Bone Metabolism and Vitamin D Implication in Gastroenteropancreatic Neuroendocrine Tumors

 , , and
, , and 
Abstract
1. Introduction
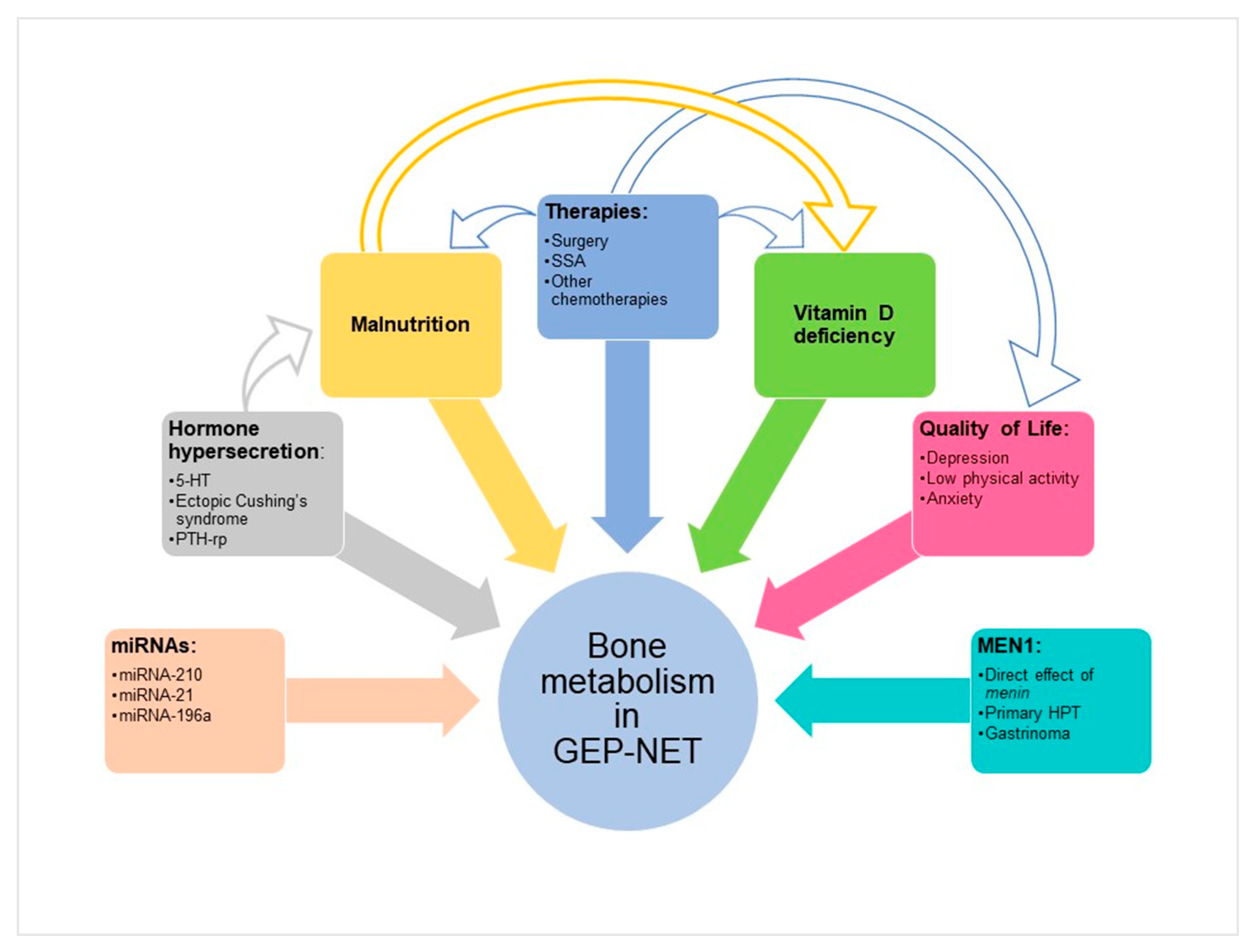
2. Mechanisms of Bone Damage in Functional and Non-Functional GEP–NET
2.1. Hormone Hypersecretion
2.2. MicroRNAs
2.3. Nutritional Status
2.4. Therapies
2.5. Impact of Quality of Life
3. Vitamin D in GEP–NET
4. GEP–NET Associated to MEN1 and Bone Health
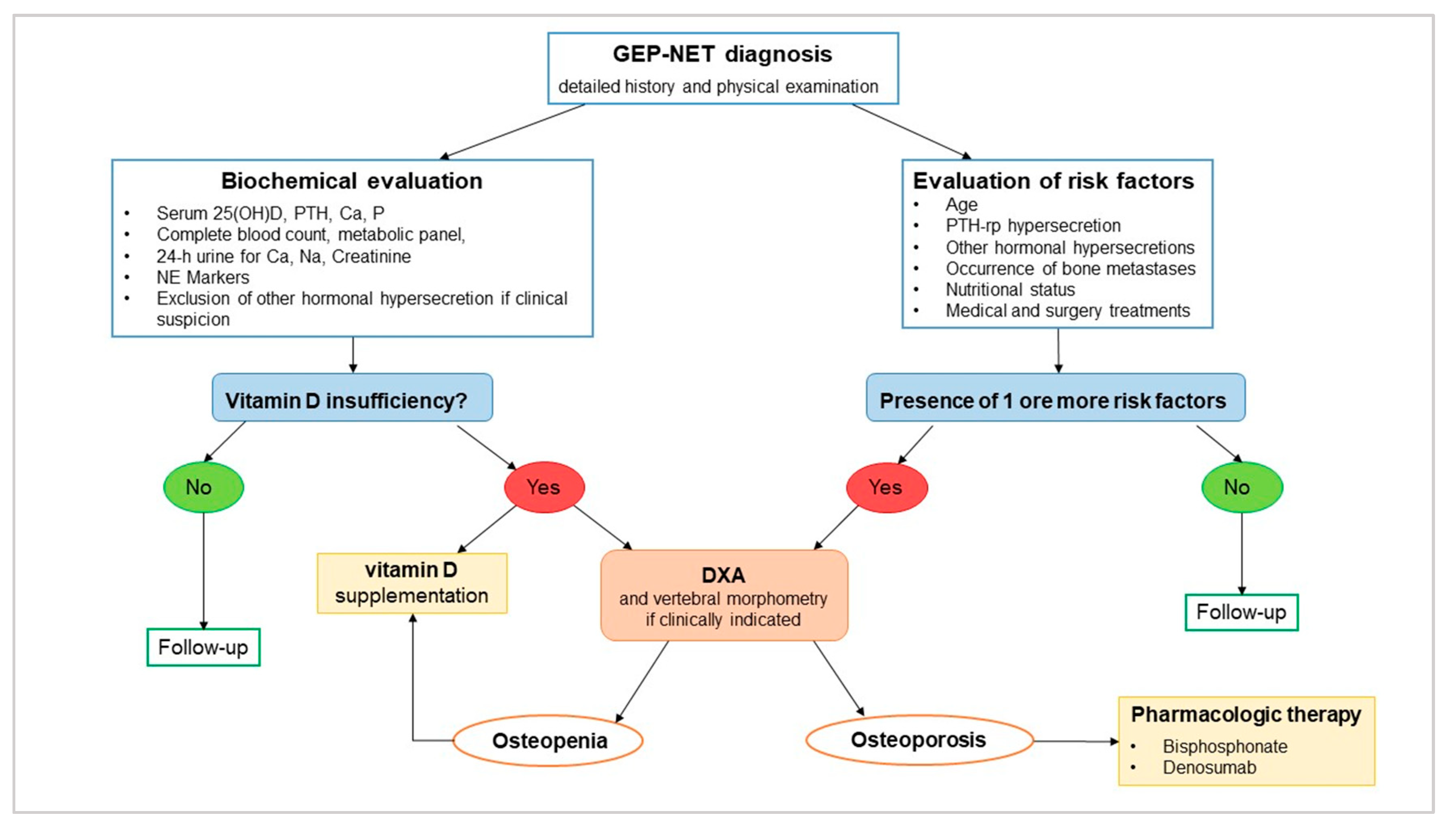
5. Clinical Management of Bone Health and Vitamin D Supplementation in GEP–NET
6. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Datta, H.K.; Ng, W.F.; Walker, J.A.; Tuck, S.P.; Varanasi, S.S. The cell biology of bone metabolism. J. Clin. Pathol. 2008, 61, 577–587. [Google Scholar] [CrossRef] [PubMed]
- Seeman, E.; Delmas, P.D. Bone quality--the material and structural basis of bone strength and fragility. N. Engl. J. Med. 2006, 354, 2250–2261. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Curtis, E.M.; Cooper, C.; Harvey, N.C. State of the art in osteoporosis risk assessment and treatment. J. Endocrinol. Invest. 2019, 42, 1149–1164. [Google Scholar] [CrossRef] [PubMed]
- Ensrud, K.E.; Crandall, C.J. Osteoporosis. Ann. Intern. Med. 2017, 167, ITC17–ITC32. [Google Scholar] [CrossRef]
- Cooper, C.; Cole, Z.A.; Holroyd, C.R.; Earl, S.C.; Harvey, N.C.; Dennison, E.M.; Melton, L.J.; Cummings, S.R.; Kanis, J.A.; Epidemiology, I.C.W.G.o.F. Secular trends in the incidence of hip and other osteoporotic fractures. Osteoporos. Int. 2011, 22, 1277–1288. [Google Scholar] [CrossRef]
- Johansson, L.; Sundh, D.; Nilsson, M.; Mellstrom, D.; Lorentzon, M. Vertebral fractures and their association with health-related quality of life, back pain and physical function in older women. Osteoporos. Int. 2018, 29, 89–99. [Google Scholar] [CrossRef]
- Stubbs, B.; Schofield, P.; Patchay, S. Mobility Limitations and Fall-Related Factors Contribute to the Reduced Health-Related Quality of Life in Older Adults With Chronic Musculoskeletal Pain. Pain Pract. 2016, 16, 80–89. [Google Scholar] [CrossRef]
- Hubscher, M.; Vogt, L.; Schmidt, K.; Fink, M.; Banzer, W. Perceived pain, fear of falling and physical function in women with osteoporosis. Gait Posture 2010, 32, 383–385. [Google Scholar] [CrossRef]
- Coleman, R.; Body, J.J.; Aapro, M.; Hadji, P.; Herrstedt, J.; Group, E.G.W. Bone health in cancer patients: ESMO Clinical Practice Guidelines. Ann. Oncol. 2014, 25, iii124–iii137. [Google Scholar] [CrossRef]
- Faggiano, A.; Ferolla, P.; Grimaldi, F.; Campana, D.; Manzoni, M.; Davi, M.V.; Bianchi, A.; Valcavi, R.; Papini, E.; Giuffrida, D.; et al. Natural history of gastro-entero-pancreatic and thoracic neuroendocrine tumors. Data from a large prospective and retrospective Italian epidemiological study: the NET management study. J. Endocrinol. Invest. 2012, 35, 817–823. [Google Scholar] [CrossRef]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Falconi, M.; Eriksson, B.; Kaltsas, G.; Bartsch, D.K.; Capdevila, J.; Caplin, M.; Kos-Kudla, B.; Kwekkeboom, D.; Rindi, G.; Kloppel, G.; et al. ENETS Consensus Guidelines Update for the Management of Patients with Functional Pancreatic Neuroendocrine Tumors and Non-Functional Pancreatic Neuroendocrine Tumors. Neuroendocrinology 2016, 103, 153–171. [Google Scholar] [CrossRef] [PubMed]
- Altieri, B.; Di Dato, C.; Martini, C.; Sciammarella, C.; Di Sarno, A.; Colao, A.; Faggiano, A.; Group, N. Bone Metastases in Neuroendocrine Neoplasms: From Pathogenesis to Clinical Management. Cancers (Basel) 2019, 11, 1332. [Google Scholar] [CrossRef] [PubMed]
- Riihimaki, M.; Hemminki, A.; Sundquist, K.; Sundquist, J.; Hemminki, K. The epidemiology of metastases in neuroendocrine tumors. Int. J. Cancer 2016, 139, 2679–2686. [Google Scholar] [CrossRef] [PubMed]
- Scharf, M.; Petry, V.; Daniel, H.; Rinke, A.; Gress, T.M. Bone Metastases in Patients with Neuroendocrine Neoplasm: Frequency and Clinical, Therapeutic, and Prognostic Relevance. Neuroendocrinology 2018, 106, 30–37. [Google Scholar] [CrossRef]
- Van Loon, K.; Zhang, L.; Keiser, J.; Carrasco, C.; Glass, K.; Ramirez, M.T.; Bobiak, S.; Nakakura, E.K.; Venook, A.P.; Shah, M.H.; et al. Bone metastases and skeletal-related events from neuroendocrine tumors. Endocr. Connect. 2015, 4, 9–17. [Google Scholar] [CrossRef]
- Giudici, F.; Cavalli, T.; Giusti, F.; Gronchi, G.; Batignani, G.; Tonelli, F.; Brandi, M.L. Natural History of MEN1 GEP-NET: Single-Center Experience After a Long Follow-Up. World J. Surg. 2017, 41, 2312–2323. [Google Scholar] [CrossRef]
- Hess, G.P.; Chen, C.C.; Liu, Z.; Yao, J.C.; Phan, A.T.; Hill, J.W. Clinical burden of illness in patients with neuroendocrine tumors. Pancreas 2012, 41, 1058–1062. [Google Scholar] [CrossRef]
- Altieri, B.; Barrea, L.; Modica, R.; Muscogiuri, G.; Savastano, S.; Colao, A.; Faggiano, A. Nutrition and neuroendocrine tumors: An update of the literature. Rev. Endocr. Metab. Disord. 2018, 19, 159–167. [Google Scholar] [CrossRef]
- Barrea, L.; Altieri, B.; Muscogiuri, G.; Laudisio, D.; Annunziata, G.; Colao, A.; Faggiano, A.; Savastano, S. Impact of Nutritional Status on Gastroenteropancreatic Neuroendocrine Tumors (GEP-NET) Aggressiveness. Nutrients 2018, 10, 1854. [Google Scholar] [CrossRef]
- Lind, A.; Wangberg, B.; Ellegard, L. Vitamin D and vitamin B12 deficiencies are common in patients with midgut carcinoid (SI-NET). Eur. J. Clin. Nutr. 2016, 70, 990–994. [Google Scholar] [CrossRef] [PubMed]
- Massironi, S.; Zilli, A.; Bernasconi, S.; Fanetti, I.; Cavalcoli, F.; Ciafardini, C.; Felicetta, I.; Conte, D. Impact of Vitamin D on the Clinical Outcome of Gastro-Entero-Pancreatic Neuroendocrine Neoplasms: Report on a Series from a Single Institute. Neuroendocrinology 2017, 105, 403–411. [Google Scholar] [CrossRef] [PubMed]
- van Driel, M.; van Leeuwen, J. Vitamin D endocrinology of bone mineralization. Mol. Cell Endocrinol. 2017, 453, 46–51. [Google Scholar] [CrossRef] [PubMed]
- van Dijk, S.C.; de Herder, W.W.; Kwekkeboom, D.J.; Zillikens, M.C.; Feelders, R.A.; van Schaik, R.H.; van Driel, M.; van Leeuwen, J.P. 5-HIAA excretion is not associated with bone metabolism in carcinoid syndrome patients. Bone 2012, 50, 1260–1265. [Google Scholar] [CrossRef]
- Sen Gupta, P.; Grozinsky-Glasberg, S.; Drake, W.M.; Akker, S.A.; Perry, L.; Grossman, A.B.; Druce, M.R. Are serotonin metabolite levels related to bone mineral density in patients with neuroendocrine tumours? Clin. Endocrinol. (Oxf) 2014, 80, 246–252. [Google Scholar] [CrossRef]
- Walsh, J.S.; Newell-Price, J.D.; DeBono, M.; Adaway, J.; Keevil, B.; Eastell, R. Circulating serotonin and bone density, structure, and turnover in carcinoid syndrome. J. Clin. Endocrinol. Metab. 2013, 98, 2902–2907. [Google Scholar] [CrossRef][Green Version]
- Byun, J.; Kim, S.H.; Jeong, H.S.; Rhee, Y.; Lee, W.J.; Kang, C.M. ACTH-producing neuroendocrine tumor of the pancreas: a case report and literature review. Ann. Hepatobiliary Pancreat. Surg. 2017, 21, 61–65. [Google Scholar] [CrossRef]
- Dobnig, H.; Stepan, V.; Leb, G.; Wolf, G.; Buchfelder, M.; Krejs, G.J. Recovery from severe osteoporosis following cure from ectopic ACTH syndrome caused by an appendix carcinoid. J. Intern. Med. 1996, 239, 365–369. [Google Scholar] [CrossRef]
- Motylewska, E.; Gawronska, J.; Niedziela, A.; Melen-Mucha, G.; Lawnicka, H.; Komorowski, J.; Swietoslawski, J.; Stepien, H. Somatostatin Analogs and Tumor Localization Do Not Influence Vitamin D Concentration in Patients with Neuroendocrine Tumors. Nutr. Cancer 2016, 68, 428–434. [Google Scholar] [CrossRef]
- Robbins, H.L.; Symington, M.; Mosterman, B.; Goodby, J.; Davies, L.; Dimitriadis, G.K.; Kaltsas, G.; Randeva, H.S.; Weickert, M.O. Supplementation of Vitamin D Deficiency in Patients with Neuroendocrine Tumors Using Over-the-Counter Vitamin D3 Preparations. Nutr. Cancer 2018, 70, 748–754. [Google Scholar] [CrossRef]
- Lourenco, D.M., Jr.; Coutinho, F.L.; Toledo, R.A.; Montenegro, F.L.; Correia-Deur, J.E.; Toledo, S.P. Early-onset, progressive, frequent, extensive, and severe bone mineral and renal complications in multiple endocrine neoplasia type 1-associated primary hyperparathyroidism. J. Bone Miner. Res. 2010, 25, 2382–2391. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, F.L.; Lourenco, D.M., Jr.; Toledo, R.A.; Montenegro, F.L.; Correia-Deur, J.E.; Toledo, S.P. Bone mineral density analysis in patients with primary hyperparathyroidism associated with multiple endocrine neoplasia type 1 after total parathyroidectomy. Clin. Endocrinol. (Oxf) 2010, 72, 462–468. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.M.; Vodopivec, D.; Christakis, I.; Lyons, G.; Wei, Q.; Waguespack, S.G.; Petak, S.M.; Grubbs, E.; Lee, J.E.; Perrier, N. Operative intervention for primary hyperparathyroidism offers greater bone recovery in patients with sporadic disease than in those with multiple endocrine neoplasia type 1-related hyperparathyroidism. Surgery 2017, 161, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Giusti, F.; Cianferotti, L.; Gronchi, G.; Cioppi, F.; Masi, L.; Faggiano, A.; Colao, A.; Ferolla, P.; Brandi, M.L. Cinacalcet therapy in patients affected by primary hyperparathyroidism associated to Multiple Endocrine Neoplasia Syndrome type 1 (MEN1). Endocrine 2016, 52, 495–506. [Google Scholar] [CrossRef]
- Fanciulli, G.; Ruggeri, R.M.; Grossrubatscher, E.; Calzo, F.L.; Wood, T.D.; Faggiano, A.; Isidori, A.; Colao, A.; Nike. Serotonin pathway in carcinoid syndrome: Clinical, diagnostic, prognostic and therapeutic implications. Rev. Endocr. Metab. Disord. 2020. [Google Scholar] [CrossRef]
- Oleinikov, K.; Avniel-Polak, S.; Gross, D.J.; Grozinsky-Glasberg, S. Carcinoid Syndrome: Updates and Review of Current Therapy. Curr. Treat. Options Oncol. 2019, 20, 70. [Google Scholar] [CrossRef]
- Chabbi-Achengli, Y.; Coudert, A.E.; Callebert, J.; Geoffroy, V.; Cote, F.; Collet, C.; de Vernejoul, M.C. Decreased osteoclastogenesis in serotonin-deficient mice. Proc. Natl. Acad. Sci. USA 2012, 109, 2567–2572. [Google Scholar] [CrossRef]
- Warden, S.J.; Nelson, I.R.; Fuchs, R.K.; Bliziotes, M.M.; Turner, C.H. Serotonin (5-hydroxytryptamine) transporter inhibition causes bone loss in adult mice independently of estrogen deficiency. Menopause 2008, 15, 1176–1183. [Google Scholar] [CrossRef]
- Lavoie, B.; Lian, J.B.; Mawe, G.M. Regulation of Bone Metabolism by Serotonin. Adv. Exp. Med. Biol. 2017, 1033, 35–46. [Google Scholar] [CrossRef]
- Ducy, P.; Karsenty, G. The two faces of serotonin in bone biology. J. Cell Biol. 2010, 191, 7–13. [Google Scholar] [CrossRef]
- Yadav, V.K.; Ryu, J.H.; Suda, N.; Tanaka, K.F.; Gingrich, J.A.; Schutz, G.; Glorieux, F.H.; Chiang, C.Y.; Zajac, J.D.; Insogna, K.L.; et al. Lrp5 controls bone formation by inhibiting serotonin synthesis in the duodenum. Cell 2008, 135, 825–837. [Google Scholar] [CrossRef] [PubMed]
- Kode, A.; Mosialou, I.; Silva, B.C.; Rached, M.T.; Zhou, B.; Wang, J.; Townes, T.M.; Hen, R.; DePinho, R.A.; Guo, X.E.; et al. FOXO1 orchestrates the bone-suppressing function of gut-derived serotonin. J. Clin. Invest. 2012, 122, 3490–3503. [Google Scholar] [CrossRef] [PubMed]
- Kindilien, S.; Goldberg, E.M.; Roberts, M.H.; Gonzales-Pacheco, D. Nutrition status, bone mass density, and selective serotonin reuptake inhibitors. Prev. Med. 2018, 113, 62–67. [Google Scholar] [CrossRef]
- Jensen, R.T.; Cadiot, G.; Brandi, M.L.; de Herder, W.W.; Kaltsas, G.; Komminoth, P.; Scoazec, J.Y.; Salazar, R.; Sauvanet, A.; Kianmanesh, R.; et al. ENETS Consensus Guidelines for the management of patients with digestive neuroendocrine neoplasms: functional pancreatic endocrine tumor syndromes. Neuroendocrinology 2012, 95, 98–119. [Google Scholar] [CrossRef] [PubMed]
- Tauchmanova, L.; Pivonello, R.; Di Somma, C.; Rossi, R.; De Martino, M.C.; Camera, L.; Klain, M.; Salvatore, M.; Lombardi, G.; Colao, A. Bone demineralization and vertebral fractures in endogenous cortisol excess: role of disease etiology and gonadal status. J. Clin. Endocrinol. Metab. 2006, 91, 1779–1784. [Google Scholar] [CrossRef]
- Cipriani, C.; Biamonte, F.; Costa, A.G.; Zhang, C.; Biondi, P.; Diacinti, D.; Pepe, J.; Piemonte, S.; Scillitani, A.; Minisola, S.; et al. Prevalence of kidney stones and vertebral fractures in primary hyperparathyroidism using imaging technology. J. Clin. Endocrinol. Metab. 2015, 100, 1309–1315. [Google Scholar] [CrossRef]
- Dimitriadis, G.K.; Angelousi, A.; Weickert, M.O.; Randeva, H.S.; Kaltsas, G.; Grossman, A. Paraneoplastic endocrine syndromes. Endocr. Relat. Cancer 2017, 24, R173–R190. [Google Scholar] [CrossRef]
- Hardy, R.S.; Zhou, H.; Seibel, M.J.; Cooper, M.S. Glucocorticoids and Bone: Consequences of Endogenous and Exogenous Excess and Replacement Therapy. Endocr. Rev. 2018, 39, 519–548. [Google Scholar] [CrossRef]
- Altieri, B.; Muscogiuri, G.; Paschou, S.A.; Vryonidou, A.; Della Casa, S.; Pontecorvi, A.; Fassnacht, M.; Ronchi, C.L.; Newell-Price, J. Adrenocortical incidentalomas and bone: from molecular insights to clinical perspectives. Endocrine 2018, 62, 506–516. [Google Scholar] [CrossRef]
- Capozzi, A.; Casa, S.D.; Altieri, B.; Pontecorvi, A. Low bone mineral density in a growth hormone deficient (GHD) adolescent. Clin. Cases Miner. Bone Metab. 2013, 10, 203–205. [Google Scholar]
- Compston, J. Glucocorticoid-induced osteoporosis: an update. Endocrine 2018, 61, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Skversky, A.L.; Kumar, J.; Abramowitz, M.K.; Kaskel, F.J.; Melamed, M.L. Association of glucocorticoid use and low 25-hydroxyvitamin D levels: results from the National Health and Nutrition Examination Survey (NHANES): 2001-2006. J. Clin. Endocrinol. Metab 2011, 96, 3838–3845. [Google Scholar] [CrossRef] [PubMed]
- Eller-Vainicher, C.; Falchetti, A.; Gennari, L.; Cairoli, E.; Bertoldo, F.; Vescini, F.; Scillitani, A.; Chiodini, I. DIAGNOSIS OF ENDOCRINE DISEASE: Evaluation of bone fragility in endocrine disorders. Eur. J. Endocrinol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Zatelli, M.C.; Grossrubatscher, E.M.; Guadagno, E.; Sciammarella, C.; Faggiano, A.; Colao, A. Circulating tumor cells and miRNAs as prognostic markers in neuroendocrine neoplasms. Endocr. Relat. Cancer 2017, 24, R223–R237. [Google Scholar] [CrossRef]
- Taipaleenmaki, H. Regulation of Bone Metabolism by microRNAs. Curr. Osteoporos. Rep. 2018, 16, 1–12. [Google Scholar] [CrossRef]
- Sun, M.; Zhou, X.; Chen, L.; Huang, S.; Leung, V.; Wu, N.; Pan, H.; Zhen, W.; Lu, W.; Peng, S. The Regulatory Roles of MicroRNAs in Bone Remodeling and Perspectives as Biomarkers in Osteoporosis. Biomed. Res. Int. 2016, 2016, 1652417. [Google Scholar] [CrossRef]
- Zhao, X.; Xu, D.; Li, Y.; Zhang, J.; Liu, T.; Ji, Y.; Wang, J.; Zhou, G.; Xie, X. MicroRNAs regulate bone metabolism. J. Bone Miner. Metab. 2014, 32, 221–231. [Google Scholar] [CrossRef]
- Liu, X.D.; Cai, F.; Liu, L.; Zhang, Y.; Yang, A.L. MicroRNA-210 is involved in the regulation of postmenopausal osteoporosis through promotion of VEGF expression and osteoblast differentiation. Biol. Chem. 2015, 396, 339–347. [Google Scholar] [CrossRef]
- Thorns, C.; Schurmann, C.; Gebauer, N.; Wallaschofski, H.; Kumpers, C.; Bernard, V.; Feller, A.C.; Keck, T.; Habermann, J.K.; Begum, N.; et al. Global microRNA profiling of pancreatic neuroendocrine neoplasias. Anticancer Res. 2014, 34, 2249–2254. [Google Scholar]
- Roldo, C.; Missiaglia, E.; Hagan, J.P.; Falconi, M.; Capelli, P.; Bersani, S.; Calin, G.A.; Volinia, S.; Liu, C.G.; Scarpa, A.; et al. MicroRNA expression abnormalities in pancreatic endocrine and acinar tumors are associated with distinctive pathologic features and clinical behavior. J. Clin. Oncol 2006, 24, 4677–4684. [Google Scholar] [CrossRef]
- Eguchi, T.; Watanabe, K.; Hara, E.S.; Ono, M.; Kuboki, T.; Calderwood, S.K. OstemiR: a novel panel of microRNA biomarkers in osteoblastic and osteocytic differentiation from mesencymal stem cells. PLoS One 2013, 8, e58796. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Bae, S.W.; Yu, S.S.; Bae, Y.C.; Jung, J.S. miR-196a regulates proliferation and osteogenic differentiation in mesenchymal stem cells derived from human adipose tissue. J. Bone Miner. Res. 2009, 24, 816–825. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.S.; Kim, H.; Kim, H.W.; Lee, J.C.; Paik, K.H.; Kang, J.; Kim, J.; Yoon, Y.S.; Han, H.S.; Sohn, I.; et al. High Expression of MicroRNA-196a Indicates Poor Prognosis in Resected Pancreatic Neuroendocrine Tumor. Medicine (Baltimore) 2015, 94, e2224. [Google Scholar] [CrossRef] [PubMed]
- Maasberg, S.; Knappe-Drzikova, B.; Vonderbeck, D.; Jann, H.; Weylandt, K.H.; Grieser, C.; Pascher, A.; Schefold, J.C.; Pavel, M.; Wiedenmann, B.; et al. Malnutrition Predicts Clinical Outcome in Patients with Neuroendocrine Neoplasia. Neuroendocrinology 2017, 104, 11–25. [Google Scholar] [CrossRef]
- Qureshi, S.A.; Burch, N.; Druce, M.; Hattersley, J.G.; Khan, S.; Gopalakrishnan, K.; Darby, C.; Wong, J.L.; Davies, L.; Fletcher, S.; et al. Screening for malnutrition in patients with gastro-entero-pancreatic neuroendocrine tumours: a cross-sectional study. BMJ Open 2016, 6, e010765. [Google Scholar] [CrossRef]
- Borre, M.; Dam, G.A.; Knudsen, A.W.; Gronbaek, H. Nutritional status and nutritional risk in patients with neuroendocrine tumors. Scand. J. Gastroenterol. 2018, 53, 284–292. [Google Scholar] [CrossRef]
- Gallo, M.; Muscogiuri, G.; Pizza, G.; Ruggeri, R.M.; Barrea, L.; Faggiano, A.; Colao, A.; Group, N. The management of neuroendocrine tumours: A nutritional viewpoint. Crit. Rev. Food Sci. Nutr. 2019, 59, 1046–1057. [Google Scholar] [CrossRef]
- Faggiano, A.; Modica, R.; Lo Calzo, F.; Camera, L.; Napolitano, V.; Altieri, B.; de Cicco, F.; Bottiglieri, F.; Sesti, F.; Badalamenti, G.; et al. Lanreotide Therapy vs Active Surveillance in MEN1-Related Pancreatic Neuroendocrine Tumors <2 Centimeters. J. Clin. Endocrinol. Metab. 2020, 105. [Google Scholar] [CrossRef]
- Cives, M.; Strosberg, J.R. Gastroenteropancreatic Neuroendocrine Tumors. CA Cancer J. Clin. 2018, 68, 471–487. [Google Scholar] [CrossRef]
- Clement, D.S.; Tesselaar, M.E.; van Leerdam, M.E.; Srirajaskanthan, R.; Ramage, J.K. Nutritional and vitamin status in patients with neuroendocrine neoplasms. World J. Gastroenterol. 2019, 25, 1171–1184. [Google Scholar] [CrossRef]
- Faggiano, A.; Lo Calzo, F.; Pizza, G.; Modica, R.; Colao, A. The safety of available treatments options for neuroendocrine tumors. Expert Opin. Drug Saf. 2017, 16, 1149–1161. [Google Scholar] [CrossRef] [PubMed]
- Faggiano, A.; Di Maio, S.; Mocerino, C.; Ottaviano, M.; De Divitiis, C.; Guarnotta, V.; Dolce, P.; Modica, R.; Puliafito, I.; Tozzi, L.; et al. Therapeutic sequences in patients with grade 1-2 neuroendocrine tumors (NET): an observational multicenter study from the ELIOS group. Endocrine 2019, 66, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Kneissel, M.; Luong-Nguyen, N.H.; Baptist, M.; Cortesi, R.; Zumstein-Mecker, S.; Kossida, S.; O’Reilly, T.; Lane, H.; Susa, M. Everolimus suppresses cancellous bone loss, bone resorption, and cathepsin K expression by osteoclasts. Bone 2004, 35, 1144–1156. [Google Scholar] [CrossRef]
- Browne, A.J.; Kubasch, M.L.; Gobel, A.; Hadji, P.; Chen, D.; Rauner, M.; Stolzel, F.; Hofbauer, L.C.; Rachner, T.D. Concurrent antitumor and bone-protective effects of everolimus in osteotropic breast cancer. Breast Cancer Res. 2017, 19, 92. [Google Scholar] [CrossRef] [PubMed]
- Fusco, V.; Porta, C.; Saia, G.; Paglino, C.; Bettini, G.; Scoletta, M.; Bonacina, R.; Vescovi, P.; Merigo, E.; Lo Re, G.; et al. Osteonecrosis of the Jaw in Patients With Metastatic Renal Cell Cancer Treated With Bisphosphonates and Targeted Agents: Results of an Italian Multicenter Study and Review of the Literature. Clin. Genitourin Cancer 2015, 13, 287–294. [Google Scholar] [CrossRef]
- Escudier, B.; Powles, T.; Motzer, R.J.; Olencki, T.; Aren Frontera, O.; Oudard, S.; Rolland, F.; Tomczak, P.; Castellano, D.; Appleman, L.J.; et al. Cabozantinib, a New Standard of Care for Patients With Advanced Renal Cell Carcinoma and Bone Metastases? Subgroup Analysis of the METEOR Trial. J. Clin. Oncol. 2018, 36, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Carbonero, R.; Rinke, A.; Valle, J.W.; Fazio, N.; Caplin, M.; Gorbounova, V.; J, O.C.; Eriksson, B.; Sorbye, H.; Kulke, M.; et al. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Neoplasms. Systemic Therapy 2: Chemotherapy. Neuroendocrinology 2017, 105, 281–294. [Google Scholar] [CrossRef]
- Pavel, M.; Gross, D.J.; Benavent, M.; Perros, P.; Srirajaskanthan, R.; Warner, R.R.P.; Kulke, M.H.; Anthony, L.B.; Kunz, P.L.; Horsch, D.; et al. Telotristat ethyl in carcinoid syndrome: safety and efficacy in the TELECAST phase 3 trial. Endocr. Relat. Cancer 2018, 25, 309–322. [Google Scholar] [CrossRef]
- Cella, D.; Beaumont, J.L.; Hudgens, S.; Marteau, F.; Feuilly, M.; Houchard, A.; Lapuerta, P.; Ramage, J.; Pavel, M.; Horsch, D.; et al. Relationship Between Symptoms and Health-related Quality-of-life Benefits in Patients With Carcinoid Syndrome: Post Hoc Analyses From TELESTAR. Clin. Ther. 2018, 40, 2006–2020 e2002. [Google Scholar] [CrossRef]
- Karppinen, N.; Linden, R.; Sintonen, H.; Tarkkanen, M.; Roine, R.; Heiskanen, I.; Matikainen, N.; Schalin-Jantti, C. Health-Related Quality of Life in Patients with Small Intestine Neuroendocrine Tumors. Neuroendocrinology 2018, 107, 366–374. [Google Scholar] [CrossRef]
- Lewis, A.R.; Wang, X.; Magdalani, L.; D’Arienzo, P.; Bashir, C.; Mansoor, W.; Hubner, R.; Valle, J.W.; McNamara, M.G. Health-related quality of life, anxiety, depression and impulsivity in patients with advanced gastroenteropancreatic neuroendocrine tumours. World J. Gastroenterol. 2018, 24, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Pearman, T.P.; Beaumont, J.L.; Cella, D.; Neary, M.P.; Yao, J. Health-related quality of life in patients with neuroendocrine tumors: an investigation of treatment type, disease status, and symptom burden. Support. Care Cancer 2016, 24, 3695–3703. [Google Scholar] [CrossRef] [PubMed]
- Weng, S.F.; Hsu, H.R.; Weng, Y.L.; Tien, K.J.; Kao, H.Y. Health-Related Quality of Life and Medical Resource Use in Patients with Osteoporosis and Depression: A Cross-Sectional Analysis from the National Health and Nutrition Examination Survey. Int. J. Environ. Res. Public Health 2020, 17, 1124. [Google Scholar] [CrossRef] [PubMed]
- Troy, K.L.; Mancuso, M.E.; Butler, T.A.; Johnson, J.E. Exercise Early and Often: Effects of Physical Activity and Exercise on Women’s Bone Health. Int. J. Environ. Res. Public Health 2018, 15, 878. [Google Scholar] [CrossRef]
- Catalano, A.; Martino, G.; Bellone, F.; Gaudio, A.; Lasco, C.; Langher, V.; Lasco, A.; Morabito, N. Anxiety levels predict fracture risk in postmenopausal women assessed for osteoporosis. Menopause 2018, 25, 1110–1115. [Google Scholar] [CrossRef]
- DeLuca, H.F. Evolution of our understanding of vitamin D. Nutr. Rev. 2008, 66, S73–S87. [Google Scholar] [CrossRef]
- Bikle, D.D. Extraskeletal actions of vitamin D. Ann. NY Acad. Sci. 2016, 1376, 29–52. [Google Scholar] [CrossRef]
- Chiang, K.C.; Chen, T.C. The anti-cancer actions of vitamin D. Anticancer Agents Med. Chem. 2013, 13, 126–139. [Google Scholar] [CrossRef]
- Souberbielle, J.C.; Body, J.J.; Lappe, J.M.; Plebani, M.; Shoenfeld, Y.; Wang, T.J.; Bischoff-Ferrari, H.A.; Cavalier, E.; Ebeling, P.R.; Fardellone, P.; et al. Vitamin D and musculoskeletal health, cardiovascular disease, autoimmunity and cancer: Recommendations for clinical practice. Autoimmun. Rev. 2010, 9, 709–715. [Google Scholar] [CrossRef]
- Tirabassi, G.; Salvio, G.; Altieri, B.; Ronchi, C.L.; Della Casa, S.; Pontecorvi, A.; Balercia, G. Adrenal disorders: Is there Any role for vitamin D? Rev. Endocr. Metab. Disord. 2017, 18, 355–362. [Google Scholar] [CrossRef]
- Holick, M.F. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am. J. Clin. Nutr. 2004, 80, 1678S–1688S. [Google Scholar] [CrossRef] [PubMed]
- Altieri, B.; Grant, W.B.; Della Casa, S.; Orio, F.; Pontecorvi, A.; Colao, A.; Sarno, G.; Muscogiuri, G. Vitamin D and pancreas: The role of sunshine vitamin in the pathogenesis of diabetes mellitus and pancreatic cancer. Crit. Rev. Food Sci. Nutr. 2017, 57, 3472–3488. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G.; Altieri, B.; Annweiler, C.; Balercia, G.; Pal, H.B.; Boucher, B.J.; Cannell, J.J.; Foresta, C.; Grubler, M.R.; Kotsa, K.; et al. Vitamin D and chronic diseases: the current state of the art. Arch. Toxicol. 2017, 91, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Altieri, B.; Muscogiuri, G.; Barrea, L.; Mathieu, C.; Vallone, C.V.; Mascitelli, L.; Bizzaro, G.; Altieri, V.M.; Tirabassi, G.; Balercia, G.; et al. Does vitamin D play a role in autoimmune endocrine disorders? A proof of concept. Rev. Endocr. Metab. Disord. 2017, 18, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G.; Barrea, L.; Altieri, B.; Di Somma, C.; Bhattoa, H.P.; Laudisio, D.; Duval, G.T.; Pugliese, G.; Annweiler, C.; Orio, F.; et al. Calcium and Vitamin D Supplementation. Myths and Realities with Regard to Cardiovascular Risk. Curr. Vasc. Pharmacol. 2019, 17, 610–617. [Google Scholar] [CrossRef]
- Sarno, G.; Nappi, R.; Altieri, B.; Tirabassi, G.; Muscogiuri, E.; Salvio, G.; Paschou, S.A.; Ferrara, A.; Russo, E.; Vicedomini, D.; et al. Current evidence on vitamin D deficiency and kidney transplant: What’s new? Rev. Endocr. Metab. Disord. 2017, 18, 323–334. [Google Scholar] [CrossRef]
- Feldman, D.; Krishnan, A.V.; Swami, S.; Giovannucci, E.; Feldman, B.J. The role of vitamin D in reducing cancer risk and progression. Nat. Rev. Cancer 2014, 14, 342–357. [Google Scholar] [CrossRef]
- Karkeni, E.; Morin, S.O.; Bou Tayeh, B.; Goubard, A.; Josselin, E.; Castellano, R.; Fauriat, C.; Guittard, G.; Olive, D.; Nunes, J.A. Vitamin D Controls Tumor Growth and CD8+ T Cell Infiltration in Breast Cancer. Front. Immunol. 2019, 10, 1307. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Altieri, B.; Penna-Martinez, M.; Badenhoop, K. Focus on vitamin D and the adrenal gland. Horm. Metab. Res. 2015, 47, 239–246. [Google Scholar] [CrossRef]
- Vuolo, L.; Di Somma, C.; Faggiano, A.; Colao, A. Vitamin D and cancer. Front. Endocrinol. (Lausanne) 2012, 3, 58. [Google Scholar] [CrossRef]
- Wasiewicz, T.; Piotrowska, A.; Wierzbicka, J.; Slominski, A.T.; Zmijewski, M.A. Antiproliferative Activity of Non-Calcemic Vitamin D Analogs on Human Melanoma Lines in Relation to VDR and PDIA3 Receptors. Int. J. Mol. Sci. 2018, 19, 2583. [Google Scholar] [CrossRef] [PubMed]
- Kotlarz, A.; Przybyszewska, M.; Swoboda, P.; Miloszewska, J.; Grygorowicz, M.A.; Kutner, A.; Markowicz, S. Differential interference of vitamin D analogs PRI-1906, PRI-2191, and PRI-2205 with the renewal of human colon cancer cells refractory to treatment with 5-fluorouracil. Tumour Biol. 2016, 37, 4699–4709. [Google Scholar] [CrossRef]
- Chiang, K.C.; Yeh, C.N.; Pang, J.H.; Hsu, J.T.; Yeh, T.S.; Chen, L.W.; Kuo, S.F.; Hsieh, P.J.; Pan, Y.C.; Takano, M.; et al. 1alpha,25(OH)2D3 Analog, MART-10, Inhibits Neuroendocrine Tumor Cell Growth Through Induction of G0/G1 Cell-cycle Arrest and Apoptosis. Anticancer Res. 2016, 36, 3307–3313. [Google Scholar] [PubMed]
- Chiang, K.C.; Yeh, C.N.; Pang, J.S.; Hsu, J.T.; Yeh, T.S.; Chen, L.W.; Kuo, S.F.; Takano, M.; Chen, T.C.; Kittaka, A.; et al. 1alpha,25(OH)2D3 Analog, MART-10, Inhibits Neuroendocrine Tumor Cell Metastasis After VEGF-A Stimulation. Anticancer Res. 2017, 37, 6215–6221. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine, S. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Schramm, S.; Lahner, H.; Jockel, K.H.; Erbel, R.; Fuhrer, D.; Moebus, S.; Heinz Nixdorf Recall Study, G. Impact of season and different vitamin D thresholds on prevalence of vitamin D deficiency in epidemiological cohorts-a note of caution. Endocrine 2017, 56, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Altieri, B.; Cavalier, E.; Bhattoa, H.P.; Perez-Lopez, F.R.; Lopez-Baena, M.T.; Perez-Roncero, G.R.; Chedraui, P.; Annweiler, C.; Della Casa, S.; Zelzer, S.; et al. Vitamin D testing: advantages and limits of the current assays. Eur. J. Clin. Nutr. 2020, 74, 231–247. [Google Scholar] [CrossRef]
- Manson, J.E.; Cook, N.R.; Lee, I.M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Gordon, D.; Copeland, T.; D’Agostino, D.; et al. Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease. N. Engl. J. Med. 2019, 380, 33–44. [Google Scholar] [CrossRef]
- Zhang, Y.; Fang, F.; Tang, J.; Jia, L.; Feng, Y.; Xu, P.; Faramand, A. Association between vitamin D supplementation and mortality: systematic review and meta-analysis. BMJ 2019, 366, l4673. [Google Scholar] [CrossRef]
- Thakker, R.V.; Newey, P.J.; Walls, G.V.; Bilezikian, J.; Dralle, H.; Ebeling, P.R.; Melmed, S.; Sakurai, A.; Tonelli, F.; Brandi, M.L.; et al. Clinical practice guidelines for multiple endocrine neoplasia type 1 (MEN1). J. Clin. Endocrinol. Metab. 2012, 97, 2990–3011. [Google Scholar] [CrossRef]
- Giusti, F.; Cianferotti, L.; Boaretto, F.; Cetani, F.; Cioppi, F.; Colao, A.; Davi, M.V.; Faggiano, A.; Fanciulli, G.; Ferolla, P.; et al. Multiple endocrine neoplasia syndrome type 1: institution, management, and data analysis of a nationwide multicenter patient database. Endocrine 2017, 58, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Norton, J.A.; Krampitz, G.; Jensen, R.T. Multiple Endocrine Neoplasia: Genetics and Clinical Management. Surg. Oncol. Clin. N. Am. 2015, 24, 795–832. [Google Scholar] [CrossRef] [PubMed]
- Dreijerink, K.M.; Varier, R.A.; van Nuland, R.; Broekhuizen, R.; Valk, G.D.; van der Wal, J.E.; Lips, C.J.; Kummer, J.A.; Timmers, H.T. Regulation of vitamin D receptor function in MEN1-related parathyroid adenomas. Mol. Cell Endocrinol. 2009, 313, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kaji, H. Menin and bone metabolism. J. Bone Miner. Metab. 2012, 30, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Igarashi, H.; Uehara, H.; Berna, M.J.; Jensen, R.T. Causes of death and prognostic factors in multiple endocrine neoplasia type 1: a prospective study: comparison of 106 MEN1/Zollinger-Ellison syndrome patients with 1613 literature MEN1 patients with or without pancreatic endocrine tumors. Medicine (Baltimore) 2013, 92, 135–181. [Google Scholar] [CrossRef]
- Lamas, C.; Navarro, E.; Casteras, A.; Portillo, P.; Alcazar, V.; Calatayud, M.; Alvarez-Escola, C.; Sastre, J.; Boix, E.; Forga, L.; et al. MEN1-associated primary hyperparathyroidism in the Spanish Registry: clinical characterictics and surgical outcomes. Endocr. Connect. 2019, 8, 1416–1424. [Google Scholar] [CrossRef]
- Twigt, B.A.; Scholten, A.; Valk, G.D.; Rinkes, I.H.; Vriens, M.R. Differences between sporadic and MEN related primary hyperparathyroidism; clinical expression, preoperative workup, operative strategy and follow-up. Orphanet J. Rare Dis. 2013, 8, 50. [Google Scholar] [CrossRef]
- Manoharan, J.; Albers, M.B.; Bollmann, C.; Maurer, E.; Mintziras, I.; Wachter, S.; Bartsch, D.K. Single gland excision for MEN1-associated primary hyperparathyroidism. Clin. Endocrinol. (Oxf) 2020, 92, 63–70. [Google Scholar] [CrossRef]
- Norton, J.A.; Venzon, D.J.; Berna, M.J.; Alexander, H.R.; Fraker, D.L.; Libutti, S.K.; Marx, S.J.; Gibril, F.; Jensen, R.T. Prospective study of surgery for primary hyperparathyroidism (HPT) in multiple endocrine neoplasia-type 1 and Zollinger-Ellison syndrome: long-term outcome of a more virulent form of HPT. Ann. Surg. 2008, 247, 501–510. [Google Scholar] [CrossRef]
- Lourenco, D.M., Jr.; Coutinho, F.L.; Toledo, R.A.; Goncalves, T.D.; Montenegro, F.L.; Toledo, S.P. Biochemical, bone and renal patterns in hyperparathyroidism associated with multiple endocrine neoplasia type 1. Clinics (Sao Paulo) 2012, 67, 99–108. [Google Scholar] [CrossRef]
- Liu, J.; Li, X.; Fan, L.; Yang, J.; Wang, J.; Sun, J.; Wang, Z. Proton pump inhibitors therapy and risk of bone diseases: An update meta-analysis. Life Sci. 2019, 218, 213–223. [Google Scholar] [CrossRef] [PubMed]
- Andersen, B.N.; Johansen, P.B.; Abrahamsen, B. Proton pump inhibitors and osteoporosis. Curr. Opin. Rheumatol. 2016, 28, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Camacho, P.M.; Petak, S.M.; Binkley, N.; Clarke, B.L.; Harris, S.T.; Hurley, D.L.; Kleerekoper, M.; Lewiecki, E.M.; Miller, P.D.; Narula, H.S.; et al. American Association of Clinical Endocrinologists and American College of Endocrinology Clinical Practice Guidelines for the Diagnosis and Treatment of Postmenopausal Osteoporosis - 2016. Endocr. Pract. 2016, 22, 1–42. [Google Scholar] [CrossRef] [PubMed]
- Lentle, B.; Koromani, F.; Brown, J.P.; Oei, L.; Ward, L.; Goltzman, D.; Rivadeneira, F.; Leslie, W.D.; Probyn, L.; Prior, J.; et al. The Radiology of Osteoporotic Vertebral Fractures Revisited. J. Bone Miner. Res. 2019, 34, 409–418. [Google Scholar] [CrossRef]
- Keum, N.; Lee, D.H.; Greenwood, D.C.; Manson, J.E.; Giovannucci, E. Vitamin D supplementation and total cancer incidence and mortality: a meta-analysis of randomized controlled trials. Ann. Oncol. 2019, 30, 733–743. [Google Scholar] [CrossRef]
- Giustina, A.; Adler, R.A.; Binkley, N.; Bollerslev, J.; Bouillon, R.; Dawson-Hughes, B.; Ebeling, P.R.; Feldman, D.; Formenti, A.M.; Lazaretti-Castro, M.; et al. Consensus statement from 2(nd) International Conference on Controversies in Vitamin D. Rev. Endocr. Metab. Disord. 2020. [Google Scholar] [CrossRef]
- Kanis, J.A.; Cooper, C.; Rizzoli, R.; Reginster, J.Y.; Scientific Advisory Board of the European Society for Clinical and Economic Aspects of Osteoporosis (ESCEO) and the Committees of Scientific Advisors and National Societies of the International Osteoporosis Foundation (IOF). European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos. Int. 2019, 30, 3–44. [Google Scholar] [CrossRef]
- Kanis, J.A.; Harvey, N.C.; McCloskey, E.; Bruyere, O.; Veronese, N.; Lorentzon, M.; Cooper, C.; Rizzoli, R.; Adib, G.; Al-Daghri, N.; et al. Algorithm for the management of patients at low, high and very high risk of osteoporotic fractures. Osteoporos. Int. 2020, 31, 1–12. [Google Scholar] [CrossRef]
- Nuti, R.; Brandi, M.L.; Checchia, G.; Di Munno, O.; Dominguez, L.; Falaschi, P.; Fiore, C.E.; Iolascon, G.; Maggi, S.; Michieli, R.; et al. Guidelines for the management of osteoporosis and fragility fractures. Intern. Emerg. Med. 2019, 14, 85–102. [Google Scholar] [CrossRef]
- Jiménez-Fonseca, P.; Carmona-Bayonas, A.; Martín-Pérez, E.; Crespo, G.; Serrano, R.; Llanos, M.; Villabona, C.; García-Carbonero, R.; Aller, J.; Capdevila, J.; et al. Health-related Quality of Life in Well-Differentiated Metastatic Gastroenteropancreatic Neuroendocrine Tumors. Cancer Metastasis. Rev. 2015, 34, 381–400. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year and Reference | Type of Study | Number of Patients | Principal Aim | Principal Findings Associated with Bone Metabolism or Vitamin D |
|---|---|---|---|---|
| Hess et al. 2012 [18] | Retrospective case-control. | 1762 NET and 3524 controls (1:2 ratio). | Comorbidities in NET. | Adjusted risk of osteoporosis/osteopenia was higher in NET patients among those 50 years or younger. |
| Van Dijk et al. 2012 [24] | Retrospective. | 84 carcinoid patients: 61 with increased 5-HT levels and 23 with low 5-HT levels (controls). | Differences in markers of bone metabolism between the two groups. | No significant differences in markers of bone metabolism between hyper-secretors and controls. |
| Sen Gupta et al. 2014 [25] | Observational. | 46 consecutive NET. | Relationships between urinary 5-HIAA and BMD measured by DXA | 41.3% had osteoporosis and 32.6% osteopenia. Urinary 5-HIAA was not an independent predictor for BMD. |
| Walsh et al. 2013 [26] | Cross-sectional. | 25 patients with carcinoid syndrome and 25 healthy controls. | Association of carcinoid syndrome with bone formation markers, BMD and bone structure. | No measures of bone density or bone structure differed significantly between cases and controls. |
| Byun et al. 2017 [27] | Case report. | Case of pNET producing ACTH. | Descriptive. | 40-year-old female patient with ophthalmologic discomfort, osteoporosis, and hypokalemia with diagnosis of pNET. |
| Dobnig et al. 1996 [28] | Case report. | Case of appendix carcinoid producing ACTH- | Descriptive. | 34-year-old female patient with multiple spontaneous rip fractures and T-score at lumbar spine -4.3 SD. Increasing of BMD after tumor resection. |
| Lind et al. 2016 [21] | Intervention. | 50 consecutive SI-NET (25 controls and 25 supplemented with vitamin D, B12 and calcium). | DXA and gastrointestinal disorders. | Control group: 46% vitamin D deficiency and 76% low BMD. Supplemented group: 28% vitamin D deficiency and 60% low BMD. Vitamin D supplementation avoid severe deficiency. |
| Massironi et al. 2017 [22] | Observational. | 138 GEP–NET. | Impact of vitamin D and OS and PFS. | 68% cases had vitamin D deficiency. Patients treated with SSA had lower vitamin D levels. At multivariate analysis, vitamin D levels significantly correlate with OS. |
| Motylewska et al. 2016 [29] | Observational. | 36 NET and 16 healthy controls. | Evaluation of vitamin D levels between the two groups. | No significant difference in vitamin D levels between NET and controls. SSA therapy did not aggravate vitamin D deficiency. |
| Robbins et al. 2018 [30] | Longitudinal, intervention. | 183 GEP-NET. | Effect of vitamin D treatment after 2 year of follow-up. | Vitamin D insufficiency decreased from 66.6% at baseline to 44.9% and 46.2% after 12 and 24 months, respectively. Previous abdominal surgery predicted vitamin D levels. |
| Lourenco et al. 2010 [31] | Cross-sectional. | 36 MEN1 patients with HPT. | Outcome of bone and renal complications. | Patients with long-standing HPT (>10 years) and gastrinoma/HPT presented significantly lower 1/3DR BMD values. |
| Coutinho et al. 2010 [32] | Case series. | 16 HPT/MEN1. | Impact of total PTx on BMD in patients with HPT/MEN1. | BMD improvement in the lumbar spine, femoral neck, and total femur after 15 months from PTx. |
| Silva et al. 2017 [33] | Retrospective. | 14 HPT/MEN1 and 104 sporadic HPT. | Impact of total PTx on BMD in patients with HPT/MEN1 vs sporadic HPT. | At baseline, HPT/MEN1 had significantly lower Z-score at lumbar spine, total hip, and femoral neck than sporadic HPT. 1 year after PTx, HPT/MEN1 showed a better Z-score only at lumbar spine compare to baseline. |
| Giusti et al. 2016 [34] | Longitudinal, intervention. | 33 MEN1. | Effect of cinacalcet on HPT. | No significant changes in BMD, and bone turnover markers after 1 year of treatment |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Altieri, B.; Di Dato, C.; Modica, R.; Bottiglieri, F.; Di Sarno, A.; Pittaway, J.F.H.; Martini, C.; Faggiano, A.; Colao, A., on behalf of NIKE group. Bone Metabolism and Vitamin D Implication in Gastroenteropancreatic Neuroendocrine Tumors. Nutrients 2020, 12, 1021. https://doi.org/10.3390/nu12041021
Altieri B, Di Dato C, Modica R, Bottiglieri F, Di Sarno A, Pittaway JFH, Martini C, Faggiano A, Colao A on behalf of NIKE group. Bone Metabolism and Vitamin D Implication in Gastroenteropancreatic Neuroendocrine Tumors. Nutrients. 2020; 12(4):1021. https://doi.org/10.3390/nu12041021
Chicago/Turabian StyleAltieri, Barbara, Carla Di Dato, Roberta Modica, Filomena Bottiglieri, Antonella Di Sarno, James F.H. Pittaway, Chiara Martini, Antongiulio Faggiano, and Annamaria Colao on behalf of NIKE group. 2020. "Bone Metabolism and Vitamin D Implication in Gastroenteropancreatic Neuroendocrine Tumors" Nutrients 12, no. 4: 1021. https://doi.org/10.3390/nu12041021
APA StyleAltieri, B., Di Dato, C., Modica, R., Bottiglieri, F., Di Sarno, A., Pittaway, J. F. H., Martini, C., Faggiano, A., & Colao, A., on behalf of NIKE group. (2020). Bone Metabolism and Vitamin D Implication in Gastroenteropancreatic Neuroendocrine Tumors. Nutrients, 12(4), 1021. https://doi.org/10.3390/nu12041021