Positive Association of Dietary Inflammatory Index with Incidence of Cardiovascular Disease: Findings from a Korean Population-Based Prospective Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Cohort Characteristics
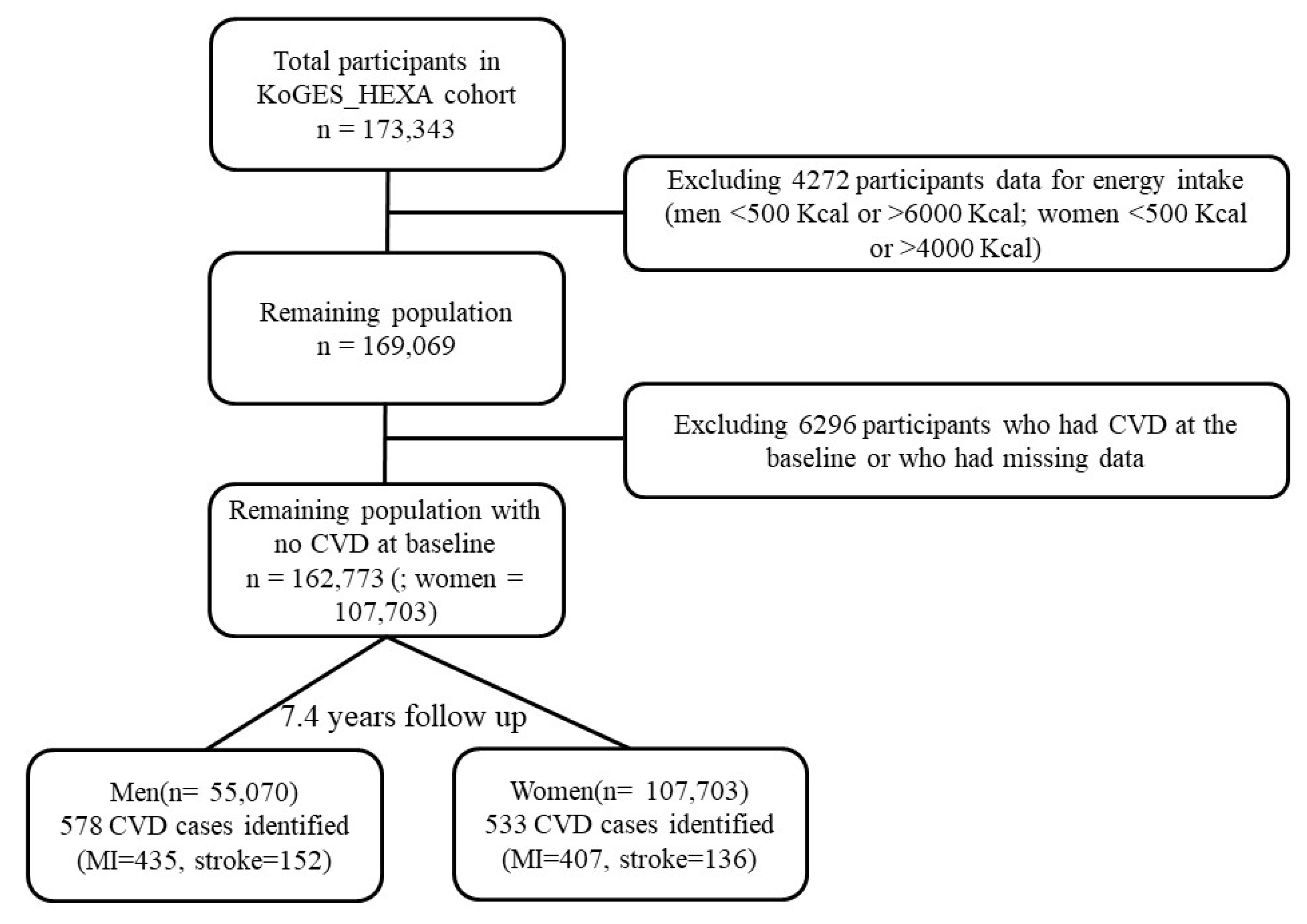
2.2. Study Population
2.3. Covariates
2.4. Dietary Assessment and Calculation of Dietary Inflammatory Index(DII)
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Diet, Nutrition and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Consultation; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Geraldo, J.M.; Alfenas, R.C. Role of diet on chronic inflammation prevention and control: Current evidences. Arq. Bras. Endocrinol. Metabol. 2008, 52, 951–967. [Google Scholar] [CrossRef]
- Galland, L. Diet and inflammation. Nutr. Clin. Pract. 2010, 25, 634–640. [Google Scholar] [CrossRef]
- Keibel, A.; Singh, V.; Sharma, M.C. Inflammation, microenvironment, and the immune system in cancer progression. Curr. Pharm. Des. 2009, 15, 1949–1955. [Google Scholar] [CrossRef]
- Harada, K.; Ferdous, T.; Mizukami, Y.; Mishima, K. Elemental diet inhibits pro-inflammatory cytokine production in keratinocytes through the suppression of NF-κB activation. Oncol. Rep. 2018, 40, 361–368. [Google Scholar] [CrossRef]
- Putaala, J.; Nieminen, T. Stroke risk period after acute myocardial infarction revised. J. Am. Heart Assoc. 2018, 7, e011200. [Google Scholar] [CrossRef]
- Bodén, S.; Wennberg, M.; Van Guelpen, B.; Johansson, I.; Lindahl, B.; Andersson, J.; Shivappa, N.; Hebert, J.R.; Nilsson, L.M. Dietary inflammatory index and risk of first myocardial infarction; a prospective population-based study. Nutr. J. 2017, 16, 21. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; De Ferranti, S.; Després, J.P.; Fullerton, H.J.; et al. Heart disease and stroke statistics-2016 update a report from the American Heart Association. Circulation 2016, 133, e38–e48. [Google Scholar]
- World Health Organization. Stroke, Cerebrovascular Accident. Available online: http://www.emro.who.int/health-topics/stroke-cerebrovascular-accident/index.html (accessed on 13 August 2019).
- Mahesh, P.; Gunathunga, M.; Jayasinghe, S.; Arnold, S.; Haniffa, R.; De Silva, A. Pre-event quality of life and its influence on the post-event quality of life among patients with ST elevation and non-ST elevation myocardial infarctions of a premier province of Sri Lanka. Health Qual. Life Outcomes 2017, 15, 154. [Google Scholar] [CrossRef]
- Medagama, A.; Bandara, R.; De Silva, C.; Galgomuwa, M.P. Management of acute coronary syndromes in a developing country; time for a paradigm shift? an observational study. BMC Cardiovasc. Disord. 2015, 15, 133. [Google Scholar] [CrossRef]
- Anderson, J.L.; Morrow, D.A. Acute myocardial infarction. N. Engl. J. Med. 2017, 376, 2053–2064. [Google Scholar] [CrossRef]
- Lee, J.; Bahk, J.; Kim, I.; Kim, Y.-Y.; Yun, S.-C.; Kang, H.-Y.; Lee, J.; Park, J.H.; Shin, S.-A.; Khang, Y.-H. Geographic variation in morbidity and mortality of cerebrovascular diseases in Korea during 2011–2015. J. Stroke Cerebrovas Dis. 2018, 27, 747–757. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef]
- Cavicchia, P.P.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Hébert, J.R. A new dietary inflammatory index predicts interval changes in serum high-sensitivity C-reactive protein. J. Nutr. 2009, 139, 2365–2372. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Tabung, F.; Hébert, J.R. A population-based dietary inflammatory index predicts levels of C-reactive protein in the Seasonal Variation of Blood Cholesterol Study (SEASONS). Public Health Nutr. 2014, 17, 1825–1833. [Google Scholar] [CrossRef]
- Wirth, M.; Burch, J.; Shivappa, N.; Violanti, J.M.; Burchfiel, C.M.; Fekedulegn, D.; Andrew, M.E.; Hartley, T.A.; Miller, D.B.; Mnatsakanova, A.; et al. Association of a dietary inflammatory index with inflammatory indices and the metabolic syndrome among police officers. J. Occup. Environ. Med. 2014, 56, 986–989. [Google Scholar] [CrossRef]
- Phillips, C.M.; Chen, L.W.; Heude, B.; Bernard, J.Y.; Harvey, N.C.; Duijts, L.; Mensink-Bout, S.M.; Polanska, K.; Mancano, G.; Suderman, M.; et al. Dietary Inflammatory Index and Non-Communicable Disease Risk: A Narrative Review. Nutrients 2019, 11, 1873. [Google Scholar] [CrossRef]
- Garcia-Arellano, A.; Martinez-Gonzalez, M.A.; Ramallal, R.; Salas-Salvado, J.; Hebert, J.R.; Corella, D.; Shivappa, N.; Forga, L.; Schroder, H.; Munoz-Bravo, C.; et al. Dietary inflammatory index and all-cause mortality in large cohorts: The SUN and PREDIMED studies. Clin. Nutr. 2019, 38, 1221–1231. [Google Scholar] [CrossRef]
- Garcia-Arellano, A.; Ramallal, R.; Ruiz-Canela, M.; Salas-Salvadó, J.; Corella, D.; Shivappa, N.; Schröder, H.; Hébert, J.; Ros, E.; Gómez-Garcia, E.; et al. Dietary inflammatory index and incidence of cardiovascular disease in the PREDIMED study. Nutrients 2015, 7, 4124–4138. [Google Scholar] [CrossRef]
- Shivappa, N.; Godos, J.; Hébert, J.R.; Wirth, M.; Piuri, G.; Speciani, A.; Grosso, G. Dietary inflammatory index and cardiovascular risk and mortality—A meta-analysis. Nutrients 2018, 10, 200. [Google Scholar] [CrossRef]
- Alkerwi, A.; Shivappa, N.; Crichton, G.; Hébert, J.R. No significant independent relationships with cardiometabolic biomarkers were detected in the Observation of Cardiovascular Risk Factors in Luxembourg study population. Nutr. Res. 2014, 34, 1058–1065. [Google Scholar] [CrossRef]
- Ramallal, R.; Toledo, E.; Martínez-González, M.A.; Hernández-Hernández, A.; García-Arellano, A.; Shivappa, N.; Hebert, J.R.; Ruiz-Canela, M. Dietary inflammatory index and incidence of cardiovascular disease in the SUN cohort. PLoS ONE 2015, 10, e0135221. [Google Scholar] [CrossRef]
- Neufcourt, L.; Assmann, K.E.; Fezeu, L.K.; Touvier, M.; Graffouillere, L.; Shivappa, N.; Hébert, J.R.; Wirth, M.D.; Hercberg, S.; Galan, P.; et al. Prospective association between the dietary inflammatory index and cardiovascular diseases in the SUpplémentation en VItamines et Minéraux AntioXydants (SU. VI. MAX) cohort. J. Am. Heart Assoc. 2016, 5, e002735. [Google Scholar] [CrossRef]
- Vissers, L.E.; Waller, M.A.; van der Schouw, Y.T.; Hebert, J.R.; Shivappa, N.; Schoenaker, D.A.; Mishra, G.D. The relationship between the dietary inflammatory index and risk of total cardiovascular disease, ischemic heart disease and cerebrovascular disease: Findings from an Australian population-based prospective cohort study of women. Atherosclerosis 2016, 253, 164–170. [Google Scholar] [CrossRef]
- Asadi, Z.; Yaghooti-Khorasani, M.; Ghazizadeh, H.; Sadabadi, F.; Mosa-Farkhany, E.; Darroudi, S.; Shabani, N.; Kamel-khodabandeh, A.; Bahrami, A.; Khorrami-Mohebbseraj, M.-S.; et al. Association between dietary inflammatory index and risk of cardiovascular disease in the Mashhad stroke and heart atherosclerotic disorder study population. IUBMB Life 2019, 1–10. [Google Scholar] [CrossRef]
- Shivappa, N.; Tavani, A.; Hébert, J.R.; Rosato, V.; La Vecchia, C. Dietary inflammatory index and acute myocardial infarction in a large Italian case–control study. Eur. J. Public Health 2018, 28, 161–166. [Google Scholar] [CrossRef]
- Agraib, L.M.; Azab, M.; Al-Shudifat, A.E.; Allehdan, S.S.; Shivappa, N.; Hebert, J.R.; Rayyem, R. Dietary inflammatory index and odds of coronary artery disease in a case-control study from Jordan. Nutrition 2019, 63, 98–105. [Google Scholar] [CrossRef]
- Okada, E.; Shirakawa, T.; Shivappa, N.; Wakai, K.; Suzuki, K.; Date, C.; Iso, H.; Hébert, J.R.; Tamakoshi, A. Dietary Inflammatory Index Is Associated with Risk of All-Cause and Cardiovascular Disease Mortality but Not with Cancer Mortality in Middle-Aged and Older Japanese Adults. J. Nutr. 2019, 149, 1451–1459. [Google Scholar] [CrossRef]
- Kim, Y.; Han, B.-G. Cohort profile: The Korean genome and epidemiology study (KoGES) consortium. Int. J. Epidemiol. 2016, 46, e20. [Google Scholar] [CrossRef]
- Ahn, Y.; Kwon, E.; Shim, J.E.; Park, M.K.; Joo, Y.; Kimm, K.; Park, C.; Kim, D.H. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef]
- Kim, J.; Kim, Y.; Ahn, Y.-O.; Paik, H.-Y.; Ahn, Y.; Tokudome, Y.; Hamajima, N.; Inouc, M.; Tajima, K. Development of a food frequency questionnaire in Koreans. Asia Pac. J. Clin. Nutr. 2003, 12, 243–250. [Google Scholar]
- National Rural Resources Development Institute. Food Composition Table, 9th ed.; Rural Development Administration, National Rural Resources Development Institute: Suwon, Korea. Available online: http://koreanfood.rda.go.kr/eng/fctFoodSrchEng/engMain (accessed on 15 July 2019).
- Kim, H.S.; Kwon, M.; Lee, H.Y.; Shivappa, N.; Hébert, J.R.; Sohn, C.; Na, W.; Kim, M.K. Higher Pro-Inflammatory Dietary Score is Associated with Higher Hyperuricemia Risk: Results from the Case-Controlled Korean Genome and Epidemiology Study_Cardiovascular Disease Association Study. Nutrients 2019, 11, 1803. [Google Scholar] [CrossRef]
- Kim, H.S.; Sohn, C.; Kwon, M.; Na, W.; Shivappa, N.; Hébert, J.R.; Kim, M.K. Positive association between dietary inflammatory index and the risk of osteoporosis: Results from the KoGES_Health Examinee (HEXA) cohort study. Nutrients 2018, 10, 1999. [Google Scholar] [CrossRef]
- Libby, P.; Ridker, P.M.; Hansson, G.K. Progress and challenges in translating the biology of atherosclerosis. Nature 2011, 473, 317–325. [Google Scholar] [CrossRef]
- Jin, R.; Yang, G.; Li, G. Inflammatory mechanisms in ischemic stroke: Role of inflammatory cells. J. Leukoc. Biol. 2010, 87, 779–789. [Google Scholar] [CrossRef]
- Lock, K.; Pomerleau, J.; Causer, L.; Altmann, D.R.; McKee, M. The global burden of disease attributable to low consumption of fruit and vegetables: Implications for the global strategy on diet. Bull. World Health Organ. 2005, 83, 100–108. [Google Scholar]
- Mizrahi, A.; Knekt, P.; Montonen, J.; Laaksonen, M.A.; Heliövaara, M.; Järvinen, R. Plant foods and the risk of cerebrovascular diseases: A potential protection of fruit consumption. Br. J. Nutr. 2009, 102, 1075–1083. [Google Scholar] [CrossRef]
- Larsson, S.C.; Virtamo, J.; Wolk, A. Total and specific fruit and vegetable consumption and risk of stroke: A prospective study. Atherosclerosis 2013, 227, 147–152. [Google Scholar] [CrossRef]
- Larsson, S.C.; Wolk, A. Dietary fiber intake is inversely associated with stroke incidence in healthy Swedish adults. J. Nutr. 2014, 144, 1952–1955. [Google Scholar] [CrossRef]
- John, J.; Ziebland, S.; Yudkin, P.; Roe, L.S.; Neil, H. Effects of fruit and vegetable consumption on plasma antioxidant concentrations and blood pressure: A randomised controlled trial. Lancet 2002, 359, 1969–1974. [Google Scholar] [CrossRef]
- He, F.J.; MacGregor, G.A. Beneficial effects of potassium. BMJ 2001, 323, 497–501. [Google Scholar] [CrossRef]
- He, J.; Whelton, P.K. Effect of dietary fiber and protein intake on blood pressure: A review of epidemiologic evidence. Clin. Exp. Hypertens. 1999, 21, 785–796. [Google Scholar] [CrossRef]
- Kurl, S.; Tuomainen, T.; Laukkanen, J.; Nyyssonen, K.; Lakka, T.; Sivenius, J.; Salonen, J. Plasma vitamin C modifies the association between hypertension and risk of stroke. Stroke 2002, 33, 1568–1573. [Google Scholar] [CrossRef]
- Boraita Perez, A. Exercise as the cornerstone of cardiovascular prevention. Rev. Esp. Cardiol. 2008, 61, 514–528. [Google Scholar]
- Hu, F.B.; Stampfer, M.J.; Solomon, C.; Liu, S.; Colditz, G.A.; Speizer, F.E.; Willett, W.C.; Manson, J.E. Physical activity and risk for cardiovascular events in diabetic women. Ann. Intern. Med. 2001, 134, 96–105. [Google Scholar] [CrossRef]
- Blair, S.N.; Kampert, J.B.; Kohl, H.W.; Barlow, C.E.; Macera, C.A.; Paffenbarger, R.S.; Gibbons, L.W. Influences of cardiorespiratory fitness and other precursors on cardiovascular disease and all-cause mortality in men and women. JAMA 1996, 276, 205–210. [Google Scholar] [CrossRef]
- Flynn, M.G.; McFarlin, B.K.; Markofski, M.M. State of the art reviews: The anti-inflammatory actions of exercise training. Am. J. Lifestyle Med. 2007, 1, 220–235. [Google Scholar] [CrossRef]
- Terrazas, S.; Brashear, L.; Escoto, A.-K.; Lynch, S.; Slaughter, D.; Xavier, N.; Estes, N.R., II; Giordano-Mooga, S. Sex differences in obesity-induced inflammation. In Translational Studies on Inflammation; IntechOpen: London, UK, 2019. [Google Scholar] [CrossRef]
- Egger, G.; Dixon, J. Inflammatory effects of nutritional stimuli: Further support for the need for a big picture approach to tackling obesity and chronic disease. Obes. Rev. 2010, 11, 137–149. [Google Scholar] [CrossRef]
- Calder, P.C.; Ahluwalia, N.; Brouns, F.; Buetler, T.; Clement, K.; Cunningham, K.; Esposito, K.; Jönsson, L.S.; Kolb, H.; Lansink, M.; et al. Dietary factors and low-grade inflammation in relation to overweight and obesity. Br. J. Nutr. 2011, 106, S5–S78. [Google Scholar] [CrossRef]
- Yatsuya, H.; Toyoshima, H.; Yamagishi, K.; Tamakoshi, K.; Taguri, M.; Harada, A.; Ohashi, Y.; Kita, Y.; Naito, Y.; Yamada, M.; et al. Body mass index and risk of stroke and myocardial infarction in a relatively lean population: Meta-analysis of 16 Japanese cohorts using individual data. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 498–505. [Google Scholar] [CrossRef]
- Elkhader, B.A.; Abdulla, A.A.; Omer, M.A.A. Correlation of smoking and myocardial infarction among sudanese male patients above 40 years of age. Pol. J. Radiol. 2016, 81, 138–140. [Google Scholar] [CrossRef]
- Gambardella, J.; Sardu, C.; Sacra, C.; Del Giudice, C.; Santulli, G. Quit smoking to outsmart atherogenesis: Molecular mechanisms underlying clinical evidence. Atherosclerosis 2017, 257, 242–245. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Quintiles of DII a | |||||
|---|---|---|---|---|---|---|
| Q1 (Anti-Inflammatory) | Q2 | Q3 | Q4 | Q5 (Pro-Inflammatory) | p for Trend b | |
| N (n = 162,773) | n = 32,525 | n = 32,546 | n = 32,548 | n = 32,589 | n = 32,565 | |
| No. of cases | 192 | 214 | 215 | 257 | 233 | |
| Range c | −7.9018~−0.9750 | −0.9749~0.4064 | 0.4064~1.2953 | 1.2953~2.1863 | 2.1863~7.1055 | |
| Age | 52.1(7.90) d | 52.2(8.10) | 52.5(8.10) | 53.1(8.40) | 54.4(8.60) | <0.0001 |
| BMI (Kg/m2) e | 24.1(2.79) | 24.0(2.90) | 24.0(2.76) | 23.8(2.80) | 23.8(2.90) | <0.0001 |
| Energy (Kcal) | 2266(578) | 1903(425) | 1671(372) | 1496(388) | 1408(364) | <0.0001 |
| Gender | ||||||
| Male (n = 55,070) | 10,668(32.8) f | 11,060(34.0) | 11,136(34.2) | 10,894(33.4) | 11,312(34.7) | <0.0001 |
| Female (n = 107, 703) | 21,857(67.2) | 21,486(66.0) | 21,412(65.8) | 21,695(66.6) | 21,253(65.3) | |
| Education level | ||||||
| Elementary school | 3816(11.9) | 4263(13.3) | 5092(15.8) | 6226(19.3) | 8456(26.4) | <0.0001 |
| Middle~high school | 19,029(59.3) | 18,852(58.8) | 18,645(57.9) | 18,502(57.6) | 17,802(55.5) | |
| College~ | 9246(28.8) | 8982(27.9) | 8415(26.2) | 7411(23.1) | 5832(18.1) | |
| Alcohol drinking | ||||||
| Never | 16,062(49.6) | 15,956(49.2) | 16,269(50.1) | 16,755(51.6) | 17,201(52.9) | <0.0001 |
| Past | 1262(3.9) | 1139(3.5) | 1096(3.4) | 1247(3.8) | 1272(3.9) | |
| Current | 15,064(46.5) | 15,330(47.3) | 15,100(46.5) | 14,494(44.6) | 14,001(43.2) | |
| Physical activity g | ||||||
| Irregular | 12,761(39.3) | 14,274(43.9) | 15,182(46.7) | 16,333(50.3) | 18,641(57.4) | <0.0001 |
| Regular | 19,685(60.7) | 18,189(56.1) | 17,301(53.3) | 16,156(49.7) | 13,834(42.6) | |
| Income (million(s) won) | ||||||
| Less than 1 | ,114(7.9) | 2291(8.4) | 2771(10.1) | 3551(12.9) | 4861(17.4) | |
| 1~2 | 4,806(18.1) | 5082(18.5) | 5409(19.7) | 5926(21.6) | 6760(24.2) | <0.0001 |
| 2~3 | 6144(23.1) | 6555(23.9) | 6306(23.1) | 6129(22.3) | 5937(21.3) | |
| More than 3 | 13,587(50.9) | 13,479(49.2) | 12,934(47.1) | 11,865(43.2) | 10,339(37.1) | |
| Marital status | ||||||
| Married | 29,135(90.2) | 29,079(89.9) | 28,805(88.9) | 28,178(86.9) | 27,409(84.7) | <0.0001 |
| Unmarried/divorced | 3182(9.8) | 3265(10.1) | 3583(11.1) | 4237(13.1) | 4960(15.3) | |
| Smoking | ||||||
| Never | 24,084(74.4) | 23,772(73.3) | 23,820(73.4) | 24,010(73.9) | 23,056(71.0) | <0.0001 |
| Past | 4427(13.7) | 4782(14.8) | 4783(14.8) | 4570(14.0) | 4591(14.1) | |
| Current | 3857(11.9) | 3864(11.9) | 3842(11.8) | 3905(12.1) | 4821(14.9) | |
| Menopause status | ||||||
| Post-menopause | 11,393(56.4) | 11,488(56.4) | 11,795(57.9) | 12,576(60.9) | 13,597(65.8) | <0.0001 |
| Pre-/peri-menopause | 8801(43.6) | 8870(43.6) | 8570(42.1) | 8082(39.1) | 7073(34.2) | |
| Family history of CVD | ||||||
| Negative | 26,321(81.1) | 26,240(80.8) | 26,226(80.8) | 26,430(81.4) | 26,724(82.3) | <0.0001 |
| Positive | 6136(18.9) | 6219(19.2) | 6239(19.2) | 6056(18.6) | 5747(17.7) | |
| Quintiles of DII Score a | pb | |||||
|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | ||
| All subjects | ||||||
| Person-years | 253,146 | 243,506 | 241,516 | 238,933 | 228,429 | |
| Crude HR (95% CI) c | ref | 1.15(0.95–1.40) | 1.15(0.95–1.40) | 1.46(1.21–1.76) | 1.63(1.35–1.98) | 0.001 |
| Multivariate HR (95% CI) d | ref | 1.13(0.92–1.39) | 1.08(0.86–1.35) | 1.37(1.10–1.71) | 1.32(1.05–1.67) | 0.003 |
| Men | ||||||
| Person-years | 81,104 | 81,614 | 82,242 | 79,945 | 80,529 | |
| Crude HR (95% CI) | ref | 1.12(0.86–1.47) | 1.04(0.79–1.36) | 1.28(0.98–1.67) | 1.46(1.12–1.91) | 0.002 |
| Multivariate HR (95% CI) | ref | 1.18(0.89–1.57) | 1.10(0.81–1.49) | 1.38(1.02–1.89) | 1.43(1.04–1.96) | 0.007 |
| Women | ||||||
| Person-years | 172,042 | 161,892 | 159,274 | 158,988 | 147,900 | |
| Crude HR (95% CI) | ref | 1.13(0.85–1.50) | 1.20(0.91–1.58) | 1.56(1.20–2.03) | 1.63(1.23–2.15) | <0.0001 |
| Multivariate HR (95% CI) | ref | 1.06(0.79–1.43) | 1.05(0.77–1.44) | 1.33(0.97–1.82) | 1.19(0.85–1.67) | 0.18 |
| Quintiles of DII Score a | pb | ||||||
|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | |||
| MI | |||||||
| All subjects | Crude HR (95% CI) c | Ref. | 1.17(0.94–1.47) | 1.21(0.97–1.50) | 1.37(1.10–1.70) | 1.58(1.27–1.98) | <0.0001 |
| Multivariate HR (95% CI) d | Ref. | 1.14(0.90–1.43) | 1.09(0.85–1.40) | 1.23(0.95–1.59) | 1.23(0.94–1.60) | 0.05 | |
| Men | Crude HR (95% CI) | Ref. | 1.06(0.78–1.44) | 0.99(0.73–1.35) | 1.08(0.79–1.46) | 1.37(1.01–1.84) | 0.04 |
| Multivariate HR (95% CI) | Ref. | 1.07(0.78–1.48) | 1.01(0.72–1.42) | 1.10(0.77–1.56) | 1.27(0.89–1.82) | 0.13 | |
| Women | Crude HR (95% CI) | Ref. | 1.26(0.91–1.74) | 1.38(1.00–1.90) | 1.64(1.20–2.24) | 1.65(1.18–2.29) | 0.0002 |
| Multivariate HR (95% CI) | Ref. | 1.20(0.86–1.69) | 1.19(0.83–1.70) | 1.38(0.95–1.99) | 1.18(0.79–1.75) | 0.25 | |
| Stroke | |||||||
| All subjects | Crude HR (95% CI) | Ref. | 1.01(0.68–1.51) | 1.01(0.68–1.50) | 1.74(1.21––2.49) | 1.80(1.24–2.61) | <0.0001 |
| Multivariate HR (95% CI) | Ref. | 1.02(0.67–1.55) | 1.04(0.67–1.61) | 1.77(1.16–2.71) | 1.55(0.99–2.44) | 0.008 | |
| Men | Crude HR (95% CI) | Ref. | 1.29(0.72–2.31) | 1.22(0.68–2.18) | 2.15(1.26–3.65) | 1.90(1.09–3.32) | 0.0017 |
| Multivariate HR (95% CI) | Ref. | 1.51(0.82–2.77) | 1.46(0.77–2.77) | 2.66(1.44–4.94) | 2.06(1.07–3.98) | 0.003 | |
| Women | Crude HR (95% CI) | Ref. | 0.77(0.44–1.35) | 0.78(0.44–1.37) | 1.34(0.81–2.20) | 1.57(0.94–2.61) | 0.06 |
| Multivariate HR (95% CI) | Ref. | 0.68(0.37–1.24) | 0.74(0.40–1.37) | 1.15(0.63–2.09) | 1.17(0.62–2.20) | 0.59 | |
| Strata | Quintiles of Dietary Inflammatory Index (DII) a | p Value c | |||||
|---|---|---|---|---|---|---|---|
| Q1 | Q2 b | Q3 | Q4 | Q5 | |||
| Physical activity d | |||||||
| All subjects | Irregular | Ref. | 1.32(0.94–1.85) | 1.25(0.88–1.77) | 1.60(1.12–2.26) | 1.42(0.99–2.04) | 0.03 |
| Regular | Ref. | 1.03(0.79–1.33) | 0.98(0.74–1.30) | 1.23(0.92–1.64) | 1.28(0.94–1.74) | 0.05 | |
| Men | Irregular | Ref. | 1.65(0.98–2.78) | 1.37(0.79–2.36) | 1.69(0.97–2.92) | 1.80(1.03–3.12) | 0.03 |
| Regular | Ref. | 1.04(0.74–1.47) | 1.03(0.71–1.49) | 1.33(0.91–1.94) | 1.30(0.86–1.94) | 0.09 | |
| Women | Irregular | Ref. | 1.11(0.71–1.72) | 1.19(0.75–1.87) | 1.56(0.99–2.46) | 1.17(0.72–1.92) | 0.37 |
| Regular | Ref. | 1.01(0.67–1.50) | 0.90(0.59–1.39) | 1.08(0.69–1.70) | 1.24(0.78–1.98) | 0.36 | |
| BMI (Kg/m2) e | |||||||
| All subjects | Normal (≤22.9) | Ref. | 1.18 (0.79–1.75) | 1.08(0.71–1.65) | 1.27(0.82–1.97) | 1.29(0.82–2.03) | 0.31 |
| Overweight (≤24.9) | Ref. | 1.09(0.74–1.59) | 1.32(0.89–1.95) | 1.64(1.10–2.45) | 1.35(0.88–2.08) | 0.02 | |
| Obese (≥25) | Ref. | 1.14(0.84–1.55) | 0.94(0.67–1.31) | 1.26(0.90–1.76) | 1.34(0.95–1.90) | 0.07 | |
| Men | Normal (≤22.9) | Ref. | 1.85(1.02–3.33) | 1.05(0.53–2.07) | 1.72(0.89–3.31) | 1.33(0.66–2.68) | 0.25 |
| Overweight (≤24.9) | Ref. | 0.95(0.55–1.62) | 1.32(0.78–2.25) | 1.10(0.62–1.95) | 1.15(0.63–2.06) | 0.36 | |
| Obese (≥25) | Ref. | 1.05(0.70–1.60) | 0.97(0.62–1.51) | 1.45(0.93–2.26) | 1.77(1.13–2.76) | 0.01 | |
| Women | Normal (≤22.9) | Ref. | 0.75(0.43–1.31) | 1.09(0.64–1.88) | 0.98(0.55–1.77) | 1.26(0.69–2.30) | 0.87 |
| Overweight (≤24.9) | Ref. | 1.19(0.68–2.10) | 1.20(0.66–2.18) | 2.38(1.34–4.21) | 1.65(0.87–3.12) | 0.01 | |
| Obese (≥25) | Ref. | 1.23(0.78–1.93) | 0.91(0.55–1.50) | 1.01(0.60–1.69) | 0.88(0.51–1.52) | 0.76 | |
| Smoking | |||||||
| All subjects | No | Ref. | 1.08(0.83–1.40) | 0.97(0.74–1.29) | 1.33(1.0–1.76) | 1.21(0.89–1.63) | 0.16 |
| Yes | Ref. | 1.21(0.87–1.69) | 1.24(0.88–1.76) | 1.41(0.99–2.00) | 1.52(1.05–2.18) | 0.004 | |
| Men | No | Ref. | 1.02(0.61–1.71) | 0.70(0.39–1.25) | 1.32(0.75–2.32) | 1.07(0.57–1.98) | 0.95 |
| Yes | Ref. | 1.27(0.90–1.78) | 1.20(0.90–1.84) | 1.41(0.97–2.03) | 1.60(1.10–2.33) | 0.002 | |
| Women | No | Ref. | 1.10(0.81–1.48) | 1.07(0.78–1.47) | 1.32(0.95–1.83) | 1.23(0.87–1.74) | 0.12 |
| Yes | Ref. | 0.58(0.12–2.71) | 0.78(0.17–3.53) | 1.63(0.38–6.97) | 0.66(0.12–3.44) | 0.54 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, I.; Kwon, M.; Shivappa, N.; Hébert, J.R.; Kim, M.K. Positive Association of Dietary Inflammatory Index with Incidence of Cardiovascular Disease: Findings from a Korean Population-Based Prospective Study. Nutrients 2020, 12, 588. https://doi.org/10.3390/nu12020588
Khan I, Kwon M, Shivappa N, Hébert JR, Kim MK. Positive Association of Dietary Inflammatory Index with Incidence of Cardiovascular Disease: Findings from a Korean Population-Based Prospective Study. Nutrients. 2020; 12(2):588. https://doi.org/10.3390/nu12020588
Chicago/Turabian StyleKhan, Imran, Minji Kwon, Nitin Shivappa, James R. Hébert, and Mi Kyung Kim. 2020. "Positive Association of Dietary Inflammatory Index with Incidence of Cardiovascular Disease: Findings from a Korean Population-Based Prospective Study" Nutrients 12, no. 2: 588. https://doi.org/10.3390/nu12020588
APA StyleKhan, I., Kwon, M., Shivappa, N., Hébert, J. R., & Kim, M. K. (2020). Positive Association of Dietary Inflammatory Index with Incidence of Cardiovascular Disease: Findings from a Korean Population-Based Prospective Study. Nutrients, 12(2), 588. https://doi.org/10.3390/nu12020588