.I.) | p-Value | ||
| Total screen time (min/day) a | −4.20 | (−9.86; 1.46) | 0.146 | 4.46 | (0.48; 8.44) | 0.028 | −1.42 | (−5.86; 3.01) | 0.529 |
| Total physical activity (min/day) b | −0.56 | (−6.65; 5.53) | 0.858 | 23.77 | (18.57; 28.97) | <0.001 | 27.30 | (21.74; 32.86) | <0.001 |
| Sugary food and beverage (times/week) a | −0.57 | (−2.09; 0.96) | 0.466 | 0.51 | (−0.42; 1.43) | 0.285 | −0.79 | (−1.77; 0.19) | 0.112 |
| Sugary treats (times/week) a | −0.13 | (−1.03; 0.78) | 0.781 | 1.20 | (0.62; 1.77) | <0.001 | 1.28 | (0.67; 1.90) | <0.001 |
| Fruit and vegetables (times/week) a | 1.43 | (−0.64; 3.49) | 0.176 | −0.37 | (−1.63; 0.89) | 0.565 | 1.21 | (−0.18; 2.61) | 0.088 |
| Cognitive SR skills (scale 1–3) a | 0.02 | (−0.04; 0.08) | 0.505 | 0.01 | (−0.03; 0.05) | 0.574 | 0.06 | (0.01; 0.11) | 0.011 |
| Emotional SR skills (1–3) a | −0.03 | (−0.04; 0.10) | 0.405 | 0.004 | (−0.04; 0.05) | 0.858 | 0.04 | (−0.02; 0.09) | 0.195 |
| General Mixed Model | Linear Mixed Models with Repeated Measures | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Children’s EBRBs and SR Skills | PEL | Comparison between Intervention and Control Group at Follow-Up c | Comparison between Follow-Up and Baseline in Control Group | Comparison between Follow-Up and Baseline in Intervention Group | ||||||
| (95% C.I.) | p-Value | diff F-B | (95% C.I.) | p-Value | diff F-B | (95% C.I.) | p-Value | |||
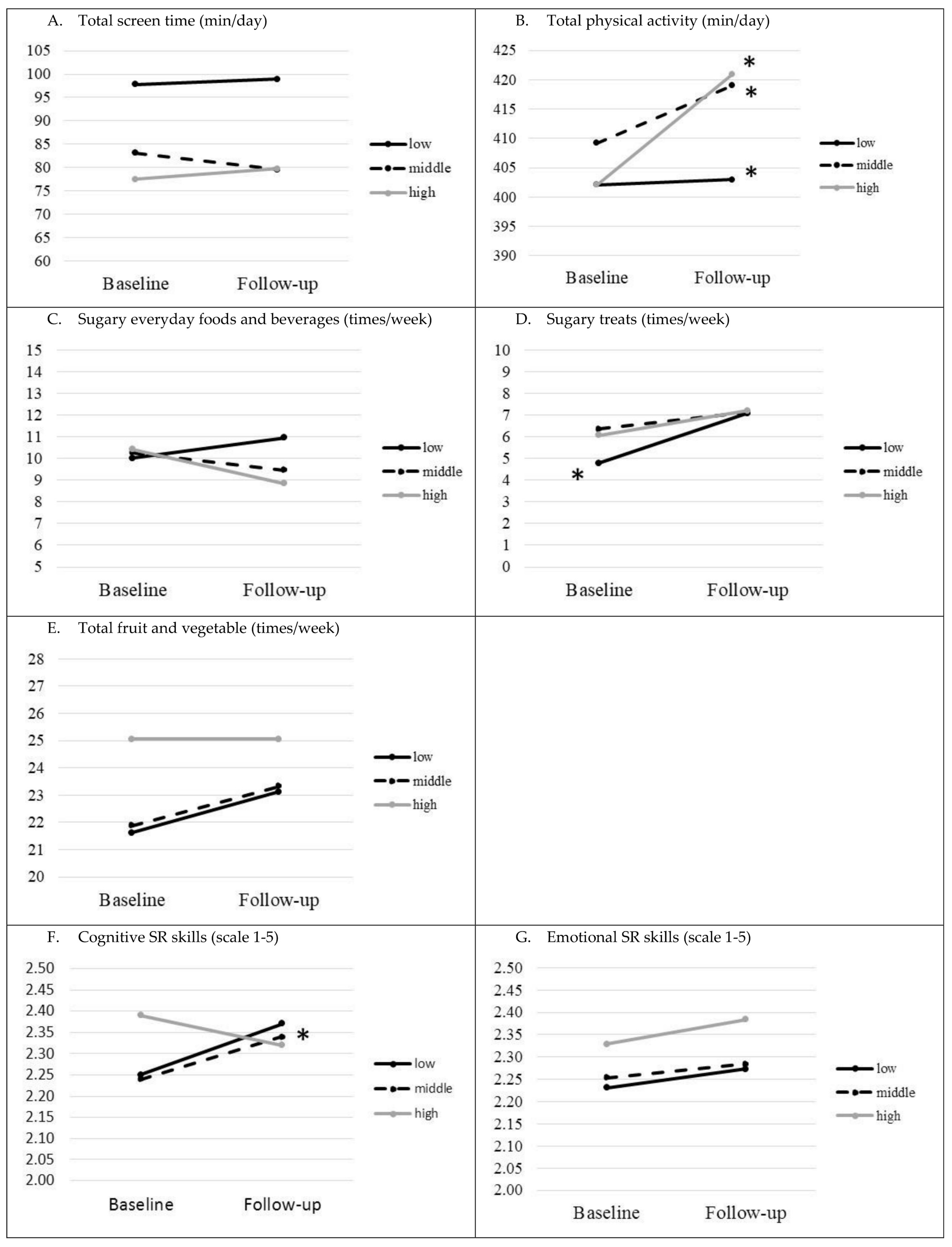
| Total screen time (min/day) a | low | −1.69 | (−12.30; 8.92) | 0.753 | 1.95 | (−5.74; 9.64) | 0.619 | −3.42 | (−11.23; 4.40) | 0.391 |
| middle | −7.88 | (−16.60; 0.84) | 0.076 | 4.05 | (−1.87; 9.98) | 0.179 | −2.00 | (−8.57; 4.57) | 0.551 | |
| high | −3.73 | (−16.13; 8.66) | 0.553 | 7.65 | (−0.10; 15.39) | 0.053 | 2.95 | (−6.86; 12.76) | 0.555 | |
| Total physical activity (min/day) b | low | −7.17 | (−24.15; 9.80) | 0.404 | 21.41 | (11.82; 31.00) | <0.001 | 22.10 | (12.89; 31.32) | <0.001 |
| middle | 1.86 | (−11.90; 15.63) | 0.787 | 26.61 | (19.56; 33.66) | <0.001 | 30.89 | (22.96; 38.83) | <0.001 | |
| high | −0.77 | (−19.96; 18.42) | 0.937 | 21.10 | (12.08; 30.13) | <0.001 | 27.66 | (16.37; 38.95) | <0.001 | |
| Sugary foods and beverages (times/week) a | low | −0.15 | (−2.70; 2.41) | 0.909 | 0.83 | (−1.07; 2.74) | 0.392 | 0.10 | (−1.71; 1.92) | 0.911 |
| middle | −1.08 | (−3.08; 0.93) | 0.286 | 0.61 | (−0.75; 1.96) | 0.380 | −0.88 | (−2.26; 0.50) | 0.210 | |
| high | −1.34 | (−4.14; 1.45) | 0.344 | 0.09 | (−1.64; 1.81) | 0.920 | −1.91 | (−4.12; 0.31) | 0.092 | |
| Sugary treats (times/week) a | low | −0.79 | (−2.86; 1.29) | 0.454 | 2.17 | (0.97; 3.37) | <0.001 | 2.22 | (1.15; 3.29) | <0.001 |
| middle | 0.52 | (−1.19; 2.22) | 0.545 | 0.93 | (0.10; 1.75) | 0.027 | 0.74 | (−0.17; 1.65) | 0.109 | |
| high | −0.07 | (−2.32; 2.18) | 0.954 | 0.89 | (−0.18; 1.96) | 0.103 | 1.02 | (−0.34; 2.38) | 0.140 | |
| Fruit and vegetables (times/week) a | low | 2.99 | (−1.00; 6.98) | 0.141 | −0.14 | (−2.75; 2.47) | 0.915 | 1.51 | (−0.98; 3.99) | 0.235 |
| middle | 0.59 | (−2.56; 3.74) | 0.710 | 0.37 | (−1.49; 2.23) | 0.695 | 1.43 | (−0.61; 3.48) | 0.169 | |
| high | 1.03 | (−3.30; 5.37) | 0.638 | −1.68 | (−3.96; 0.60) | 0.149 | 0.31 | (−2.74; 3.36) | 0.841 | |
| Cognitive SR skills (scale 1–3) a | low | 0.11 | (0.00; 0.21) | 0.051 | −0.11 | (−0.22; 0.00) | 0.052 | 0.04 | (−0.08; 0.15) | 0.513 |
| middle | 0.001 | (−0.09; 0.09) | 0.987 | −0.03 | (−0.13; 0.06) | 0.468 | 0.10 | (0.01; 0.20) | 0.038 | |
| high | −0.06 | (−0.18; 0.07) | 0.380 | 0.04 | (−0.09; 0.18) | 0.536 | −0.04 | (−0.18; 0.09) | 0.543 | |
| Emotional SR skills (scale 1–3) a | low | 0.01 | (−0.12; 0.13) | 0.921 | −0.02 | (−0.11; 0.08) | 0.750 | 0.03 | (−0.07; 0.12) | 0.563 |
| middle | 0.05 | (−0.05; 0.15) | 0.313 | −0.02 | (−0.09; 0.05) | 0.547 | 0.04 | (−0.04; 0.12) | 0.286 | |
| high | 0.01 | (−0.13; 0.16) | 0.861 | 0.07 | (−0.02; 0.16) | 0.141 | 0.03 | (−0.09; 0.15) | 0.611 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ray, C.; Figuereido, R.; Vepsäläinen, H.; Lehto, R.; Pajulahti, R.; Skaffari, E.; Sainio, T.; Hiltunen, P.; Lehto, E.; Korkalo, L.; et al. Effects of the Preschool-Based Family-Involving DAGIS Intervention Program on Children’s Energy Balance-Related Behaviors and Self-Regulation Skills: A Clustered Randomized Controlled Trial. Nutrients 2020, 12, 2599. https://doi.org/10.3390/nu12092599
Ray C, Figuereido R, Vepsäläinen H, Lehto R, Pajulahti R, Skaffari E, Sainio T, Hiltunen P, Lehto E, Korkalo L, et al. Effects of the Preschool-Based Family-Involving DAGIS Intervention Program on Children’s Energy Balance-Related Behaviors and Self-Regulation Skills: A Clustered Randomized Controlled Trial. Nutrients. 2020; 12(9):2599. https://doi.org/10.3390/nu12092599
Chicago/Turabian StyleRay, Carola, Rejane Figuereido, Henna Vepsäläinen, Reetta Lehto, Riikka Pajulahti, Essi Skaffari, Taina Sainio, Pauliina Hiltunen, Elviira Lehto, Liisa Korkalo, and et al. 2020. "Effects of the Preschool-Based Family-Involving DAGIS Intervention Program on Children’s Energy Balance-Related Behaviors and Self-Regulation Skills: A Clustered Randomized Controlled Trial" Nutrients 12, no. 9: 2599. https://doi.org/10.3390/nu12092599
APA StyleRay, C., Figuereido, R., Vepsäläinen, H., Lehto, R., Pajulahti, R., Skaffari, E., Sainio, T., Hiltunen, P., Lehto, E., Korkalo, L., Sääksjärvi, K., Sajaniemi, N., Erkkola, M., & Roos, E. (2020). Effects of the Preschool-Based Family-Involving DAGIS Intervention Program on Children’s Energy Balance-Related Behaviors and Self-Regulation Skills: A Clustered Randomized Controlled Trial. Nutrients, 12(9), 2599. https://doi.org/10.3390/nu12092599