Shea Nut Oil Extracts Enhance the Intra-Articular Sodium Hyaluronate Effectiveness on Surgically Induced OA Progression in Rats


Abstract
1. Introduction
2. Materials and Methods
2.1. ACLT + MMx-Induced OA Animal Model
2.2. Experimental Design
2.3. Knee Width and Weight-Bearing Test
2.4. Histopathological Examination of Knee Joint
2.5. Metabolic Profile of Blood Biochemistry Assays
2.6. Statistical Analysis
3. Results
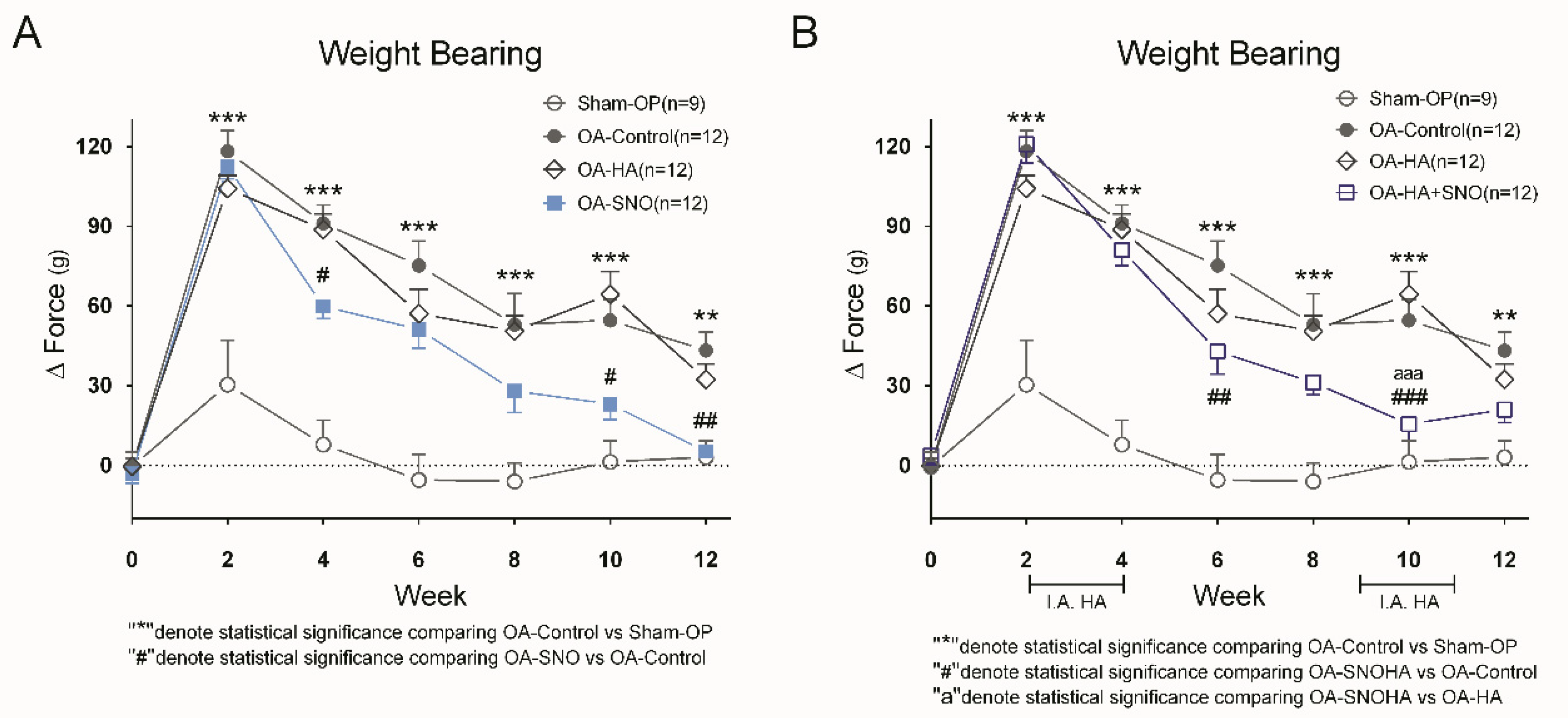
3.1. SNO, but not HA, Attenuates Knee Joint Pain and Inflammatory Swelling in ACLT + MMx-Induced OA Rats
3.2. SNO, HA Alone, and HA Plus SNO, Offered Significant Improvement in Cartilage Integrity in Knee OA Rats
3.3. Metabolic Profiling of OA Rats Receiving Daily Oral Supplementation of SNO
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Litwic, A.; Edwards, M.H.; Dennison, E.M.; Cooper, C. Epidemiology and Burden of Osteoarthritis. Br. Med. Bull. 2013, 105, 185–199. [Google Scholar] [CrossRef] [PubMed]
- Neogi, T. The Epidemiology and Impact of Pain in Osteoarthritis. Osteoarthr. Cartil. 2013, 21, 1145–1153. [Google Scholar] [CrossRef] [PubMed]
- Dominick, K.L.; Ahern, F.M.; Gold, C.H.; Heller, D.A. Health-Related Quality of Life and Health Service Use among Older Adults with Osteoarthritis. Arthritis Rheum. 2004, 51, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.J.; Riordan, E.A. The Impact of Arthritis on Pain and Quality of Life: An Australian Survey. Int. J. Rheum. Dis. 2014, 17, 149–155. [Google Scholar] [CrossRef]
- Barbour, K.E.; Helmick, C.G.; Boring, M.; Brady, T.J. Vital Signs: Prevalence of Doctor-Diagnosed Arthritis and Arthritis-Attributable Activity Limitation - United States, 2013–2015. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 246–253. [Google Scholar] [CrossRef]
- Felson, D.T.; Zhang, Y. An Update on the Epidemiology of Knee and Hip Osteoarthritis with a View to Prevention. Arthritis Rheum. 1998, 41, 1343–1355. [Google Scholar] [CrossRef]
- Roos, E.M.; Arden, N.K. Strategies for the Prevention of Knee Osteoarthritis. Nat. Rev. Rheumatol. 2016, 12, 92–101. [Google Scholar] [CrossRef]
- O’Neill, T.W.; Felson, D.T. Mechanisms of Osteoarthritis (Oa) Pain. Curr. Osteoporos. Rep. 2018, 16, 611–616. [Google Scholar] [CrossRef]
- Hunter, D.J.; Schofield, D.; Callander, E. The Individual and Socioeconomic Impact of Osteoarthritis. Nat. Rev. Rheumatol. 2014, 10, 437–441. [Google Scholar] [CrossRef]
- Wehling, P.; Evans, C.; Wehling, J.; Maixner, W. Effectiveness of Intra-Articular Therapies in Osteoarthritis: A Literature Review. Ther. Adv. Musculoskelet Dis. 2017, 9, 183–196. [Google Scholar] [CrossRef]
- Bannuru, R.R.; Osani, M.; Vaysbrot, E.E.; McAlindon, T.E. Comparative Safety Profile of Hyaluronic Acid Products for Knee Osteoarthritis: A Systematic Review and Network Meta-Analysis. Osteoarthr. Cartil. 2016, 24, 2022–2041. [Google Scholar] [CrossRef]
- Busse, P.; Vater, C.; Stiehler, M.; Nowotny, J.; Kasten, P.; Bretschneider, H.; Goodman, S.B.; Gelinsky, M.; Zwingenberger, S. Cytotoxicity of Drugs Injected into Joints in Orthopaedics. Bone Joint Res. 2019, 8, 41–48. [Google Scholar] [CrossRef]
- Altman, R.; Fredericson, M.; Bhattacharyya, S.K.; Bisson, B.; Abbott, T.; Yadalam, S.; Kim, M. Association between Hyaluronic Acid Injections and Time-to-Total Knee Replacement Surgery. J. Knee Surg. 2016, 29, 564–570. [Google Scholar] [CrossRef]
- Delbarre, A.; Amor, B.; Bardoulat, I.; Tetafort, A.; Pelletier-Fleury, N. Do Intra-Articular Hyaluronic Acid Injections Delay Total Knee Replacement in Patients with Osteoarthritis - a Cox Model Analysis. PLoS ONE 2017, 12, e0187227. [Google Scholar] [CrossRef]
- Maheu, E.; Rannou, F.; Reginster, J.Y. Efficacy and Safety of Hyaluronic Acid in the Management of Osteoarthritis: Evidence from Real-Life Setting Trials and Surveys. Semin. Arthritis Rheum. 2016, 45 (Suppl. 4), S28–S33. [Google Scholar] [CrossRef]
- Dasa, V.; Lim, S.; Heeckt, P. Real-World Evidence for Safety and Effectiveness of Repeated Courses of Hyaluronic Acid Injections on the Time to Knee Replacement Surgery. Am. J. Orthop. (Belle Mead NJ) 2018, 47. [Google Scholar] [CrossRef] [PubMed]
- Honfo, F.G.; Akissoe, N.; Linnemann, A.R.; Soumanou, M.; Van Boekel, M.A. Nutritional Composition of Shea Products and Chemical Properties of Shea Butter: A Review. Crit. Rev. Food Sci. Nutr. 2014, 54, 673–686. [Google Scholar] [CrossRef] [PubMed]
- Cheras, P.A.; Myers, S.P.; Paul-Brent, P.A.; Outerbridge, K.H.; Nielsen, G.V. Randomized Double-Blind Placebo-Controlled Trial on the Potential Modes of Action of Sheaflex70 in Osteoarthritis. Phytother. Res. 2010, 24, 1126–1131. [Google Scholar] [PubMed]
- Chen, S.P.; Lo, S.F.; Wang, Y.C.; Chou, T.Y.; Chang, K.M.; Chou, L.W. Validating Efficacy of Shea Nut Oil Extract in Knee Osteoarthritis Patients. Evid. Based Complem. Altern. Med. 2013, 2013, 147163. [Google Scholar] [CrossRef]
- Kao, J.H.; Lin, S.H.; Lai, C.F.; Lin, Y.C.; Kong, Z.L.; Wong, C.S. Shea Nut Oil Triterpene Concentrate Attenuates Knee Osteoarthritis Development in Rats: Evidence from Knee Joint Histology. PLoS ONE 2016, 11, e0162022. [Google Scholar] [CrossRef]
- Chen, I.J.; Lin, S.H.; Wong, C.S. Oral Shea Nut Oil Triterpene Concentrate Supplement Ameliorates Pain and Histological Assessment of Articular Cartilage Deterioration in an Aclt Injured Rat Knee Osteoarthritis Model. PLoS ONE 2019, 14, e0215812. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, K.A.; Paszcuk, A.F.; Passos, G.F.; Silva, E.S.; Bento, A.F.; Meotti, F.C.; Calixto, J.B. Activation of Cannabinoid Receptors by the Pentacyclic Triterpene Alpha,Beta-Amyrin Inhibits Inflammatory and Neuropathic Persistent Pain in Mice. Pain 2011, 152, 1872–1887. [Google Scholar] [CrossRef] [PubMed]
- Otuki, M.F.; Ferreira, J.; Lima, F.V.; Meyre-Silva, C.; Malheiros, A.; Muller, L.A.; Cani, G.S.; Santos, A.R.; Yunes, R.A.; Calixto, J.B. Antinociceptive Properties of Mixture of Alpha-Amyrin and Beta-Amyrin Triterpenes: Evidence for Participation of Protein Kinase C and Protein Kinase a Pathways. J. Pharmacol. Exp. Ther. 2005, 313, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.H.; Chuang, H.Y.; Chen, C.H.; Chen, W.K.; Hwang, J.J. Lupeol Acetate Ameliorates Collagen-Induced Arthritis and Osteoclastogenesis of Mice through Improvement of Microenvironment. Biomed. Pharmacother. 2016, 79, 231–240. [Google Scholar] [CrossRef]
- Gupta, R.; Sharma, A.K.; Sharma, M.C.; Dobhal, M.P.; Gupta, R.S. Evaluation of Antidiabetic and Antioxidant Potential of Lupeol in Experimental Hyperglycaemia. Nat. Prod. Res. 2012, 26, 1125–1129. [Google Scholar] [CrossRef]
- Singh, D.; Arya, P.V.; Sharma, A.; Dobhal, M.P.; Gupta, R.S. Modulatory Potential of Alpha-Amyrin against Hepatic Oxidative Stress through Antioxidant Status in Wistar Albino Rats. J. Ethnopharmacol. 2015, 161, 186–193. [Google Scholar] [CrossRef]
- Cardoso, B.K.; de Oliveira, H.L.M.; Melo, U.Z.; Cfaa Campo Fernandez, C.M.M.; Goncalves, J.E.; Laverde, A., Jr.; Romagnolo, M.B.; Linde, G.A.; Gazim, Z.C. Antioxidant Activity of Alpha and Beta-Amyrin Isolated from Myrcianthes Pungens Leaves. Nat. Prod. Res. 2018, 1–5. [Google Scholar] [CrossRef]
- Parvez, M.K.; Alam, P.; Arbab, A.H.; Al-Dosari, M.S.; Alhowiriny, T.A.; Alqasoumi, S.I. Analysis of Antioxidative and Antiviral Biomarkers Beta-Amyrin, Beta-Sitosterol, Lupeol, Ursolic Acid in Guiera Senegalensis Leaves Extract by Validated Hptlc Methods. Saudi Pharm. J. 2018, 26, 685–693. [Google Scholar] [CrossRef]
- Sudirman, S.; Chen, C.K.; Long, B.T.; Chang, H.W.; Tsou, D.; Kong, Z.L. Vitellaria Paradoxa Nut Triterpene-Rich Extract Ameliorates Symptoms of Inflammation on Post-Traumatic Osteoarthritis in Obese Rats. J. Pain Res. 2020, 2020, 261–271. [Google Scholar] [CrossRef]
- Euppayo, T.; Punyapornwithaya, V.; Chomdej, S.; Ongchai, S.; Nganvongpanit, K. Effects of Hyaluronic Acid Combined with Anti-Inflammatory Drugs Compared with Hyaluronic Acid Alone, in Clinical Trials and Experiments in Osteoarthritis: A Systematic Review and Meta-Analysis. BMC Musculosk. Disord. 2017, 18, 387. [Google Scholar] [CrossRef]
- Bove, S.E.; Calcaterra, S.L.; Brooker, R.M.; Huber, C.M.; Guzman, R.E.; Juneau, P.L.; Schrier, D.J.; Kilgore, K.S. Weight Bearing as a Measure of Disease Progression and Efficacy of Anti-Inflammatory Compounds in a Model of Monosodium Iodoacetate-Induced Osteoarthritis. Osteoarthr. Cartil. 2003, 11, 821–830. [Google Scholar] [CrossRef]
- Fernihough, J.; Gentry, C.; Malcangio, M.; Fox, A.; Rediske, J.; Pellas, T.; Kidd, B.; Bevan, S.; Winter, J. Pain Related Behaviour in Two Models of Osteoarthritis in the Rat Knee. Pain 2004, 112, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Gerwin, N.; Bendele, A.M.; Glasson, S.; Carlson, C.S. The Oarsi Histopathology Initiative - Recommendations for Histological Assessments of Osteoarthritis in the Rat. Osteoarthr. Cartil. 2010, 18 (Suppl. 3), S24–S34. [Google Scholar] [CrossRef] [PubMed]
- Mobasheri, A.; Rayman, M.P.; Gualillo, O.; Sellam, J.; van der Kraan, P.; Fearon, U. The Role of Metabolism in the Pathogenesis of Osteoarthritis. Nat. Rev. Rheumatol. 2017, 13, 302–311. [Google Scholar] [CrossRef] [PubMed]
- McAlindon, T.E.; Bannuru, R.R.; Sullivan, M.C.; Arden, N.K.; Berenbaum, F.; Bierma-Zeinstra, S.M.; Hawker, G.A.; Henrotin, Y.; Hunter, D.J.; Kawaguchi, H.; et al. Oarsi Guidelines for the Non-Surgical Management of Knee Osteoarthritis. Osteoarthr. Cartil. 2014, 22, 363–388. [Google Scholar] [CrossRef]
- Hochberg, M.C.; Altman, R.D.; April, K.T.; Benkhalti, M.; Guyatt, G.; McGowan, J.; Towheed, T.; Welch, V.; Wells, G.; Tugwell, P. American College of Rheumatology 2012 Recommendations for the Use of Nonpharmacologic and Pharmacologic Therapies in Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. 2012, 64, 465–474. [Google Scholar] [CrossRef]
- Jevsevar, D.S. Treatment of Osteoarthritis of the Knee: Evidence-Based Guideline, 2nd Edition. J. Am. Acad. Orthop. Surg. 2013, 21, 571–576. [Google Scholar]
- Urban, H.; Little, C.B. The Role of Fat and Inflammation in the Pathogenesis and Management of Osteoarthritis. Rheumatology 2018, 57 (Suppl. 4), iv10–iv21. [Google Scholar] [CrossRef]
- Onur, T.; Wu, R.; Metz, L.; Dang, A. Characterisation of Osteoarthritis in a Small Animal Model of Type 2 Diabetes Mellitus. Bone Joint Res. 2014, 3, 203–211. [Google Scholar] [CrossRef]
- Mooney, R.A.; Sampson, E.R.; Lerea, J.; Rosier, R.N.; Zuscik, M.J. High-Fat Diet Accelerates Progression of Osteoarthritis after Meniscal/Ligamentous Injury. Arthritis Res. Ther. 2011, 13, R198. [Google Scholar] [CrossRef]
- Datta, P.; Zhang, Y.; Parousis, A.; Sharma, A.; Rossomacha, E.; Endisha, H.; Wu, B.; Kacprzak, I.; Mahomed, N.N.; Gandhi, R.; et al. High-Fat Diet-Induced Acceleration of Osteoarthritis Is Associated with a Distinct and Sustained Plasma Metabolite Signature. Sci. Rep. 2017, 7, 8205. [Google Scholar] [CrossRef] [PubMed]
- De Sire, A.; de Sire, R.; Petito, V.; Masi, L.; Cisari, C.; Gasbarrini, A.; Scaldaferri, F.; Invernizzi, M. Gut-Joint Axis: The Role of Physical Exercise on Gut Microbiota Modulation in Older People with Osteoarthritis. Nutrients 2020, 12, 574. [Google Scholar] [CrossRef]
- Berthelot, J.M.; Sellam, J.; Maugars, Y.; Berenbaum, F. Cartilage-Gut-Microbiome Axis: A New Paradigm for Novel Therapeutic Opportunities in Osteoarthritis. RMD Open 2019, 5, e001037. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.Y.; Stabler, T.; Pei, F.X.; Kraus, V.B. Both Systemic and Local Lipopolysaccharide (Lps) Burden Are Associated with Knee Oa Severity and Inflammation. Osteoarthr. Cartil. 2016, 24, 1769–1775. [Google Scholar] [CrossRef] [PubMed]
- Collins, K.H.; Paul, H.A.; Reimer, R.A.; Seerattan, R.A.; Hart, D.A.; Herzog, W. Relationship between Inflammation, the Gut Microbiota, and Metabolic Osteoarthritis Development: Studies in a Rat Model. Osteoarthr. Cartil. 2015, 23, 1989–1998. [Google Scholar] [CrossRef] [PubMed]
- Szychlinska, M.A.; Di Rosa, M.; Castorina, A.; Mobasheri, A.; Musumeci, G. A Correlation between Intestinal Microbiota Dysbiosis and Osteoarthritis. Heliyon 2019, 5, e01134. [Google Scholar] [CrossRef]
- Favazzo, L.J.; Hendesi, H.; Villani, D.A.; Soniwala, S.; Dar, Q.A.; Schott, E.M.; Gill, S.R.; Zuscik, M.J. The Gut Microbiome-Joint Connection: Implications in Osteoarthritis. Curr. Opin. Rheumatol. 2020, 32, 92–101. [Google Scholar] [CrossRef]
- De Melo, K.M.; de Oliveira, F.T.B.; Costa Silva, R.A.; Gomes Quindere, A.L.; Marinho Filho, J.D.B.; Araujo, A.J.; Barros Pereira, E.D.; Carvalho, A.A.; Chaves, M.H.; Rao, V.S.; et al. Alpha, Beta-Amyrin, a Pentacyclic Triterpenoid from Protium Heptaphyllum Suppresses Adipocyte Differentiation Accompanied by Down Regulation of Ppargamma and C/Ebpalpha in 3t3-L1 Cells. Biomed. Pharmacother. 2019, 109, 1860–1866. [Google Scholar] [CrossRef]
- Santos, F.A.; Frota, J.T.; Arruda, B.R.; de Melo, T.S.; da Silva, A.A.; Brito, G.A.; Chaves, M.H.; Rao, V.S. Antihyperglycemic and Hypolipidemic Effects of Alpha, Beta-Amyrin, a Triterpenoid Mixture from Protium Heptaphyllum in Mice. Lipids Health Dis. 2012, 11, 98. [Google Scholar] [CrossRef]
- Sudhahar, V.; Kumar, S.A.; Sudharsan, P.T.; Varalakshmi, P. Protective Effect of Lupeol and Its Ester on Cardiac Abnormalities in Experimental Hypercholesterolemia. Vasc. Pharmacol. 2007, 46, 412–418. [Google Scholar] [CrossRef]
- Lippiello, L.; Walsh, T.; Fienhold, M. The Association of Lipid Abnormalities with Tissue Pathology in Human Osteoarthritic Articular Cartilage. Metabolism 1991, 40, 571–576. [Google Scholar] [CrossRef]
- Wu, C.L.; Kimmerling, K.A.; Little, D.; Guilak, F. Serum and Synovial Fluid Lipidomic Profiles Predict Obesity-Associated Osteoarthritis, Synovitis, and Wound Repair. Sci. Rep. 2017, 7, 44315. [Google Scholar] [CrossRef] [PubMed]
- Bastiaansen-Jenniskens, Y.M.; Siawash, M.; van de Lest, C.H.; Verhaar, J.A.; Kloppenburg, M.; Zuurmond, A.M.; Stojanovic-Susulic, V.; Van Osch, G.J.; Clockaerts, S. Monounsaturated and Saturated, but Not N-6 Polyunsaturated Fatty Acids Decrease Cartilage Destruction under Inflammatory Conditions: A Preliminary Study. Cartilage 2013, 4, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Ikeuchi, M.; Izumi, M.; Aso, K.; Sugimura, N.; Kato, T.; Tani, T. Effects of Intra-Articular Hyaluronic Acid Injection on Immunohistochemical Characterization of Joint Afferents in a Rat Model of Knee Osteoarthritis. Eur. J. Pain 2015, 19, 334–340. [Google Scholar] [CrossRef]
- Boettger, M.K.; Kummel, D.; Harrison, A.; Schaible, H.G. Evaluation of Long-Term Antinociceptive Properties of Stabilized Hyaluronic Acid Preparation (Nasha) in an Animal Model of Repetitive Joint Pain. Arthritis Res. Ther. 2011, 13, R110. [Google Scholar] [CrossRef]
- Jimbo, S.; Terashima, Y.; Teramoto, A.; Takebayashi, T.; Ogon, I.; Watanabe, K.; Sato, T.; Ichise, N.; Tohse, N.; Yamashita, T. Antinociceptive Effects of Hyaluronic Acid on Monoiodoacetate-Induced Ankle Osteoarthritis in Rats. J. Pain Res. 2019, 12, 191–200. [Google Scholar] [CrossRef]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. Oarsi Guidelines for the Non-Surgical Management of Knee, Hip, and Polyarticular Osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef]
- Henrotin, Y.; Lambert, C.; Couchourel, D.; Ripoll, C.; Chiotelli, E. Nutraceuticals: Do They Represent a New Era in the Management of Osteoarthritis? - A Narrative Review from the Lessons Taken with Five Products. Osteoarthr. Cartil. 2011, 19, 1–21. [Google Scholar] [CrossRef]
- Wang, A.; Leong, D.J.; Cardoso, L.; Sun, H.B. Nutraceuticals and Osteoarthritis Pain. Pharmacol. Ther. 2018, 187, 167–179. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sham-OP (n = 7) | OA-Control (n = 12) | OA-HA (n = 12) | OA-SNO (n = 12) | OA-SNOHA (n = 12) | |
|---|---|---|---|---|---|
| Cartilage matrix loss 0% (mm) | 0 *** | 2.292 ± 0.074 | 1.951 ± 0.087 ** | 1.864 ± 0.107 ** | 1.865 ± 0.060 *** |
| Cartilage matrix loss 50% (mm) | 0 *** | 0.792 ± 0.144 | 0.386 ± 0.102 * | 0.342 ± 0.103 * | 0.272 ± 0.116 ** |
| Cartilage matrix loss 100% (mm) | 0 ** | 0.372 ± 0.093 | 0.183 ± 0.076 | 0.217 ± 0.075 | 0.160 ± 0.061 |
| Medial Tibia Cartilage Degeneration Score | 0 *** | 6.208 ± 0.408 | 5.000 ± 0.371 * | 5.750 ± 0.439 | 4.791 ± 0.307 ** |
| └ Outside zone | 0 *** | 1.625 ± 0.334 | 1.458 ± 0.289 | 1.875 ± 0.326 | 1.375 ± 0.287 |
| └ Middle zone | 0 *** | 1.875 ± 0.163 | 1.708 ± 0.185 | 2.042 ± 0.153 | 1.833 ± 0.130 |
| └ Inside zone | 0 *** | 2.708 ± 0.195 | 1.833 ± 0.214 ** | 1.833 ± 0.177 ** | 1.583 ± 0.133 *** |
| Total cartilage degeneration width (mm) | 0 *** | 2.475 ± 0.073 | 2.213 ± 0.070 * | 2.335 ± 0.073 | 2.215 ± 0.058 ** |
| Significant cartilage degeneration width (mm) | 0 *** | 0.947 ± 0.111 | 0.612 ± 0.110 * | 0.528 ± 0.127 * | 0.368 ± 0.117 *** |
| Zonal depth ratio of lesions | 0 *** | 0.469 ± 0.039 | 0.358 ± 0.029 * | 0.331 ± 0.024 ** | 0.313 ± 0.020 *** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, I.-J.; Wong, C.-S. Shea Nut Oil Extracts Enhance the Intra-Articular Sodium Hyaluronate Effectiveness on Surgically Induced OA Progression in Rats. Nutrients 2020, 12, 957. https://doi.org/10.3390/nu12040957
Chen I-J, Wong C-S. Shea Nut Oil Extracts Enhance the Intra-Articular Sodium Hyaluronate Effectiveness on Surgically Induced OA Progression in Rats. Nutrients. 2020; 12(4):957. https://doi.org/10.3390/nu12040957
Chicago/Turabian StyleChen, Ing-Jung, and Chih-Shung Wong. 2020. "Shea Nut Oil Extracts Enhance the Intra-Articular Sodium Hyaluronate Effectiveness on Surgically Induced OA Progression in Rats" Nutrients 12, no. 4: 957. https://doi.org/10.3390/nu12040957
APA StyleChen, I.-J., & Wong, C.-S. (2020). Shea Nut Oil Extracts Enhance the Intra-Articular Sodium Hyaluronate Effectiveness on Surgically Induced OA Progression in Rats. Nutrients, 12(4), 957. https://doi.org/10.3390/nu12040957