Association of the SH2B1 rs7359397 Gene Polymorphism with Steatosis Severity in Subjects with Obesity and Non-Alcoholic Fatty Liver Disease

 ,
,  , , , , ,
, , , , ,  ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. General Measurements
2.3. Dietary Assessment
2.4. Hepatic Imaging Tests
2.5. Metabolomics
2.6. Genotyping
2.7. Statistical Analyses
3. Results
3.1. Characteristics of the Participants
3.2. Hepatic Status According to Genetic Variant Alleles
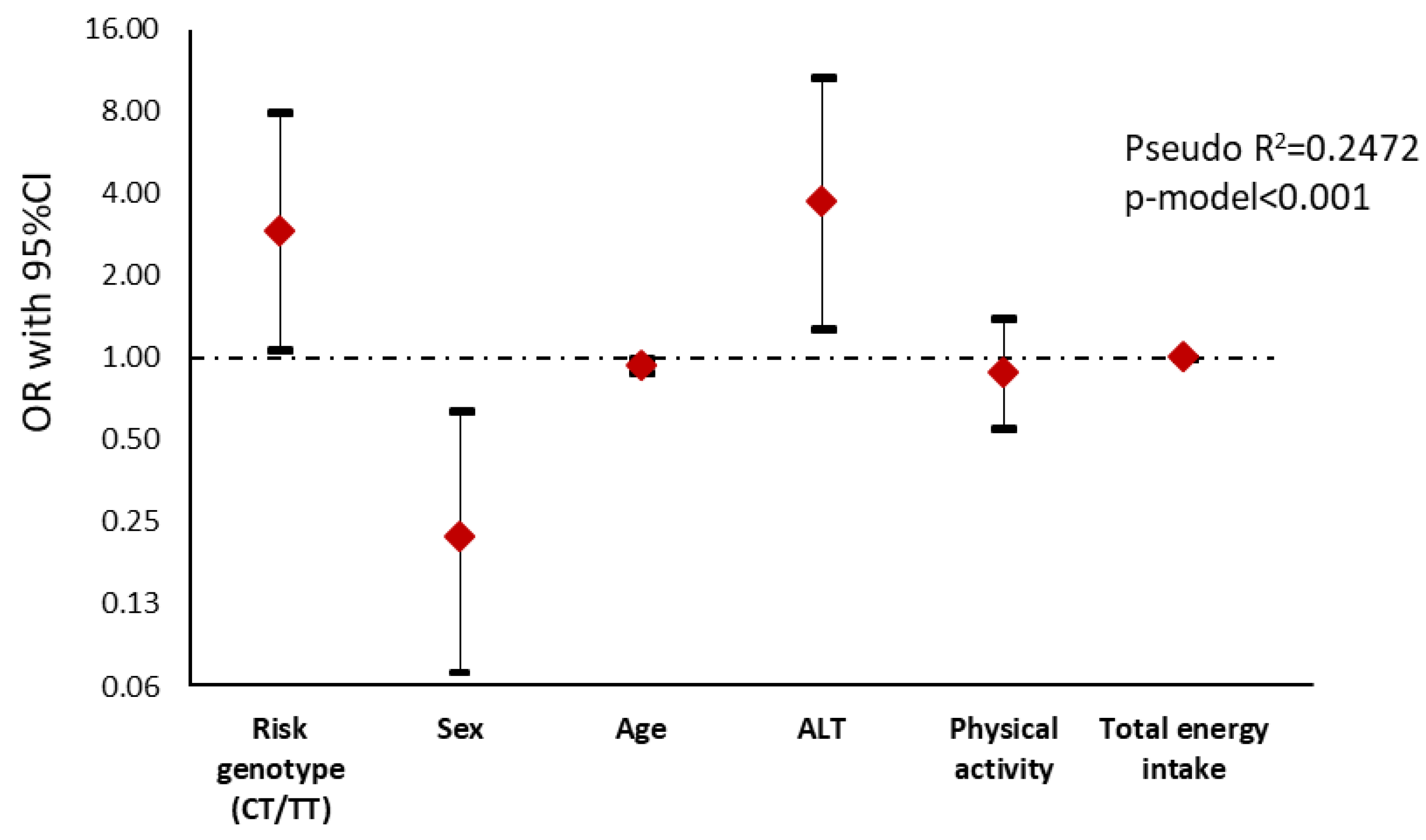
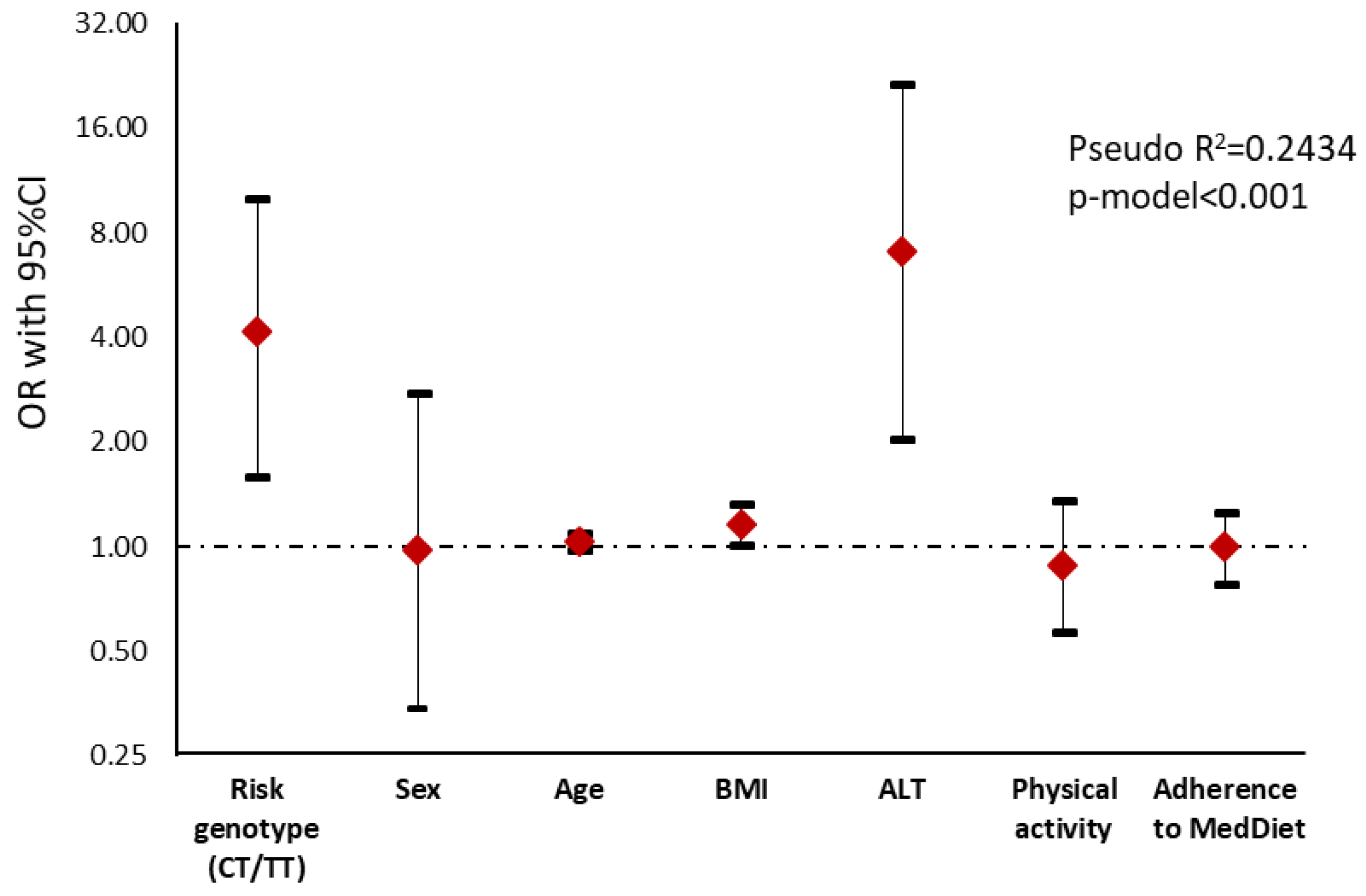
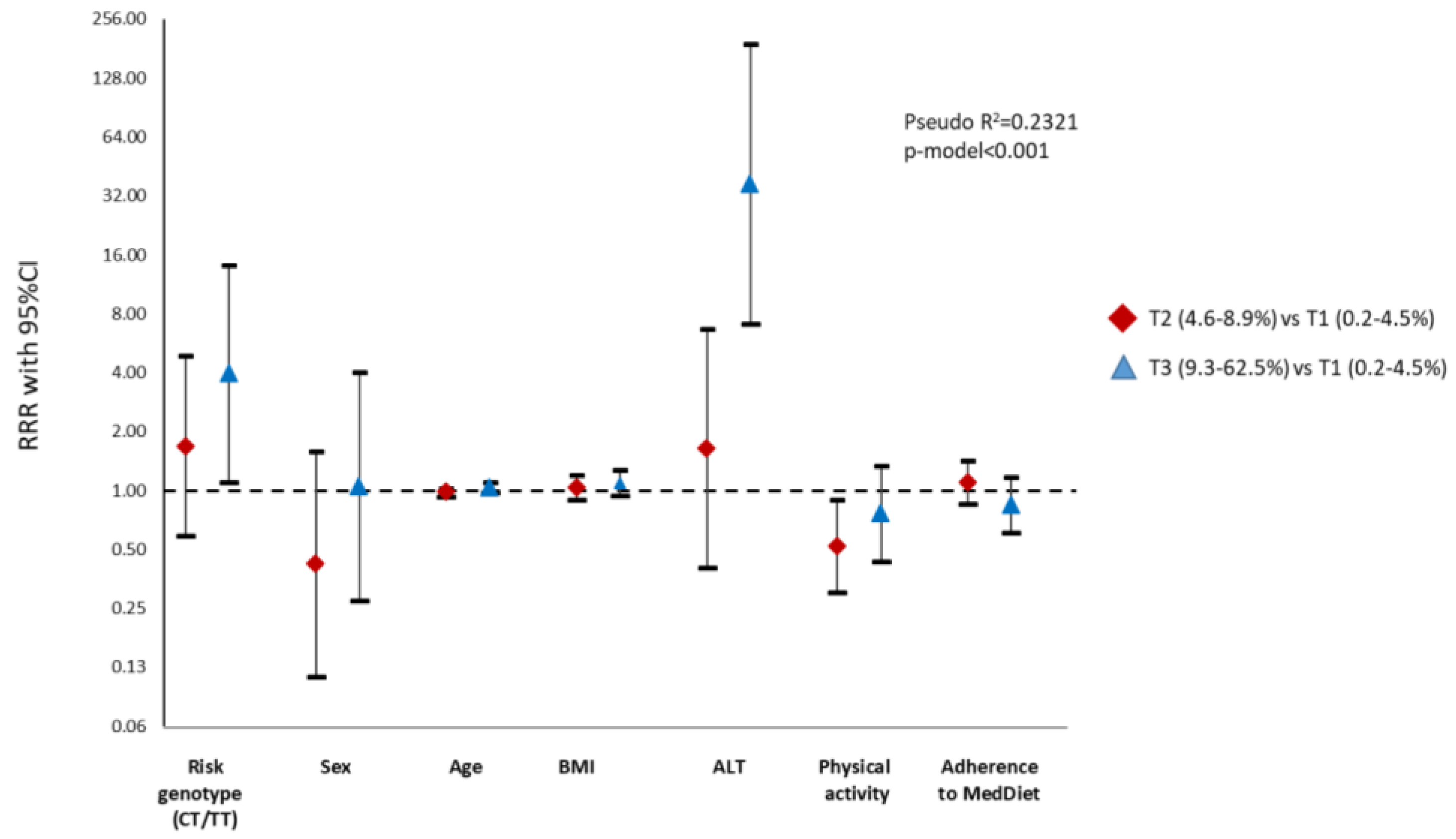
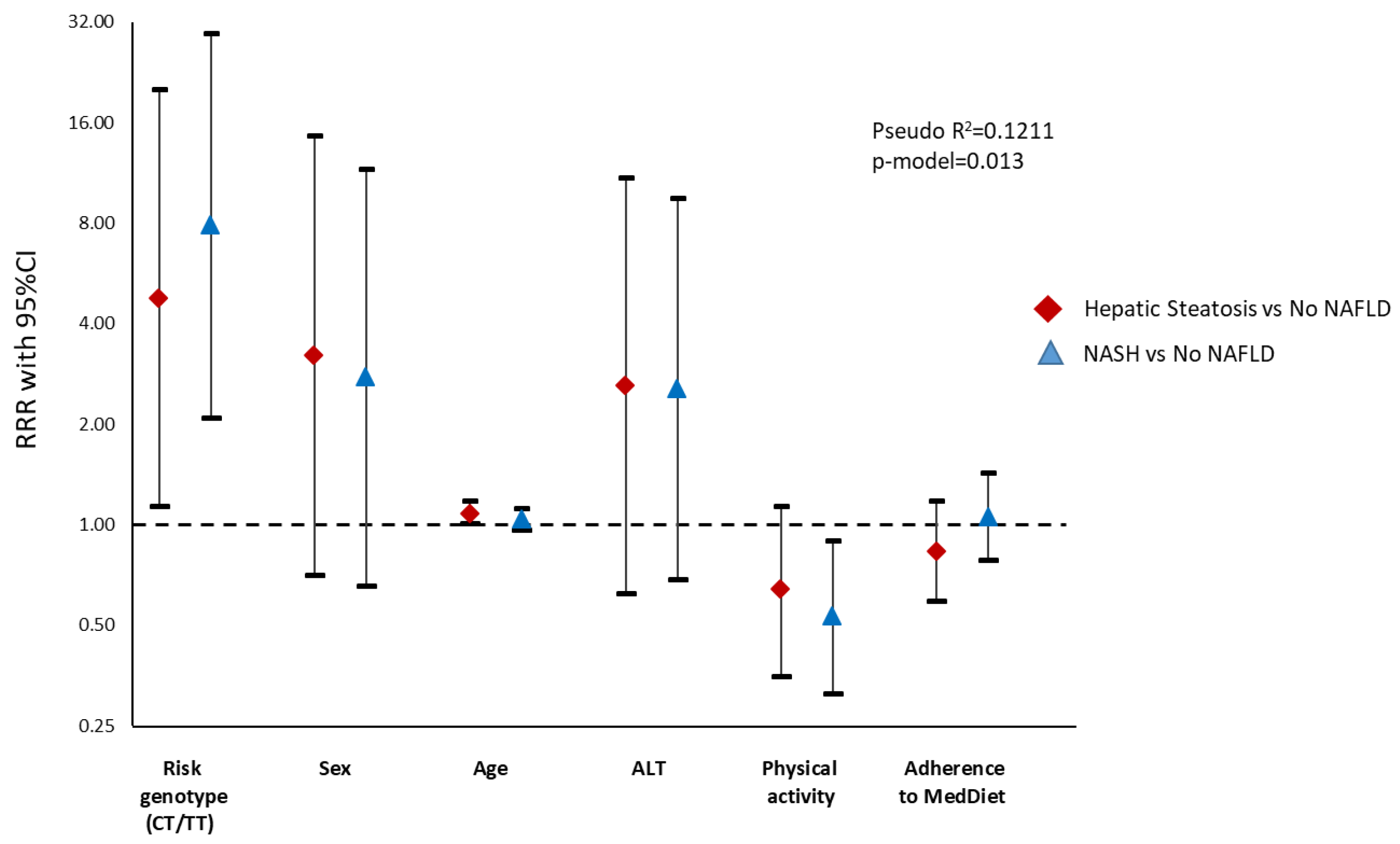
3.3. Association between Genotype and Advanced Stages of the Disease
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Benedict, M.; Zhang, X. Non-alcoholic fatty liver disease: An expanded review. World J. Hepatol. 2017, 9, 715–732. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed]
- Cantero, I.; Abete, I.; Monreal, J.I.; Martinez, J.A.; Zulet, M.A. Fruit fiber consumption specifically improves liver health status in obese subjects under energy restriction. Nutrients 2017, 9, 667. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Zheng, D.; Liu, J.; Fang, L.; Li, Q. Atherogenic index of plasma is a novel predictor of non-alcoholic fatty liver disease in obese participants: A cross-sectional study. Lipids Health Dis. 2018, 17, 284. [Google Scholar] [CrossRef]
- Tanaka, N.; Kimura, T.; Fujimori, N.; Nagaya, T.; Komatsu, M.; Tanaka, E. Current status, problems, and perspectives of non-alcoholic fatty liver disease research. World J. Gastroenterol. 2019, 25, 163–177. [Google Scholar] [CrossRef]
- Araújo, A.R.; Rosso, N.; Bedogni, G.; Tiribelli, C.; Bellentani, S. Global epidemiology of non-alcoholic fatty liver disease/non-alcoholic steatohepatitis: What we need in the future. Liver Int. 2018, 38, 47–51. [Google Scholar] [CrossRef]
- Xie, D.Y.; Fan, H.K.; Ren, Z.G.; Fan, J.; Gao, Q. Identifying Clonal Origin of Multifocal Hepatocellular Carcinoma and Its Clinical Implications. Clin. Transl. Gastroenterol. 2019, 10, e00006. [Google Scholar] [CrossRef]
- Feldman, A.; Eder, S.K.; Felder, T.K.; Kedenko, L.; Paulweber, B.; Stadlmayr, A.; Huber-Schönauer, U.; Niederseer, D.; Stickel, F.; Auer, S.; et al. Clinical and Metabolic Characterization of Lean Caucasian Subjects with Non-alcoholic Fatty Liver. Am. J. Gastroenterol. 2017, 112, 102–110. [Google Scholar] [CrossRef]
- Marin-Alejandre, B.A.; Abete, I.; Cantero, I.; Riezu-Boj, J.I.; Milagro, F.I.; Monreal, J.I.; Elorz, M.; Herrero, J.I.; Benito-Boillos, A.; Quiroga, J.; et al. Association between sleep disturbances and liver status in obese subjects with nonalcoholic fatty liver disease: A comparison with healthy controls. Nutrients 2019, 11, 322. [Google Scholar] [CrossRef]
- Marin-Alejandre, B.A.; Abete, I.; Cantero, I.; Monreal, J.I.; Elorz, M.; Herrero, J.I.; Benito-Boillos, A.; Quiroga, J.; Martinez-Echeverria, A.; Uriz-Otano, J.I.; et al. The Metabolic and Hepatic Impact of Two Personalized Dietary Strategies in Subjects with Obesity and Nonalcoholic Fatty Liver Disease: The Fatty Liver in Obesity (FLiO) Randomized Controlled Trial. Nutrients 2019, 11, 2543. [Google Scholar] [CrossRef]
- Galarregui, C.; Zulet, M.A.; Cantero, I.; Marín-Alejandre, B.A.; Monreal, J.I.; Elorz, M.; Benito-Boillos, A.; Herrero, J.I.; Tur, J.A.; Abete, I.; et al. Interplay of glycemic index, glycemic load, and dietary antioxidant capacity with insulin resistance in subjects with a cardiometabolic risk profile. Int. J. Mol. Sci. 2018, 19, 3662. [Google Scholar] [CrossRef]
- Cantero, I.; Elorz, M.; Abete, I.; Marin, B.A.; Herrero, J.I.; Monreal, J.I.; Benito, A.; Quiroga, J.; Martínez, A.; Huarte, M.P.; et al. Ultrasound/elastography techniques, lipidomic and blood markers compared to magnetic resonance imaging in non-alcoholic fatty liver disease adults. Int. J. Med. Sci. 2019, 16, 75–83. [Google Scholar] [CrossRef]
- Machado, M.V.; Cortez-Pinto, H. Non-alcoholic fatty liver disease: What the clinician needs to know. World J. Gastroenterol. 2014, 20, 12956–12980. [Google Scholar] [CrossRef]
- Recaredo, G.; Marin-Alejandre, B.A.; Cantero, I.; Monreal, J.I.; Herrero, J.I.; Benito-Boillos, A.; Elorz, M.; Tur, J.A.; Martínez, J.A.; Zulet, M.A.; et al. Association between Different Animal Protein Sources and Liver Status in Obese Subjects with Non-Alcoholic Fatty Liver Disease: Fatty Liver in Obesity (FLiO) Study. Nutrients 2019, 11, 2359. [Google Scholar] [CrossRef]
- Haupt, A.; Thamer, C.; Heni, M.; MacHicao, F.; MacHann, J.; Schick, F.; Stefan, N.; Fritsche, A.; Häring, H.U.; Staiger, H. Novel Obesity Risk Loci Do Not Determine Distribution of Body Fat Depots: A Whole- body MRI/MRS study. Obesity 2010, 18, 1212–1217. [Google Scholar] [CrossRef]
- Lin, Y.C.; Chang, P.F.; Chang, M.H.; Ni, Y.H. Genetic determinants of hepatic steatosis and serum cytokeratin-18 fragment levels in Taiwanese children. Liver Int. 2018, 38, 1300–1307. [Google Scholar] [CrossRef]
- Bril, F.; Millán, L.; Kalavalapalli, S.; McPhaul, M.J.; Caulfield, M.P.; Martinez-Arranz, I.; Alonso, C.; Ortiz Betes, P.; Mato, J.M.; Cusi, K. Use of a metabolomic approach to non-invasively diagnose non-alcoholic fatty liver disease in patients with type 2 diabetes mellitus. Diabetes Obes. Metab. 2018, 20, 1702–1709. [Google Scholar] [CrossRef]
- Pelusi, S.; Baselli, G.; Pietrelli, A.; Dongiovanni, P.; Donati, B.; McCain, M.V.; Meroni, M.; Fracanzani, A.L.; Romagnoli, R.; Petta, S.; et al. Rare Pathogenic Variants Predispose to Hepatocellular Carcinoma in Nonalcoholic Fatty Liver Disease. Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef]
- Younes, R.; Bugianesi, E. Should we undertake surveillance for HCC in patients with NAFLD? J. Hepatol. 2018, 68, 326–334. [Google Scholar] [CrossRef]
- de Luis, D.A.; Izaola, O.; Primo, D.; Aller, R. A circadian rhythm-related MTNR1B genetic variant (rs10830963) modulate body weight change and insulin resistance after 9 months of a high protein/low carbohydrate vs a standard hypocaloric diet. J. Diabetes Complicat. 2020, 34, 107534. [Google Scholar] [CrossRef]
- Ramos-Lopez, O.; Riezu-Boj, J.I.; Milagro, F.I.; Cuervo, M.; Goni, L.; Martinez, J.A. Prediction of Blood Lipid Phenotypes Using Obesity-Related Genetic Polymorphisms and Lifestyle Data in Subjects with Excessive Body Weight. Int. J. Genom. 2018, 2018, 4283078. [Google Scholar] [CrossRef]
- Sheng, L.; Liu, Y.; Jiang, L.; Chen, Z.; Zhou, Y.; Cho, K.W.; Rui, L. Hepatic SH2B1 and SH2B2 regulate liver lipid metabolism and VLDL secretion in mice. PLoS ONE 2013, 8, e83269. [Google Scholar] [CrossRef]
- Cheng, Y.; Duan, C.; Zhang, C. New perspective on SH2B1: An accelerator of cancer progression. Biomed. Pharmacother. 2020, 121, 109651. [Google Scholar] [CrossRef]
- Al-Hakeem, M.M. Implication of SH2B1 gene polymorphism studies in gestational diabetes mellitus in Saudi pregnant women. Saudi J. Biol. Sci. 2014, 21, 610–615. [Google Scholar] [CrossRef]
- Lange, L.A.; Graff, M.; Lange, E.M.; Young, K.L.; Richardson, A.S.; Mohlke, K.L.; North, K.E.; Harris, K.M.; Gordon-Larsen, P. Evidence for Association between SH2B1 Gene Variants and Glycated Hemoglobin in Nondiabetic European American Young Adults: The Add Health Study. Ann. Hum. Genet. 2016, 80, 294–305. [Google Scholar] [CrossRef]
- de la Iglesia, R.; Lopez-Legarrea, P.; Abete, I.; Bondia-Pons, I.; Navas-Carretero, S.; Forga, L.; Martinez, J.A.; Zulet, M.A. A new dietary strategy for long-term treatment of the metabolic syndrome is compared with the American Heart Association (AHA) guidelines: The MEtabolic Syndrome REduction in NAvarra (RESMENA) project. Br. J. Nutr. 2014, 111, 643–652. [Google Scholar] [CrossRef]
- Zulet, M.A.; Bondia-Pons, I.; Abete, I.; De La Iglesia, R.; López-Legarrea, P.; Forga, L.; Navas-Carretero, S.; Martinez, J.A. The reduction of the metabolyc syndrome in Navarra-Spain (RESMENA-S) study; A multidisciplinary strategy based on chrononutrition and nutritional education, together with dietetic and psychological control. Nutr. Hosp. 2011, 26, 16–26. [Google Scholar]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef]
- Strauss, S.; Gavish, E.; Gottlieb, P.; Katsnelson, L. Interobserver and intraobserver variability in the sonographic assessment of fatty liver. AJR Am. J. Roentgenol. 2007, 189, W320–W323. [Google Scholar] [CrossRef]
- Lee, S.S.; Park, S.H. Radiologic evaluation of nonalcoholic fatty liver disease. World J Gastroenterol. 2014, 20, 7392–7402. [Google Scholar] [CrossRef]
- Alonso, C.; Fernández-Ramos, D.; Varela-Rey, M.; Martínez-Arranz, I.; Navasa, N.; Van Liempd, S.M.; Lavín Trueba, J.L.; Mayo, R.; Ilisso, C.P.; de Juan, V.G.; et al. Metabolomic Identification of Subtypes of Nonalcoholic Steatohepatitis. Gastroenterology 2017, 152, 1449–1461. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Lopez, O.; Riezu-Boj, J.I.; Milagro, F.I.; Goni, L.; Cuervo, M.; Martinez, J.A. Association of the Gly482Ser PPARGC1A gene variant with different cholesterol outcomes in response to two energy-restricted diets in subjects with excessive weight. Nutrition 2018, 47, 83–89. [Google Scholar] [CrossRef]
- Ramos-Lopez, O.; Riezu-Boj, J.I.; Milagro, F.I.; Goni, L.; Cuervo, M.; Martinez, J.A. Differential lipid metabolism outcomes associated with ADRB2 gene polymorphisms in response to two dietary interventions in overweight/obese subjects. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 165–172. [Google Scholar] [CrossRef]
- Younes, R.; Bugianesi, E. A spotlight on pathogenesis, interactions and novel therapeutic options in NAFLD. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 80–82. [Google Scholar] [CrossRef]
- Del Campo, J.A.; Gallego-Durán, R.; Gallego, P.; Grande, L. Genetic and epigenetic regulation in nonalcoholic fatty liver disease (NAFLD). Int. J. Mol. Sci. 2018, 19, 911. [Google Scholar] [CrossRef] [PubMed]
- Quinlan, A.R.; Hall, I.M. BEDTools: A flexible suite of utilities for comparing genomic features. Bioinformatics 2010, 26, 841–842. [Google Scholar] [CrossRef] [PubMed]
- Tortora, R.; Rispo, A.; Alisi, A.; Imperatore, N.; Crudele, A.; Ferretti, F.; Nobili, V.; Miele, L.; Gerbino, N.; Caporaso, N.; et al. PNPLA3 rs738409 Polymorphism Predicts Development and Severity of Hepatic Steatosis but Not Metabolic Syndrome in Celiac Disease. Nutrients 2018, 10, 1239. [Google Scholar] [CrossRef]
- Volckmar, A.L.; Bolze, F.; Jarick, I.; Knoll, N.; Scherag, A.; Reinehr, T.; Illig, T.; Grallert, H.; Wichmann, H.E.; Wiegand, S.; et al. Mutation screen in the GWAS derived obesity gene SH2B1 including functional analyses of detected variants. BMC Med. Genom. 2012, 5, 1–10. [Google Scholar] [CrossRef]
- Rui, L. SH2B1 regulation of energy balance, body weight, and glucose metabolism. World J. Diabetes. 2014, 5, 511. [Google Scholar] [CrossRef]
- Mansego, M.L.; Milagro, F.I.; Zulet, M.A.; Martinez, J.A. SH2B1 CpG-SNP is associated with body weight reduction in obese subjects following a dietary restriction program. Ann. Nutr. Metab. 2014, 66, 1–9. [Google Scholar] [CrossRef]
- Morris, D.L.; Cho, K.W.; Zhou, Y.; Rui, L. SH2B1 enhances insulin sensitivity by both stimulating the insulin receptor and inhibiting tyrosine dephosphorylation of insulin receptor substrate proteins. Diabetes 2009, 58, 2039–2047. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Zhou, Y.; Carter-Su, C.; Myers, M.G.; Rui, L. SH2B1 Enhances Leptin Signaling by Both Janus Kinase 2 Tyr 813 Phosphorylation-Dependent and -Independent Mechanisms. Mol. Endocrinol. 2007, 21, 2270–2281. [Google Scholar] [CrossRef] [PubMed]
- Rider, L.; Diakonova, M. Adapter Protein SH2B1β Binds Filamin A to Regulate Prolactin-Dependent Cytoskeletal Reorganization and Cell Motility. Mol. Endocrinol. 2011, 25, 1231–1243. [Google Scholar] [CrossRef] [PubMed]
- Abdollahi, H.; Azodi, M.Z.; Hatami, B. Protein interaction mapping interpretation of none alcoholic fatty liver disease model of rats after fat diet feeding. Gastroenterol. Hepatol. Bed Bench. 2017, 10, 146–153. [Google Scholar]
- Martinez, J.A.; Navas-Carretero, S.; Saris, W.H.; Astrup, A. Personalized weight loss strategies-the role of macronutrient distribution. Nat. Rev. Endocrinol. 2014, 10, 749–760. [Google Scholar] [CrossRef]
- Abete, I.; Astrup, A.; Martínez, J.A.; Thorsdottir, I.; Zulet, M.A. Obesity and the metabolic syndrome: Role of different dietary macronutrient distribution patterns and specific nutritional components on weight loss and maintenance. Nutr. Rev. 2010, 68, 214–231. [Google Scholar] [CrossRef]
- de Luis, D.A.; Izaola, O.; Primo, D.; Aller, R. Association of the rs10830963 polymorphism in melatonin receptor type 1B (MTNR1B) with metabolic response after weight loss secondary to a hypocaloric diet based in Mediterranean style. Clin. Nutr. 2018, 37, 1563–1568. [Google Scholar] [CrossRef]
- de Luis, D.A.; Izaola, O.; Primo, D.; Aller, R.; Ortola, A.; Gómez, E.; Lopez, J.J. The association of SNP276G>T at adiponectin gene with insulin resistance and circulating adiponectin in response to two different hypocaloric diets. Diabetes Res. Clin. Pract. 2018, 137, 93–99. [Google Scholar] [CrossRef]
- Roman, S.; Ojeda-Granados, C.; Ramos-Lopez, O.; Panduro, A. Genome-based nutrition: An intervention strategy for the prevention and treatment of obesity and nonalcoholic steatohepatitis. World J. Gastroenterol. 2015, 21, 3449–3461. [Google Scholar] [CrossRef]
- Ramos-Lopez, O.; Riezu-Boj, J.I.; Milagro, F.I.; Cuervo, M.; Goni, L.; Martinez, J.A. Models Integrating Genetic and Lifestyle Interactions on Two Adiposity Phenotypes for Personalized Prescription of Energy-Restricted Diets With Different Macronutrient Distribution. Front. Genet. 2019, 10, 686. [Google Scholar] [CrossRef]
- Ma, J.; Hennein, R.; Liu, C.; Long, M.T.; Hoffmann, U.; Jacques, P.F.; Lichtenstein, A.H.; Hu, F.B.; Levy, D. Improved Diet Quality Associates with Reduction in Liver Fat, Particularly in Individuals with High Genetic Risk Scores for Nonalcoholic Fatty Liver Disease. Gastroenterology 2018, 155, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Nobili, V.; Liccardo, D.; Bedogni, G.; Salvatori, G.; Gnani, D.; Bersani, I.; Alisi, A.; Valenti, L.; Raponi, M. Influence of dietary pattern, physical activity, and I148M PNPLA3 on steatosis severity in at-risk adolescents. Genes Nutr. 2014, 9, 392. [Google Scholar] [CrossRef] [PubMed]
- Jamshidi, Y.; Snieder, H.; Ge, D.; Spector, T.D.; O’Dell, S.D. The SH2B gene is associated with serum leptin and body fat in normal female twins. Obesity (Silver Spring) 2007, 15, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Galatola, M.; Cielo, D.; Panico, C.; Stellato, P.; Malamisura, B.; Carbone, L.; Gianfrani, C.; Troncone, R.; Greco, L.; Auricchio, R. Presymptomatic Diagnosis of Celiac Disease in Predisposed Children: The Role of Gene Expression Profile. J Pediatr. Gastroenterol. Nutr. 2017, 65, 314–320. [Google Scholar] [CrossRef]
- Abete, I.; Goyenechea, E.; Zulet, M.A.; Martínez, J.A. Obesity and metabolic syndrome: Potential benefit from specific nutritional components. Nutr. Metab. Cardiovasc. Dis. 2011, 21 (Suppl. 2), B1–B15. [Google Scholar] [CrossRef]
- Chang, Y.; Cho, Y.K.; Cho, J.; Jung, H.S.; Yun, K.E.; Ahn, J.; Sohn, C.I.; Shin, H.; Ryu, S. Alcoholic and Nonalcoholic Fatty Liver Disease and Liver-Related Mortality: A Cohort Study. Am. J. Gastroenterol. 2019, 114, 620–629. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease—Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef]
- Seko, Y.; Sumida, Y.; Tanaka, S.; Mori, K.; Taketani, H.; Ishiba, H.; Hara, T.; Okajima, A.; Umemura, A.; Nishikawa, T.; et al. Effect of sodium glucose cotransporter 2 inhibitor on liver function tests in Japanese patients with non-alcoholic fatty liver disease andtype 2 diabetes mellitus. Hepatol. Res. 2017, 47, 1072–1078. [Google Scholar] [CrossRef]
- Hsu, C.-L.; Wu, F.-Z.; Lin, K.-H.; Chen, Y.-H.; Wu, P.-C.; Chen, Y.-H.; Chen, C.S.; Wang, W.H.; Mar, G.Y.; Yu, H.C. Role of Fatty Liver Index and Metabolic Factors in the Prediction of Nonalcoholic Fatty Liver Disease in a Lean Population Receiving Health Checkup. Clin. Transl. Gastroenterol. 2019, 10, 1–8. [Google Scholar] [CrossRef]
- Kelishadi, R.; Qorbani, M.; Heshmat, R.; Motamed-Gorji, N.; Motlagh, M.E.; Ziaodini, H.; Taheri, M.; Shafiee, G.; Aminaee, T.; Ahadi, Z.; et al. Association of alanine aminotransferase concentration with cardiometabolic risk factors in children and adolescents: The CASPIAN-V cross- sectional study. Sao Paulo Med. J. 2018, 136, 511–519. [Google Scholar] [CrossRef]
- Mayo, R.; Crespo, J.; Martínez-Arranz, I.; Banales, J.M.; Arias, M.; Mincholé, I.; Aller de la Fuente, R.; Jimenez-Agüero, R.; Alonso, C.; de Luis, D.A.; et al. Metabolomic-based noninvasive serum test to diagnose nonalcoholic steatohepatitis: Results from discovery and validation cohorts. Hepatol. Commun. 2018, 2, 807–820. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Nascimbeni, F.; Ballestri, S.; Fairweather, D.; Win, S.; Than, T.A.; Abdelmalek, M.F.; Suzuki, A. Sex Differences in Nonalcoholic Fatty Liver Disease: State of the Art and Identification of Research Gaps. Hepatology 2019, 70, 1457–1469. [Google Scholar] [CrossRef] [PubMed]
- Marchisello, S.; Di Pino, A.; Scicali, R.; Urbano, F.; Piro, S.; Purrello, F.; Rabuazzo, A.M. Pathophysiological, Molecular and Therapeutic Issues of Nonalcoholic Fatty Liver Disease: An Overview. Int. J. Mol. Sci. 2019, 20, 1948. [Google Scholar] [CrossRef]
- Arsik, I.; Frediani, J.K.; Frezza, D.; Chen, W.; Ayer, T.; Keskinocak, P.; Jin, R.; Konomi, J.V.; Barlow, S.E.; Xanthakos, S.A.; et al. Alanine Aminotransferase as a Monitoring Biomarker in Children with Nonalcoholic Fatty Liver Disease: A Secondary Analysis Using TONIC Trial Data. Children (Basel, Switzerland) 2018, 5, 64. [Google Scholar] [CrossRef]
- Martin-Rodriguez, J.L.; Gonzalez-Cantero, J.; Gonzalez-Cantero, A.; Arrebola, J.P.; Gonzalez-Calvin, J.L. Diagnostic accuracy of serum alanine aminotransferase as biomarker for nonalcoholic fatty liver disease and insulin resistance in healthy subjects, using 3T MR spectroscopy. Medicine (Baltimore) 2017, 96. [Google Scholar] [CrossRef]
- Ma, X.; Liu, S.; Zhang, J.; Dong, M.; Wang, Y.; Wang, M.; Xin, Y. Proportion of NAFLD patients with normal ALT value in overall NAFLD patients: A systematic review and meta-analysis. BMC Gastroenterol. 2020, 20, 10. [Google Scholar] [CrossRef]
- Papatheodoridi, M.; Cholongitas, E. Diagnosis of Non-alcoholic Fatty Liver Disease (NAFLD): Current Concepts. Curr. Pharm. Des. 2018, 24, 4574–4586. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| rs7359397_SH2B1 | |||
|---|---|---|---|
| CC (No-Risk Genotype) n = 54 | CT/TT (Risk Genotype) n = 56 | p-Value | |
| Body composition | |||
| Weight (kg) | 94.2 (14.6) | 97.3 (1.8) | 0.133 |
| BMI (kg/m2) | 33.4 (4.1) | 34.3 (3.6) | 0.105 |
| Age (y) | 51 (47.0–57.0) | 49.5 (45.0–56.5) | 0.797 |
| Sex n (%) | |||
| Male | 25 (46.3) | 37 (66.1) | 0.037 |
| Female | 29 (53.7) | 19 (33.9) | |
| WC (cm) | 108.3 (9.7) | 111.1 (9.1) | 0.119 |
| DXA Body Fat Mass (kg) | 38.0 (32.8–44.6) | 38.6 (34.3–44.5) | 0.935 |
| DXA Lean Mass (kg) | 51.9 (43.9–56.9) | 55.5 (49.4–61.8) | 0.059 |
| DXA VAT (kg) | 2.1 (1.4–3.0) | 2.4 (1.8–3.1) | 0.129 |
| Biochemical parameters | |||
| Glucose (mg/dL) | 100 (91.0–111.0) | 102.5 (92.5–102.5) | 0.421 |
| Insulin (U/mL) | 14.1 (9.0–19.8) | 20.1 (13.4–25.5) | 0.002 |
| TG (mg/dL) | 106.5 (76.0–157.0) | 127.5 (84.5–160.0) | 0.066 |
| TC (mg/dL) | 197.5 (40.4) | 191.3 (36.8) | 0.346 |
| HDL-c (mg/dL) | 54.5 (47.0–64.0) | 47.0 (40.0–55.5) | 0.003 |
| LDL-c (mg/dL) | 117.1 (33.9) | 115.3 (35.1) | 0.788 |
| HOMA-IR | 3.5 (2.2–4.7) | 4.9 (3.5–6.7) | 0.001 |
| HbA1C (%) | 5.6 (5.4–5.9) | 5.6 (5.4–5.9) | 0.622 |
| TyG index | 8.5 (8.1–8.9) | 8.7 (8.3–9.0) | 0.051 |
| Triglycerides/HDL-c (ratio) | 1.8 (1.2–3.2) | 2.7 (1.7–3.3) | 0.021 |
| Waist*TyG index | 929.8 (862.3–1001.3) | 971.2 (900.8–1033.8) | 0.030 |
| HCY (µmol/L) | 14.5 (12.2–16.4) | 15.1 (11.6–18.1) | 0.627 |
| AIP | 0.5 (0.2–1.1) | 0.9 (0.5–1.2) | 0.012 |
| rs7359397_SH2B1 | |||
|---|---|---|---|
| CC (No-Risk Genotype) n = 54 | CT/TT (Risk Genotype) n = 56 | p-Value | |
| Energy and macronutrients | |||
| Total energy (kcal/day) | 2649.7 (2181.9–3257.9) | 2369.4 (1952.7–2827.7) | 0.101 |
| Carbohydrates (%E) | 42.3 (6.8) | 43.0 (6.8) | 0.612 |
| Proteins (%E) | 15.7 (14.9–18.1) | 17.3 (15.4–20.4) | 0.028 |
| Fats (%E) | 38.1 (6.14) | 36.7 (7.3) | 0.308 |
| MUFA (%E) | 18.6 (15.5–20.9) | 16.2 (14.0–20.0) | 0.045 |
| PUFA (%E) | 5.4 (4.4–6.7) | 5.1 (4.4–6.4) | 0.466 |
| SFA (%E) | 10.4 (9.3–12.1) | 10.3 (9.21–1.8) | 0.750 |
| Dietary fiber (g/day) | 25.2 (21.2–30.1) | 21.3 (17.0–26.8) | 0.049 |
| Glycemic Index | 53.3 (48.5–58.9) | 54.9 (49.1–57.8) | 0.988 |
| Glycemic Load | 158.6 (98.2–205.6) | 139.1 (95.4–176.9) | 0.449 |
| Lifestyle factors | |||
| Adherence to MedDiet | 5.9 (2.1) | 6.0 (2.0) | 0.678 |
| Physical activity n (%) | |||
| Sedentary | 21 (38.8) | 24 (42.8) | |
| Mild | 16 (29.6) | 13 (23.2) | 0.685 |
| Moderated | 9 (16.6) | 13 (23.2) | |
| Elevated | 8 (14.8) | 6 (10.71) | |
| rs7359397_SH2B1 | |||
|---|---|---|---|
| CC (No-Risk Genotype) n = 54 | CT/TT (Risk Genotype) n = 56 | p-Value | |
| Liver markers | |||
| CRP (mg/dL) | 0.2 (0.1–0.4) | 0.2 (0.1–0.5) | 0.959 |
| FGF21 (pg/mL) | 182.0 (96.6–302.0) | 214.0 (122.0–478.0) | 0.109 |
| AST (U/L) | 23.5 (18.0–28.0) | 21.0 (18.0–29.0) | 0.995 |
| ALT (U/L) | 26.0 (18.0–39.0) | 30.0 (22.0–46.0) | 0.266 |
| Ratio AST/ALT | 0.8 (0.6–1.0) | 0.7 (0.6–0.9) | 0.149 |
| GGT (U/L) | 26.0 (19.0–40.0) | 32.0 (22.5–44.0) | 0.109 |
| FLI | 79.8 (66.3–91.2) | 87.5 (76.6–93.7) | 0.032 |
| Liver imaging techniques | |||
| Grade of steatosis (ultrasonography) n (%) | |||
| Mild steatosis | 39 (72.2) | 22 (39.29) | |
| Moderate steatosis | 11 (20.37) | 26 (46.43) | 0.001 |
| Severe steatosis | 4 (7.41) | 8 (14.29) | |
| TE liver stiffness (kPa) | 4.5 (3.8–6.1) | 4.5 (3.8–5.6) | 0.738 |
| MRI Hepatic Volume (mL) | 1701.0 (1409.0–1998.0) | 1843.0 (1589.0–2111.0) | 0.150 |
| MRI Liver fat—Dixon (%) | 4.5 (2.9–8.9) | 6.9 (4.4–12.4) | 0.055 |
| MRI Hepatic Iron—Dixon (%) | 31.8 (28.2–44.2) | 32.4 (29.2–38.0) | 0.950 |
| Lipidomic analysis (OWLiver®-test) n (%) | |||
| No NAFLD | 16 (29.6) | 4 (7.3) | |
| Hepatic steatosis | 14 (25.9) | 13 (23.6) | 0.006 |
| NASH | 24 (44.4) | 38 (69.1) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perez-Diaz-del-Campo, N.; Abete, I.; Cantero, I.; Marin-Alejandre, B.A.; Monreal, J.I.; Elorz, M.; Herrero, J.I.; Benito-Boillos, A.; Riezu-Boj, J.I.; Milagro, F.I.; et al. Association of the SH2B1 rs7359397 Gene Polymorphism with Steatosis Severity in Subjects with Obesity and Non-Alcoholic Fatty Liver Disease. Nutrients 2020, 12, 1260. https://doi.org/10.3390/nu12051260
Perez-Diaz-del-Campo N, Abete I, Cantero I, Marin-Alejandre BA, Monreal JI, Elorz M, Herrero JI, Benito-Boillos A, Riezu-Boj JI, Milagro FI, et al. Association of the SH2B1 rs7359397 Gene Polymorphism with Steatosis Severity in Subjects with Obesity and Non-Alcoholic Fatty Liver Disease. Nutrients. 2020; 12(5):1260. https://doi.org/10.3390/nu12051260
Chicago/Turabian StylePerez-Diaz-del-Campo, Nuria, Itziar Abete, Irene Cantero, Bertha Araceli Marin-Alejandre, J. Ignacio Monreal, Mariana Elorz, José Ignacio Herrero, Alberto Benito-Boillos, Jose I. Riezu-Boj, Fermín I. Milagro, and et al. 2020. "Association of the SH2B1 rs7359397 Gene Polymorphism with Steatosis Severity in Subjects with Obesity and Non-Alcoholic Fatty Liver Disease" Nutrients 12, no. 5: 1260. https://doi.org/10.3390/nu12051260
APA StylePerez-Diaz-del-Campo, N., Abete, I., Cantero, I., Marin-Alejandre, B. A., Monreal, J. I., Elorz, M., Herrero, J. I., Benito-Boillos, A., Riezu-Boj, J. I., Milagro, F. I., Tur, J. A., Martinez, J. A., & Zulet, M. A. (2020). Association of the SH2B1 rs7359397 Gene Polymorphism with Steatosis Severity in Subjects with Obesity and Non-Alcoholic Fatty Liver Disease. Nutrients, 12(5), 1260. https://doi.org/10.3390/nu12051260