Relationship between Magnesium Intake and Chronic Pain in U.S. Adults


Abstract
1. Introduction
2. Materials and Methods
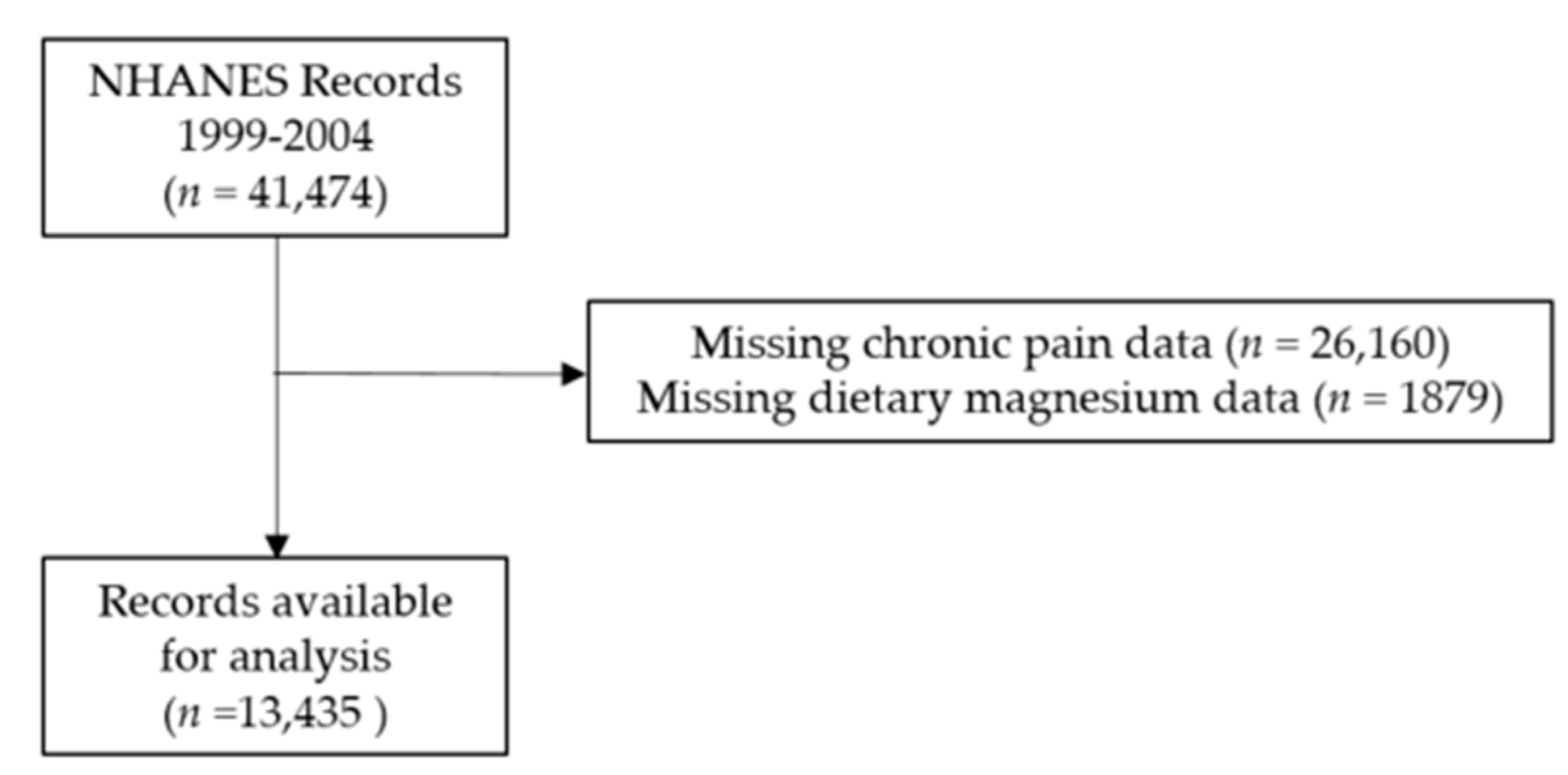
2.1. Data Source and Subjects
2.2. Variables
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Dahlhamer, J.; Lucas, J.; Zelaya, C.; Nahin, R.; Mackey, S.; DeBar, L.; Kerns, R.; Von Korff, M.; Porter, L.; Helmick, C. Prevalence of chronic pain and high-impact chronic pain among adults—United States, 2016. Morb. Mortal. Wkly. Rep. 2018, 67, 1001. [Google Scholar] [CrossRef]
- Simon, L.S. Relieving pain in America: A blueprint for transforming prevention, care, education, and research. J. Pain Palliat. Care Pharmacother. 2012, 26, 197–198. [Google Scholar] [CrossRef]
- US Department of Health and Human Services. Office of Disease Prevention Health Promotion; Healthy People 2020: Washington, DC, USA, 2014.
- Dowell, D.; Haegerich, T.M.; Chou, R. CDC Guideline for Prescribing Opioids for Chronic Pain—United States, 2016CDC Guideline for Prescribing Opioids for Chronic Pain, 2016CDC Guideline for Prescribing Opioids for Chronic Pain, 2016. JAMA J. Am. Med Assoc. 2016, 315, 1624–1645. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Michalsen, A. Management of chronic pain using complementary and integrative medicine. BMJ 2017, 357, j1284. [Google Scholar] [CrossRef]
- Frieden, T.R.; Houry, D. Reducing the risks of relief—the CDC opioid-prescribing guideline. N. Engl. J. Med. 2016, 374, 1501–1504. [Google Scholar] [CrossRef]
- Tick, H.; Nielsen, A.; Pelletier, K.R.; Bonakdar, R.; Simmons, S.; Glick, R.; Ratner, E.; Lemmon, R.L.; Wayne, P.; Zador, V. Evidence-based nonpharmacologic strategies for comprehensive pain care: The Consortium Pain Task Force white paper. Explore 2018, 14, 177–211. [Google Scholar] [CrossRef]
- Ehde, D.M.; Dillworth, T.M.; Turner, J.A. Cognitive-behavioral therapy for individuals with chronic pain: Efficacy, innovations, and directions for research. Am. Psychol. 2014, 69, 153. [Google Scholar] [CrossRef]
- Hilton, L.; Hempel, S.; Ewing, B.A.; Apaydin, E.; Xenakis, L.; Newberry, S.; Colaiaco, B.; Maher, A.R.; Shanman, R.M.; Sorbero, M.E. Mindfulness meditation for chronic pain: Systematic review and meta-analysis. Ann. Behav. Med. 2016, 51, 199–213. [Google Scholar] [CrossRef]
- Knoerl, R.; Lavoie Smith, E.M.; Weisberg, J. Chronic pain and cognitive behavioral therapy: An integrative review. West. J. Nurs. Res. 2016, 38, 596–628. [Google Scholar] [CrossRef]
- MacPherson, H.; Vertosick, E.; Foster, N.; Lewith, G.; Linde, K.; Sherman, K.; Witt, C.; Vickers, A. The persistence of the effects of acupuncture after a course of treatment: A meta-analysis of patients with chronic pain. Pain 2017, 158, 784. [Google Scholar] [CrossRef]
- Skelly, A.C.; Chou, R.; Dettori, J.R.; Turner, J.A.; Friedly, J.L.; Rundell, S.D.; Fu, R.; Brodt, E.D.; Wasson, N.; Winter, C. Noninvasive Nonpharmacological Treatment for Chronic Pain: A Systematic Review; Agency for Heathcare Research and Quality: Rockville, MD, USA, 2018.
- Tamin, T.Z.; Murdana, N.; Pitoyo, Y.; Safitri, E.D. Exercise Intervention for Chronic Pain Management, Muscle Strengthening, and Functional Score in Obese Patients with Chronic Musculoskeletal Pain: A Systematic Review and Meta-analysis. Acta Med. Indones. 2018, 50, 299–308. [Google Scholar]
- Turner, J.A.; Holtzman, S.; Mancl, L. Mediators, moderators, and predictors of therapeutic change in cognitive–behavioral therapy for chronic pain. Pain 2007, 127, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Vickers, A.J.; Cronin, A.M.; Maschino, A.C.; Lewith, G.; MacPherson, H.; Foster, N.E.; Sherman, K.J.; Witt, C.M.; Linde, K.; Acupuncture Trialists’ Collaboration, f.t. Acupuncture for chronic pain: Individual patient data meta-analysis. Arch. Intern. Med. 2012, 172, 1444–1453. [Google Scholar] [CrossRef]
- de Williams de, C.; Amanda, C.; Eccleston, C.; Morley, S. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst. Rev. 2012, 11, CD007407. [Google Scholar] [CrossRef] [PubMed]
- Substance Abuse and Mental Health Services Administration. Results from the 2013 National Survey on Drug Use and Health: Summary of National Findings; NSDUH Series H-48; HHS Publication No.(SMA) 14-4863; U.S. Department of Health and Human Services: Rockville, MD, USA, 2014.
- Malpuech-Brugere, C.; Nowacki, W.; Daveau, M.; Gueux, E.; Linard, C.; Rock, E.; Lebreton, J.; Mazur, A.; Rayssiguier, Y. Inflammatory response following acute magnesium deficiency in the rat. Biochim. Et Biophys. Acta 2000, 1501, 91–98. [Google Scholar] [CrossRef]
- Volpe, S.L. Magnesium in disease prevention and overall health. Adv. Nutr. 2013, 4, 378s–383s. [Google Scholar] [CrossRef]
- de Baaij, J.H.; Hoenderop, J.G.; Bindels, R.J. Magnesium in man: Implications for health and disease. Physiol. Rev. 2015, 95, 1–46. [Google Scholar] [CrossRef]
- Grober, U.; Schmidt, J.; Kisters, K. Magnesium in prevention and therapy. Nutrients 2015, 7, 8199–8226. [Google Scholar] [CrossRef]
- Rosanoff, A.; Weaver, C.M.; Rude, R.K. Suboptimal magnesium status in the United States: Are the health consequences underestimated? Nutr. Rev. 2012, 70, 153–164. [Google Scholar] [CrossRef]
- Nielsen, F.H.; Milne, D.B.; Gallagher, S.; Johnson, L.; Hoverson, B. Moderate magnesium deprivation results in calcium retention and altered potassium and phosphorus excretion by postmenopausal women. Magnes. Res. Off. Organ Int. Soc. Dev. Res. Magnes. 2007, 20, 19–31. [Google Scholar]
- Tarleton, E.K.; Littenberg, B. Magnesium intake and depression in adults. J. Am. Board Fam. Med. 2015, 28, 249–256. [Google Scholar] [CrossRef]
- Tarleton, E.K. Factors influencing magnesium consumption among adults in the United States. Nutr. Rev. 2018. [Google Scholar] [CrossRef]
- Banerjee, S.; Jones, S. CADTH Rapid Response Reports: Magnesium as an Alternative or Adjunct to Opioids for Migraine and Chronic Pain: A Review of the Clinical Effectiveness and Guidelines; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2017.
- Centers for Disease Control and Prevention. Questionnaires, Datasets, and Related Documentation. Available online: http://www.cdc.gov/nchs/nhanes/nhanes_questionnaires.htm (accessed on 20 May 2020).
- Johnson, C.L.; Paulose-Ram, R.; Ogden, C.L. National Health and Nutrition Examination Survey: Analytic Guidelines 1999–2010. Vital Health Stat 2013, 2. [Google Scholar]
- National Center for Health Statistics. National Health and Nutrition Examination Survey: Analytic Guidelines, 2011–2014 and 2015–2016. Available online: https://wwwn.cdc.gov/nchs/nhanes/AnalyticGuidelines.aspx (accessed on 20 May 2020).
- Ismail, Y.; Ismail, A.A. The underestimated problem of using serum magnesium measurements to exclude magnesium deficiency in adults; a health warning is needed for "normal" results. Clin. Chem. Lab. Med. Cclm Fescc 2010, 48, 323–327. [Google Scholar] [CrossRef]
- Institute of Medicine. Dietary Reference Intakes: Calcium, Phosphorous, Magnesium, Vitamin D, and Flouride; National Academy Press: Washington, DC, USA, 1997. [Google Scholar]
- Ford, E.S.; Mokdad, A.H. Dietary magnesium intake in a national sample of US adults. J. Nutr. 2003, 133, 2879–2882. [Google Scholar] [CrossRef]
- Moshfegh, A.; Goldman, J.; Cleveland, L. What We Eat in America, NHANES 2001–2002: Usual Nutrient Intakes from Food Compared to Dietary Reference Intakes. 28 March. Available online: https://www.ars.usda.gov/ARSUserFiles/80400530/pdf/0102/usualintaketables2001-02.pdf (accessed on 28 March 2020).
- Moshfegh, A.; Goldman, J.; Ahuja, J.; Rhodes, D.; LaComb, R. What We Eat in America, NHANES 2005–2006: Usual Nutrient Intakes from Food and Water Compared to 1997 Dietary Reference Intakes for Vitamin D, Calcium, Phosphorous, and Magnesium. Available online: https://www.ars.usda.gov/ARSUserFiles/80400530/pdf/0506/usual_nutrient_intake_vitD_ca_phos_mg_2005-06.pdf (accessed on 13 March 2020).
- Oliveira, A.R.; Cruz, K.J.; Severo, J.S.; Morais, J.B.; Freitas, T.E.; Araujo, R.S.; Marreiro, D.D. Hypomagnesemia and its relation with chronic low-grade inflammation in obesity. Rev. da Assoc. Med. Bras. 2017, 63, 156–163. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, A.R.S.; Cruz, K.J.C.; Morais, J.B.S.; Severo, J.S.; De Freitas, T.E.C.; Veras, A.L.; da Rocha Romero, A.B.; Colli, C.; do Nascimento Nogueira, N.; Torres-Leal, F.L. Magnesium status and its relationship with C-reactive protein in obese women. Biol. Trace Elem. Res. 2015, 168, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Kreutzwiser, D.; Tawfic, Q.A. Expanding Role of NMDA Receptor Antagonists in the Management of Pain. Cns Drugs 2019, 33, 347–374. [Google Scholar] [CrossRef] [PubMed]
- Alexa, T.; Marza, A.; Voloseniuc, T.; Tamba, B. Enhanced analgesic effects of tramadol and common trace element coadministration in mice. J. Neurosci. Res. 2015, 93, 1534–1541. [Google Scholar] [CrossRef]
- Chiu, H.Y.; Yeh, T.H.; Huang, Y.C.; Chen, P.Y. Effects of Intravenous and Oral Magnesium on Reducing Migraine: A Meta-analysis of Randomized Controlled Trials. Pain Physician 2016, 19, E97–E112. [Google Scholar]
- Choi, H.; Parmar, N. The use of intravenous magnesium sulphate for acute migraine: Meta-analysis of randomized controlled trials. Eur. J. Emerg. Med. Off. J. Eur. Soc. Emerg. Med. 2014, 21, 2–9. [Google Scholar] [CrossRef]
- Bagis, S.; Karabiber, M.; As, I.; Tamer, L.; Erdogan, C.; Atalay, A. Is magnesium citrate treatment effective on pain, clinical parameters and functional status in patients with fibromyalgia? Rheumatol. Int. 2013, 33, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Engen, D.J.; McAllister, S.J.; Whipple, M.O.; Cha, S.S.; Dion, L.J.; Vincent, A.; Bauer, B.A.; Wahner-Roedler, D.L. Effects of transdermal magnesium chloride on quality of life for patients with fibromyalgia: A feasibility study. J. Integr. Med. 2015, 13, 306–313. [Google Scholar] [CrossRef]
- Pickering, G.; Morel, V.; Simen, E.; Cardot, J.M.; Moustafa, F.; Delage, N.; Picard, P.; Eschalier, S.; Boulliau, S.; Dubray, C. Oral magnesium treatment in patients with neuropathic pain: A randomized clinical trial. Magnes. Res. Off. Organ Int. Soc. Dev. Res. Magnes. 2011, 24, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Tarleton, E.K.; Littenberg, B.; MacLean, C.D.; Kennedy, A.G.; Daley, C. Role of magnesium supplementation in the treatment of depression: A randomized clinical trial. PLoS ONE 2017, 12, e0180067. [Google Scholar] [CrossRef] [PubMed]
- Kantor, E.D.; Rehm, C.D.; Du, M.; White, E.; Giovannucci, E.L. Trends in dietary supplement use among us adults from 1999–2012. JAMA J. Am. Med Assoc. 2016, 316, 1464–1474. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. The National Health and Nutritiona Examination Survey Documentation, Codebook, and Frequencies; Dietary Interview—Individual Foods, First Day; CDC: Atlanta, GA, USA, 2008.



{kind=link}
{kind=link}
| Variable | Control | Chronic Pain | |||||
|---|---|---|---|---|---|---|---|
| N | Mean or Percent | Standard Deviation | N | Mean or Percent | Standard Deviation | p | |
| Mg intake/body weight (mg/kg) | 11,280 | 3.7 | 2.1 | 1898 | 3.3 | 1.9 | <0.001 |
| Total Mg intake (mg) | 11,488 | 275 | 145 | 1947 | 262 | 142 | 0.003 |
| Total Energy Intake (kcal/day) | 11,488 | 2111 | 1015 | 1947 | 2044 | 1016 | 0.006 |
| Mg intake/energy intake (mg/kcal) | 11,486 | 0.14 | 0.05 | 1947 | 0.13 | 0.05 | 0.90 |
| Mg intake ≥ EAR | 11,488 | 35% | 1947 | 32% | 0.015 | ||
| Age (year) | 11,488 | 49.4 | 19.3 | 1947 | 52.4 | 17.1 | <0.001 |
| Age ≥ 65 | 11,488 | 27% | 1947 | 26% | 0.98 | ||
| Male Gender | 11,488 | 48% | 1947 | 43% | 0.004 | ||
| BMI (kg/m2) | 11,197 | 28.2 | 6.1 | 1869 | 29.6 | 7.1 | <0.001 |
| Race | |||||||
| Non-Hispanic White | 5637 | 49.1% | 1140 | 58.6% | <0.001 | ||
| Non-Hispanic Black | 2195 | 19.1% | 359 | 18.4% | |||
| Mexican American | 2714 | 23.6% | 311 | 16.0% | |||
| Other Hispanic | 541 | 4.7% | 72 | 3.7% | |||
| Other Race | 401 | 3.5% | 65 | 3.3% | |||
| Daily Activity | <0.001 | ||||||
| Sitting | 2807 | 24.5% | 639 | 32.9% | |||
| Walking | 6163 | 53.7% | 918 | 47.3% | |||
| Walking and Light Lifting | 1758 | 15.3% | 275 | 14.2% | |||
| Walking and Heavy Lifting | 749 | 6.5% | 110 | 5.7% | |||
| Alcohol Intake per Week | 10,889 | 2.9 | 7.1 | 1869 | 2.9 | 8.6 | 0.80 |
| Current Smoker | 11,471 | 20% | 1946 | 29% | <0.001 | ||
| High School Graduate | 11,463 | 68% | 1946 | 68% | 0.011 | ||
| Low Household Income | 10,713 | 48% | 1848 | 54% | 0.003 | ||
| Currently Married or Living as Married | 11,081 | 62% | 1885 | 62% | 0.026 | ||
| Kidney Dysfunction | 11,151 | 12% | 1891 | 16% | <0.001 | ||
| Atherosclerotic Disease | 11,488 | 10% | 1947 | 20% | <0.001 | ||
| Rheumatoid Arthritis | 11,475 | 5% | 1938 | 12% | <0.001 | ||
| Osteoarthritis | 11,475 | 6% | 1938 | 17% | <0.001 | ||
| Chronic Obstructive Pulmonary Disease | 11,488 | 4% | 1947 | 9% | <0.001 | ||
| Diabetes Mellitus | 11,488 | 12% | 1947 | 17% | <0.001 | ||
| Obese | 11,197 | 31% | 1869 | 41% | <0.001 | ||
| All | Females | Males | Age < 65 | Age 65+ | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| (n = 11,105) | (n = 5780) | (n = 5325) | (n = 8188) | (n = 2917) | ||||||
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
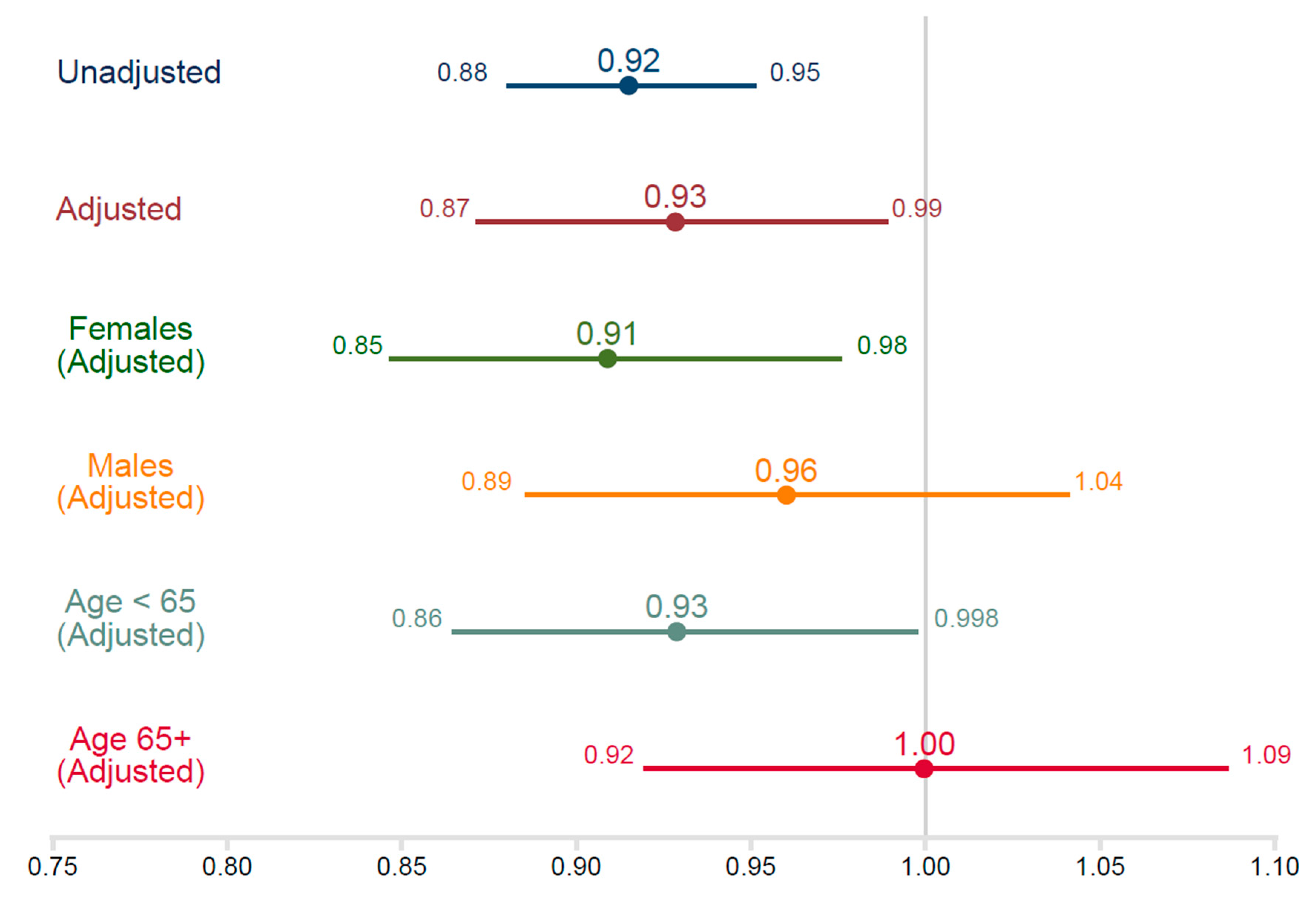
| Mg intake/body weight (mg/kg) | 0.93 * | 0.87, 0.99 | 0.91 * | 0.85, 0.98 | 0.96 | 0.89, 1.04 | 0.93 * | 0.86, 0.998 | 1.00 | 0.92, 1.09 |
| Age (year) | 1.00 | 0.99, 1.00 | 1.00 | 0.99, 1.00 | 1.00 | 0.99, 1.01 | -- | -- | -- | -- |
| Male Gender | 0.79 ** | 0.68, 0.91 | -- | -- | -- | -- | 0.81 * | 0.69, 0.95 | 0.70 * | 0.52, 0.94 |
| Race | ||||||||||
| White | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- | 1.00 | -- |
| Mexican American | 0.49 ** | 0.40, 0.60 | 0.62 ** | 0.47, 0.81 | 0.35 ** | 0.25, 0.50 | 0.45 ** | 0.36, 0.56 | 0.66 | 0.43, 1.01 |
| Other Hispanic | 0.70 * | 0.49, 1.00 | 0.62 | 0.35, 1.09 | 0.79 | 0.43, 1.45 | 0.64 * | 0.44, 0.94 | 0.79 | 0.39, 1.60 |
| Non-Hispanic Black | 0.76 * | 0.62, 0.93 | 0.73 * | 0.53, 0.92 | 0.78 | 0.56, 1.08 | 0.70 * | 0.55, 0.89 | 0.81 | 0.55, 1.19 |
| Other Race | 0.88 | 0.58, 1.32 | 0.99 | 0.61, 1.62 | 0.72 | 0.39, 1.33 | 0.78 | 0.51, 1.19 | 0.97 | 0.43, 2.19 |
| Low Household Income | 1.20 * | 1.00, 1.44 | 1.18 | 0.95, 1.45 | 0.72 | 0.39, 1.33 | 1.39 ** | 1.14, 1.69 | 0.82 | 0.61, 1.12 |
| High School Graduate | 0.93 | 0.80, 1.07 | 0.93 | 0.77, 1.13 | 0.94 | 0.73, 1.21 | 0.92 | 0.78, 1.09 | 0.79 | 0.55, 1.12 |
| Currently Married | 1.37 ** | 1.18, 1.59 | 0.93 | 0.77, 1.13 | 1.75 ** | 1.34, 1.2.28 | 1.38 ** | 1.18, 1.62 | 1.03 | 0.78, 1.35 |
| Total Daily Calorie Intake | 1.00 | 1.00. 1.00 | 1.00 | 1.00. 1.00 | 1.00 | 1.00. 1.00 | 1.00 | 1.00, 1.00 | 1.00 | 1.00, 1.00 |
| Daily Activity | ||||||||||
| Sitting | 1.00 | 1.00. 1.00 | 1.00 | 1.00. 1.00 | 1.00 | 1.00. 1.00 | 1.00 | 1.00. 1.00 | 1.00 | 1.00. 1.00 |
| Walking | 0.86 | 0.74, 1.01 | 0.82 | 0.65, 1.04 | 0.92 | 0.76, 1.12 | 0.86 | 0.70, 1.04 | 1.00 | 0.76, 1.32 |
| Walking and Light Lifting | 0.88 | 0.74, 1.05 | 0.93 | 0.69, 1.23 | 0.85 | 0.63, 1.13 | 0.86 | 0.70, 1.06 | 0.98 | 0.57, 1.67 |
| Walking and Heavy Lifting | 1.04 | 0.81, 1.33 | 1.39 | 0.75, 2.59 | 0.95 | 0.75, 1.20 | 1.00 | 0.76, 1.31 | 1.40 | 0.50, 3.93 |
| Current Smoker | 1.69 ** | 1.43, 2.00 | 1.70 ** | 1.39, 2.08 | 1.74 ** | 1.39, 2.17 | 1.59 ** | 1.33, 1.89 | 1.16 | 0.76, 1.78 |
| Alcohol Intake per Week | 1.01 | 1.00, 1.01 | 0.99 | 0.97, 1.02 | 1.01 * | 1.00, 1.02 | 1.01 | 1.00, 1.01 | 1.00 | 0.98, 1.02 |
| Kidney Dysfunction | 1.11 | 0.88, 1.39 | 1.04 | 0.78, 1.40 | 1.26 | 0.86, 1.83 | 1.40 * | 1.02, 1.93 | 0.95 | 0.72, 1.26 |
| Atherosclerotic Disease | 1.56 ** | 1.24, 1.94 | 1.55 * | 1.15, 2.08 | 1.51 * | 1.14, 2.01 | 1.84 ** | 1.32, 2.57 | 1.70 ** | 1.35, 2.15 |
| Rheumatoid Arthritis | 3.27 ** | 2.64, 4.05 | 2.61 ** | 1.97, 3.44 | 4.34 ** | 3.09, 6.11 | 3.86 ** | 2.86, 5.21 | 2.03 ** | 1.39, 3.00 |
| Osteoarthritis | 3.04 ** | 2.39, 3.87 | 3.02 ** | 2.27, 4.01 | 3.08 ** | 2.14, 4.43 | 3.98 ** | 2.98, 5.31 | 2.05 ** | 1.46, 2.86 |
| Chronic Obstructive Pulmonary Disease | 1.70 ** | 1.32, 2.20 | 1.68 ** | 1.28, 2.21 | 1.78 * | 1.10, 2.81 | 1.76 * | 1.21, 2.57 | 1.58 | 0.98, 2.56 |
| Diabetes Mellitus | 1.30 * | 1.08, 1.58 | 1.48 ** | 1.20, 1.82 | 1.10 | 0.82, 1.47 | 1.29 * | 1.01, 1.65 | 1.39 * | 1.01, 1.03 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarleton, E.K.; Kennedy, A.G.; Rose, G.L.; Littenberg, B. Relationship between Magnesium Intake and Chronic Pain in U.S. Adults. Nutrients 2020, 12, 2104. https://doi.org/10.3390/nu12072104
Tarleton EK, Kennedy AG, Rose GL, Littenberg B. Relationship between Magnesium Intake and Chronic Pain in U.S. Adults. Nutrients. 2020; 12(7):2104. https://doi.org/10.3390/nu12072104
Chicago/Turabian StyleTarleton, Emily K., Amanda G. Kennedy, Gail L. Rose, and Benjamin Littenberg. 2020. "Relationship between Magnesium Intake and Chronic Pain in U.S. Adults" Nutrients 12, no. 7: 2104. https://doi.org/10.3390/nu12072104
APA StyleTarleton, E. K., Kennedy, A. G., Rose, G. L., & Littenberg, B. (2020). Relationship between Magnesium Intake and Chronic Pain in U.S. Adults. Nutrients, 12(7), 2104. https://doi.org/10.3390/nu12072104