Consumption of Goat Cheese Naturally Rich in Omega-3 and Conjugated Linoleic Acid Improves the Cardiovascular and Inflammatory Biomarkers of Overweight and Obese Subjects: A Randomized Controlled Trial

 , , ,
, , ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Design
2.3. Dietetic, Physical Activity and Comorbidities’ Data
2.4. Anthropometric Variables
2.5. Blood Collection
2.6. Compliance and Adverse Events
2.7. Statistical Analysis
3. Results
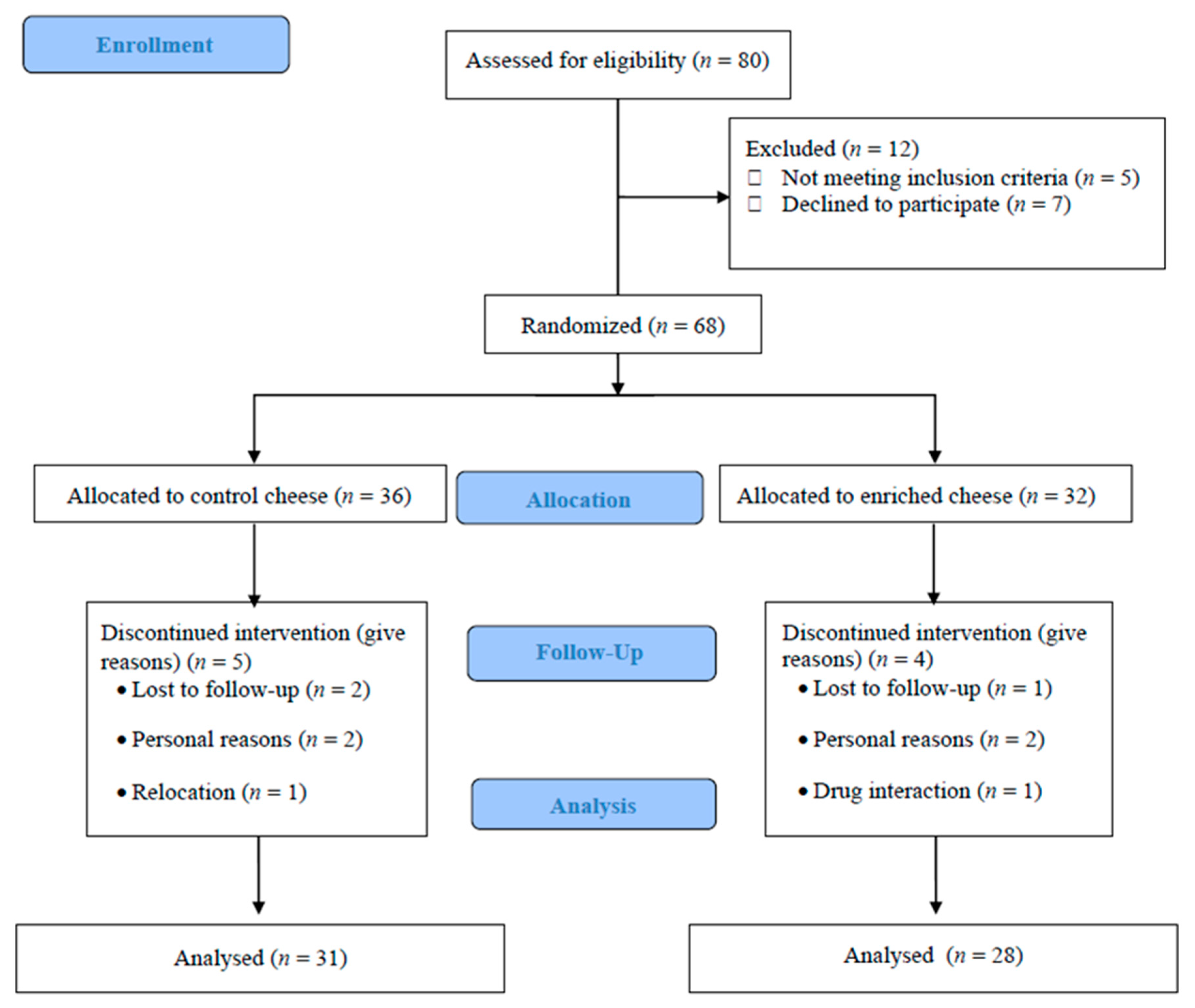
3.1. Recruitment and Study Population
3.2. Baseline Characteristics
3.3. Dietetic and Anthropometric Variables
3.4. Blood Pressure and Biochemical Variables
3.5. Inflammation Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Di Nicolantonio, J.; Lucan, S.C. The evidence of saturated fat and for sugar related to coronary heart disease. Prog. Cardiovasc. Dis. 2016, 58, 464–472. [Google Scholar] [CrossRef] [PubMed]
- De Goede, J.; Geleijnse, J.; Ding, E.; Soedamah-Muthu, S. Effect of cheese consumption on blood lipids: A systematic review and meta-analysis of randomized controlled trials. Nutr. Rev. 2015, 73, 259–275. [Google Scholar] [CrossRef] [PubMed]
- Dias, C.; Wood, L.; Garg, M. Effects of dietary saturated and n-6 polyunsaturated fatty acids on the incorporation of long-chain n-3 polyunsaturated fatty acids into blood lipids. Eur. J. Clin. Nutr. 2016, 70, 812–818. [Google Scholar] [CrossRef] [PubMed]
- Klok, M.; Jakobsdottir, S.; Drent, M. The role of leptin and ghrelin in the regulation of food intake and body weight in humans: A review. Obes. Rev. 2007, 8, 21–34. [Google Scholar] [CrossRef]
- Joseph, S.; Jacques, H.; Plourde, M.; Mitchell, P.; McLeod, R.; Jones, P. Conjugated linoleic acid supplementation for 8 weeks does not affect body composition, lipid profile, or safety biomarkers in overweight, hyperlipidemic men. J. Nutr. 2011, 141, 1286–1291. [Google Scholar] [CrossRef]
- Fontecha, J.; Calvo, M.V.; Juarez, M.; Gil, A.; Martínez-Vizcaino, V. Milk and dairy product consumption and cardiovascular diseases: An overview of systematic reviews and meta-analyses. Adv. Nutr. 2019, 10, S164–S189. [Google Scholar] [CrossRef]
- Dawczynski, C.; Massey, K.; Ness, C.; Kiehntopf, M.; Stepanow, S.; Platzer, M.; Grun, M.; Nicolau, A.; Jahreis, G. Randomized placebo-controlled intervention with n-3 LC-PUFA-supplemented yoghurt: Effects on circulating eicosanoids and cardiovascular risk factors. Clin. Nutr. 2013, 32, 686–696. [Google Scholar] [CrossRef]
- De Oliveira Otto, M.; Nettleton, J.; Lemaitre, R.M.; Steffen, L.; Kromhout, D.; Rich, S.; Tsay, M.Y.; Jacobs, D.R.; Mozaffarian, D. Biomarkers of dairy fatty acids and risk of cardiovascular disease in the multi-ethnic study of atherosclerosis. J. Am. Heart Assoc. 2013, 2, e000092. [Google Scholar] [CrossRef]
- Dittrich, M.; Jahreis, G.; Bothor, K.; Drechsel, C.; Kiehntopf, M.; Blüher, M. Benefits of foods supplemented with vegetable oils rich in α-linolenic, stearidonic or docosahexaenoic acid in hypertriglyceridemic subjects: A double-blind, randomized, controlled trail. Eur. J. Nutr. 2014, 54, 881–893. [Google Scholar] [CrossRef]
- Houston, D.; Driver, K.; Bush, A.; Kritchevsky, S. The association between cheese consumption and cardiovascular risk factors among adults. J. Hum. Nutr. Diet. 2008, 21, 129–140. [Google Scholar] [CrossRef]
- World Medical Association (WMA). Declaration of Helsinki. Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Santurino, C.; Calvo, M.; Gómez-Candela, C.; Fontecha, J. Characterization of naturally goat cheese enriched in conjugated linoleic acid and omega-3 fatty acids for human clinical trial in overweight and obese subjects. PharmaNutrition 2017, 5, 8–17. [Google Scholar] [CrossRef]
- Khandelwal, S.; Demonty, I.; Jeemon, P.; Lakshmy, R.; Mukherjee, R.; Gupta, R.; Snehi, U.; Niveditha, D.; Singh, Y.; van der Knaap, H.C.; et al. Independent and interactive effects of plant sterols and fish oil n-3 long-chain polyunsaturated fatty acids on the plasma lipid profile of mildly hyperlipidaemic Indian adults. Br. J. Nutr. 2009, 102, 722. [Google Scholar] [CrossRef] [PubMed]
- Intorre, F.; Foddai, M.; Azzini, E.; Martin, B.; Montel, M.; Catasta, G. Differential effect of cheese fatty acid composition on blood lipid profile and redox status in normolipidemic volunteers: A pilot study. Int. J. Food Sci. Nutr. 2011, 62, 660–669. [Google Scholar] [CrossRef]
- Stone, N.; Robinson, J.; Lichtenstein, A.; Bairey Merz, C.; Blum, C.; Eckel, R. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults. Circulation 2013, 129, S1–S45. [Google Scholar] [CrossRef]
- Kim, B.; Lim, H.; Lee, H.; Lee, H.; Kang, W.; Kim, E. The effects of conjugated linoleic acid (CLA) on metabolic syndrome patients: A systematic review and meta-analysis. J. Funct. Foods 2016, 25, 588–598. [Google Scholar] [CrossRef]
- Klop, B.; Proctor, S.; Mamo, J.; Botham, K.; Castro Cabezas, M. Understanding postprandial inflammation and its relationship to lifestyle behaviour and metabolic diseases. Int. J. Vasc. Med. 2012, 2012, 947417. [Google Scholar] [CrossRef]
- López Gómez, J.; Pérez Castrillón, J.; Romero Bobillo, E.; De Luis Román, D. Efecto del tratamiento dietoterápico de la obesidad sobre el metabolismo óseo. Nutr. Hosp. 2016, 33, 1452–1460. [Google Scholar]
- Marrugat, J.; Solanas, P.; D’Agostino, R.; Sullivan, L.; Ordovas, J.; Cordón, F.; Ramos, R.; Sala, J. Estimación del riesgo coronario en España mediante la ecuación de Framingham calibrada. Revista Esp. Cardiol. 2003, 56, 253–261. [Google Scholar] [CrossRef]
- Navarro-Alarcón, M.; Cabrera-Vique, C.; Ruiz-López, M.; Olalla, M.; Artacho, R.; Giménez, R.; Quintana, V.; Bergillos, T. Levels of Se, Zn, Mg and Ca in commercial goat and cow milk fermented products: Relationship with their chemical composition and probiotic starter culture. Food Chem. 2011, 129, 1126–1131. [Google Scholar] [CrossRef] [PubMed]
- Intorre, F.; Venneria, E.; Finotti, E.; Foddai, M.; Toti, E.; Catasta, G. Fatty acid content of serum lipid fractions and blood lipids in normolipidaemic volunteers fed two types of cheese having different fat compositions: A pilot study. Int. J. Food Sci. Nutr. 2012, 64, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Nestel, P.; Mellett, N.; Pally, S.; Wong, G.; Barlow, C.; Croft, K.; Mori, T.A.; Meikle, P.K. Effects of low-fat or full-fat fermented and non-fermented dairy foods on selected cardiovascular biomarkers in overweight adults. Br. J. Nutr. 2013, 110, 2242–2249. [Google Scholar] [CrossRef] [PubMed]
- Pannu, P.; Calton, E.; Soares, M. Calcium and vitamin d in obesity and related chronic disease. In Advances in Food and Nutrition Research; Academic Press: Cambridge, MA, USA, 2016; pp. 57–100. [Google Scholar]
- Pariza, M. Perspective on the safety and effectiveness of conjugated linoleic acid. Am. J. Clin. Nutr. 2004, 79, 11325–11365. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, R.; Høstmark, A.; Haug, A.; Skeie, S. Effect of a high intake of cheese on cholesterol and metabolic syndrome: Results of a randomized trial. Food Nutr. Res. 2015, 59, 27–51. [Google Scholar] [CrossRef]
- Obregón, O.; Gestne, A.; Lares, M.; Castro, J.; Stulin, I.; Rivas, K. Estatinas y factor de necrosis tumoral alfa. Revista Latinoam. Hipertens. 2010, 5, 6–10. [Google Scholar]
- Piepoli, M.; Hoes, A.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.; Cooney, M.T.; Corrà, U.; Bernard Cosyns, C.; Deaton, C.; et al. European guidelines on cardiovascular disease prevention in clinical practice (version 2016). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef]
- Pranger, I.; Muskiet, F.; Kema, I.; Singh-Povel, C.; Bakker, S.K. Potential biomarkers for fat from dairy and fish and their association with cardiovascular risk factors: Cross-sectional data from the lifelines biobank and cohort study. Nutrients 2019, 11, 1099. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Rubio, M.; Barbany, M.; Moreno, B. Consenso SEEDO 2007 para la evaluación del sobrepeso y la obesidad y el establecimiento de criterios de intervención terapéutica. Med. Clín. 2007, 128, 184–196. [Google Scholar]
- Sánchez, F.; Albo Castaño, M.; Casallo Blanco, S.; Vizuete Calero, A.; Matías Salces, L. Importancia de las apoproteínas A1 y B como marcadores de riesgo cardiovascular. An. Med. Interna 2008, 25, 199–200. [Google Scholar] [CrossRef]
- Shaikh, N.; Yantha, J.; Shaikh, S.; Rowe, W.; Laidlaw, M.; Cockerline, C.; Ali, A.; Holub, B.; Jackowski, G. Efficacy of a unique omega-3 formulation on the correction of nutritional deficiency and its effects on cardiovascular disease risk factors in a randomized controlled VASCAZEN® REVEAL Trial. Mol. Cell. Biochem. 2014, 396, 9–22. [Google Scholar] [CrossRef]
- Stone, N.; Robinson, J.; Lichtenstein, A.; Goff, D.; Lloyd-Jones, D.; Smith, S.; Blum, C.; Schwartz, J.S. Treatment of blood cholesterol to reduce atherosclerotic cardiovascular disease risk in adults: Synopsis of the 2013 americcollege of cardiology/American heart association cholesterol guideline. Ann. Int. Med. 2014, 160, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Aguillón, G.J.; Cruzat, C.A.; Cuenca, M.J.; Cuchacovich, T.M. El polimorfismo genético del factor de necrosis tumoral alfa como factor de riesgo en patología. Revista Méd Chile 2012, 130, 1043–1050. [Google Scholar]
- Warensjo, E.; Jansson, J.; Cederholm, T.; Boman, K.; Eliasson, M.; Hallmans, G.; Johansson, I.; Sjogren, P. Biomarkers of milk fat and the risk of myocardial infarction in men and women: A prospective, matched case-control study. Am. J. Clin. Nut. 2010, 92, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Aymé, S.; Rath, A.; Bellet, B. WHO International Classification of Diseases (ICD) Revision Process: Incorporating rare diseases into the classification scheme: State of art. Orphanet J. Rare Dis. 2018, 5, P1. [Google Scholar]
- Castro, I.; Monteiro, V.; Barroso, L.; Bertolami, M. Effect of eicosapentaenoic/docosahexaenoic fatty acids and soluble fibers on blood lipids of individuals classified into different levels of lipidemia. Nutrition 2007, 23, 127–137. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Week 0 | Week 12 | Week 12–Week 0 | ||||
|---|---|---|---|---|---|---|---|
| CG | EG | CG | EG | CG | EG | p–Value | |
| Age (years) | 47.60 ± 9.40 | 48.50 ± 7.80 | - | - | - | - | - |
| Men (n) | 8 | 6 | - | - | - | - | - |
| Women (n) | 23 | 22 | - | - | - | - | - |
| Weight (kg) | 85.6 ± 11.30 | 86.80 ± 15.80 | 82.18 ± 11.77 | 83.13 ± 15.75 | −3.41 ± 3.13 | −3.66 ± 2.46 | 0.865 |
| BMI (kg/m2) | 31.05 ± 3.30 | 30.74 ± 4.20 | 30.47 ± 3.69 | 30.54 ± 4.09 | −1.12 ± 0.20 | −0.93 ± 0.17 | 0.756 |
| Waist circ. (cm) | 105.0 ± 10.50 | 99.55 ± 10.60 | 96.29 ± 12.79 | 97.03 ± 11.09 | −5.74 ± 6.63 | −5.87 ± 3.18 | 0.889 |
| BMD (g/cm2) | 1.17 ± 0.12 | 1.16 ± 0.13 | 1.17 ± 0.12 | 1.16 ± 0.14 | −0.004 ± 0.01 | −0.002 ± 0.14 | 0.767 |
| Lean mass (%) | 45.23 ± 7.77 | 46.15 ± 9.72 | 44.75 ± 8.00 | 45.72 ± 9.84 | −0.49 ± 1.24 | −0.43 ± 1.21 | 0.723 |
| Android fat (%) | 51.62 ± 7.19 | 50.72 ± 7.14 | 48.83 ± 9.29 | 48.92 ± 7.82 | −2.80 ± 2.99 | −1.80 ± 2.44 | 0.436 |
| Gynoid fat (%) | 47.24 ± 7.53 | 47.22 ± 8.24 | 45.64 ± 8.22 | 45.20 ± 8.14 | −1.60 ± 1.99 | −2.02 ± 1.90 | 0.356 |
| Total fat mass (%) | 46.94 ± 5.87 | 46.27 ± 6.29 | 44.55 ± 6.87 | 43.11 ± 6.67 | −1.79 ± 1.80 | −1.72 ± 1.68 | 0.645 |
| Systolic BP (mm Hg) | 110.3 ± 14.00 | 110.9 ± 13.10 | 110.7 ± 10.09 | 105.64 ± 22.05 | 0.45 ± 9.41 | −5.21 ± 21.35 | 0.123 |
| Diastolic BP (mm Hg) | 77.50 ± 10.70 | 76.50 ± 9.50 | 76.90 ± 8.53 | 75.07 ± 8.38 | −0.61 ± 7.99 | −1.46 ± 7.79 | 0.385 |
| HR (rate per minute) | 75.30 ± 10.50 | 77.70 ± 10.50 | 68.10 ± 11.97 | 75.71 ± 13.70 | −7.23 ± 9.39 | −1.96 ± 10.97 | 0.259 |
| (mg/dL) | CG | EG | Week 12–Week 0 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Week 0 | Week 12 | Week 0 | Week 12 | CG | EG | CI 95% | ||||
| TC | 201.80 ± 40.41 | 197.16 ± 36.95 | 195.39 ± 37.38 | 201.46 ± 38.81 | −2 (−90; 43) | 6.5 (−24; 50) | 10.72 (0.37; 22.74) | # | ||
| HDL-C | 54.97 ± 16.47 | * | 53.97 ± 11.08 | 47.89 ± 8.00 | * | 52.00 ± 9.24 | 2 (−48; 12) | 4.5 (−5; 16) | 5.11 (1.96; 11.46) | # |
| LDL-C | 128.97 ± 31.34 | 125.61 ± 29.29 | 127.32 ± 32.45 | 129.71 ± 31.59 | 3 (−11; 16) | 2.5 (−9; 31) | 1.39 (−2.15; 5.92) | |||
| TAG | 89.00 ± 42.24 | 87.81 ± 47.65 | 100.71 ± 34.33 | 99.50 ± 31.59 | 6 (−65; 75) | 1 (−56; 53) | −0.02 (−12.8; 14.62) | |||
| ApoA1 | 161.32 ± 26.62 | 153.94 ± 20.85 | 150.68 ± 16.30 | 152.14 ± 18.40 | −1 (−28; 9.6) | 0.3 (−9.8; 24) | 2.74 (−0.3; 6.98) | |||
| ApoB | 102.42 ± 21.45 | 101.65 ± 22.06 | 102.86 ± 23.33 | 108.00 ± 26.20 | −2* (−19; 27) | 3.5* (−20; 34) | 5.92 (0.81; 11.77) | |||
| Glucose | 93.06 ± 8.08 | 95.39 ± 8.49 | 90.82 ± 9.40 | 94.54 ± 7.54 | 2.32 (70.04; 94.06) | 3.71 (67.05; 95.04) | 0.05 (–0.1; 0.19) | |||
| Ratio | CG (n = 31) | EG (n = 28) | ||
|---|---|---|---|---|
| Week 0 | Week 12 | Week 0 | Week 12 | |
| TC/HDL-C | 3.67 ± 2.5 | 3.67 ± 3.3 | 4.06 ± 4.6 | 3.87 ± 4.6 |
| LDL-C/HDL-C | 1.71 ± 1.9 | 1.72 ± 2.6 | 1.91 ± 4.0 | 1.79 ± 3.4 * |
| ApoB/ApoA1 | 0.63 ± 0.8 | 0.66 ± 1.1 | 0.68 ± 1.43 | 0.71 ± 1.42 |
| CG | EG | Week 12–Week 0 | CI 95% | ||||
|---|---|---|---|---|---|---|---|
| Week 0 | Week 12 | Week 0 | Week 12 | CG | EG | ||
| CRP (mg/L) | 2.67 ± 4.36 | 2.98 ± 7.62 | 2.95 ± 6.06 | 1.02 ± 6.33 | 0.03 (−18.12; 32.1) | −0.76 (−12.34; 3.38) | –10.72 (0.37; 22.74) # |
| TNF-α (pg/mL) | 3.88 ± 1.45 | 4.47 ± 1.43 | 4.51 ± 1.57 | 4.85 ± 1.71 | 0.5 (−0.8; 18.3) | 0.75 (−1.2; 2.5) | −0.46 (−246; 0.28) |
| IL-6 (pg/mL) | 2.60 ± 2.37 | 3.70 ± 2.25 | 2.70 ± 1.53 | 3.65 ± 1.60 | 1.2 (−1.7; 3.2) | 0.95 (−2; 5.2) | −0.12 (−0.82; 0.6) |
| Fibrinogen (mg/dL) | 397 ± 102.82 | 413 ± 97.33 | 419 ± 124.14 | 346 ± 129.64 | −13 (−333;425) | −17 (−202; 106) | −26.88 (−81.27; 22.96) |
| OxLDL (ng/mL) | 72.71 ± 238.10 | 80.53 ± 245.14 | 135.09 ± 229.32 | 113.47 ± 218.01 | 0.01 (−164.2; 654.9) | −0.31 (−250.9; 90.4) | −13.3 (−87.2; 16.9) |
| FFA (mM) | 0.28 ± 0.17 | 0.25 ± 0.08 | 0.28 ± 0.11 | 0.23 ± 0.10 | −0.01 (−0.47; 0.21) | −0.06 (−0.41; 0.2) | −0.03 (−0.09; 0.04) |
| CG | EG | Week12–Week 0 | CI 95% | ||||
|---|---|---|---|---|---|---|---|
| Week 0 | Week 12 | Week 0 | Week 12 | CG | EG | ||
| Vitamin D (ng/mL) | 14.26 ± 6.15 | 21.89 ± 6.94 | 13.95 ± 6.06 | 22.5 ± 6.33 | 7 (1; 23) | 8 (0; 17) | 0.39 (−2.2; 2.26) |
| Calcium (mg/dL) | 9.16 ± 0.38 | 9.24 ± 0.30 | 9.16 ± 0.32 | 9.30 ± 0.35 | 0.1 (−0.6; 0.7) | 0.15 (−0.3; 0.9) | 0.05 (−0.1; 0.19) |
| Phosphorous (mg/dL) | 3.35 ± 0.39 | 3.41 ± 0.52 | 3.46 ± 0.59 | 3.32 ± 0.47 | 0.1 (−0.8; 0.8) | −0.1 (−1.4; 0.8) | −0.19 (−0.41; 0.02) |
| Ghrelin (pg/mL) | 9.9 ± 13.75 | 10 ± 14.42 | 8.45 ± 19.62 | 8.10 ± 20.69 | 0.6 (−35.7; 40.3) | 0.05 (−41.8; 39.2) | −0.37 (−7.72; 6.78) |
| Leptin (pg/mL) | 14.14 ± 10.74 | 11.01 ± 10.00 | 14.80 ± 10.80 | 11.15 ± 10.50 | −1.8 (−23.03; 13.1) | −2.7 (−9.5; 2.5) | −0.12 (−0.82; 0.6) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santurino, C.; López-Plaza, B.; Fontecha, J.; Calvo, M.V.; Bermejo, L.M.; Gómez-Andrés, D.; Gómez-Candela, C. Consumption of Goat Cheese Naturally Rich in Omega-3 and Conjugated Linoleic Acid Improves the Cardiovascular and Inflammatory Biomarkers of Overweight and Obese Subjects: A Randomized Controlled Trial. Nutrients 2020, 12, 1315. https://doi.org/10.3390/nu12051315
Santurino C, López-Plaza B, Fontecha J, Calvo MV, Bermejo LM, Gómez-Andrés D, Gómez-Candela C. Consumption of Goat Cheese Naturally Rich in Omega-3 and Conjugated Linoleic Acid Improves the Cardiovascular and Inflammatory Biomarkers of Overweight and Obese Subjects: A Randomized Controlled Trial. Nutrients. 2020; 12(5):1315. https://doi.org/10.3390/nu12051315
Chicago/Turabian StyleSanturino, Cristina, Bricia López-Plaza, Javier Fontecha, María V. Calvo, Laura M. Bermejo, David Gómez-Andrés, and Carmen Gómez-Candela. 2020. "Consumption of Goat Cheese Naturally Rich in Omega-3 and Conjugated Linoleic Acid Improves the Cardiovascular and Inflammatory Biomarkers of Overweight and Obese Subjects: A Randomized Controlled Trial" Nutrients 12, no. 5: 1315. https://doi.org/10.3390/nu12051315
APA StyleSanturino, C., López-Plaza, B., Fontecha, J., Calvo, M. V., Bermejo, L. M., Gómez-Andrés, D., & Gómez-Candela, C. (2020). Consumption of Goat Cheese Naturally Rich in Omega-3 and Conjugated Linoleic Acid Improves the Cardiovascular and Inflammatory Biomarkers of Overweight and Obese Subjects: A Randomized Controlled Trial. Nutrients, 12(5), 1315. https://doi.org/10.3390/nu12051315