Markers of Bone Health and Impact of Whey Protein Supplementation in Army Initial Entry Training Soldiers: A Double-Blind Placebo-Controlled Study

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
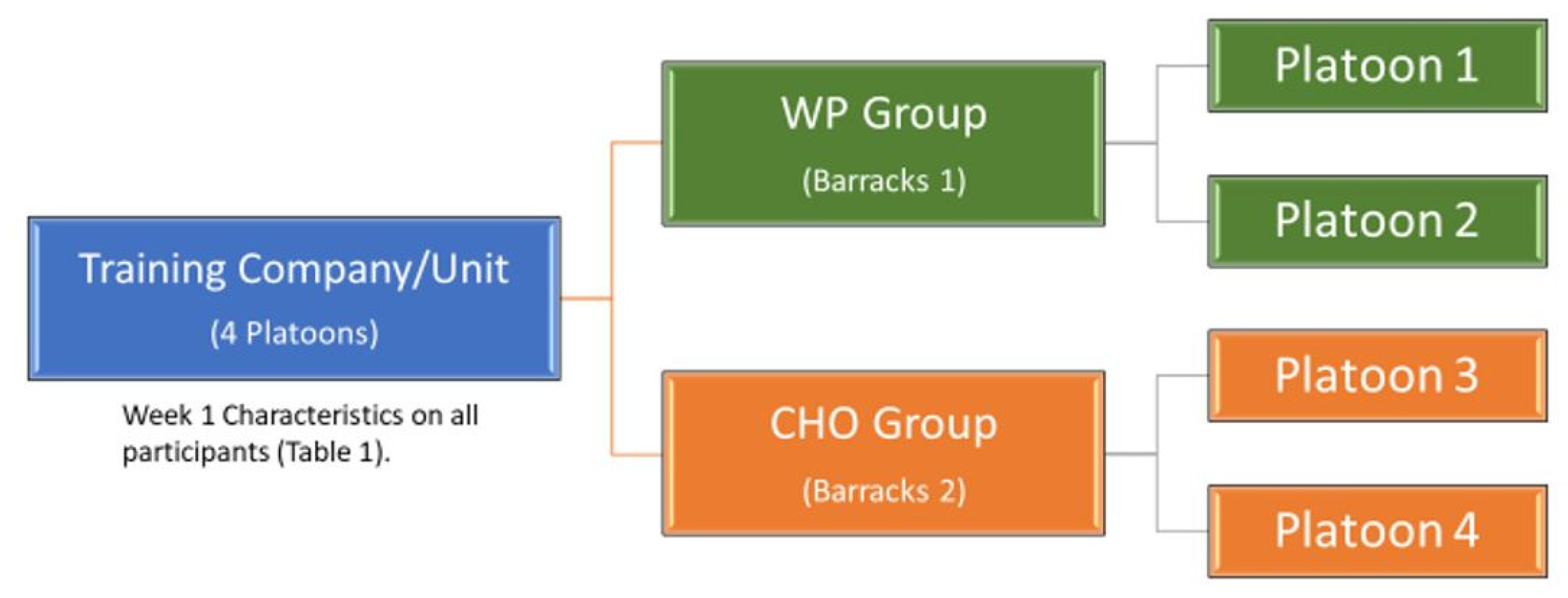
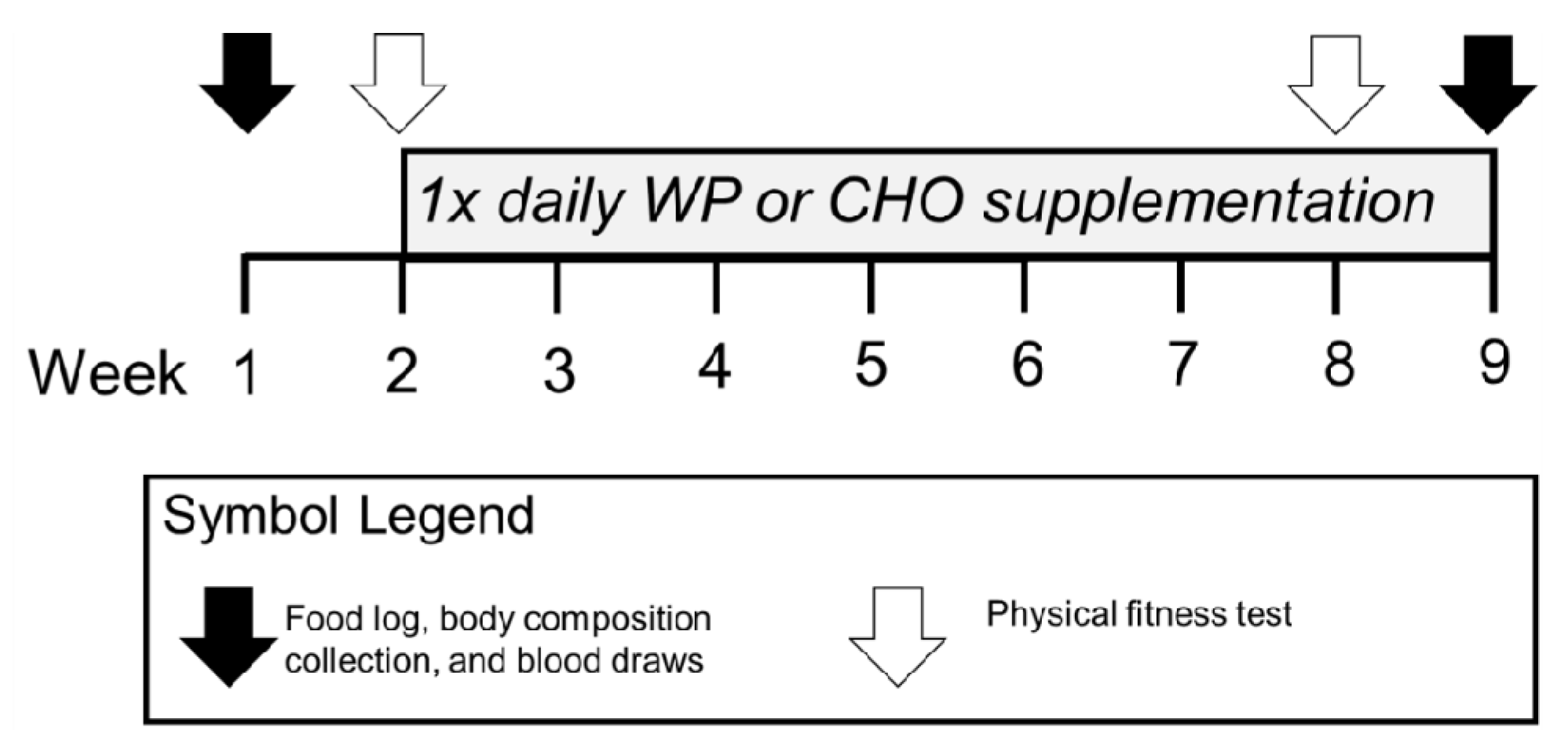
2.1. Study Design and Population
2.2. Intervention
2.3. Outcome Measures
2.4. Body Measures
2.5. Height and Weight
2.6. Body Composition
2.7. Physiological Biomarkers
2.8. Statistical Analysis
3. Results
3.1. Baseline Analysis
3.2. Effects of Supplements
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| IET | Initial Entry Training |
| P1NP | Procollagen type 1N propeptide |
| CTX | C-terminal crosslinking telopeptide of type 1 collagen |
| FM | Fat Mass |
| FFM | Fat Free Mass |
| WP | Whey Protein |
| CHO | Carbohydrate |
| ACSM | American College of Sports Medicine |
| APFT | Army Physical Fitness Test |
References
- Almeida, S.A.; Williams, K.M.; Shaffer, R.A.; Brodine, S.K. Epidemiological patterns of musculoskeletal injuries and physical training. Med. Sci. Sports Exerc. 1999, 31, 1176–1182. [Google Scholar] [CrossRef]
- Piantanida, N.A.; Knapik, J.J.; Brannen, S.; O’Connor, F. Injuries during Marine Corps officer basic training. Mil. Med. 2000, 165, 515–520. [Google Scholar] [CrossRef]
- Shaffer, R.A.; Brodine, S.K.; Ito, S.I.; Le, A.T. Epidemiology of illness and injury among U.S. Navy and Marine Corps female training populations. Mil. Med. 1999, 164, 17–21. [Google Scholar] [CrossRef]
- Shaffer, R.A.; Rauh, M.J.; Brodine, S.K.; Trone, D.W.; Macera, C.A. Predictors of stress fracture susceptibility in young female recruits. Am. J. Sports Med. 2006, 34, 108–115. [Google Scholar] [CrossRef]
- Trone, D.W.; Cipriani, D.J.; Raman, R.; Wingard, D.L.; Shaffer, R.A.; Macera, C.A. Self-reported smoking and musculoskeletal overuse injury among male and female U.S. Marine Corps recruits. Mil. Med. 2014, 179, 735–743. [Google Scholar] [CrossRef] [PubMed]
- Knapik, J.J.; Brosch, L.C.; Venuto, M.; Swedler, D.I.; Bullock, S.H.; Gaines, L.S.; Murphy, R.J.; Tchandja, J.; Jones, B.H. Effect on injuries of assigning shoes based on foot shape in air force basic training. Am. J. Prev. Med. 2010, 38, S197–S211. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.; Woodward, A. Risk factors for injury during basic military training. Is there a social element to injury pathogenesis? J. Occup. Med. 1994, 36, 1120–1126. [Google Scholar] [CrossRef] [PubMed]
- Devlin, J.D.; Knapik, J.J.; Solomon, Z.; Hauret, K.G.; Morris, K.; Carter, R.; McGill, R.; Paoli, L. Incidence of admission to the physical training and rehabilitation programs in initial entry training during fiscal year 2011. Mil. Med. 2014, 179, 547–552. [Google Scholar] [CrossRef][Green Version]
- Kelly, E.W.; Bradway, L.F. A team approach to the treatment of musculoskeletal injuries suffered by Navy recruits: A method to decrease attrition and improve quality of care. Mil. Med. 1997, 162, 354–359. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Trone, D.W.; Cipriani, D.J.; Raman, R.; Wingard, D.L.; Shaffer, R.A.; Macera, C.A. The association of self-reported measures with poor training outcomes among male and female U.S. Navy recruits. Mil. Med. 2013, 178, 43–49. [Google Scholar] [CrossRef]
- Bergman, B.P.; Miller, S.A. Unfit for further service: Trends in medical discharge from the British Army 1861-1998. J. R. Army Med. Corps 2000, 146, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Bergman, B.P.; Miller, S.A. Equal opportunities, equal risks? Overuse injuries in female military recruits. J. Public Health Med. 2001, 23, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Geary, K.G.; Irvine, D.; Croft, A.M. Does military service damage females? An analysis of medical discharge data in the British armed forces. Occup. Med. 2002, 52, 85–90. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sharma, J.; Greeves, J.P.; Byers, M.; Bennett, A.N.; Spears, I.R. Musculoskeletal injuries in British Army recruits: A prospective study of diagnosis-specific incidence and rehabilitation times. BMC Musculoskelet. Disord. 2015, 16, 106. [Google Scholar] [CrossRef] [PubMed]
- Moran, D.S.; Evans, R.K.; Hadad, E. Imaging of lower extremity stress fracture injuries. Sports Med. 2008, 38, 345–356. [Google Scholar] [CrossRef]
- Knapik, J.J.; Sharp, M.A.; Darakjy, S.; Jones, S.B.; Hauret, K.G.; Jones, B.H. Temporal changes in the physical fitness of US Army recruits. Sports Med. 2006, 36, 613–634. [Google Scholar] [CrossRef]
- Knapik, J.J.; Darakjy, S.; Hauret, K.G.; Canada, S.; Scott, S.; Rieger, W.; Marin, R.; Jones, B.H. Increasing the physical fitness of low-fit recruits before basic combat training: An evaluation of fitness, injuries, and training outcomes. Mil. Med. 2006, 171, 45–54. [Google Scholar] [CrossRef]
- Taanila, H.; Suni, J.H.; Kannus, P.; Pihlajamaki, H.; Ruohola, J.P.; Viskari, J.; Parkkari, J. Risk factors of acute and overuse musculoskeletal injuries among young conscripts: A population-based cohort study. BMC Musculoskelet. Disord. 2015, 16, 104. [Google Scholar] [CrossRef]
- Nindl, B.C.; Williams, T.J.; Deuster, P.A.; Butler, N.L.; Jones, B.H. Strategies for optimizing military physical readiness and preventing musculoskeletal injuries in the 21st century. US Army Med. Dep. J. 2013, 20, 5–23. [Google Scholar]
- Knapik, J.; Montain, S.J.; McGraw, S.; Grier, T.; Ely, M.; Jones, B.H. Stress fracture risk factors in basic combat training. Int. J. Sports Med. 2012, 33, 940–946. [Google Scholar] [CrossRef]
- Evans, R.K.; Antczak, A.J.; Lester, M.; Yanovich, R.; Israeli, E.; Moran, D.S. Effects of a 4-month recruit training program on markers of bone metabolism. Med. Sci. Sports Exerc. 2008, 40, S660–S670. [Google Scholar] [CrossRef] [PubMed]
- Lutz, L.J.; Karl, J.P.; Rood, J.C.; Cable, S.J.; Williams, K.W.; Young, A.J.; McClung, J.P. Vitamin D status, dietary intake, and bone turnover in female Soldiers during military training: A longitudinal study. J. Int. Soc. Sports Nutr. 2012, 9, 38. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, M.S.; Loan, L.A.; Azuero, A.; Hobbs, C. The consequences of modern military deployment on calcium status and bone health. Nurs. Clin. N. Am. 2010, 45, 109–122. [Google Scholar] [CrossRef] [PubMed]
- Johansson, H.; Oden, A.; Kanis, J.A.; McCloskey, E.V.; Morris, H.A.; Cooper, C.; Vasikaran, S. A meta-analysis of reference markers of bone turnover for prediction of fracture. Calcif. Tissue Int. 2014, 94, 560–567. [Google Scholar] [CrossRef]
- Rosen, H.N.; Moses, A.C.; Garber, J.; Iloputaife, I.D.; Ross, D.S.; Lee, S.L.; Greenspan, S.L. Serum CTX: A new marker of bone resorption that shows treatment effect more often than other markers because of low coefficient of variability and large changes with bisphosphonate therapy. Calcif. Tissue Int. 2000, 66, 100–103. [Google Scholar] [CrossRef]
- Rantalainen, T.; Heinonen, A.; Linnamo, V.; Komi, P.V.; Takala, T.E.; Kainulainen, H. Short-term bone biochemical response to a single bout of high-impact exercise. J. Sports Sci. Med. 2009, 8, 553–559. [Google Scholar]
- Mosti, M.P.; Kaehler, N.; Stunes, A.K.; Hoff, J.; Syversen, U. Maximal strength training in postmenopausal women with osteoporosis or osteopenia. J. Strength Cond. Res. 2013, 27, 2879–2886. [Google Scholar] [CrossRef]
- Ogata, M.; Ide, R.; Takizawa, M.; Tanaka, M.; Tetsuo, T.; Sato, A.; Iwasaki, N.; Uchigata, Y. Association between basal metabolic function and bone metabolism in postmenopausal women with type 2 diabetes. Nutrition 2015, 31, 1394–1401. [Google Scholar] [CrossRef]
- Tenforde, A.S.; Sayres, L.C.; Sainani, K.L.; Fredericson, M. Evaluating the relationship of calcium and vitamin D in the prevention of stress fracture injuries in the young athlete: A review of the literature. PM R 2010, 2, 945–949. [Google Scholar] [CrossRef]
- Lappe, J.; Cullen, D.; Haynatzki, G.; Recker, R.; Ahlf, R.; Thompson, K. Calcium and vitamin d supplementation decreases incidence of stress fractures in female navy recruits. J. Bone Miner. Res. 2008, 23, 741–749. [Google Scholar] [CrossRef]
- Gaffney-Stomberg, E.; Lutz, L.J.; Rood, J.C.; Cable, S.J.; Pasiakos, S.M.; Young, A.J.; McClung, J.P. Calcium and vitamin D supplementation maintains parathyroid hormone and improves bone density during initial military training: A randomized, double-blind, placebo controlled trial. Bone 2014, 68, 46–56. [Google Scholar] [CrossRef]
- McAdam, J.S.; McGinnis, K.D.; Beck, D.T.; Haun, C.T.; Romero, M.A.; Mumford, P.W.; Roberson, P.A.; Young, K.C.; Lohse, K.R.; Lockwood, C.M.; et al. Effect of Whey Protein Supplementation on Physical Performance and Body Composition in Army Initial Entry Training Soldiers. Nutrients 2018, 10, 1248. [Google Scholar] [CrossRef] [PubMed]
- McGinnis, K.D.; McAdam, J.S.; Lockwood, C.M.; Young, K.C.; Roberts, M.D.; Sefton, J.M. Impact of Protein and Carbohydrate Supplementation on Musculoskeletal Injuries in Army Initial Entry Training Soldiers. Nutrients 2018, 10, 1938. [Google Scholar] [CrossRef] [PubMed]
- Lutz, L.J.; Gaffney-Stomberg, E.; Karl, J.P.; Hughes, J.M.; Guerriere, K.I.; McClung, J.P. Dietary Intake in Relation to Military Dietary Reference Values During Army Basic Combat Training; a Multi-center, Cross-sectional Study. Mil. Med. 2019, 184, e223–e230. [Google Scholar] [CrossRef]
- McLellan, T.M. Protein supplementation for military personnel: A review of the mechanisms and performance outcomes. J. Nutr. 2013, 143, 1820S–S1833S. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bihuniak, J.D.; Insogna, K.L. The effects of dietary protein and amino acids on skeletal metabolism. Mol. Cell. Endocrinol. 2015, 410, 78–86. [Google Scholar] [CrossRef]
- Uenishi, K.; Ishida, H.; Toba, Y.; Aoe, S.; Itabashi, A.; Takada, Y. Milk basic protein increases bone mineral density and improves bone metabolism in healthy young women. Osteoporos. Int. 2007, 18, 385–390. [Google Scholar] [CrossRef]
- Huang, W.C.; Chang, Y.C.; Chen, Y.M.; Hsu, Y.J.; Huang, C.C.; Kan, N.W.; Chen, S.S. Whey Protein Improves Marathon-Induced Injury and Exercise Performance in Elite Track Runners. Int. J. Med. Sci. 2017, 14, 648–654. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.D.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Montain, S.J.; McGraw, S.M.; Ely, M.R.; Grier, T.L.; Knapik, J.J. A retrospective cohort study on the influence of UV index and race/ethnicity on risk of stress and lower limb fractures. BMC Musculoskelet. Disord. 2013, 14, 135. [Google Scholar] [CrossRef]
- Fraser, W.D.; Colston, K.W.; Stevenson, J.C. Bone and Calcium Metabolism. In The Immunoassay Handbook, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2013; pp. 705–720. [Google Scholar]
- McAdam, J.; McGinnis, K.; Ory, R.; Young, K.; Fruge, A.D.; Roberts, M.; Sefton, J. Estimation of energy balance and training volume during Army Initial Entry Training. J. Int. Soc. Sports Nutr. 2018, 15, 55. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, N.; Black, M.; Paul, E.; Pasco, J.A.; Kotowicz, M.A.; Schneider, H.G. Age-related reference intervals for bone turnover markers from an Australian reference population. Bone 2013, 55, 271–276. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, T.J.; Izard, R.M.; Walsh, N.P.; Tang, J.C.Y.; Fraser, W.D.; Greeves, J.P. Skeletal macro- and microstructure adaptations in men undergoing arduous military training. Bone 2019, 125, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Ihle, R.; Loucks, A.B. Dose-response relationships between energy availability and bone turnover in young exercising women. J. Bone Miner. Res. 2004, 19, 1231–1240. [Google Scholar] [CrossRef]
- Flakoll, P.J.; Judy, T.; Flinn, K.; Carr, C.; Flinn, S. Postexercise protein supplementation improves health and muscle soreness during basic military training in Marine recruits. J. Appl. Physiol. 1985 2004, 96, 951–956. [Google Scholar] [CrossRef]
- Boone, C.H.; Stout, J.R.; Beyer, K.S.; Fukuda, D.H.; Hoffman, J.R. Muscle strength and hypertrophy occur independently of protein supplementation during short-term resistance training in untrained men. Appl. Physiol. Nutr. Metab. 2015, 40, 797–802. [Google Scholar] [CrossRef]
- Morton, R.W.; Murphy, K.T.; McKellar, S.R.; Schoenfeld, B.J.; Henselmans, M.; Helms, E.; Aragon, A.A.; Devries, M.C.; Banfield, L.; Krieger, J.W.; et al. A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. Br. J. Sports Med. 2018, 52, 376–384. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Caucasian (N = 36) | Other (N = 54) | Combined (N = 90) | p-Value |
|---|---|---|---|---|
| Age (years) | 0.52 | |||
| Mean (SD) | 21.806 (3.54) | 22.30 (3.50) | 22.10 (3.51) | |
| Range | 18.00–35.00 | 18.00–32.00 | 18.00–35.000 | |
| Height (cm) | 0.002 | |||
| Mean (SD) | 176.97 (7.27) | 171.97 (7.44) | 173.97 (7.74) | |
| Range | 160.30–191.90 | 157.50–189.50 | 157.500–191.900 | |
| Weight (kg) | 0.25 | |||
| Mean (SD) | 78.85 (13.90) | 75.28 (14.41) | 76.71 (14.24) | |
| Range | 57.00–117.40 | 50.30–107.30 | 50.30–117.40 | |
| FFM (kg) | 0.29 | |||
| Mean (SD) | 61.64 (9.36) | 59.45 (9.72) | 60.33 (9.59) | |
| Range | 49.04–84.81 | 43.08–87.94 | 43.08–87.94 | |
| FM (kg) | 0.35 | |||
| Mean (SD) | 17.21 (6.73) | 15.82 (6.92) | 16.38 (6.84) | |
| Range | 6.43–32.59 | 1.57–35.14 | 1.57–35.14 | |
| P1NP (ng/mL) | 0.72 | |||
| N | 15 | 32 | 47 | |
| Mean (SD) | 86.63 (40.09) | 81.82 (45.15) | 84.17 (42.31) | |
| Range | 33.68–184.38 | 36.52–200.20 | 33.68–200.20 | |
| CTX (ng/L) | 0.09 | |||
| N | 10 | 21 | 31 | |
| Mean (SD) | 788.43 (282.30) | 654.68 (307.66) | 713.62 (301.76) | |
| Range | 377.12–1557.95 | 235.82–1589.58 | 235.82–1589.58 | |
| Vitamin D (ng/mL) | 0.04 | |||
| N | 16 | 33 | 49 | |
| Mean (SD) | 24.50 (9.25) | 19.42 (5.82) | 21.90 (8.01) | |
| Range | 14.10–45.67 | 7.71–27.56 | 7.71–45.67 | |
| Calcium (mg/dL) | 0.68 | |||
| N | 16 | 24 | 40 | |
| Mean (SD) | 8.37 (0.49) | 8.42 (0.43) | 8.40 (0.45) | |
| Range | 7.50–9.30 | 7.60–9.40 | 7.50–9.40 |
| Parameter | P1NP | CTX |
|---|---|---|
| (Intercept) | 87.77 *** | 767.51 *** |
| (74.68, 100.85) | (664.41, 870.60) | |
| Age (years) | −4.39 ** | −26.63 * |
| (−7.28, −1.50) | (−49.35, -3.90) | |
| FM (kg) | −3.06 *** | −11.54 |
| (−4.63, −1.48) | (−23.37, 0.29) | |
| Ethnicity (CC/Other) | −15.54 | −110.29 |
| (−34.29, 3.21) | (−248.26, 27.67) | |
| Run Time (s) | −0.93 | |
| (−2.12, 0.26) | ||
| N | 42 | 59 |
| R2 | 0.48 | 0.32 |
| Variable | Mean Diff (SD) | Effect Size (95% CI) | Category |
|---|---|---|---|
| P1NP | |||
| WP | 3.577 (23.639) | 0.084 (−0.168 to 0.337) | Negligible |
| CHO | 5.857 (23.343) | 0.135 (−0.098 to 0.368) | Negligible |
| CTX | |||
| WP | −10.513 (262.353) | −0.040 (−0.458 to 0.378) | Negligible |
| CHO | 14.752 (236.728) | 0.043 (−0.236 to 0.322) | Negligible |
| Ratio | |||
| WP | 0.006 (0.060) | 0.088 (-0.347 to 0.523) | Negligible |
| CHO | 0.016 (0.044) | 0.342 (-0.082 to 0.766) | Small |
| Calcium | |||
| WP | −0.138 (0.511) | −0.333 (−0.981 to 0.316) | Small |
| CHO | −0.067 (0.440) | −0.142 (−0.53 to 0.245) | Negligible |
| Vitamin D | |||
| WP | 3.255 (6.142) | 0.380 (0.024 to 0.735) | Small |
| CHO | 4.722 (3.814) | 0.965 (0.559 to 1.371) | Large |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sefton, J.M.; Lyons, K.D.; Beck, D.T.; Haun, C.T.; Romero, M.A.; Mumford, P.W.; Roberson, P.A.; Young, K.C.; Roberts, M.D.; McAdam, J.S. Markers of Bone Health and Impact of Whey Protein Supplementation in Army Initial Entry Training Soldiers: A Double-Blind Placebo-Controlled Study. Nutrients 2020, 12, 2225. https://doi.org/10.3390/nu12082225
Sefton JM, Lyons KD, Beck DT, Haun CT, Romero MA, Mumford PW, Roberson PA, Young KC, Roberts MD, McAdam JS. Markers of Bone Health and Impact of Whey Protein Supplementation in Army Initial Entry Training Soldiers: A Double-Blind Placebo-Controlled Study. Nutrients. 2020; 12(8):2225. https://doi.org/10.3390/nu12082225
Chicago/Turabian StyleSefton, JoEllen M., Kaitlin D. Lyons, Darren T. Beck, Cody T. Haun, Matthew A. Romero, Petey W. Mumford, Paul A. Roberson, Kaelin C. Young, Michael D. Roberts, and Jeremy S. McAdam. 2020. "Markers of Bone Health and Impact of Whey Protein Supplementation in Army Initial Entry Training Soldiers: A Double-Blind Placebo-Controlled Study" Nutrients 12, no. 8: 2225. https://doi.org/10.3390/nu12082225
APA StyleSefton, J. M., Lyons, K. D., Beck, D. T., Haun, C. T., Romero, M. A., Mumford, P. W., Roberson, P. A., Young, K. C., Roberts, M. D., & McAdam, J. S. (2020). Markers of Bone Health and Impact of Whey Protein Supplementation in Army Initial Entry Training Soldiers: A Double-Blind Placebo-Controlled Study. Nutrients, 12(8), 2225. https://doi.org/10.3390/nu12082225