Oropharyngeal Colostrum Positively Modulates the Inflammatory Response in Preterm Neonates


 ,
,  ,
, 
Abstract
1. Introduction
2. Methods
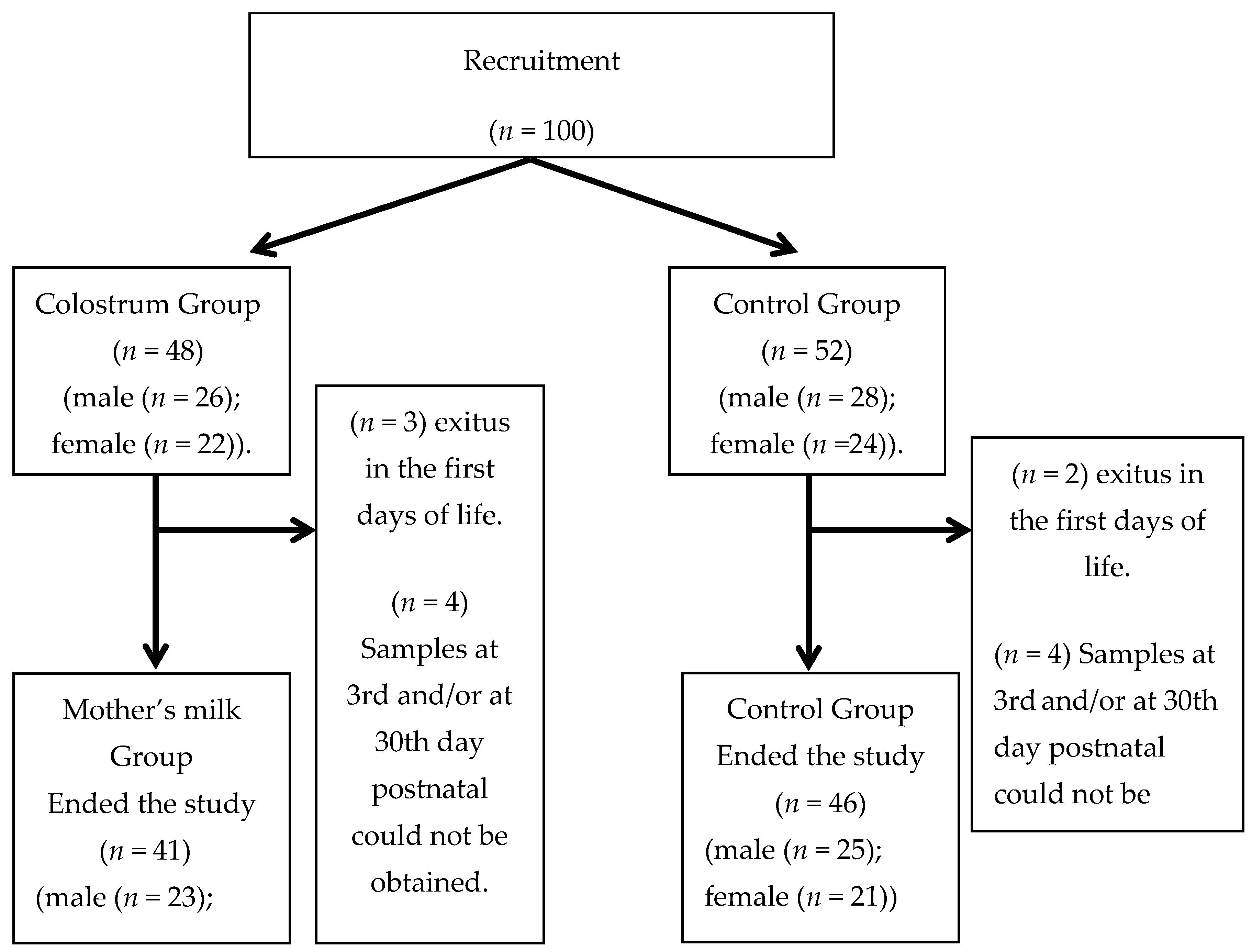
2.1. Experimental Design and Subjects
2.2. Milk Sampling and Administration
2.3. Sample Collection and Analysis
2.4. Maternal and Neonatal Outcomes
2.5. Inflammatory Parameters Measurement
2.6. Statistical Analysis
3. Results
3.1. Maternal and Neonatal General Characteristics
3.2. Clinical Outcomes
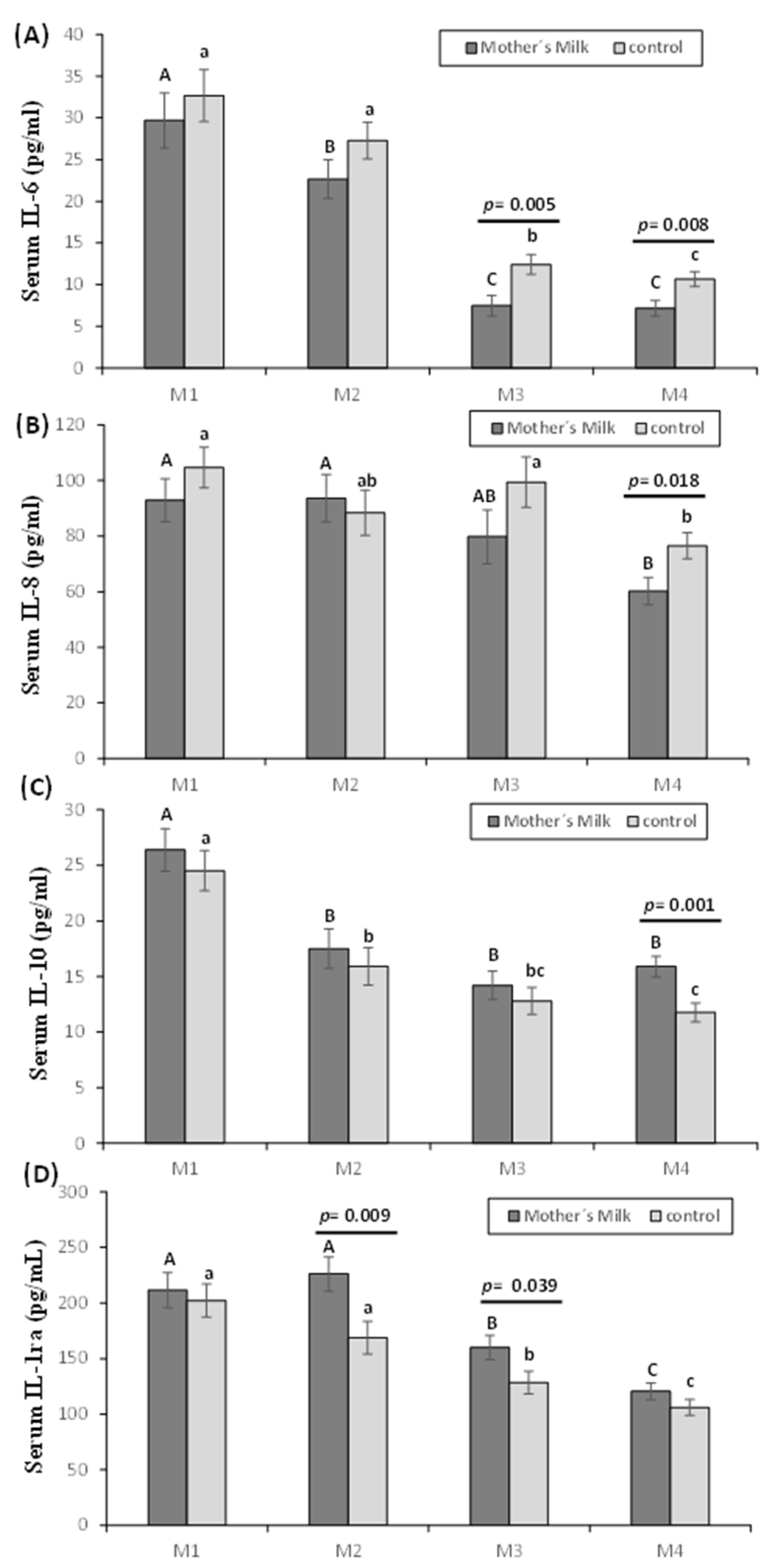
3.3. Pro- and Anti-Inflammatory Interleukins
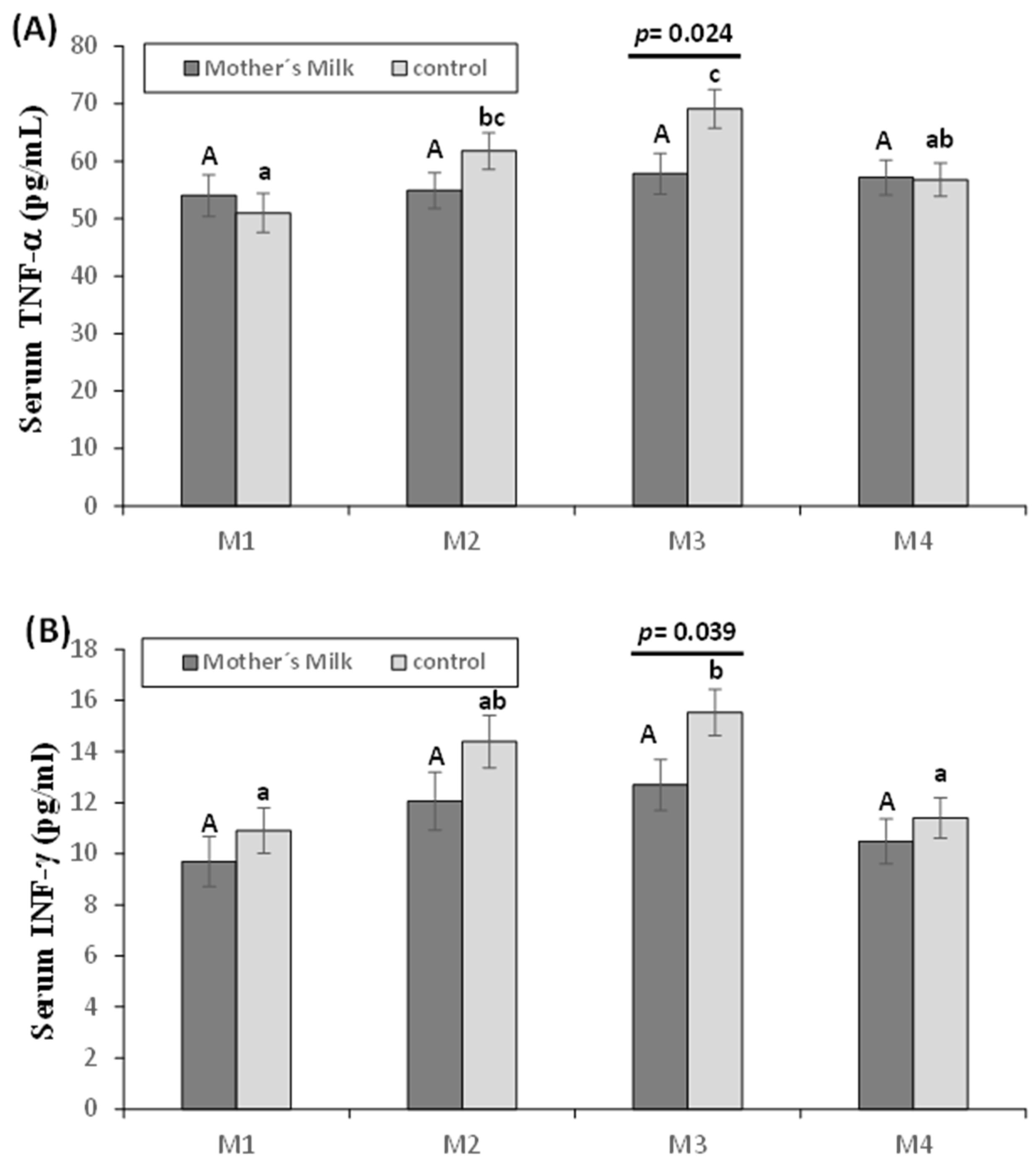
3.4. Other Cytokines: TNF-α and INF-γ
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Romero, R.; Miranda, J.; Chaiworapongsa, T.; Korzeniewski, S.J.; Chaemsaithong, P.; Gotsch, F.; Dong, Z.; Ahmed, A.I.; Yoon, B.H.; Hassan, S.S.; et al. Prevalence and clinical significance of sterile intra-amniotic inflammation in patients with preterm labor and intact membranes. Am. J. Reprod. Immunol. 2014, 72, 458–474. [Google Scholar] [CrossRef] [PubMed]
- Gotsch, F.; Romero, R.; Kusanovic, J.P.; Mazaki-Tovi, S.; Pineles, B.L.; Erez, O.; Espinoza, J.; Hassan, S.S. The fetal inflammatory response syndrome. Clin. Obstet. Gynecol. 2007, 50, 652–683. [Google Scholar] [CrossRef] [PubMed]
- McAdams, R.M.; Juul, S.E. The role of cytokines and inflammatory cells in perinatal brain injury. Neurol. Res. Int. 2012, 2012, 561494. [Google Scholar] [CrossRef] [PubMed]
- Iliodromiti, Z.; Zygouris, D.; Sifakis, S.; Pappa, K.I.; Tsikouras, P.; Salakos, N.; Daniilidis, A.; Siristatidis, C.; Vrachnis, N. Acute lung injury in preterm fetuses and neonates: Mechanisms and molecular pathways. J. Matern-Fetal Neonatal Med. 2013, 26, 1696–1704. [Google Scholar] [CrossRef]
- Amerrican College of Obstetricians and Gynecologists. ACOG committee opinion no. 561: Nonmedically indicated early-term deliveries. Obstet. Gynecol. 2013, 121, 911–915. [Google Scholar] [CrossRef]
- Shah, B.A.; Padbury, J.F. Neonatal sepsis: An old problem with new insights. Virulence 2014, 5, 170–178. [Google Scholar] [CrossRef]
- Pammi, M.; Flores, A.; Leeflang, M.; Versalovic, J. Molecular assays in the diagnosis of neonatal sepsis: A systematic review and meta-analysis. Pediatrics 2011, 128, e973–e985. [Google Scholar] [CrossRef]
- Arad, I.; Bar-Oz, B.; Ergaz, Z.; Nir, A.; Barak, V. Interleukin-6 and N-terminal pro-brain natriuretic peptide cord blood levels in premature infants: Correlations with perinatal variables. Isr. Med. Assoc. J. 2010, 12, 419–423. [Google Scholar]
- Caldas, J.P.; Vilela, M.M.; Braghini, C.A.; Mazzola, T.N.; Marba, S.T. Antenatal maternal corticosteroid administration and markers of oxidative stress and inflammation in umbilical cord blood from very low birth weight preterm newborn infants. J. Pediatr. 2012, 88, 61–66. [Google Scholar] [CrossRef]
- Ronnestad, A.; Abrahamsen, T.G.; Medbø, S.; Reigstad, H.; Lossius, K.; Kaaresen, P.I.; Egeland, T.; Engelund, I.E.; Irgens, L.M.; Markestad, T. Late-onset septicemia in a Norwegian national cohort of extremely premature infants receiving very early full human milk feeding. Pediatrics 2005, 115, e269–e276. [Google Scholar] [CrossRef]
- Liu, B.; Newburg, D.S. Human milk glycoproteins protect infants against human pathogens. Breastfeed. Med. 2013, 8, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Meinzen-Derr, J.; Poindexter, B.; Wrage, L.; Morrow, A.L.; Stoll, B.; Donovan, E.F. Role of human milk in extremely low birth weight infants’ risk of necrotizing enterocolitis or death. J. Perinatol. 2009, 29, 57–62. [Google Scholar] [CrossRef]
- Underwood, M.A. Human milk for the premature infant. Pediatr. Clin. N. Am. 2013, 60, 189–207. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, N.A.; Meier, P.P.; Groer, M.W.; Zeller, J.M.; Engstrom, J.L.; Fogg, L. A pilot study to determine the safety and feasibility of oropharyngeal administration of own mother’s colostrum to extremely low-birth-weight infants. Adv. Neonatal Care 2010, 10, 206–212. [Google Scholar] [CrossRef]
- Zhang, Y.; Ji, F.; Hu, X.; Cao, Y.; Latour, J.M. Oropharyngeal Colostrum Administration in Very Low Birth Weight Infants: A Randomized Controlled Trial. Pediatr. Crit. Care Med. 2017, 18, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, N.A.; Meier, P.P.; Mw, G.; Zeller, J.M. Oropharyngeal administration of colostrum to extremely low birth weight infants: Theoretical perspectives. J. Perinatol. 2009, 29, 1–7. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lee, J.; Kim, H.S.; Jung, Y.H.; Choi, K.Y.; Shin, S.H.; Kim, E.K.; Choi, J.H. Oropharyngeal colostrum administration in extremely premature infants: An RCT. Pediatrics 2015, 135, e357–e366. [Google Scholar] [CrossRef] [PubMed]
- Panchal, H.; Athalye-Jape, G.; Patole, S. Oropharyngeal Colostrum for Preterm Infants: A Systematic Review and Meta-Analysis. Adv. Nutr. 2019, 10, 1152–1162. [Google Scholar] [CrossRef]
- Moreno-Fernandez, J.; Sanchez-Martinez, B.; Serrano-Lopez, L.; Martin-Alvarez, E.; Diaz-Castro, J.; Pena-Caballero, M.; Martin-Peregrina, F.; Alonso-Moya, M.; Maldonado-Lozano, J.; Ochoa, J.J.; et al. Enhancement of immune response mediated by oropharyngeal colostrum administration in preterm neonates. Pediatr. Allergy Immunol. 2019, 30, 234–241. [Google Scholar] [CrossRef]
- de Vries, L.S.; Eken, P.; Dubowitz, L.M. The spectrum of leukomalacia using cranial ultrasound. Behav. Brain Res. 1992, 49, 1–6. [Google Scholar] [CrossRef]
- Walsh, M.C.; Kliegman, R.M. Necrotizing enterocolitis: Treatment based on staging criteria. Pediatr. Clin. N. Am. 1986, 33, 179–201. [Google Scholar] [CrossRef]
- Levy, M.M.; Fink, M.P.; Marshall, J.C.; Abraham, E.; Angus, D.; Cook, D.; Cohen, J.; Opal, S.M.; Vincent, J.L.; Ramsay, G. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit. Care Med. 2003, 31, 1250–1256. [Google Scholar] [CrossRef] [PubMed]
- Gephart, S.M.; Weller, M. Colostrum as oral immune therapy to promote neonatal health. Adv. Neonatal Care 2014, 14, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Sty, A.C.; Sangild, P.T.; Skovgaard, K.; Thymann, T.; Bjerre, M.; Chatterton, D.E.; Purup, S.; Boye, M.; Heegaard, P.M. Spray Dried, Pasteurised Bovine Colostrum Protects Against Gut Dysfunction and Inflammation in Preterm Pigs. J. Pediatr. Gastroenterol. Nutr. 2016, 63, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, N.A.; Groer, M.W.; Zeller, J.M.; Engstron, J.L.; Fogg, L.; Du, H.; Caplan, M. A Randomized Controlled Trial of the Oropharyngeal Administration of Mother’s Colostrum to Extremely Low Birth Weight Infants in the First Days of Life. Neonatal Intens. Care 2011, 24, 31–35. [Google Scholar]
- Nadeau-Vallee, M.; Chin, P.Y.; Belarbi, L.; Brien, M.E.; Pundir, S.; Berryer, M.H.; Beaudry-Richard, A.; Madaan, A.; Sharkey, D.J.; Lupien-Meilleur, A.; et al. Antenatal Suppression of IL-1 Protects against Inflammation-Induced Fetal Injury and Improves Neonatal and Developmental Outcomes in Mice. J. Immunol. 2017, 198, 2047–2062. [Google Scholar] [CrossRef]
- Chiesa, C.; Pacifico, L.; Natale, F.; Hofer, N.; Osborn, J.F.; Resch, B. Fetal and early neonatal interleukin-6 response. Cytokine 2015, 76, 1–12. [Google Scholar] [CrossRef]
- Schollin, J. Interleukin-8 in neonatal sepsis. Acta Paediatr. 2001, 90, 961–962. [Google Scholar] [CrossRef]
- Machado, J.R.; Soave, D.F.; da Silva, M.V.; de Menezes, L.B.; Etchebehere, R.M.; Monteiro, M.L.; dos Reis, M.A.; Correa, R.R.; Celes, M.R. Neonatal sepsis and inflammatory mediators. Mediat. Inflamm. 2014, 2014, 269681. [Google Scholar] [CrossRef]
- Labrousse, D.; Perret, M.; Hayez, D.; Da Silva, S.; Badiou, C.; Couzon, F.; Bes, M.; Chavanet, P.; Lina, G.; Vandenesch, F.; et al. Kineret®/IL-1ra Blocks the IL-1/IL-8 Inflammatory Cascade during Recombinant Panton Valentine Leukocidin-Triggered Pneumonia but Not during S. aureus Infection. PLoS ONE 2014, 9, e97546. [Google Scholar] [CrossRef]
- Agarwal, S.; Karmaus, W.; Davis, S.; Gangur, V. Immune markers in breast milk and fetal and maternal body fluids: A systematic review of perinatal concentrations. J. Hum. Lact 2011, 27, 171–186. [Google Scholar] [CrossRef] [PubMed]
- Ballard, O.; Morrow, A.L. Human Milk Composition: Nutrients and Bioactive Factors. Pediatr. Clin. N. Am. 2013, 60, 49–74. [Google Scholar] [CrossRef] [PubMed]
- Rocha, G.; Proenca, E.; Guedes, A.; Carvalho, C.; Areias, A.; Ramos, J.P.; Rodrigues, T.; Guimaraes, H. Cord blood levels of IL-6, IL-8 and IL-10 may be early predictors of bronchopulmonary dysplasia in preterm newborns small for gestational age. Dis. Markers 2012, 33, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Buescher, E.S.; Malinowska, I. Soluble receptors and cytokine antagonists in human milk. Pediatr. Res. 1996, 40, 839–844. [Google Scholar] [CrossRef] [PubMed]
- Castellote, C.; Casillas, R.; Ramirez-Santana, C.; Perez-Cano, F.J.; Castell, M.; Moretones, M.G.; Lopez-Sabater, M.C.; Franch, A. Premature delivery influences the immunological composition of colostrum and transitional and mature human milk. J. Nutr. 2011, 141, 1181–1187. [Google Scholar] [CrossRef]
- Aghai, Z.H.; Saslow, J.G.; Mody, K.; Eydelman, R.; Bhat, V.; Stahl, G.; Pyon, K.; Bhandari, V. IFN-gamma and IP-10 in tracheal aspirates from premature infants: Relationship with bronchopulmonary dysplasia. Pediatr. Pulmonol. 2013, 48, 8–13. [Google Scholar] [CrossRef]
- Harijith, A.; Choo-Wing, R.; Cataltepe, S.; Yasumatsu, R.; Aghai, Z.H.; Janer, J.; Andersson, S.; Homer, R.J.; Bhandari, V. A role for matrix metalloproteinase 9 in IFNgamma-mediated injury in developing lungs: Relevance to bronchopulmonary dysplasia. Am. J. Respir. Cell Mol. Biol. 2011, 44, 621–630. [Google Scholar] [CrossRef]
- Smilowitz, J.T.; Lebrilla, C.B.; Mills, D.A.; German, J.B.; Freeman, S.L. Breast milk oligosaccharides: Structure-function relationships in the neonate. Annu. Rev. Nutr. 2014, 34, 143–169. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Maternal and Neonatal Characteristics | Units | Mother’s Milk Group | Control Group | p-Value |
|---|---|---|---|---|
| Type of birth | Vaginal (%) | 47.5 | 34.8 | 0.33 |
| Cesarean (%) | 52.5 | 65.2 | ||
| Prenatal corticosteroids | No (%) | 12.5 | 10.9 | 0.47 |
| Yes (%) | 89.1 | 87.5 | ||
| Prenatal antibiotics | No (%) | 20.5 | 15.2 | 0.49 |
| Yes (%) | 76.9 | 84.8 | ||
| Prenatal amniotic infection risk * | No (%) | 32.5 | 39.1 | 0.41 |
| Yes (%) | 67.5 | 60.9% | ||
| Gestational age (weeks) | 29.9 ± 0.4 | 29.5 ± 0.3 | 0.34 | |
| Sex | Male (%) | 60.0 | 56.5% | 0.91 |
| Female (%) | 40.0 | 43.5% | ||
| Apgar 1 | min | 6.4 ± 0.3 | 6.6 ± 0.3 | 0.65 |
| Apgar 5 | min | 8.1 ± 0.2 | 8.1 ± 0.2 | 0.83 |
| Weight | g | 1230.1 ± 48.2 | 1267.6 ± 52.4 | 0.60 |
| Height | cm | 38.6 ± 0.5 | 38.4 ± 0.7 | 0.69 |
| Head circumference | cm | 27.1 ± 0.4 | 27.0 ± 0.4 | 0.83 |
| Weight gaining first month | g | 612.9 ± 31.7 | 527.4 ± 49.2 | 0.06 |
| CRIB Score | 2.2 ± 0.4 | 2.0 ± 0.4 | 0.17 | |
| Enteral Feeding | mL/kg/day | |||
| M2 | 39.1 ± 3.8 | 34.5 ± 4.4 | 0.53 | |
| M3 | 152.1 ± 9.9 | 162.2 ± 6.3 | 0.21 | |
| M4 | 160.8 ± 5.7 | 166.8 ± 8.3 | 0.84 | |
| Parenteral Feeding | (mL/kg/day) | |||
| M2 | 84.8 ± 5.6 | 82.4 ± 5.6 | 0.92 | |
| M3 | 19.3 ± 9.0 | 12.2 ± 4.2 | 0.15 | |
| M4 | 7.5 ± 5.2 | 6.3 ± 4.2 | 0.54 |
| Clinical outcomes | Mother’s Milk Group | Control Group | p-Value |
|---|---|---|---|
| Days to achieve full enteral feeding * | 7.2 ± 0.6 | 9.1 ± 0.7 | 0.04 |
| Volume of full enteral feeding (mL) * | 118.9 ± 5.3 | 107.8 ± 5.7 | 0.38 |
| NEC at the end of the study (Bell stage ≥ 2) | 2 (4.9%) | 2 (4.3%) | 1 |
| Proven Sepsis at the end of the study | 3 (7.3%) | 2 (4.4%) | 0.66 |
| MV during 1st month of life | 9 (21.9%) | 13 (28.2%) | 0.72 |
| Abnormalities in ultrasound brain scan at 1st month of life | 14 (34.1%) | 10(21.7%) | 0.11 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martín-Álvarez, E.; Diaz-Castro, J.; Peña-Caballero, M.; Serrano-López, L.; Moreno-Fernández, J.; Sánchez-Martínez, B.; Martín-Peregrina, F.; Alonso-Moya, M.; Maldonado-Lozano, J.; Hurtado-Suazo, J.A.; et al. Oropharyngeal Colostrum Positively Modulates the Inflammatory Response in Preterm Neonates. Nutrients 2020, 12, 413. https://doi.org/10.3390/nu12020413
Martín-Álvarez E, Diaz-Castro J, Peña-Caballero M, Serrano-López L, Moreno-Fernández J, Sánchez-Martínez B, Martín-Peregrina F, Alonso-Moya M, Maldonado-Lozano J, Hurtado-Suazo JA, et al. Oropharyngeal Colostrum Positively Modulates the Inflammatory Response in Preterm Neonates. Nutrients. 2020; 12(2):413. https://doi.org/10.3390/nu12020413
Chicago/Turabian StyleMartín-Álvarez, Estefanía, Javier Diaz-Castro, Manuela Peña-Caballero, Laura Serrano-López, Jorge Moreno-Fernández, Belen Sánchez-Martínez, Francisca Martín-Peregrina, Mercedes Alonso-Moya, José Maldonado-Lozano, Jose A. Hurtado-Suazo, and et al. 2020. "Oropharyngeal Colostrum Positively Modulates the Inflammatory Response in Preterm Neonates" Nutrients 12, no. 2: 413. https://doi.org/10.3390/nu12020413
APA StyleMartín-Álvarez, E., Diaz-Castro, J., Peña-Caballero, M., Serrano-López, L., Moreno-Fernández, J., Sánchez-Martínez, B., Martín-Peregrina, F., Alonso-Moya, M., Maldonado-Lozano, J., Hurtado-Suazo, J. A., & Ochoa, J. J. (2020). Oropharyngeal Colostrum Positively Modulates the Inflammatory Response in Preterm Neonates. Nutrients, 12(2), 413. https://doi.org/10.3390/nu12020413