Food Sources and Nutrient Intakes of Filipino Working Adults


Abstract
1. Background
2. Methodology
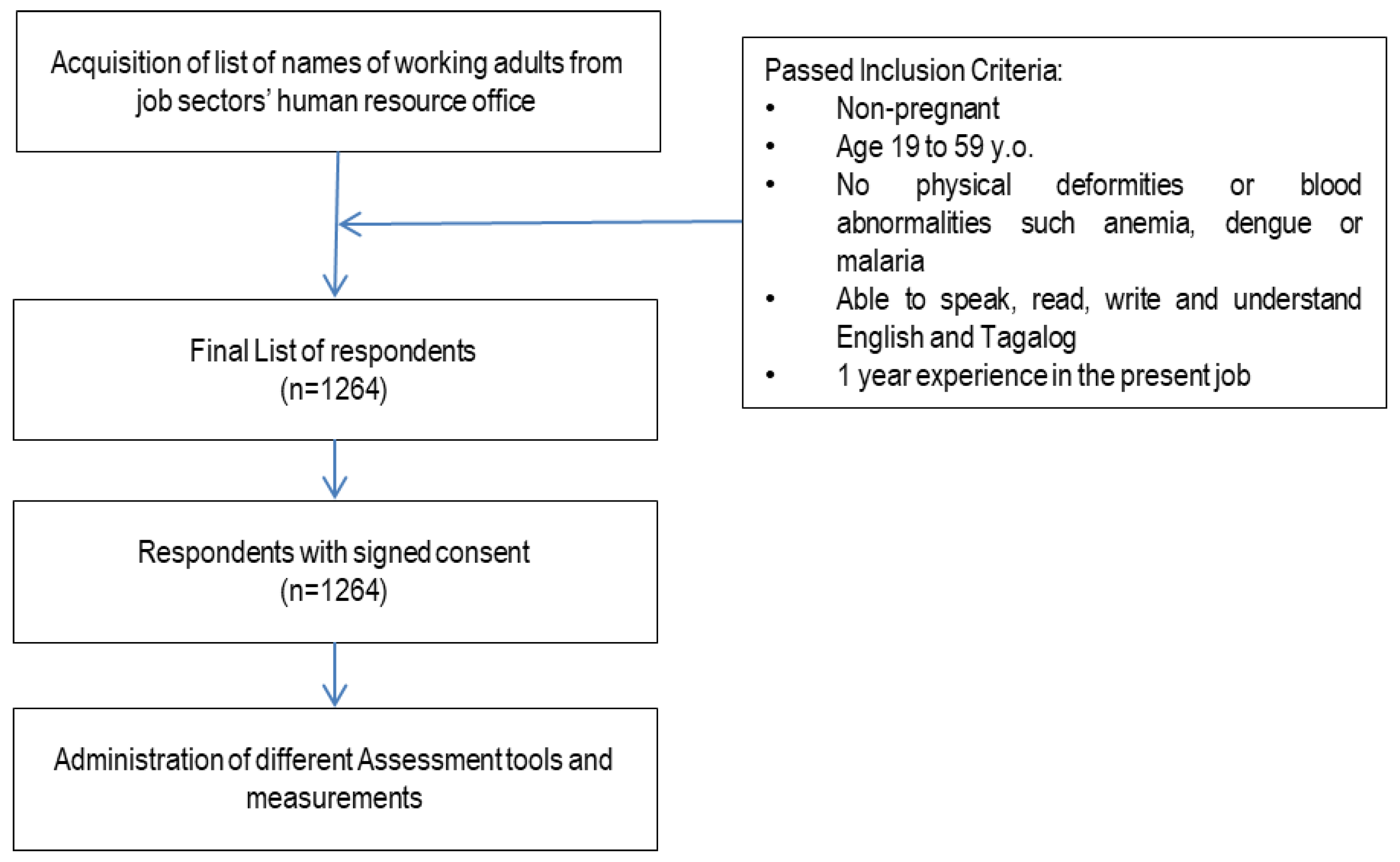
2.1. Study Design and Population
2.2. Anthropometric Measurements
2.3. Statistical Analysis for the Usual Energy Intake
2.4. Dietary Assessment
2.5. Physical Activity
- Three or more days of vigorous-intensity activity for at least 20 min per day;
- Five or more days of moderate-intensity activity;
- Walking for at least 30 min per day.
2.6. Ethical Considerations
3. Results
3.1. Socio-Economic, Demographic, and Anthropometric Characteristics of the Study Population
3.2. Energy Intake
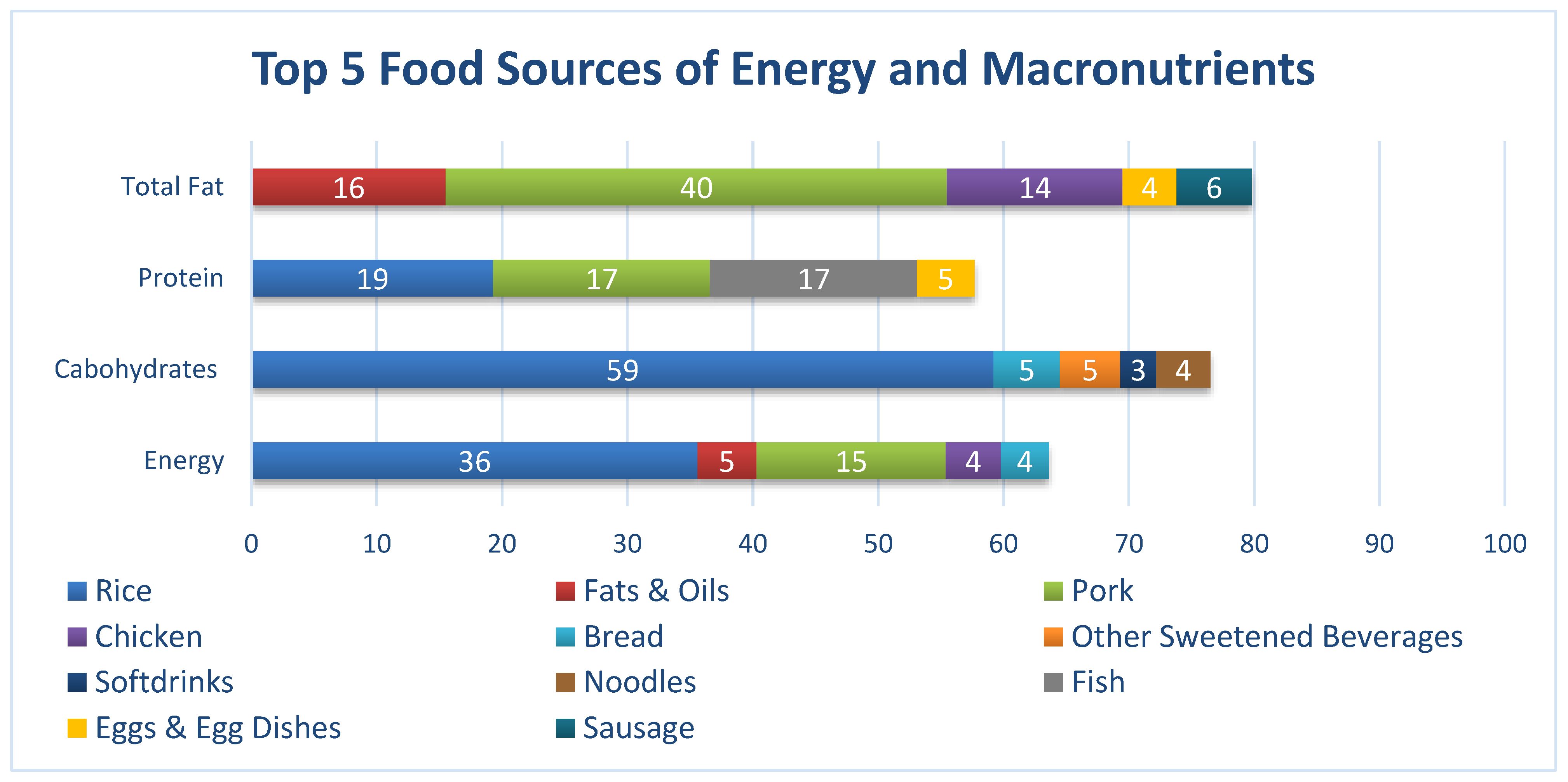
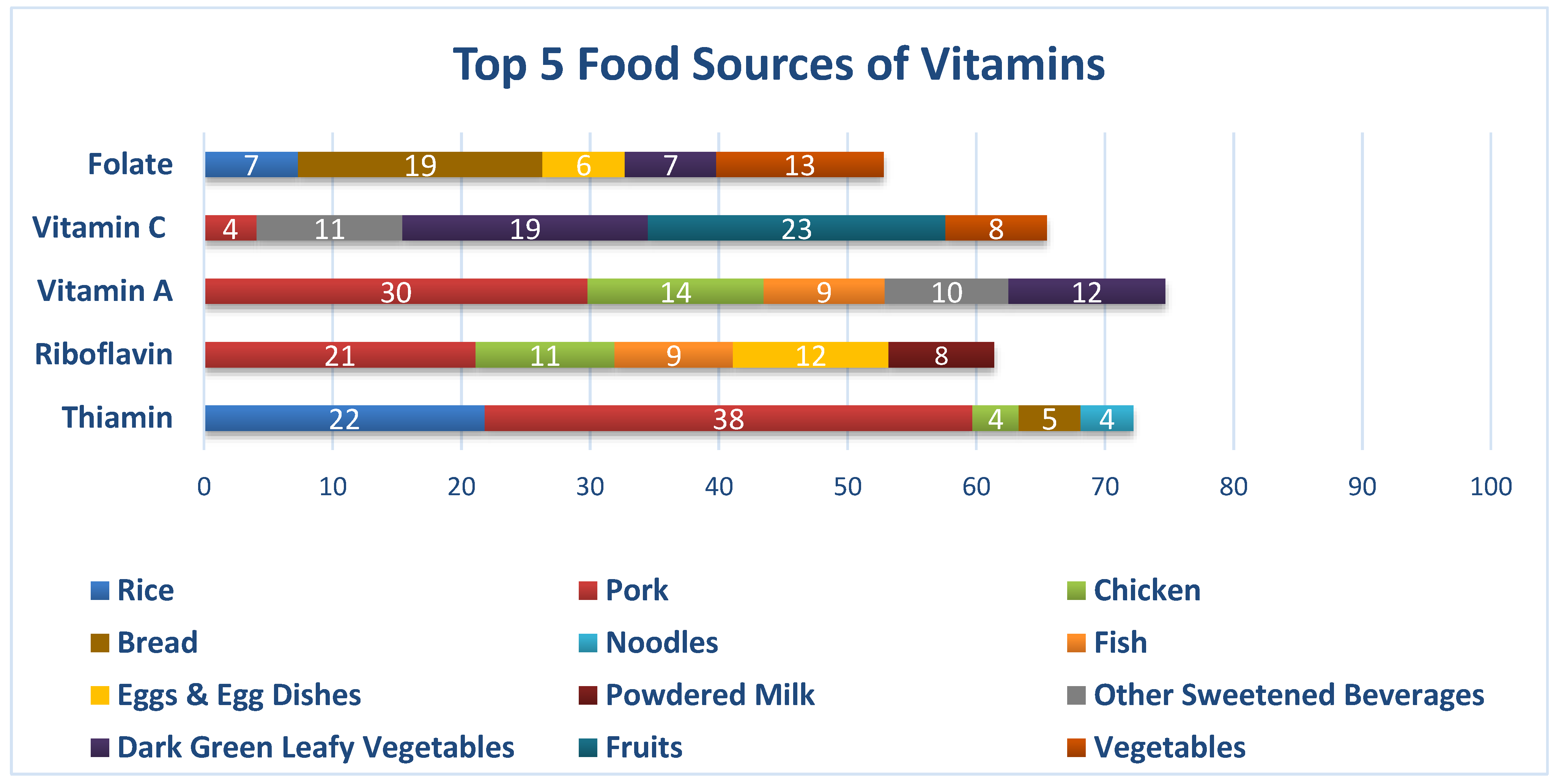
3.3. Nutrient Intake
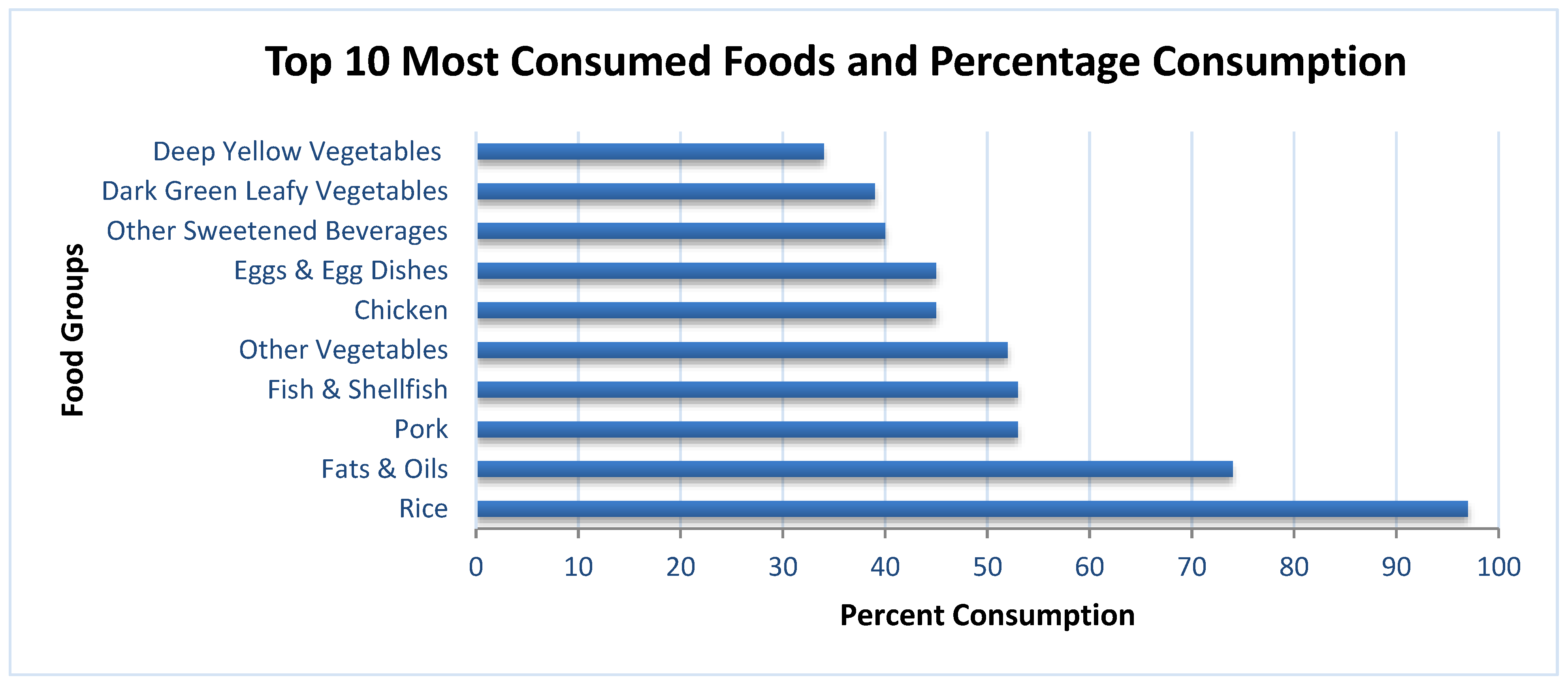
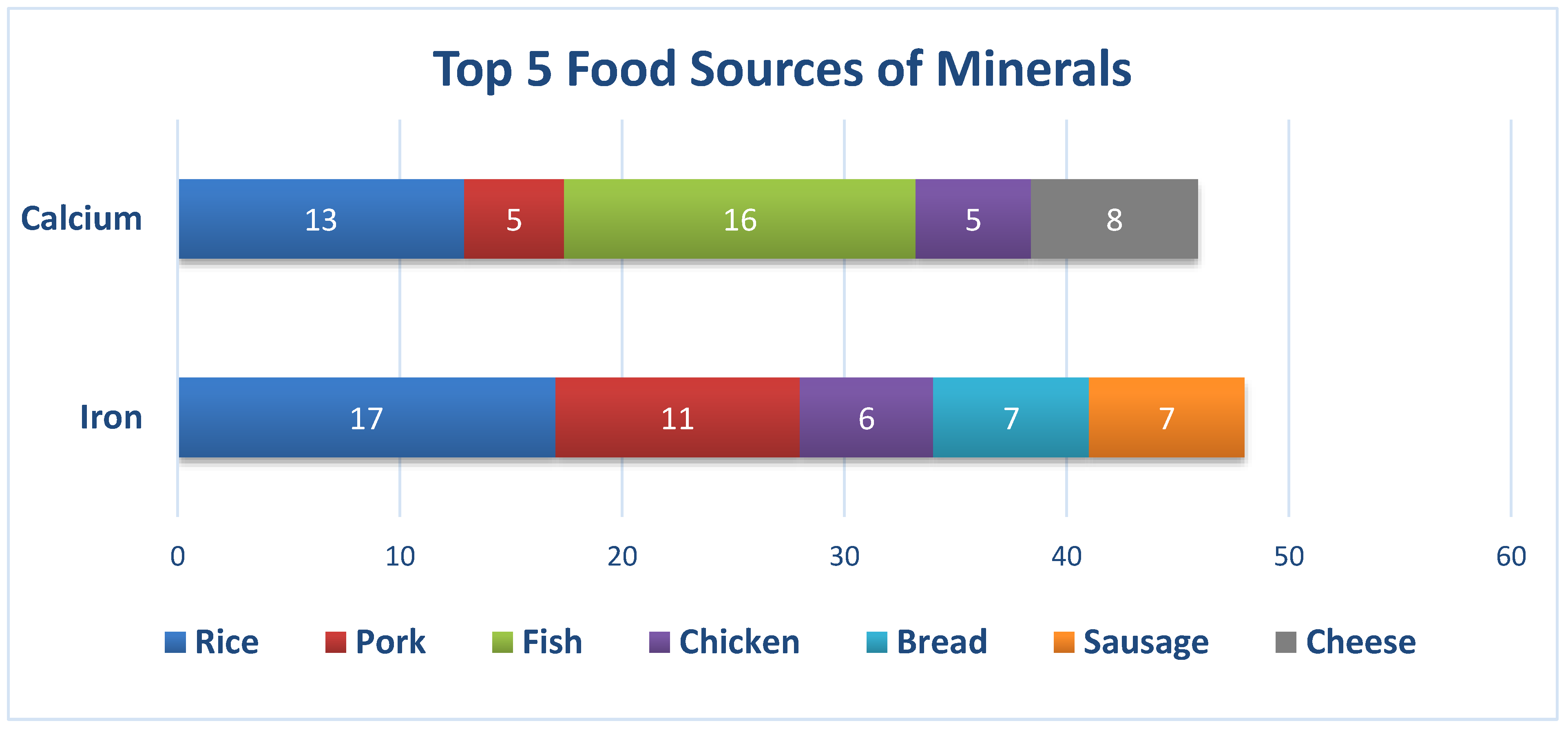
3.4. Food Intake
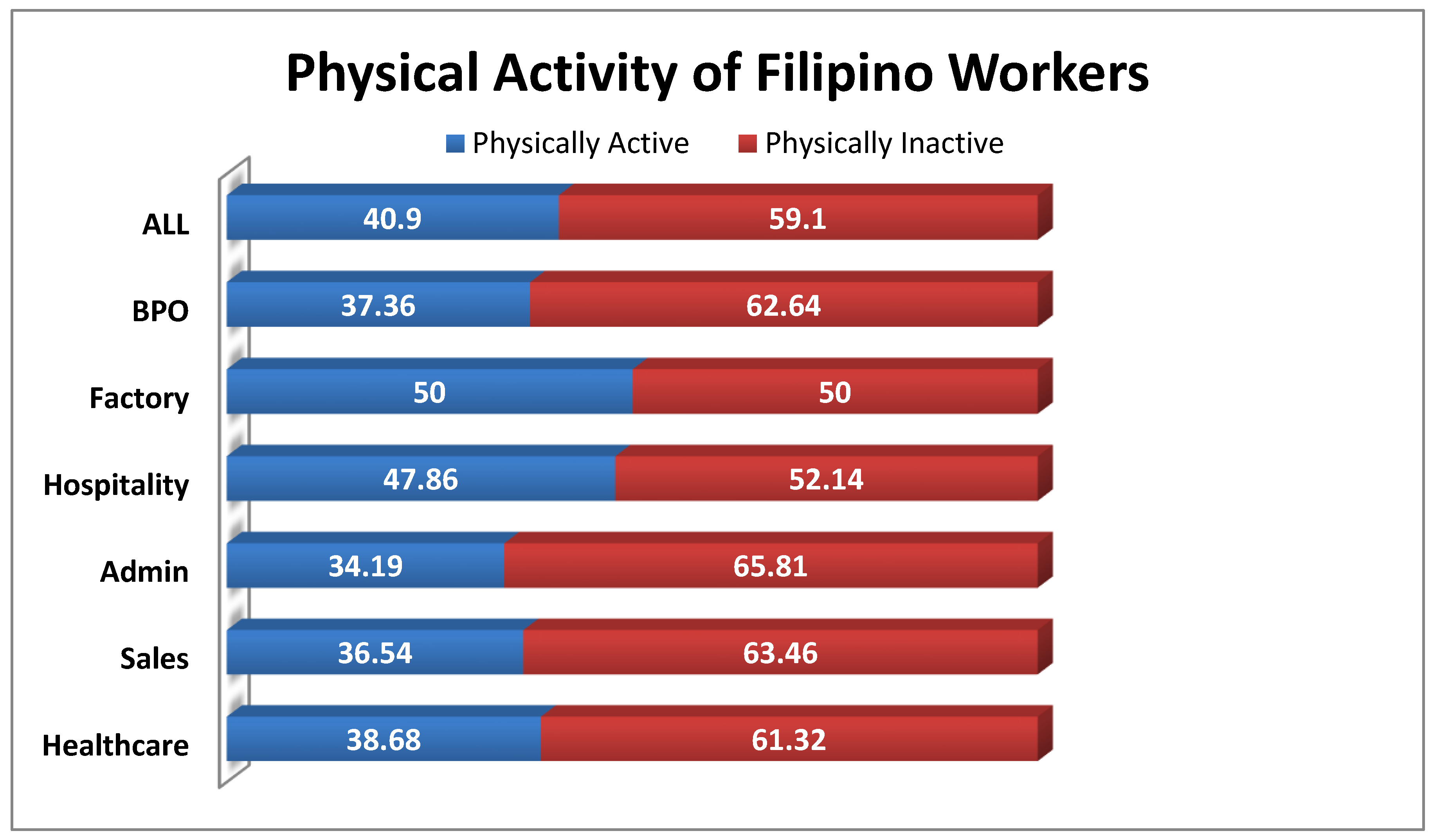
3.5. Physical Activity
3.6. Medical History
4. Discussion
4.1. Inadequate Energy and Nutrient Intake
4.2. Physical Activity and Inactivity
4.3. Limitations of the Study
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| WHO | World Health Organization |
| EAR | Estimated Adequate Requirement |
| AMDR | Acceptable Macronutrient Distribution Ranges |
| EER | Estimated Energy Requirements |
| GDP | Gross Domestic Product |
| LMIC | Low-Middle Income Countries |
| NCD | Non-Communicable Diseases |
| COPD | Chronic Obstructive Pulmonary Disease |
| FCT | Food Composition Table |
| BPO | Business Process Outsourcing |
| BMI | Body Mass Index |
| IOM | Institute of Medicine |
| PAL | Physical Activity Level |
| AI | Adequate Intake |
| RNI | Recommended Nutrient Intakes |
| FNRI | Food and Nutrition Research Institute |
| CIOMS | Council for International Organizations of Medical Sciences |
| FIERC | FNRI Institutional Ethics Review Committee |
| ICF | Informed Consent Form |
| BMR | Basal Metabolic Rate |
| LDL | Low Density Lipoprotein |
| CVD | Cardiovascular Disease |
| CHD | Coronary Heart Disease |
References
- World Health Organization. Constitution of the World Health Organization. WHO is South-East Asia. 1947. Available online: http://www.searo.who.int/about/constitution/en/ (accessed on 14 September 2019).
- Shearer, J.; Graham, T.E.; Skinner, T.L. Nutra-ergonomics: Influence of nutrition on physical employment standards and the health of workers. Appl. Physiol. Nutr. Metab. 2016, 41, S165–S174. [Google Scholar] [CrossRef] [PubMed]
- World Bank Group. The World Bank and Nutrition. 1 April 2019. Available online: https://www.worldbank.org/en/topic/nutrition/overview (accessed on 14 September 2019).
- GDB 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2015, 388, 1659–1724. [Google Scholar]
- Bloom, D.; Cafiero, E.; Abrahams-Gessel, S.; Bloom, L.R.; Fathima, S.; Feigl, A.B. The Global Economic Burden of Non-communicable Diseases; World Economic Forum: Geneva, Switzerland, 2011. [Google Scholar]
- Goettler, A.; Grosse, A.; Sonntag, D. Productivity loss due to overweight and obesity: A systematic review of indirect costs. BMJ Open 2015, 7. [Google Scholar] [CrossRef] [PubMed]
- Lehnert, T.; Sonntag, D.; Konnopka, A.; Riedel-Heller, S.; Konig, H.-H. Economic costs of overweight and obesity. Best Pract. Res. Clin. Endocrinol. Metab. 2013, 27, 105–115. [Google Scholar] [CrossRef]
- Ross, J.; Horton, S. Economic Consequences of Iron Deficiency; The Micronutrient Initiative: Ottawa, ON, Canada, 1998. [Google Scholar]
- Institute for Health Metrics and Evaluation. Global Burden of Disease; University of Washington: Seattle, WA, USA, 2017. [Google Scholar]
- Agdeppa, I.A.; Perlas, L.A.; Capanzana, M.V. Vitamin D status of Filipino Adults: Evidence from the 8th National Nutrition Survey 2013. Malays. J. Nutr. 2018, 24, 395–406. [Google Scholar]
- Food and Nutrition Research Institute. 8th National Nutrition Survey Overview: Health and Nutritional Status of Filipino Adults, 20–59 Years Old; Department of Science and Technology—Food and Nutrition Research Institute: Taguig, Philippines, 2018.
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Lancet Physical Activity Series Working Group. Impact of Physical Inactivity on the World’s Major NonCommunicable Diseases. Natl. Inst. Health Public Access 2012, 380, 219–229. [Google Scholar]
- Piano, M.R.; Burke, L.; Kang, M.; Phillips, S.A. Effects of Repeated Binge Drinking on Blood Pressure Levels and Other Cardiovascular Health Metrics in Young Adults: National Health and Nutrition Examination Survey, 2011–2014. J. Am. Heart Assoc. 2018, 7, e008733. [Google Scholar] [CrossRef]
- International Labor Office. Poor Workplace Nutrition Hits Workers’ Health and Productivity, Says New ILO Report; International Labour Office: Geneva, Switzerland, 2005. [Google Scholar]
- Kant, A.K. Dietary Patterns and Health Outcomes. J. Am. Diet. Assoc. 2004, 104, 615–635. [Google Scholar] [CrossRef]
- Philippine Statistics Authority. Labor Force. July 2019. Philippine Statistics Authority: Labor and Employment. Available online: https://psa.gov.ph/tags/labor-force (accessed on 12 September 2019).
- FAO. Proceedings of Discussions on Food Composition; Food Policy and Nutrition Division Report; FAO: Rome, Italy, 1994. [Google Scholar]
- Philippine Statistics Authority. 2012 Census of Philippine Business and Industry—Economy-Wide for All Establishments; Census of Philippine Business and Industry: Quezon City, Philippines, 2015.
- López-Olmedo, N.; Carriquiry, A.L.; Rodríguez-Ramírez, S.; Ramírez-Silva, I.; Espinosa-Montero, J.; Hernández-Barrera, L.; Campirano, F.; Martínez-Tapia, B.; Rivera, J.A. Usual Intake of Added Sugars and Saturated Fats Is High while Dietary Fiber Is Low in the Mexican Population. J. Nutr. 2016, 146, 1856S–1865S. [Google Scholar] [CrossRef]
- Carriquiry, A.L. Assessing the prevalence of nutrient inadequacy. Public Health Nutr. 2007, 2, 22–34. [Google Scholar] [CrossRef]
- Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids; National Academies Press: Washington, DC, USA, 2000. [Google Scholar]
- Angeles-Agdeppa, I.; Sun, Y.; Denney, L.; Tanda, K.V.; Octavio, R.A.D.; Carriquiry, A.; Capanzana, M.V. Food sources, energy and nutrient intakes of adults: 2013 Philippines National Nutrition Survey. Nutr. J. 2019, 18, 59. [Google Scholar] [CrossRef] [PubMed]
- Siega-Riz, A.; Deming, D.; Reidy, K.; Fox, M.; Condon, E.; Briefel, R. Food Consumption Patterns of infants and toddlers: Where are we now? J. Am. Diet. Assoc. 2010, 110, S38–S51. [Google Scholar] [CrossRef] [PubMed]
- National Economic and Development Authority. About Ambisyon Natin 2014. AmbiyonNatin2040. Available online: http://2040.neda.gov.ph/wp-content/uploads/2016/04/A-Long-Term-Vision-for-the-Philippines.pdf (accessed on 5 November 2019).
- Xu, S.; Xue, Y. Protein intake and obesity in young adolescents. Exp. Ther. Med. 2016, 11, 1545–1549. [Google Scholar] [CrossRef] [PubMed]
- University of Eastern Finland. Dietary proteins and protein sources and risk of death: The Kuopio Ischaemic Heart Disease Risk Factor Study. Am. J. Clin. Nutr. 2019, 109, 1462–1471. [Google Scholar] [CrossRef]
- DiNicolantonio, J.J.; Lucan, S.C.; O’Keefe, J.H. The Evidence for Saturated Fat and for Sugar Related to Coronary Heart Disease. Prog. Cardiovasc. Dis. 2016, 58, 464–472. [Google Scholar] [CrossRef]
- Siri-Tarino, P.W.; Krauss, R.M. Diet, Lipids and Cardiovascular disease. Curr. Opin. Lipidol. 2016, 27, 323–328. [Google Scholar] [CrossRef]
- Vessby, B. Dietary fat, fatty acid composition in plasma and the metabolic syndrome. Curr. Opin. Lipidol. 2003, 14, 15–19. [Google Scholar] [CrossRef]
- Shan, Z.; Rehm, C.D.; Rogers, G. Trends in Dietary Carbohydrate, Protein, and Fat Intake and Diet Quality among US Adults, 1999–2016. JAMA 2019, 322, 1178–1187. [Google Scholar] [CrossRef]
- Woodward-Lopez, G.; Kao, J.; Ritchie, L. To what extent have sweetened beverages contributed to the obesity epidemic? Public Health Nutr. 2010, 14, 499–509. [Google Scholar] [CrossRef]
- The Nielsen Company. What’s Next after Sugar Tax; Nielsen Company: New York, NY, USA, 2018. [Google Scholar]
- Kant, A.K.; Schatzkin, A. Consumption of Energy-Dense, Nutrient-Poor Foods by the US Population: Effect on Nutrient Profiles. J. Am. Coll. Nutr. 1994, 13, 285–291. [Google Scholar] [CrossRef]
- McNaughton, S.A.; Mishra, G.D.; Brunner, E.J. Food patterns associated with blood lipids are predictive of coronary heart disease: The Whitehall II study. Br. J. Nutr. 2009, 102, 619–624. [Google Scholar] [CrossRef]
- Pedro, M.; Benavides, R.; Barba, C. Dietary changes and their health implications in the Philippines. Philipp. J. Sci. 2006, 146, 20–23. [Google Scholar]
- Stein, A.; Qaim, M. The human and economic cost of hidden hunger. Food Nutr. Bull. 2007, 28, 125–134. [Google Scholar] [CrossRef]
- Diaz, J.; de las Cagigas, A.; Rodriguez, R. Micronutrient deficiencies in developing and affluent countries. Eur. J. Clin. Nutr. 2003, 57, S70–S72. [Google Scholar] [CrossRef]
- PLoS Medicine Editors. Poor Diet in Shift Workers: A New Occupational Health. PLoS Med. Open Access 2011, 8, e1001152. [Google Scholar]
- Lukaski, H. Vitamin and mineral status: Effects on physical performance. Nutrition 2004, 20, 632–644. [Google Scholar] [CrossRef]
- Charoenbut, P.; Klaewkla, J.; Srisorrachatr, S.; Arphorn, S.; Wijitwanna, S. Workplace and individual factors influence eating. Malays. J. Nutr. 2018, 24, 417–426. [Google Scholar]
- World Health Organization. Physical Activity. 23 February 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 17 January 2020).
- Thorp, A.A.; Owen, N.; Neuhaus, M.; Dunstan, D.W. Sedentary Behaviors and Subsequent Health Outcomes in Adults: A systematic review of longitudinal studies. Am. J. Prev. Med. 2011, 41, 207–215. [Google Scholar] [CrossRef]
- Harvey, J.A.; Chastin, S.M.; Skelton, D.A. Prevalence of Sedentary Behavior in Older Adults: A Systematic Review. Int. J. Environ. Res. Public Health 2013, 10, 6645–6661. [Google Scholar] [CrossRef]
- Genin, P.M.; Dessenne, P.; Finaud, J.; Pereira, B.; Dutheil, F.; Thivel, D.; Duclos, M. Effect of Work-Related Sedentary Time on Overall Health Profile in Active vs. Inactive Office Workers. Front. Public Health 2018, 6, 279. [Google Scholar] [CrossRef]
- Jalayondeja, C.; Jalayondeja, W.; Mekhora, K.; Bhuanantanondh, P.; Dusadi-Isariyavong, A.; Upiriyasakul, R. Break in Sedentary Behavior Reduces the Risk of Noncommunicable Diseases and Cardiometabolic Risk Factors among Workers in a Petroleum Company. Int. J. Environ. Res. Public Health 2017, 5, 501. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Work Sector | Type of Work | Mean Age (y) | Calculated Sample Size |
|---|---|---|---|
| BPO 1 | Call Center Agents | 31 | 174 (14%) |
| Factory | Automotive, Industrial Plants | 35 | 312 (25%) |
| Hospitality and Foods | Hotel staff, Food Service workers, Waiters, Cooks | 32 | 140 (11%) |
| Administration | Office Work | 33 | 272 (21%) |
| Sales | Sales Agent and Associates (Real estate, Malls etc.) | 30 | 260 (21%) |
| Healthcare | Nurses, Hospital Staff | 32 | 106 (8%) |
| Total sample (n) | 1264 | ||
| Socio-Economic, Demographic Characteristics and Nutritional Status | |||
|---|---|---|---|
| n | % | ||
| Gender | Male | 631 | 49.9 |
| Female | 633 | 50.1 | |
| Civil Status | Single | 754 | 59.6 |
| Married | 469 | 37.1 | |
| Separated/Widowed | 41 | 3.24 | |
| Educational Status | No education | 2 | 0.2 |
| Elementary graduate | 75 | 5.9 | |
| High school graduate | 390 | 30.8 | |
| Vocational/College graduate | 797 | 63 | |
| Job Sector | BPO 1 | 174 | 13.8 |
| Factory | 312 | 24.7 | |
| Hospitality | 140 | 11.1 | |
| Admin | 272 | 21.5 | |
| Sales | 260 | 20.6 | |
| Healthcare | 106 | 8.4 | |
| Household Monthly Income | Less than Php25,000 | 404 | 32 |
| Php25,000-Php75,000 | 443 | 35 | |
| Php75,001- Php150,000 | 136 | 10.8 | |
| More than Php150,000 | 89 | 7 | |
| Don’t know/Decline to respond | 192 | 15.3 | |
| Sources of Funds (multiple answer) | Salary/Wages | 1264 | 100 |
| Selling goods/services | 244 | 19.3 | |
| Money Lending/Others | 40 | 3.2 | |
| Tenure in Work | Less than a year | 395 | 31.2 |
| 1 to 5 years | 516 | 40.8 | |
| 5 years or more | 353 | 27.9 | |
| Nutritional Status and Physical Measurements | |||
| Nutritional Status | Underweight | 50 | 4 |
| Normal | 618 | 48.9 | |
| Overweight | 391 | 30.9 | |
| Obese | 205 | 15.8 | |
| Physical Measurements (Mean ± SD) | Body Weight (kg) | 65.1 | 15.2 |
| Height (cm) | 159.8 | 8.6 | |
| BMI (kg/m2) | 25.4 | 4.7 | |
| Mean Intake ± SE | |||||||
|---|---|---|---|---|---|---|---|
| Nutrients | All (n = 1264) | BPO (n = 174) | Factory (n = 312) | Hospitality (n = 140) | Admin (n = 272) | Sales (n = 260) | Healthcare (n = 106) |
| Energy(kcal/d) | 1768.8 ± 13 | 1761.3 ± 31 | 1715.3 ± 25.3 | 1990.5 ± 48.8 | 1806.9 ± 31.7 | 1745.3 ± 28 | 1610.6 ± 38.6 |
| EER G (kcal) | 2401.5 ± 12 | 2474.4 ± 37 | 2440.8 ± 21.3 | 2444.7 ± 36.5 | 2333.3 ± 26.4 | 2382.4 ± 27 | 2335.2 ± 45.3 |
| Macronutrients | |||||||
| Total fat (g/d) | 56.56 ± 0.5 | 61.6 ± 1.3 | 47.2 ± 0.9 | 65.1 ± 2 | 58.6 ± 1.1 | 58.7 ± 1.0 | 57 ± 1.4 |
| Saturated fat (g/d) | 26.73 ± 0.3 | 29.8 ± 0.7 | 23.3 ± 0.6 | 29.6 ± 0.8 | 26.9 ± 0.7 | 27 ± 0.6 | 26.5 ± 0.5 |
| MUFA (g/d) | 21.20 ± 0.2 | 23.9 ± 0.6 | 16.9 ± 0.4 | 24.7 ± 0.7 | 22.1 ± 0.5 | 22.2 ± 0.5 | 20.1 ± 0.5 |
| 9.45 ± 0.1 | 10.2 ± 0.3 | 7.9 ± 0.2 | 10.7 ± 0.4 | 10.2 ± 0.2 | 9.8 ± 0.2 | 8.9 ± 0.3 | |
| PUFA (g/d) | |||||||
| Carbohydrate (g/d) | 238.47 ± 2 | 216.3 ± 4.1 | 251.4 ± 4 | 268.5 ± 7.5 | 245.1 ± 4.7 | 229.5 ± 4.1 | 203.4 ± 5.7 |
| Total sugars (g/d) | 31.13 ± 0.5 | 33.4 ± 1.2 | 27.6 ± 0.8 | 34.4 ± 1.5 | 33.4 ± 1 | 29.3 ± 1.2 | 32.6 ± 1.4 |
| Dietary fiber (g/d) | 7.97 ± 0.07 | 7.5 ± 0.2 | 8 ± 0.1 | 8.4 ± 0.2 | 8.6 ± 0.2 | 7.8 ± 0.2 | 7.2 ± 0.3 |
| Protein (g/d) | 67.14 ± 0.5 | 67.9 ± 1.5 | 64.6 ± 1.1 | 76.6 ± 1.6 | 66.1 ± 1.2 | 67.2 ± 1.2 | 63.7 ± 1.6 |
| As percentage of Total Energy | |||||||
| Total fat (%) | 27.75 ± 0.2 | 30.1 ± 0.5 | 23.6 ± 0.3 | 28.2 ± 0.5 | 28.6 ± 0.3 | 28.9 ± 0.3 | 30.5 ± 0.4 |
| Protein (%) | 15.5 ± 0.05 | 15.6 ± 0.08 | 15.3 ± 0.1 | 15.9 ± 0.2 | 15 ± 0.09 | 15.6 ± 0.1 | 16.5 ± 0.2 |
| Carbohydrate (%) | 55.27 ± 0.2 | 51.9 ± 0.5 | 59.8 ± 0.4 | 54.7 ± 0.6 | 55 ± 0.3 | 54.1 ± 0.4 | 51.6 ± 0.6 |
| Antioxidants | |||||||
| Vitamin C (mg/d) | 33.24 ± 0.6 | 34 ± 1.4 | 30.1 ± 0.9 | 29.1 ± 1.4 | 35.7 ± 1.3 | 36 ± 2 | 36.9 ± 2.6 |
| Vitamin E (mgα-TE) | 4.42 ± 0.04 | 4.6 ± 0.07 | 4.1 ± 0.06 | 4.7 ± 0.1 | 4.6 ± 0.08 | 4.3 ± 0.1 | 4.6 ± 0.2 |
| B vitamins | |||||||
| Thiamin (mg/d) | 0.77 ± 7.4 | 0.8 ± 0.01 | 0.7 ± 0.01 | 0.9 ± 0.02 | 0.8 ± 0.02 | 0.8 ± 0.02 | 0.7 ± 0.02 |
| Riboflavin (mg/d) | 0.61 ± 5.8 | 0.6 ± 0.01 | 0.6 ± 0.01 | 0.7 ± 0.02 | 0.6 ± 0.01 | 0.6 ± 0.01 | 0.6 ± 0.02 |
| Niacin (mg/d) | 21.01 ± 0.2 | 21.2 ± 0.5 | 21.2 ± 0.3 | 24 ± 0.5 | 20.1 ± 0.4 | 20.7 ± 0.4 | 19.6 ± 0.5 |
| Vitamin B6 (mg/d) | 2.42 ± 0.03 | 2.4 ± 0.06 | 2.3 ± 0.05 | 2.5 ± 0.05 | 2.4 ± 0.07 | 2.7 ± 0.09 | 2.1 ± 0.07 |
| Vitamin B12 (µg/d) | 4.41 ± 0.06 | 4.1 ± 0.2 | 4.7 ± 0.1 | 4.9 ± 0.2 | 4 ± 0.1 | 4.4 ± 0.1 | 5.1 ± 0.3 |
| Folate (µg DFE E) | 179.58 ± 1.7 | 176 ± 5.1 | 187.3 ± 3.3 | 164.6 ± 4.9 | 184.3 ± 2.9 | 180 ± 3.6 | 170.8 ± 6.5 |
| Bone-related nutrients | |||||||
| Calcium (mg/d) | 354.85 ± 3.7 | 339.3 ± 5.6 | 348.8 ± 7.8 | 399.4 ± 14.4 | 371 ± 8.5 | 334.4 ± 9.5 | 373.6 ± 15.3 |
| Phosphorus (mg/d) | 911.42 ± 7.1 | 883.7 ± 16.8 | 911.7 ± 14.9 | 1015.5 ± 19.7 | 909.4 ± 16.5 | 898.6 ± 16.6 | 859.3 ± 21.7 |
| Magnesium (mg/d) | 183.52 ± 1.5 | 190.0 ± 3.9 | 178.1 ± 2.8 | 198.2 ± 4.6 | 188.1 ± 3.3 | 178.3 ± 3.1 | 169.3 ± 5.5 |
| Vitamin D (µg/d) | 4.0 ± 0.03 | 3.5 ± 0.08 | 4.4 ± 0.07 | 4.4 ± 0.1 | 3.7 ± 0.08 | 4 ± 0.09 | 4 ± 0.1 |
| Other micronutrients | |||||||
| Vitamin A (μgRE/d) | 567.46 ± 7.1 | 557.4 ± 20.3 | 531.2 ± 13.4 | 731 ± 24.6 | 610.4 ± 14.2 | 503.2 ± 11.5 | 528.5 ± 26.3 |
| Iron (mg/d) | 9.71 ± 0.08 | 9.6 ± 0.2 | 9.4 ± 0.1 | 10.7 ± 0.3 | 9.9 ± 0.2 | 9.6 ± 0.2 | 9.2 ± 0.3 |
| Zinc (mg/d) | 9.71 ± 0.06 | 7.4 ± 0.2 | 6.7 ± 0.1 | 8.2 ± 0.2 | 7.5 ± 0.1 | 7.5 ± 0.1 | 7 ± 0.2 |
| Sodium (mg/d) | 1038.6 ± 13 | 1160.1 ± 33 | 916.9 ± 21.6 | 1086.9 ± 48.4 | 1096.1 ± 31.9 | 1076.8 ± 29 | 971.6 ± 35.4 |
| Potassium (mg/d) | 1617.8 ± 12 | 1617.7 ± 29 | 1532.4 ± 24.5 | 1833.1 ± 36.2 | 1670.6 ± 28.1 | 1598.7 ± 27 | 1507.2 ± 37.1 |
| Selenium (µg/d) | 116.84 ± 1 | 116.7 ± 2.2 | 111.2 ± 1.8 | 139.8 ± 3 | 113.9 ± 2.2 | 117.2 ± 2.1 | 110.8 ± 3.3 |
| Prevalence of Inadequacy (% < EAR A/LAMDR B) | Prevalence of Excessiveness (% > UL C/UAMDR D) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All (n = 1264) | BPO (n = 174) | Factory (n = 312) | Hospitality (n = 140) | Admin (n = 272) | Sales (n = 260) | Healthcare (n = 106) | All (n = 1264) | BPO (n = 174) | Factory (n = 312) | Hospitality (n = 140) | Admin (n = 272) | Sales (n = 260) | Healthcare (n = 106) | |
| Macronutrients | ||||||||||||||
| Protein | 23.9 | 22.8 | 29.1 | 8.4 | 26.5 | 23.9 | 28.3 | - | - | - | - | - | - | - |
| As percentage of Total Energy | ||||||||||||||
| Total Fat (%) | <1 | <1 | 5.9 | 1.2 | 0 | <1 | 0 | 33.7 | 49.6 | 13.8 | 37.7 | 36.3 | 39.2 | 54.1 |
| Protein (%) | 0 | 0 | <1 | 0 | 0 | 0 | <1 | 58.1 | 72.7 | 51.7 | 64.1 | 47.5 | 61.5 | 70.8 |
| Carbohydrate (%) | 47.7 | 67.3 | 24.7 | 51.1 | 49.5 | 55.2 | 69.8 | <1 | <1 | 1.2 | <1 | 0 | 0 | 0 |
| Antioxidants | ||||||||||||||
| Vitamin C | 87.1 | 88.8 | 92.6 | 92.7 | 85.2 | 81.6 | 82.5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Vitamin E | - | - | - | - | - | - | - | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| B Vitamins | ||||||||||||||
| Thiamin | 76.6 | 83.8 | 86.2 | 63.8 | 72.9 | 71.2 | 84.9 | - | - | - | - | - | - | - |
| Riboflavin | 95.8 | 98.9 | 96.1 | 90.8 | 93.9 | 95.3 | 93.6 | - | - | - | - | - | - | - |
| Niacin | 3.1 | 4.6 | 3.6 | <1 | 4.4 | 2.7 | 2.7 | 2.3 | 3.1 | 2.9 | 4.7 | 2.1 | 1.7 | <1 |
| Vitamin B6 | 8.7 | 5.9 | 11.2 | <1 | 10.6 | 11.1 | 10 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Vitamin B12 | 6.2 | 11.8 | 6.5 | 3.3 | 11.6 | 2.1 | 6.3 | - | - | - | - | - | - | - |
| Folate | 97.9 | 96.9 | 97.5 | 98.6 | 99.1 | 97.9 | 97.1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Bone-Related Nutrients | ||||||||||||||
| Calcium | 94.7 | 99.8 | 94.2 | 88.6 | 93.2 | 94 | 91.6 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Phosphorus | 7.5 | 6.9 | 8.4 | 1.3 | 8.8 | 9.8 | 8.4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Magnesium | - | - | - | - | - | - | - | - | <1 | <1 | <1 | <1 | <1 | <1 |
| Vitamin D | - | - | - | - | - | - | - | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Other Micronutrients | ||||||||||||||
| Vitamin A | 39.7 | 43.4 | 45.6 | 16.7 | 29.4 | 48.1 | 48.8 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Iron | 99 | 99.4 | 99.3 | 96.6 | 98.5 | 99.5 | 98.6 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Zinc | 2.5 | 2.2 | 6.2 | <1 | 2.1 | 1.7 | 1.8 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Selenium | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Disease/Medical Condition Currently Being Treated m | All (n = 1264) | |
|---|---|---|
| n | % | |
| Acute infection | 62 | 25.51 |
| Allergy | 9 | 3.70 |
| Anemia | 6 | 2.47 |
| Cancer | 3 | 1.23 |
| Cardiovascular disease | 5 | 2.06 |
| Digestive & liver problem | 21 | 8.64 |
| Diabetes | 16 | 6.58 |
| Electrolyte imbalance | 17 | 7.00 |
| Gout, arthritis | 11 | 4.53 |
| Hypertension | 62 | 25.51 |
| Kidney disease | 3 | 1.23 |
| Muscle/body pain | 18 | 7.41 |
| Neurological disorder | 5 | 2.06 |
| Pulmonary disorder | 26 | 10.70 |
| Others (HIV, genetic diseases) | 3 | 1.23 |
| Medications/Non-Prescription Drugs or Herbal Supplements Presently Taken m | ||
| Herbal/food supplements | 71 | 22.12 |
| Hormonal/birth control pills | 15 | 4.67 |
| Maintenance/prescription drugs | 135 | 42.06 |
| Slimming pills | 2 | 0.62 |
| Vitamin & mineral supplements | 127 | 39.56 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angeles-Agdeppa, I.; S. Custodio, M.R. Food Sources and Nutrient Intakes of Filipino Working Adults. Nutrients 2020, 12, 1009. https://doi.org/10.3390/nu12041009
Angeles-Agdeppa I, S. Custodio MR. Food Sources and Nutrient Intakes of Filipino Working Adults. Nutrients. 2020; 12(4):1009. https://doi.org/10.3390/nu12041009
Chicago/Turabian StyleAngeles-Agdeppa, Imelda, and Ma. Rosel S. Custodio. 2020. "Food Sources and Nutrient Intakes of Filipino Working Adults" Nutrients 12, no. 4: 1009. https://doi.org/10.3390/nu12041009
APA StyleAngeles-Agdeppa, I., & S. Custodio, M. R. (2020). Food Sources and Nutrient Intakes of Filipino Working Adults. Nutrients, 12(4), 1009. https://doi.org/10.3390/nu12041009