Prospective Association between Whole Grain Consumption and Hypertension: The Furukawa Nutrition and Health Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Procedure
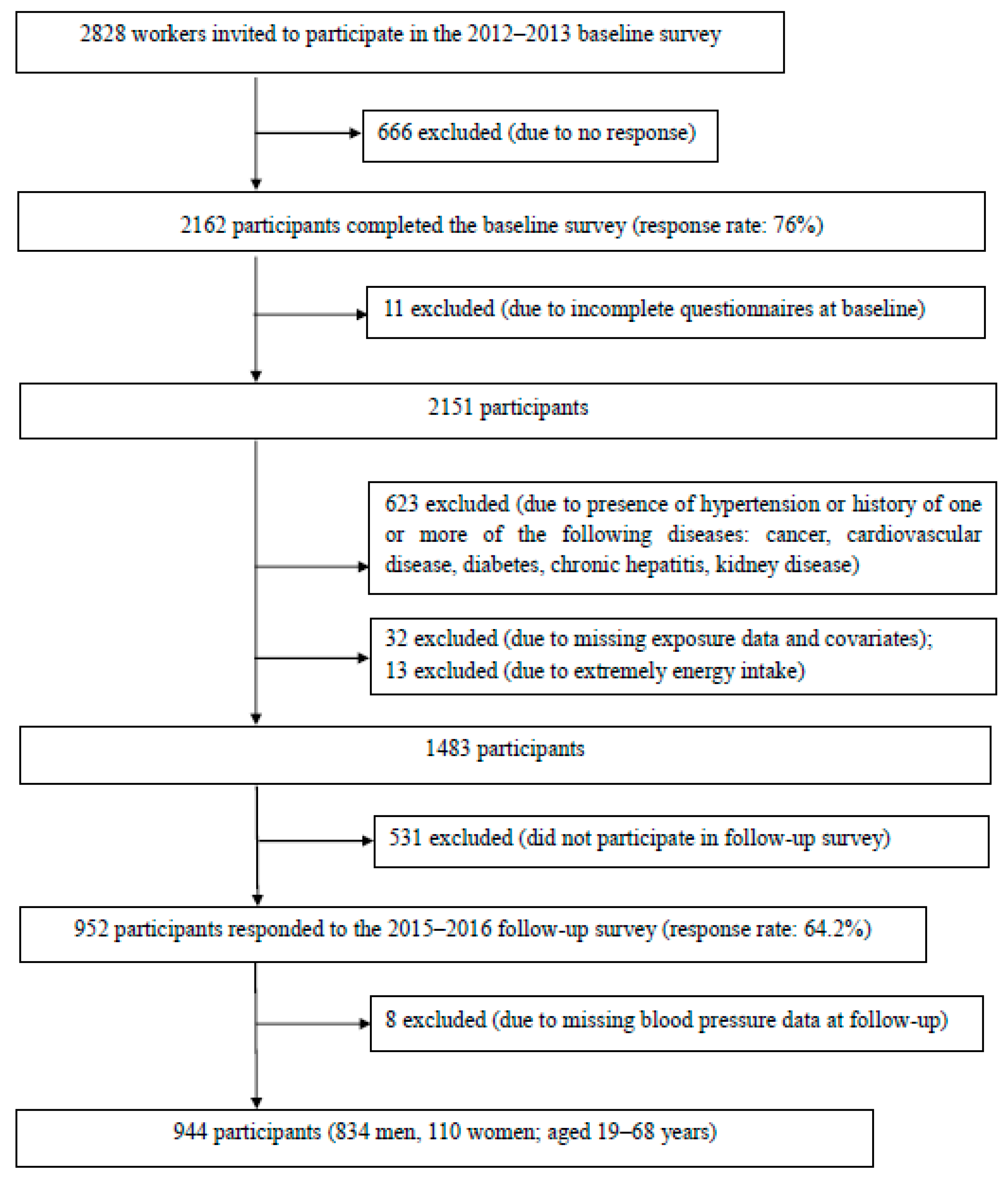
2.2. Participants
2.3. Definition of Hypertension
2.4. Assessment of Dietary Intakes
2.5. Assessment of Other Health-Related Variables
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Forouzanfar, M.H.; Liu, P.; Roth, G.A.; Ng, M.; Biryukov, S.; Marczak, L.; Alexander, L.; Estep, K.; Hassen Abate, K.; Akinyemiju, T.F.; et al. Global burden of hypertension and systolic blood pressure of at least 110 to 115 mm Hg, 1990–2015. JAMA 2017, 317, 165–182. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Hypertension. Available online: https://www.who.int/news-room/fact-sheets/detail/hypertension (accessed on 1 February 2020).
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Knuppel, S.; Iqbal, K.; Andriolo, V.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of hypertension: A systematic review and dose-response meta-analysis of prospective studies. Adv. Nutr. 2017, 8, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Millen, B.E.; Abrams, S.; Adams-Campbell, L.; Anderson, C.A.; Brenna, J.T.; Campbell, W.W.; Clinton, S.; Hu, F.; Nelson, M.; Neuhouser, M.L. The 2015 Dietary Guidelines Advisory Committee scientific report: Development and major conclusions. Adv. Nutr. 2016, 7, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Micha, R.; Khatibzadeh, S.; Shi, P.; Andrews, K.G.; Engell, R.E.; Mozaffarian, D. Global, regional and national consumption of major food groups in 1990 and 2010: A systematic analysis including 266 country-specific nutrition surveys worldwide. BMJ Open 2015, 5, e008705. [Google Scholar] [CrossRef] [PubMed]
- Miki, T.; Eguchi, M.; Kuwahara, K.; Kochi, T.; Akter, S.; Kashino, I.; Hu, H.; Kurotani, K.; Kabe, I.; Kawakami, N.; et al. Breakfast consumption and the risk of depressive symptoms: The Furukawa Nutrition and Health Study. Psychiatry Res. 2019, 273, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Comparison of relative validity of food group intakes estimated by comprehensive and brief-type self-administered diet history questionnaires against 16 d dietary records in Japanese adults. Public Health Nutr. 2011, 14, 1200–1211. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Honda, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Both comprehensive and brief self-administered diet history questionnaires satisfactorily rank nutrient intakes in Japanese adults. J. Epidemiol. 2012, 22, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Science and Technology Agency. Standard Tables of Food Composition in Japan, 5th Revised and Enlarged ed.; Printing Bureau of the Ministry of Finance: Tokyo, Japan, 2005. (In Japanese)
- Akter, S.; Eguchi, M.; Kurotani, K.; Kochi, T.; Pham, N.M.; Ito, R.; Kuwahara, K.; Tsuruoka, H.; Mizoue, T.; Kabe, I.; et al. High dietary acid load is associated with increased prevalence of hypertension: The Furukawa Nutrition and Health Study. Nutrition 2015, 31, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Esmaillzadeh, A.; Mirmiran, P.; Azizi, F. Whole-grain consumption and the metabolic syndrome: A favorable association in Tehranian adults. Eur. J. Clin. Nutr. 2005, 59, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Shobako, N.; Fukuhara, I.; Satoh, H.; Kobayashi, E.; Kusakari, T.; Suwa, M.; Matsumoto, M.; Ishikado, A. Rice bran supplement containing a functional substance, the novel peptide Leu-Arg-Ala, has anti-hypertensive effects: A double-blind, randomized, placebo-controlled study. Nutrients 2019, 11, 726. [Google Scholar] [CrossRef] [PubMed]
- Shobako, N.; Ishikado, A.; Ogawa, Y.; Sono, Y.; Kusakari, T.; Suwa, M.; Matsumoto, M.; Ohinata, K. Vasorelaxant and antihypertensive effects that are dependent on the endothelial NO system exhibited by rice bran-derived tripeptide. J. Agric. Food Chem. 2019, 67, 1437–1442. [Google Scholar] [CrossRef] [PubMed]
- Ardiansyah; Shirakawa, H.; Koseki, T.; Ohinata, K.; Hashizume, K.; Komai, M. Rice bran fractions improve blood pressure, lipid profile, and glucose metabolism in stroke-prone spontaneously hypertensive rats. J. Agric. Food Chem. 2006, 54, 1914–1920. [Google Scholar] [CrossRef] [PubMed]
- Jan-On, G.; Sangartit, W.; Pakdeechote, P.; Kukongviriyapan, V.; Sattayasai, J.; Senaphan, K.; Kukongviriyapan, U. Virgin rice bran oil alleviates hypertension through the upregulation of eNOS and reduction of oxidative stress and inflammation in L-NAME-induced hypertensive rats. Nutrition 2020, 69, 110575. [Google Scholar] [CrossRef] [PubMed]
- Ma, P.; Li, T.; Ji, F.; Wang, H.; Pang, J. Effect of GABA on blood pressure and blood dynamics of anesthetic rats. Int. J. Clin. Exp. Med. 2015, 8, 14296–14302. [Google Scholar] [PubMed]
- Marques, F.Z.; Nelson, E.; Chu, P.Y.; Horlock, D.; Fiedler, A.; Ziemann, M.; Tan, J.K.; Kuruppu, S.; Rajapakse, N.W.; El-Osta, A.; et al. High-Fiber Diet and Acetate Supplementation Change the Gut Microbiota and Prevent the Development of Hypertension and Heart Failure in Hypertensive Mice. Circulation 2017, 135, 964–977. [Google Scholar] [CrossRef]


{kind=link}
| Frequency of Whole Grain Intake | ||||
|---|---|---|---|---|
| Never | Rarely | Sometimes or Always | ptrend1) | |
| No. of participants | 530 | 221 | 193 | |
| Age, years (mean ± SD) | 39.7 ± 8.7 | 39.4 ± 8.8 | 40.9 ± 8.0 | 0.18 |
| Females, % | 10.6 | 11.3 | 15.0 | 0.12 |
| Work site (survey in April 2012), % | 56.0 | 52.9 | 44.6 | 0.01 |
| Smoking status (current), % | 34.9 | 28.1 | 21.8 | <0.001 |
| Physical activity during work, housework, or commuting to work (≥20 METs-hours/day), % | 28.3 | 19.5 | 12.4 | <0.001 |
| Leisure-time physical activity (≥10 METs-hours/week), % | 24.9 | 30.3 | 34.2 | 0.01 |
| Body mass index (mean ± SD), kg/m2 | 22.4 ± 2.8 | 23.0 ± 3.2 | 22.4 ± 2.6 | 0.02 |
| Night or rotating shift work (yes), % | 26.8 | 13.6 | 8.8 | <0.001 |
| Overtime work (≥30 hours/month), % | 24.5 | 26.2 | 26.9 | 0.47 |
| Alcohol consumption (current), % 2) | 52.5 | 47.1 | 53.9 | 0.97 |
| Dietary nutrient and food intake (mean ± SD) | ||||
| Total energy, kcal/day | 1753 ± 484 | 1854 ± 482 | 1781 ± 444 | 0.02 |
| Carbohydrate, % energy | 55.3 ± 8.1 | 55.3 ± 7.4 | 53.6 ± 7.8 | 0.03 |
| Fat, % energy | 23.7 ± 5.7 | 24.1 ± 4.8 | 25.1 ± 5.6 | 0.01 |
| Protein, % energy | 13.4 ± 2.6 | 13.9 ± 2.3 | 14.2 ± 2.2 | <0.001 |
| Sodium, mg/1000 kcal | 2300 ± 473 | 2322 ± 436 | 2282 ± 401 | 0.66 |
| Vegetables, g/1000 kcal | 108.5 ± 59.9 | 129.4 ± 69.4 | 138.4 ± 71.7 | <0.001 |
| Fruits, g/1000 kcal | 36.4 ± 44.1 | 48.4 ± 48.7 | 51.5 ± 52.2 | <0.001 |
| Pulses, g/1000 kcal | 24.2 ± 20.1 | 25.4 ± 17.5 | 29.7 ± 19.9 | 0.004 |
| Meats, g/1000 kcal | 39.9 ± 18.2 | 39.4 ± 18.5 | 38.8 ± 16.2 | 0.76 |
| Dairy, g/1000 kcal | 47.9 ± 51.8 | 48.1 ± 43.5 | 62.7 ± 53.0 | 0.002 |
| Soft drinks, g/1000 kcal | 52.1 ± 80.0 | 41.6 ± 51.0 | 32.2 ± 51.5 | 0.003 |
| Rice, g/1000 kcal | 186.3 ± 67.0 | 188.5 ± 60.3 | 172.8 ± 68.0 | 0.03 |
| Bread, g/1000 kcal | 22.5 ± 18.9 | 20.1 ± 15.0 | 22.0 ± 17.9 | 0.25 |
| Noodles, g/1000 kcal | 44.4 ± 31.5 | 43.6 ± 27.4 | 41.4 ± 26.8 | 0.49 |
| Frequency of Whole Grain Intake | |||||||
|---|---|---|---|---|---|---|---|
| Never | Rarely | Sometimes or Always | ptrend1) | ||||
| Participants (n) | 530 | 221 | 193 | ||||
| Cases (n) | 57 | 24 | 8 | ||||
| Adjusted odds ratios (95% CI) | |||||||
| Model 12) | 1.00 | (Reference) | 1.04 | (0.62–1.75) | 0.35 | (0.16–0.77) | 0.02 |
| Model 23) | 1.00 | (Reference) | 1.02 | (0.57–1.83) | 0.36 | (0.16–0.83) | 0.04 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kashino, I.; Eguchi, M.; Miki, T.; Kochi, T.; Nanri, A.; Kabe, I.; Mizoue, T. Prospective Association between Whole Grain Consumption and Hypertension: The Furukawa Nutrition and Health Study. Nutrients 2020, 12, 902. https://doi.org/10.3390/nu12040902
Kashino I, Eguchi M, Miki T, Kochi T, Nanri A, Kabe I, Mizoue T. Prospective Association between Whole Grain Consumption and Hypertension: The Furukawa Nutrition and Health Study. Nutrients. 2020; 12(4):902. https://doi.org/10.3390/nu12040902
Chicago/Turabian StyleKashino, Ikuko, Masafumi Eguchi, Takako Miki, Takeshi Kochi, Akiko Nanri, Isamu Kabe, and Tetsuya Mizoue. 2020. "Prospective Association between Whole Grain Consumption and Hypertension: The Furukawa Nutrition and Health Study" Nutrients 12, no. 4: 902. https://doi.org/10.3390/nu12040902
APA StyleKashino, I., Eguchi, M., Miki, T., Kochi, T., Nanri, A., Kabe, I., & Mizoue, T. (2020). Prospective Association between Whole Grain Consumption and Hypertension: The Furukawa Nutrition and Health Study. Nutrients, 12(4), 902. https://doi.org/10.3390/nu12040902