Zinc Burden Evokes Copper Deficiency in the Hypoalbuminemic Hemodialysis Patients

 ,
,
Abstract
1. Introduction
2. Patients and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Prasad, A.S.; Brewer, G.J.; Schoomaker, E.B.; Rabbani, P. Hypocupremia Induced by Zinc Therapy in Adults. JAMA 1978, 240, 2166. [Google Scholar] [CrossRef]
- Lu, J.; Stewart, A.J.; Sadler, P.J.; Pinheiro, T.J.; Blindauer, C.A. Albumin as a zinc carrier: Properties of its high-affinity zinc-binding site. Biochem. Soc. Trans. 2008, 36, 1317–1321. [Google Scholar] [CrossRef]
- Miyata, S.; Okuno, T.; Shimamura, Y.; Miyake, T. Absorption and excertion of zinc in the aged. Nippon. Ronen Igakkai Zasshi. Jpn. J. Geriatr. 1987, 24, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Condon, C.J.; Freeman, R.M. Zinc Metabolism in Renal Failure. Ann. Intern. Med. 1970, 73, 531. [Google Scholar] [CrossRef] [PubMed]
- Abdulla, M. How adequate is plasma zinc as an indicator of zinc status? Prog. Clin. Biol. Res. 1983, 129, 171–183. [Google Scholar] [PubMed]
- Gomi, T.; Yuhara, M.; Nakayama, D.; Kasatani, T.; Ikeda, T.; Saito, M. Zinc metabolism in chronic hemodialysis patients. J. Jpn. Soc. Dial. Ther. 1984, 17, 39–46. [Google Scholar] [CrossRef]
- Duncan, A.; Yacoubian, C.; Watson, N.; Morrison, I. The risk of copper deficiency in patients prescribed zinc supplements. J. Clin. Pathol. 2015, 68, 723–725. [Google Scholar] [CrossRef]
- Duncan, A.; Talwar, D.; Morrison, I. The predictive value of low plasma copper and high plasma zinc in detecting zinc-induced copper deficiency. Ann. Clin. Biochem. Int. J. Lab. Med. 2016, 53, 575–579. [Google Scholar] [CrossRef]
- Hayton, B.A.; Broome, H.E.; Lilenbaum, R.C. Copper deficiency-induced anemia and neutropenia secondary to intestinal malabsorption. Am. J. Hematol. 1995, 48, 45–47. [Google Scholar] [CrossRef]
- Schleper, B.; Stuerenburg, H.J. Copper deficiency-associated myelopathy in a 45-year-old woman. J. Neurol. 2001, 248, 705–706. [Google Scholar] [CrossRef]
- Kumar, N.; Ahlskog, J.E.; Klein, C.J.; Port, J.D. Imaging features of copper deficiency myelopathy: A study of 25 cases. Neuroradiology 2005, 48, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Everett, C.M.; Matharu, M.; Gawler, J. Neuropathy progressing to myeloneuropathy 20 years after partial gastrectomy. Neurology 2006, 66, 1451. [Google Scholar] [CrossRef] [PubMed]
- Halfdanarson, T.R.; Kumar, N.; Phyliky, R.L.; Hogan, W.J.; Li, C.-Y. Hematological manifestations of copper deficiency: A retrospective review. Eur. J. Haematol. 2008, 80, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Jaiser, S.; Winston, G.P. Copper deficiency myelopathy. J. Neurol. 2010, 257, 869–881. [Google Scholar] [CrossRef]
- Gletsu, N.; Broderius, M.; Frediani, J.; Zhao, V.M.; Griffith, D.P.; Davis, S.S.; Sweeney, J.F.; Lin, E.; Prohaska, J.R.; Ziegler, T.R. Incidence and prevalence of copper deficiency following roux-en-y gastric bypass surgery. Int. J. Obes. 2011, 36, 328–335. [Google Scholar] [CrossRef]
- Willis, M.S.; Monaghan, S.A.; Miller, M.L.; McKenna, R.W.; Perkins, W.D.; Levinson, B.S.; Bhushan, V.; Kroft, S.H. Zinc-induced copper defiency: A report of three cases initially recognized on bone marrow examination. Am. J. Clin. Pathol. 2005, 123, 125–131. [Google Scholar] [CrossRef]
- Halfdanarson, T.R.; Kumar, N.; Hogan, W.J.; Murray, J.A. Copper Deficiency in Celiac Disease. J. Clin. Gastroenterol. 2009, 43, 162–164. [Google Scholar] [CrossRef]
- Stec, J.; Podracká, Ľ.; Pavkovčeková, O.; Kollár, J.; Pavkovčeková, O. Zinc and Copper Metabolism in Nephrotic Syndrome. Nephron 1990, 56, 186–187. [Google Scholar] [CrossRef]
- Schlockow, I. Über ein eigenartiges Rückenmarksleiden der Zinkhüttenarbeiter. Dtsch. Med. Wöchensch. 1875, 1, 208–210, 221–222. (In German) [Google Scholar]
- Lanska, D.J.; Remler, B. Myelopathy among zinc-smelter workers in Upper Silesia during the late 19th century. Neurology 2014, 82, 1175–1179. [Google Scholar] [CrossRef]
- Sugiura, T.; Goto, K.; Ito, K.; Ueta, A.; Fujimoto, S.; Togari, H. Chronic zinc toxicity in an infant who received zinc therapy for atopic dermatitis. Acta Paediatr. 2005, 94, 1333–1335. [Google Scholar] [CrossRef] [PubMed]
- Yaldizli, Ö.; Johansson, U.; Gizewski, E.R.; Maschke, M. Copper deficiency myelopathy induced by repetitive parenteral zinc supplementation during chronic hemohemodialysis. J. Neurol. 2006, 253, 1507–1509. [Google Scholar] [CrossRef] [PubMed]
- Nations, S.P.; Boyer, P.J.; Love, L.A.; Burritt, M.F.; Butz, J.A.; Wolfe, G.I.; Hynan, L.; Reisch, J.; Trivedi, J.R. Denture cream: An unusual source of excess zinc, leading to hypocupremia and neurologic disease. Neurology 2008, 71, 639–643. [Google Scholar] [CrossRef] [PubMed]
- Hedera, P.; Peltier, A.; Fink, J.K.; Wilcock, S.; London, Z.; Brewer, G.J. Myelopolyneuropathy and pancytopenia due to copper deficiency and high zinc levels of unknown origin II. The denture cream is a primary source of excessive zinc. NeuroToxicology 2009, 30, 996–999. [Google Scholar] [CrossRef]
- Prodan, C.I.; Holland, N.; Wisdom, P.; Burstein, S.; Bottomley, S. CNS demyelination associated with copper deficiency and hyperzincemia. Neurology 2002, 59, 1453–1456. [Google Scholar] [CrossRef]
- Hedera, P.; Fink, J.K.; Bockenstedt, P.L.; Brewer, G.J. Myelopolyneuropathy and Pancytopenia Due to Copper Deficiency and High Zinc Levels of Unknown Origin. Arch. Neurol. 2003, 60, 1303–1306. [Google Scholar] [CrossRef]
- Kumar, N.; Elliott, M.A.; Hoyer, J.D.; Harper, C.M., Jr.; Ahlskog, J.E.; Phyliky, R.L. “Myelodysplastic syndrome,” myeloneuropathy, and copper deficiency. Mayo. Clin. Proc. 2005, 80, 943–946. [Google Scholar] [CrossRef]
- Tormoehlen, L.M.; Kumar, N. Neurotoxicology: Five new things. Neurol. Clin. Pract. 2012, 2, 301–310. [Google Scholar] [CrossRef]
- Yuzbasiyan-Gurkan, V.; Grider, A.; Nostrant, T.; Cousins, R.J.; Brewer, G.J. Treatment of Wilson’s Disease with Zinc: X. Intestinal Metallothionein Induction. J. Lab. Clin. Med. 1992, 120, 380–386. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Zinc < 60 (μg/dL) N = 27 | Zinc ≧ 60 (μg/dL) N = 38 | ||||
|---|---|---|---|---|---|
| Average | SD | Average | SD | ||
| Age(Y) | 73.9 | 11.9 | 71.0 | 11.6 | |
| Heritage(Y) | 8.5 | 9.3 | 6.0 | 4.2 | |
| T-Cho(mg/dL) | 147.9 | 26.2 | 151.2 | 28.7 | |
| TP(g/dL) | 6.2 | 0.6 | 6.4 | 0.5 | |
| Alb(g/dL) | 3.2 | 0.3 | 3.5 | 0.3 | ※※ |
| CRP(mg/L) | 0.5 | 0.9 | 0.3 | 0.7 | |
| ALP(IU) | 240.7 | 73.4 | 239.6 | 105.9 | |
| WBC(×103) | 5.3 | 1.7 | 5.9 | 2.1 | |
| Hb(g/dL) | 10.4 | 1.0 | 11.1 | 1.1 | |
| MCV(fl) | 93.7 | 6.9 | 94.1 | 5.3 | |
| TSAT(%) | 19.8 | 8.5 | 21.2 | 8.3 | |
| Ferritin(ng/mL) | 71.0 | 55.1 | 77.5 | 67.2 | |
| Cu(μ/dL) | 85.8 | 21.6 | 80.1 | 20.1 | |
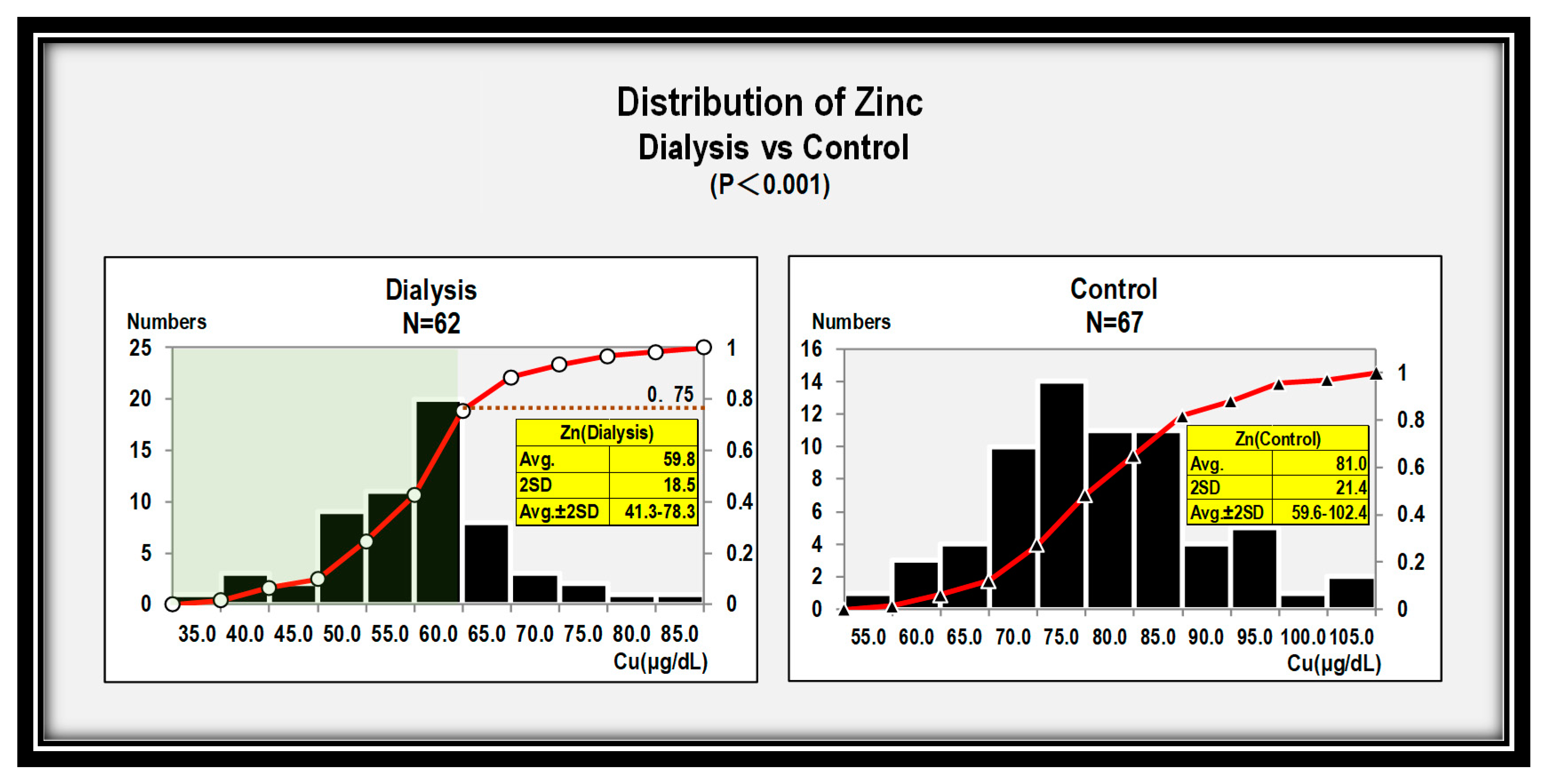
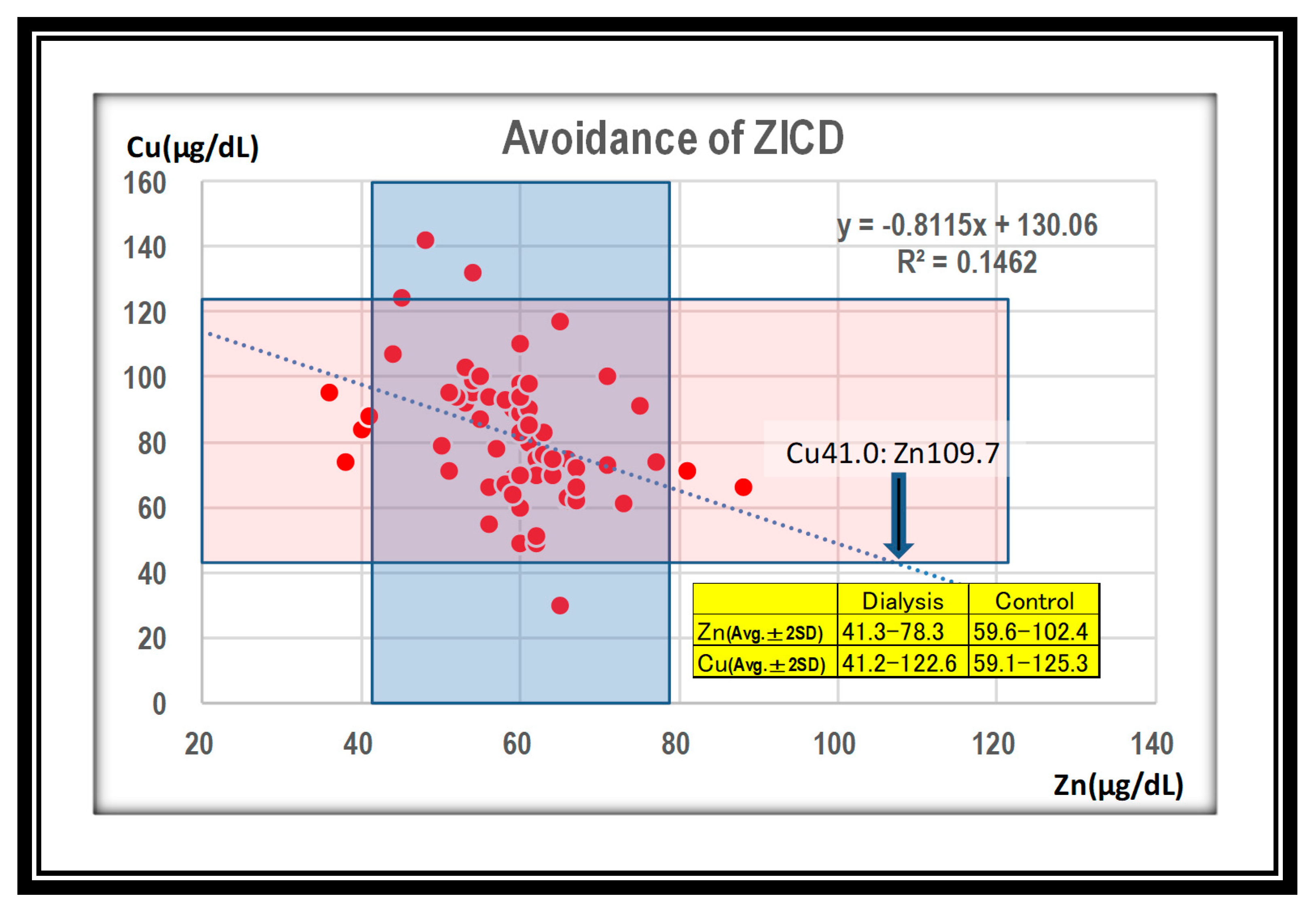
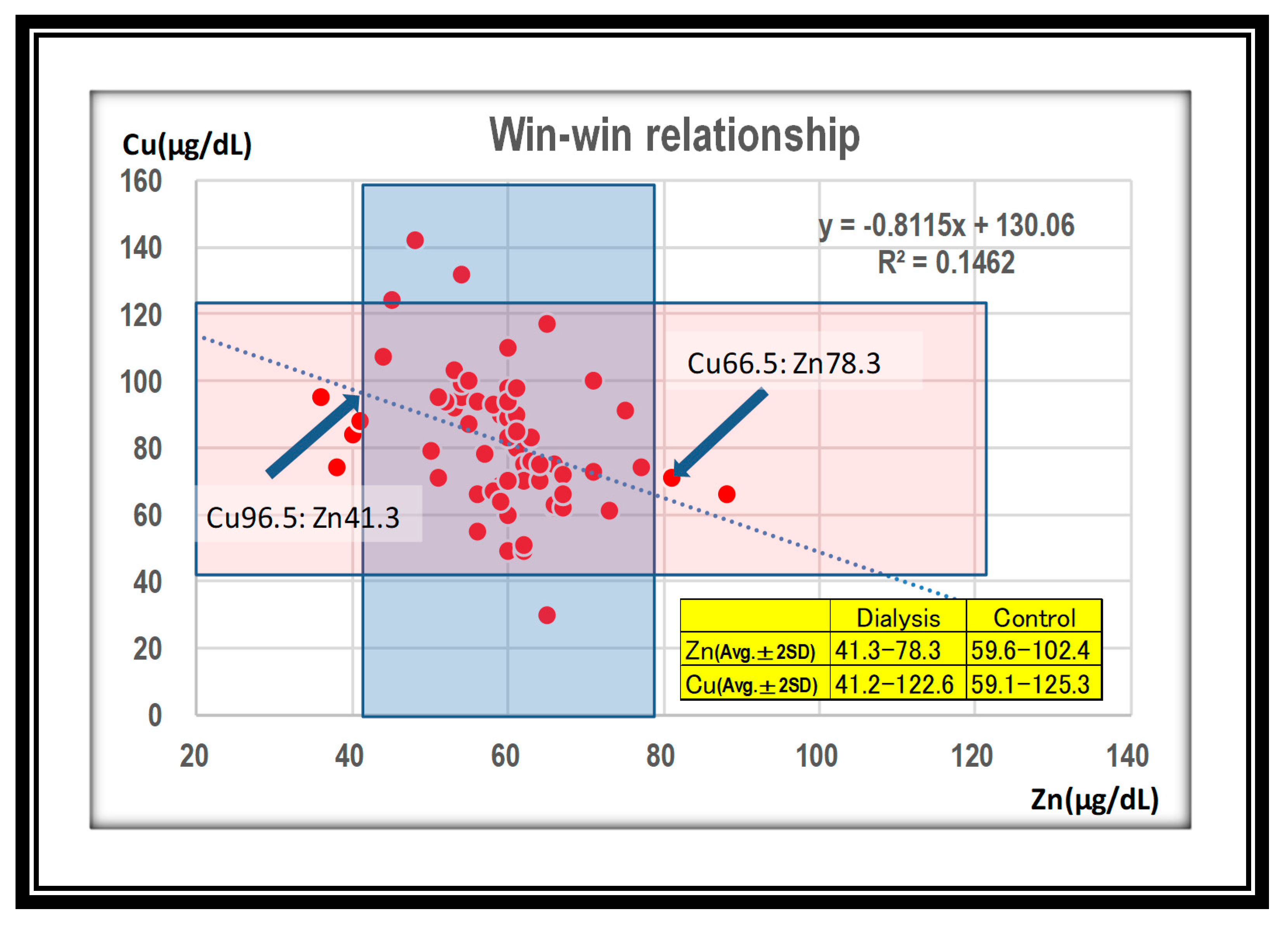
| Zn (μg/dL) | 41.3~78.3 |
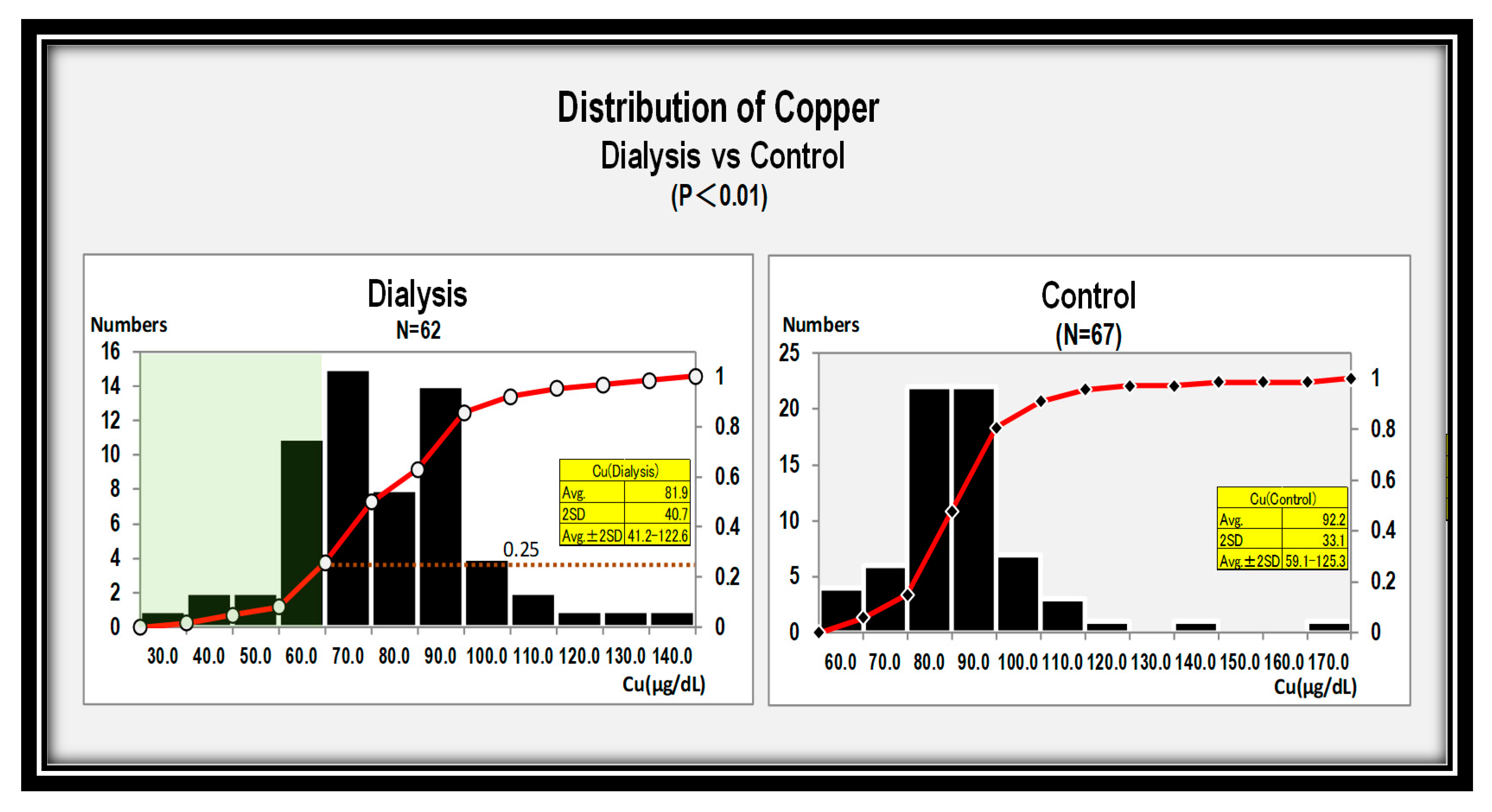
| Cu (μg/dL) | 66.5~96.5 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishime, K.; Kondo, M.; Saito, K.; Miyawaki, H.; Nakagawa, T. Zinc Burden Evokes Copper Deficiency in the Hypoalbuminemic Hemodialysis Patients. Nutrients 2020, 12, 577. https://doi.org/10.3390/nu12020577
Nishime K, Kondo M, Saito K, Miyawaki H, Nakagawa T. Zinc Burden Evokes Copper Deficiency in the Hypoalbuminemic Hemodialysis Patients. Nutrients. 2020; 12(2):577. https://doi.org/10.3390/nu12020577
Chicago/Turabian StyleNishime, Keizo, Morihiro Kondo, Kazuhiro Saito, Hisashi Miyawaki, and Takahiko Nakagawa. 2020. "Zinc Burden Evokes Copper Deficiency in the Hypoalbuminemic Hemodialysis Patients" Nutrients 12, no. 2: 577. https://doi.org/10.3390/nu12020577
APA StyleNishime, K., Kondo, M., Saito, K., Miyawaki, H., & Nakagawa, T. (2020). Zinc Burden Evokes Copper Deficiency in the Hypoalbuminemic Hemodialysis Patients. Nutrients, 12(2), 577. https://doi.org/10.3390/nu12020577