Parent Stress as a Consideration in Childhood Obesity Prevention: Results from the Guelph Family Health Study, a Pilot Randomized Controlled Trial

 , ,
on behalf of the Guelph Family Health Study
, ,
on behalf of the Guelph Family Health Study
Abstract
1. Introduction
2. Materials and Methods
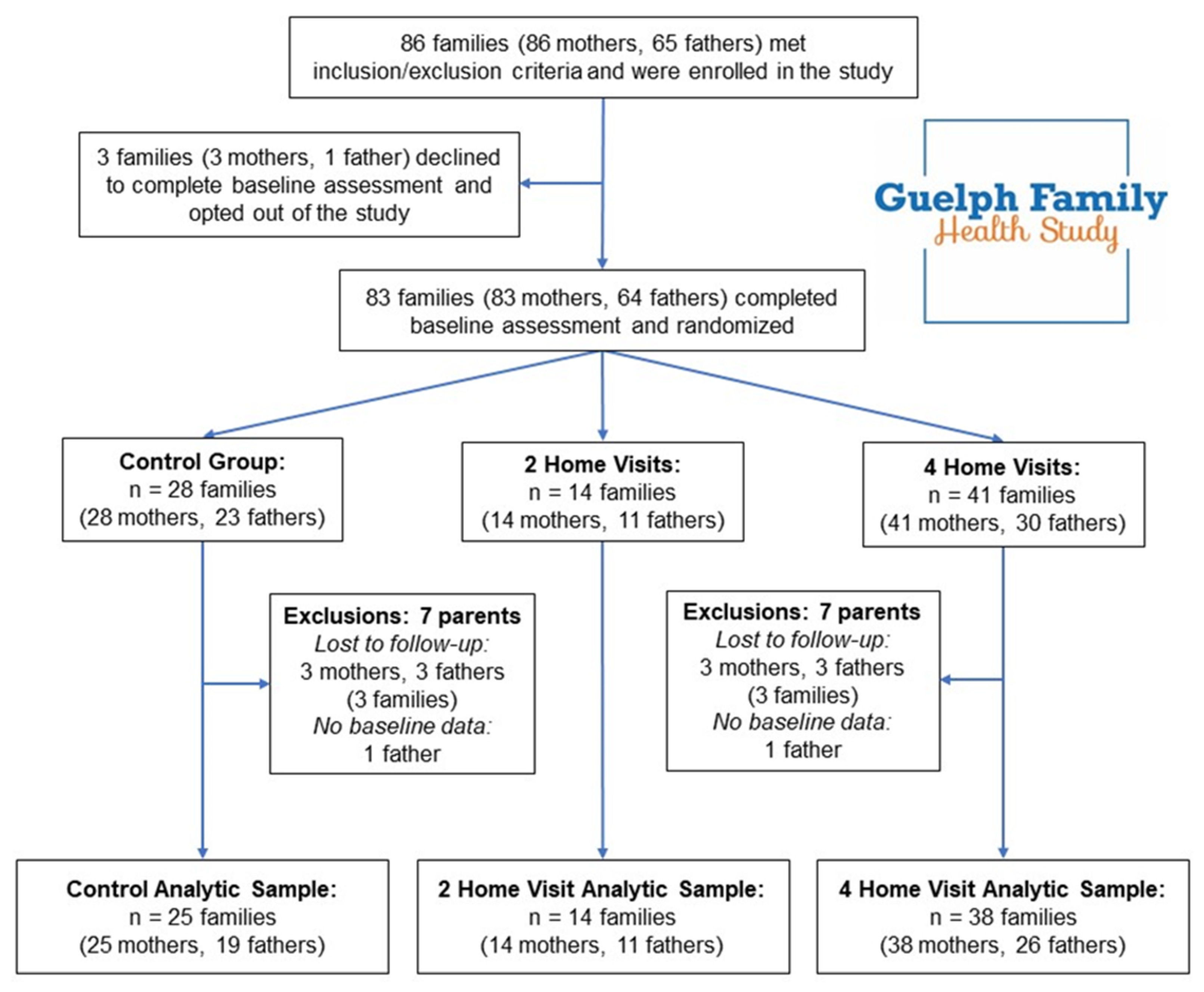
2.1. Study Participants
2.2. Exclusions and Losses to Follow-Up
2.3. GFHS Intervention
2.4. Stress Measures
2.5. Statistical Methods
3. Results
3.1. Descriptive Data
3.2. Mean Stress Levels
3.3. Post-Intervention
3.4. 1-Year Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
| Measure | Intervention Group | Baseline Mean (SD) | Post-Intervention Mean (SD) | Difference from Control 1 B (95% CI) p Value | 1-Year Follow-Up Mean (SD) | Difference from Control 1 β (95% CI) p Value |
|---|---|---|---|---|---|---|
| Analysis of mothers in the 2 home visit (n = 14) and 4 home visit (n = 37) groups compared to the control (n = 25) | ||||||
| General Stress | Control | 6.32 (2.12) | 6.63 (1.69) | −1.07 (−2.27, 0.13) 0.08 | 6.64 (1.92) | −0.34 (−1.68, 1.01) 0.62 |
| 2HV | 5.92 (2.33) | 5.21 (2.01) | 6.29 (2.33) | |||
| 4HV | 6.84 (1.88) | 6.33 (2.08) | −0.42 (−1.35, 0.51) 0.37 | 6.66 (1.71) | −0.08 (−1.13, 0.97) 0.88 | |
| Parenting Distress | Control | 29.68 (6.64) | 28.13 (9.28) | 0.71 (−5.31, 6.72) 0.81 | 30.91 (8.26) | −3.01 (−7.74, 1.73) 0.21 |
| 2HV | 23.07 (5.86) | 26.14 (8.20) | 25.36 (6.06) | |||
| 4HV | 29.92 (10.25) | 27.06 (9.27) | −1.10 (−5.65, 3.45) 0.63 | 29.74 (7.57) | −1.52 (−5.18, 2.14) 0.41 | |
| Depressive Symptoms | Control | 6.80 (4.34) | 6.67 (5.01) | −0.50 (−3.80, 2.79) 0.76 | 6.73 (4.73) | −0.35 (−1.67, 0.97) 0.60 |
| 2HV | 4.71 (4.38) | 5.43 (4.57) | 4.57 (2.53) | |||
| 4HV | 7.58 (5.58) | 6.19 (5.51) | −0.60 (−3.19, 2.00) 0.65 | 6.57 (4.97) | 0.06 (−1.00, 1.12) 0.91 | |
| Analysis of fathers in the 2 home visit (n = 11) and 4 home visit (n = 26) groups compared to the control (n = 19) | ||||||
| General Stress | Control | 6.26 (2.10) | 5.88 (2.20) | 0.32 (−1.01, 1.66) 0.63 | 6.57 (2.06) | −0.57 (−2.13, 0.99) 0.46 |
| 2HV | 6.82 (1.78) | 6.60 (1.58) | 6.33 (2.29) | |||
| 4HV | 6.77 (1.69) | 6.77 (1.69) | 0.66 (−0.41, 1.74) 0.22 | 5.90 (2.11) | −1.05 (−2.31, 0.22) 0.10 | |
| Parenting Distress | Control | 27.53 (5.50) | 28.65 (5.72) | −1.62 (−6.07, 2.83) 0.47 | 27.57 (4.38) | −1.24 (−6.77, 4.29) 0.65 |
| 2HV | 28.27 (9.33) | 27.10 (4.89) | 27.33 (6.36) | |||
| 4HV | 29.35 (7.59) | 28.14 (8.07) | −1.12 (−4.74, 2.49) 0.54 | 28.33 (8.89) | −0.06 (−4.52, 4.41) 0.98 | |
| Depressive Symptoms | Control | 7.63 (3.39) | 7.06 (4.38) | −0.78 (−4.26, 2.71) 0.66 | 7.86 (3.23) | −0.10 (−1.97, 1.78) 0.92 |
| 2HV | 5.82 (3.52) | 5.70 (3.89) | 4.00 (2.35) | |||
| 4HV | 7.77 (5.80) | 6.32 (5.01) | −0.97 (−3.78, 1.84) 0.49 | 7.67 (4.53) | −0.61 (−2.11, 0.89) 0.42 | |
| Analysis of families in the 2 home visit (n = 14) and 4 home visit (n = 36) groups compared to control (n = 24) | ||||||
| Household Chaos | Control | 31.04 (6.31) | 31.74 (6.45) | −0.43 (−3.66, 2.81) 0.79 | 33.00 (6.20) | −3.42 (−7.16, 0.32) 0.07 |
| 2HV | 30.50 (8.48) | 31.00 (8.17) | 29.54 (8.08) | |||
| 4HV | 31.22 (8.47) | 30.89 (8.14) | −0.74 (−3.33, 1.86) 0.57 | 30.57 (7.92) | −2.22 (−5.19, 0.73) 0.14 | |
References
- Pont, S.J.; Puhl, R.; Cook, S.R.; Slusser, W. Stigma Experienced by Children and Adolescents with Obesity. Pediatrics 2017, 140, e20173034. [Google Scholar] [CrossRef] [PubMed]
- Tsiros, M.D.; Olds, T.; Buckley, J.D.; Grimshaw, P.; Brennan, L.; Walkley, J.; Hills, A.P.; Howe, P.R.C.; Coates, A.M. Health-related quality of life in obese children and adolescents. Int. J. Obes. 2009, 33, 387–400. [Google Scholar] [CrossRef] [PubMed]
- Lobstein, T.; Baur, L.; Uauy, R. Obesity in children and young people: A crisis in public health. Obes. Rev. 2004, 5, 4–85. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation Prioritizing Areas for Action in the Field of Population-Based Prevention of Childhood Obesity: Report of a WHO Forum and Technical Meeting; WHO: Geneva, Switzerland, 2009.
- Singer, M.R.; Moore, L.L.; Garrahie, E.J.; Ellison, R.C. The tracking of nutrient intake in young children: The Framingham Children’s Study. Am. J. Public Health 1995, 85, 1673–1677. [Google Scholar] [CrossRef]
- Moore, L.L.; Nguyen, U.S.D.T.; Rothman, K.J.; Cupples, L.A.; Ellison, R.C. Preschool physical activity level and change in body fatness in young children: The Framingham Children’s Study. Am. J. Epidemiol. 1995, 142, 982–988. [Google Scholar] [CrossRef]
- Wang, Y.; Cai, L.; Wu, Y.; Wilson, R.F.; Weston, C.; Fawole, O.; Bleich, S.N.; Cheskin, L.J.; Showell, N.N.; Lau, B.D.; et al. What childhood obesity prevention programmes work? A systematic review and meta-analysis. Obes. Rev. 2015, 16, 547–565. [Google Scholar] [CrossRef]
- Hendrie, G.A.; Brindal, E.; Corsini, N.; Gardner, C.; Baird, D.; Golley, R.K. Combined Home and School Obesity Prevention Interventions for Children. Health Educ. Behav. 2012, 39, 159–171. [Google Scholar] [CrossRef]
- Lindsay, A.C.; Sussner, K.M.; Kim, J.; Gortmaker, S.L. The role of parents in preventing childhood obesity. Future Child. 2006, 16, 169–186. [Google Scholar] [CrossRef] [PubMed]
- Favaro, A.; Santonastaso, P. Effects of parents’ psychological characteristics and eating behaviour on childhood obesity and dietary compliance. J. Psychosom. Res. 1995, 39, 145–151. [Google Scholar] [CrossRef]
- Walton, K.; Simpson, J.R.; Darlington, G.; Haines, J. Parenting stress: A cross-sectional analysis of associations with childhood obesity, physical activity, and TV viewing. BMC Pediatrics 2014, 14, 244. [Google Scholar] [CrossRef] [PubMed]
- Parks, E.P.; Kumanyika, S.; Moore, R.H.; Stettler, N.; Wrotniak, B.H.; Kazak, A. Influence of stress in parents on child obesity and related behaviors. Pediatrics 2012, 130, e1096–e1104. [Google Scholar] [CrossRef] [PubMed]
- Halliday, J.A.; Palma, C.L.; Mellor, D.; Green, J.; Renzaho, A.M.N. The relationship between family functioning and child and adolescent overweight and obesity: A systematic review. Int. J. Obes. 2014, 38, 480–493. [Google Scholar] [CrossRef]
- Bates, C.R.; Buscemi, J.; Nicholson, L.M.; Cory, M.; Jagpal, A.; Bohnert, A.M. Links between the organization of the family home environment and child obesity: A systematic review. Obes. Rev. 2018, 19, 716–727. [Google Scholar] [CrossRef] [PubMed]
- Tate, E.B.; Wood, W.; Liao, Y.; Dunton, G.F. Do stressed mothers have heavier children? A meta-analysis on the relationship between maternal stress and child body mass index. Obes. Rev. 2015, 16, 351–361. [Google Scholar] [CrossRef]
- Fiese, B.H.; Hooker, K.A.; Kotary, L.; Schwagler, J.; Rimmer, M. Family Stories in the Early Stages of Parenthood. J. Marriage Fam. 1995, 57, 763–770. [Google Scholar] [CrossRef]
- Fiese, B.H.; Tomcho, T.J.; Douglas, M.; Josephs, K.; Poltrock, S.; Baker, T. A review of 50 years of research on naturally occurring family routines and rituals: Cause for celebration? J. Fam. Psychol. 2002, 16, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Markson, S.; Fiese, B.H. Family Rituals as a Protective Factor for Children with Asthma. J. Pediatrics Psychol. 2000, 25, 471–480. [Google Scholar] [CrossRef]
- Everhart, R.S.; Fiese, B.H.; Reis, H.; Sprecher, S.; Everhart, R.S.; Fiese, B.H. Family Routines and Rituals. Encycl. Hum. Relatsh. 2013, 20, 284–299. [Google Scholar]
- Beagan, B.; Chapman, G.E.; D’Sylva, A.; Bassett, B.R. “It’s just easier for me to do it”: Rationalizing the family division of foodwork. Sociology 2008, 42, 653–671. [Google Scholar] [CrossRef]
- Ristovski-Slijepcevic, S.; Chapman, G.E.; Beagan, B.L. Being a ‘Good Mother’: Dietary governmentality in the family food practices of three ethnocultural groups in Canada. J. Soc. Study Health Illn. Med. 2010, 14, 467–483. [Google Scholar] [CrossRef]
- Ayanian, J.Z.; Block, J.P.; He, Y.; Zaslavsky, A.M.; Ding, L. Psychosocial stress and change in weight among US adults. Am. J. Epidemiol. 2009, 170, 181–192. [Google Scholar]
- Lee, M.R.; Cacic, K.; Demers, C.H.; Haroon, M.; Heishman, S.; Hommer, D.W.; Epstein, D.H.; Ross, T.J.; Stein, E.A.; Heilig, M.; et al. Gender differences in neural–behavioral response to self-observation during a novel fMRI social stress task. Neuropsychologia 2014, 53, 257–263. [Google Scholar] [CrossRef]
- Meshefedjian, G.A.; Fournier, M.; Blanchard, D.; Frigault, L.-R.R. Gender-specific correlates of perceived life stress: A population-based study, Montreal, Canada, 2012. Can. J. Public Health 2019, 110, 563–574. [Google Scholar] [CrossRef] [PubMed]
- Shivpuri, S.; Gallo, L.C.; Crouse, J.R.; Allison, M.A. The association between chronic stress type and C-reactive protein in the multi-ethnic study of atherosclerosis: Does gender make a difference? J. Behav. Med. 2012, 35, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Steptoe, A.; Hamer, M.; Chida, Y. The effects of acute psychological stress on circulating inflammatory factors in humans: A review and meta-analysis. Brain Behav. Immun. 2007, 21, 901–912. [Google Scholar] [CrossRef]
- Haines, J.; Douglas, S.; Mirotta, J.A.; O’Kane, C.; Breau, R.; Walton, K.; Krystia, O.; Chamoun, E.; Annis, A.; Darlington, G.A.; et al. Guelph Family Health Study: Pilot study of a home-based obesity prevention intervention. Can. J. Public Health 2018, 109, 549–560. [Google Scholar] [CrossRef]
- Ackerman, N.W. The Psychodynamics of Family Life; Basic Books: New York, NY, USA, 1958. [Google Scholar]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- Abidin, R.R. Parenting Stress Index Professional Manual; Par Inc.: Lutz, FL, USA, 2012. [Google Scholar]
- McKelvey, L.M.; Whiteside-Mansell, L.; Faldowski, R.A.; Shears, J.; Ayoub, C.; Hart, A.D. Validity of the Short Form of the Parenting Stress Index for Fathers of Toddlers. J. Child Fam. Stud. 2009, 18, 102–111. [Google Scholar] [CrossRef]
- Andresen, E.M.; Byers, K.; Friary, J.; Kosloski, K.; Montgomery, R. Performance of the 10-item Center for Epidemiologic Studies Depression scale for caregiving research. SAGE Open Med. 2013, 1, 205031211351457. [Google Scholar] [CrossRef] [PubMed]
- Matheny, A.P.; Wachs, T.D.; Ludwig, J.L.; Phillips, K. Bringing order out of chaos: Psychometric characteristics of the confusion, hubbub, and order scale. J. Appl. Dev. Psychol. 1995, 16, 429–444. [Google Scholar] [CrossRef]
- Davison, K.K.; Kitos, N.; Aftosmes-Tobio, A.; Ash, T.; Agaronov, A.; Sepulveda, M.; Haines, J. The forgotten parent: Fathers’ representation in family interventions to prevent childhood obesity. Prev. Med. (Baltimore) 2018, 111, 170–176. [Google Scholar] [CrossRef]
- SAS Institute Inc. SAS/IML® 14.1 User’s Guide; SAS Institute Inc.: Cary, NC, USA, 2015. [Google Scholar]
- Mirotta, J.A.; Darlington, G.A.; Buchholz, A.C.; Haines, J.; Ma, D.W.L.; Duncan, A.M. Guelph Family Health Study’s Home-Based Obesity Prevention Intervention Increases Fibre and Fruit Intake in Preschool-Aged Children. Can. J. Diet. Pract. Res. 2018, 79, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Krystia, O.; Ambrose, T.; Darlington, G.; Ma, D.W.L.; Buchholz, A.C.; Haines, J. A randomized home-based childhood obesity prevention pilot intervention has favourable effects on parental body composition: Preliminary evidence from the Guelph Family Health Study. BMC Obes. 2019, 6, 10. [Google Scholar] [CrossRef] [PubMed]
- O’Kane, C.; Irwin, J.D.; Morrow, D.; Tang, L.; Wong, S.; Buchholz, A.C.; Ma, D.W.L.; Haines, J. Motivational interviewing with families in the home environment. Patient Educ. Couns. 2019, 102, 2073–2080. [Google Scholar] [CrossRef] [PubMed]
- Rao, P.A.; Beidel, D.C. The Impact of Children with High-Functioning Autism on Parental Stress, Sibling Adjustment, and Family Functioning. Behav. Modif. 2009, 33, 437–451. [Google Scholar] [CrossRef]
- Hayes, S.A.; Watson, S.L. The Impact of Parenting Stress: A Meta-analysis of Studies Comparing the Experience of Parenting Stress in Parents of Children With and Without Autism Spectrum Disorder. J. Autism Dev. Disord. 2013, 43, 629–642. [Google Scholar] [CrossRef]
- Barroso, N.E.; Mendez, L.; Graziano, P.A.; Bagner, D.M. Parenting Stress through the Lens of Different Clinical Groups: A Systematic Review & Meta-Analysis. J. Abnorm. Child Psychol. 2018, 46, 449–461. [Google Scholar]
- Levine, A.; Zagoory-Sharon, O.; Feldman, R.; Lewis, J.G.; Weller, A. Measuring cortisol in human psychobiological studies. Physiol. Behav. 2007, 90, 43–53. [Google Scholar] [CrossRef]
- Besemer, K.L.; Dennison, S.M. Family Imprisonment, Maternal Parenting Stress and Its Impact on Mother-Child Relationship Satisfaction. J. Child Fam. Stud. 2018, 27, 3897–3908. [Google Scholar] [CrossRef]
- Malia, J.A. A reader’s guide to family stress literature. J. Loss Trauma 2007, 12, 223–243. [Google Scholar] [CrossRef]
- Dekel, R.; Goldblatt, H.; Keidar, M.; Solomon, Z.; Polliack, M. Being a Wife of a Veteran with Posttraumatic Stress Disorder. Fam. Relat. 2005, 54, 24–36. [Google Scholar] [CrossRef]
- Schwichtenberg, A.; Poehlmann, J. Applied behaviour analysis: Does intervention intensity relate to family stressors and maternal well-being? J. Intellect. Disabil. Res. 2007, 51, 598–605. [Google Scholar] [CrossRef]
- Rickards, A.L.; Walstab, J.E.; Wright-Rossi, R.A.; Simpson, J.; Reddihough, D.S. One-year follow-up of the outcome of a randomized controlled trial of a home-based intervention programme for children with autism and developmental delay and their families. Child Care Health Dev. 2009, 35, 593–602. [Google Scholar] [CrossRef]
- Toth, S.L.; Sturge-Apple, M.L.; Rogosch, F.A.; Cicchetti, D. Mechanisms of change: Testing how preventative interventions impact psychological and physiological stress functioning in mothers in neglectful families. Dev. Psychopathol. 2015, 27, 1661–1674. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lester, P.; Liang, L.-J.; Milburn, N.; Mogil, C.; Woodward, K.; Nash, W.; Aralis, H.; Sinclair, M.; Semaan, A.; Klosinski, L.; et al. Evaluation of a Family-Centered Preventive Intervention for Military Families: Parent and Child Longitudinal Outcomes. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Harkness, S.; Super, C. Culture and Parenting. In Handbook of Parenting; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1995; Volume 2, pp. 253–280. [Google Scholar]
- Hoff, E.; Laursen, B.; Tardiff, T. Socioeconomic Status and Parenting. In Handbook of Parenting; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1995; pp. 231–252. [Google Scholar]
- Nomaguchi, K.; House, A.N. Racial-Ethnic Disparities in Maternal Parenting Stress. J. Health Soc. Behav. 2013, 54, 386–404. [Google Scholar] [CrossRef] [PubMed]

| Characteristic (Individual) | Overall n = 133 Parents | Control n = 44 Parents | Intervention n = 89 Parents |
| Baseline age (years), mean (SD) | 35.5 (4.6) | 34.8 (4.8) | 35.9 (4.6) |
| Relation to child, n (%) | |||
| Father | 56 (42.1%) | 19 (43.2%) | 37 (41.6%) |
| Mother | 77 (57.9%) | 25 (56.8%) | 52 (58.4%) |
| Ethnicity, n (%) | |||
| White | 109 (82.0%) | 37 (84.1%) | 72 (80.9%) |
| Other (e.g., Chinese, Latin American, South Asian, West Asian) | 22 (16.5%) | 5 (11.4%) | 16 (18.9%) |
| Not reported | 2 (1.5%) | 2 (4.5%) | 0 (0.0%) |
| Education, n (%) | |||
| College diploma or less | 30 (22.6%) | 7 (15.9%) | 23 (25.8%) |
| Some university or degree | 35 (33.8%) | 14 (38.1%) | 31 (34.8%) |
| Postgraduate training | 56 (42.1%) | 21 (47.7%) | 35 (39.3%) |
| Did not disclose | 2 (1.5%) | 2 (4.5%) | 0 (0.0%) |
| Characteristic (Family Level) | n = 77 families | n = 25 families | n = 52 families |
| Marital status, n (%) | |||
| Married | 66 (85.7%) | 22 (88.0%) | 44 (84.6%) |
| Other (i.e., living with partner, divorced) | 11 (14.3%) | 3 (12.0%) | 8 (15.4%) |
| Annual household income, n (%) | |||
| < $60,000 | 16 (20.8%) | 5 (20.0%) | 11 (21.2%) |
| $60,000 to $99,999 | 24 (31.2%) | 5 (20.0%) | 19 (36.5%) |
| $100,000+ | 34 (44.2%) | 14 (56.0%) | 20 (38.5%) |
| Not reported | 3 (3.9%) | 1 (4.0%) | 2 (3.8%) |
| Number of children, n (%) | |||
| 1 | 17 (22.1%) | 7 (28.0%) | 10 (19.2%) |
| 2 | 45 (58.4%) | 15 (60.0%) | 30 (57.7%) |
| 3 or more | 15 (19.5%) | 3 (12.0%) | 12 (23.1%) |
| Measure | Intervention Group | Baseline Mean (SD) | Post-Intervention Mean (SD) | Difference from Control 1 β (95% CI) p value | 1-Year Follow-Up Mean (SD) | Difference from Control 1 β (95% CI) p Value |
|---|---|---|---|---|---|---|
| Analysis of mothers in the home visit groups (n = 52) compared to the control group (n = 25) | ||||||
| General Stress | Intervention | 6.60 (2.02) | 6.02 (2.10) | −0.60 (−1.47, 0.27) 0.18 | 6.55 (1.89) | −0.15 (−1.13, 0.83) 0.76 |
| Control | 6.32 (2.12) | 6.63 (1.69) | 6.63 (1.92) | |||
| Parenting Distress | Intervention | 28.04 (9.70) | 26.80 (8.91) | −0.62 (−4.90, 3.65) 0.77 | 28.49 (8.91) | −1.92 (−5.37, 1.53) 0.27 |
| Control | 29.68 (6.64) | 28.13 (9.28) | 30.91 (8.26) | |||
| Depressive Symptoms | Intervention | 6.78 (5.39) | 5.98 (5.23) | −0.57 (−2.98, 1.84) 0.64 | 6.00 (4.48) | −0.92 (−2.87, 1.04) 0.35 |
| Control | 6.80 (4.34) | 6.67 (5.01) | 6.73 (4.73) | |||
| Analysis of fathers in the home visit groups (n = 37) compared to the control group (n = 19) | ||||||
| General Stress | Intervention | 6.78 (1.86) | 6.72 (1.63) | 0.56 (−0.43, 1.56) 0.26 | 6.03 (2.14) | −0.90 (−2.08, 0.27) 0.13 |
| Control | 6.26 (2.10) | 5.88 (2.20) | 6.57 (2.06) | |||
| Parenting Distress | Intervention | 29.03 (8.03) | 27.81 (7.16) | −1.28 (−4.60, 2.04) 0.44 | 28.03 (8.12) | −0.41 (−4.56, 3.74) 0.84 |
| Control | 27.53 (5.50) | 28.65 (5.72) | 27.57 (4.38) | |||
| Depressive Symptoms | Intervention | 7.19 (5.25) | 6.13 (4.63) | −0.91 (−3.48, 1.67) 0.48 | 6.57 (4.31) | −0.70 (−2.98, 1.58) 0.54 |
| Control | 7.63 (3.39) | 7.06 (4.38) | 7.86 (3.23) | |||
| Analysis of families in the home visit groups (n = 52) compared to control group (n = 25) | ||||||
| Household Chaos | Intervention | 31.02 (8.39) | 30.92 (8.07) | 0.65 (−3.06, 1.77) 0.60 | 30.29 (7.89) | −2.57 (−5.34, 0.21) 0.07 |
| Control | 31.04 (6.31) | 31.74 (6.45) | 33.00 (6.20) | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hruska, V.; Darlington, G.; Haines, J.; Ma, D.W.L., on behalf of the Guelph Family Health Study. Parent Stress as a Consideration in Childhood Obesity Prevention: Results from the Guelph Family Health Study, a Pilot Randomized Controlled Trial. Nutrients 2020, 12, 1835. https://doi.org/10.3390/nu12061835
Hruska V, Darlington G, Haines J, Ma DWL on behalf of the Guelph Family Health Study. Parent Stress as a Consideration in Childhood Obesity Prevention: Results from the Guelph Family Health Study, a Pilot Randomized Controlled Trial. Nutrients. 2020; 12(6):1835. https://doi.org/10.3390/nu12061835
Chicago/Turabian StyleHruska, Valerie, Gerarda Darlington, Jess Haines, and David W. L. Ma on behalf of the Guelph Family Health Study. 2020. "Parent Stress as a Consideration in Childhood Obesity Prevention: Results from the Guelph Family Health Study, a Pilot Randomized Controlled Trial" Nutrients 12, no. 6: 1835. https://doi.org/10.3390/nu12061835
APA StyleHruska, V., Darlington, G., Haines, J., & Ma, D. W. L., on behalf of the Guelph Family Health Study. (2020). Parent Stress as a Consideration in Childhood Obesity Prevention: Results from the Guelph Family Health Study, a Pilot Randomized Controlled Trial. Nutrients, 12(6), 1835. https://doi.org/10.3390/nu12061835