The Effects of Vitamin D-Enriched Mushrooms and Vitamin D3 on Cognitive Performance and Mood in Healthy Elderly Adults: A Randomised, Double-Blinded, Placebo-Controlled Trial



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
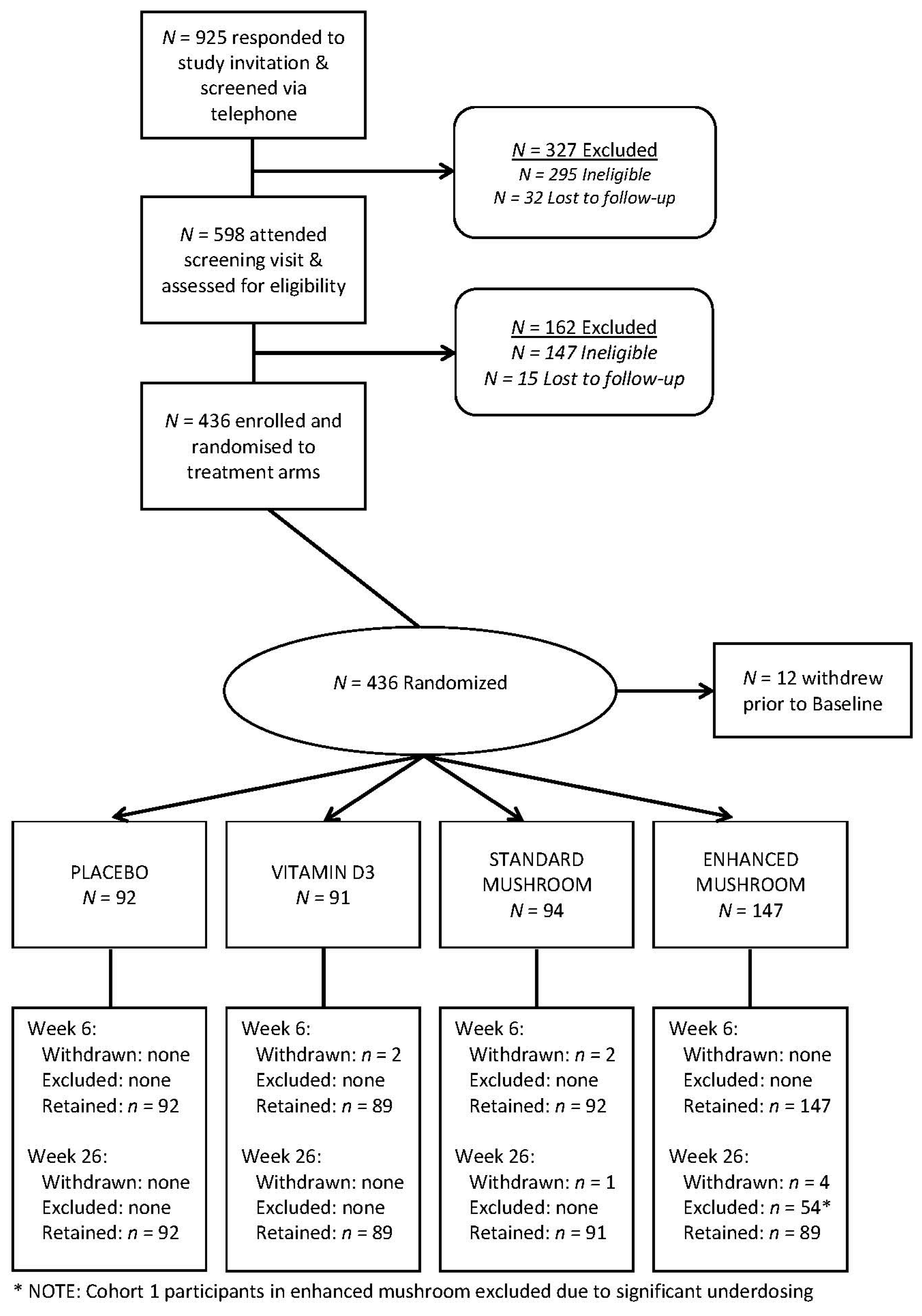
2.2. Participants and Screening
2.3. Intervention
2.4. Cognition and Mood Measures
2.5. Vitamin D Metabolite and Serum Biomarkers
2.6. Anthropometric and Covariate Measures
2.7. Power and Statistical Analysis
3. Results
3.1. Capsule Composition, Compliance and Adverse Events
3.2. Baseline Characteristics
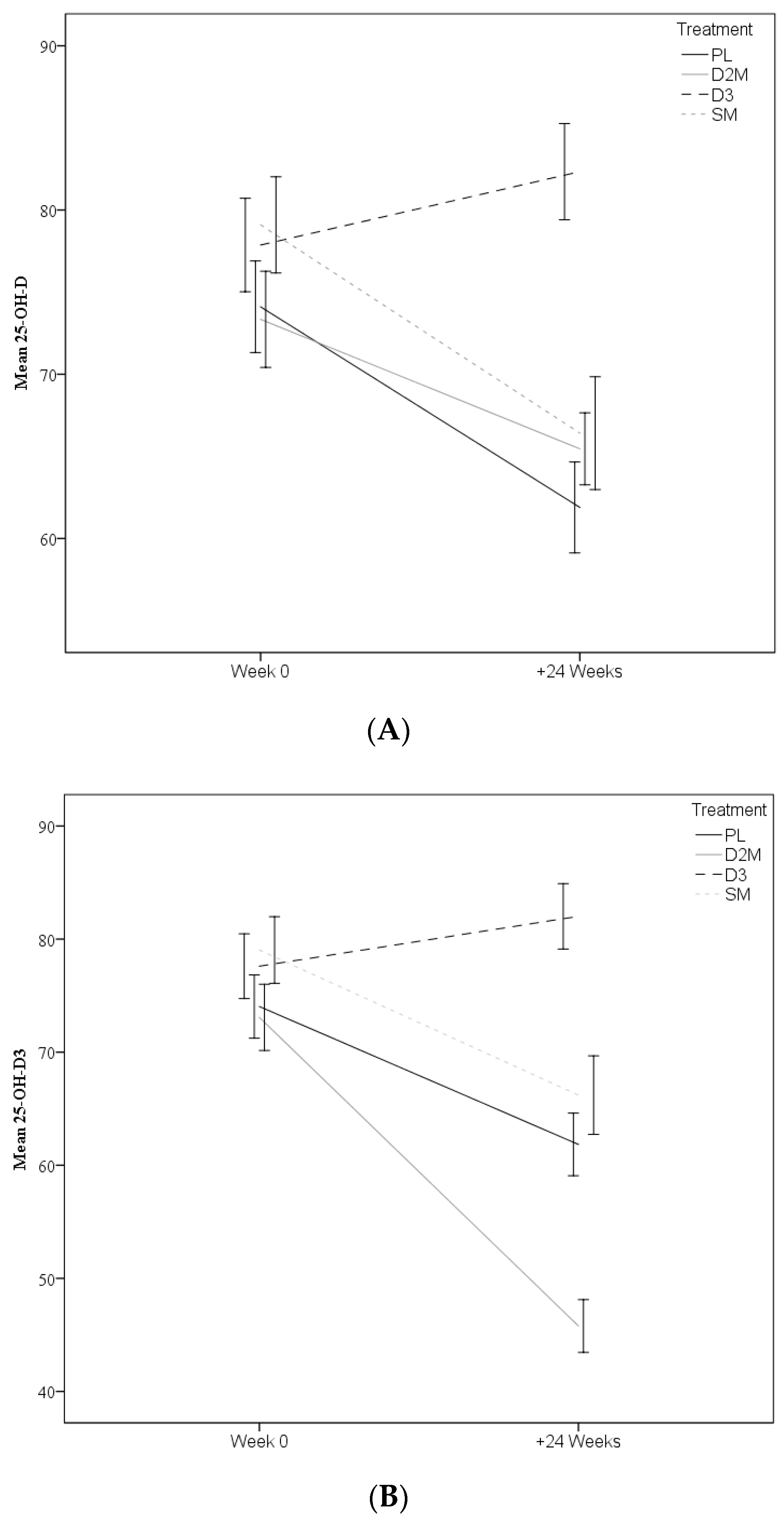
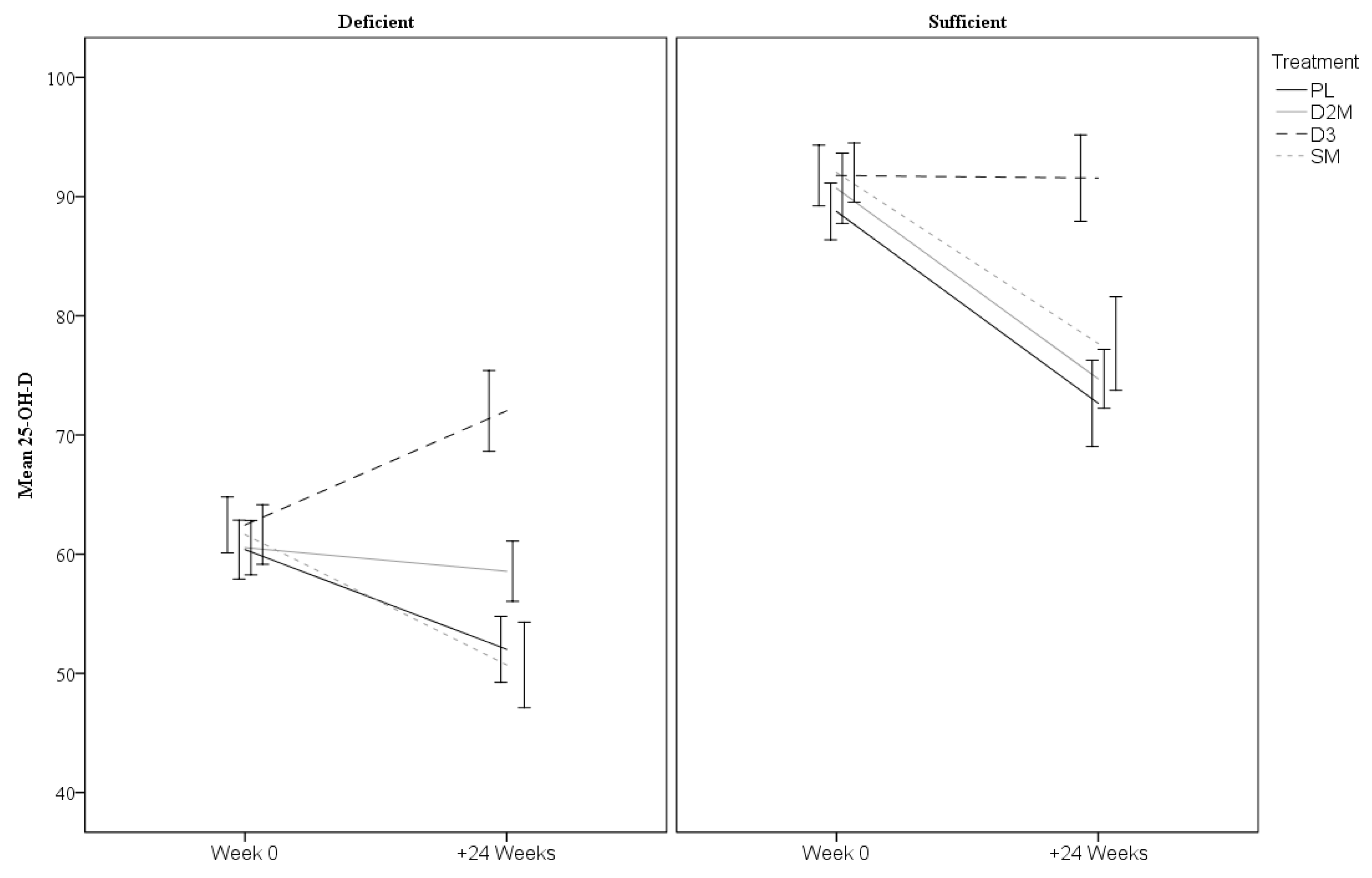
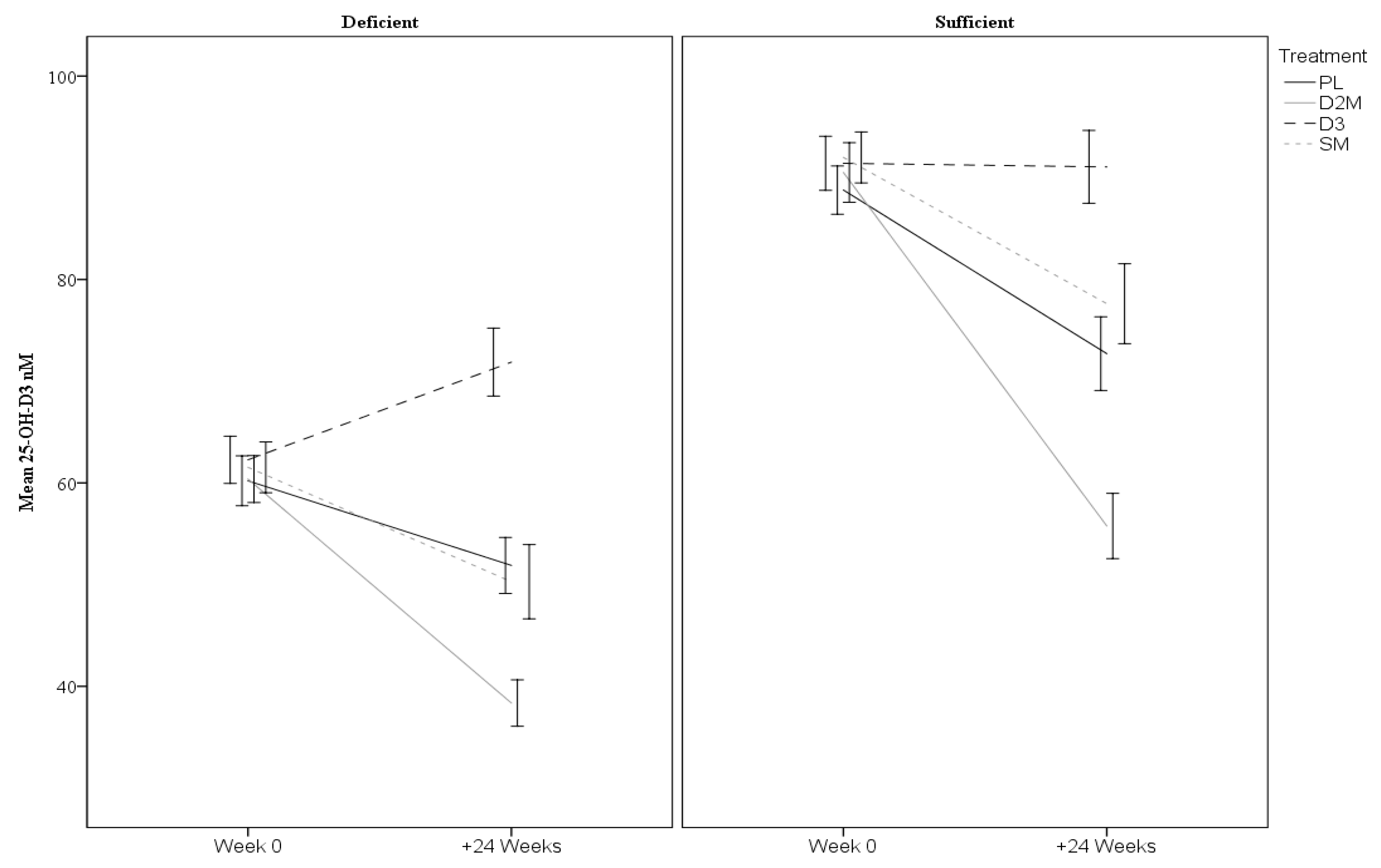
3.3. Vitamin D Outcomes
3.4. Cognitive and Mood Outcomes
4. Discussion
Study Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Keller, J.N. Age-related neuropathology, cognitive decline, and Alzheimer’s disease. Ageing Res. Rev. 2006, 5, 1–13. [Google Scholar] [CrossRef]
- Deary, I.J.; Corley, J.; Gow, A.J.; Harris, S.E.; Houlihan, L.M.; Marioni, R.E.; Penke, L.; Rafnsson, S.B.; Starr, J.M. Age-associated cognitive decline. Br. Med. Bull. 2009, 92, 135–152. [Google Scholar] [CrossRef] [PubMed]
- Salthouse, T.A. What and When of Cognitive Aging. Curr. Dir. Psychol. Sci. 2004, 13, 140–144. [Google Scholar] [CrossRef] [Green Version]
- Salthouse, T.A. The processing-speed theory of adult age differences in cognition. Psychol. Rev. 1995, 103, 403–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dark-Freudeman, A.; West, R.L.; Viverito, K.M. Future Selves and Aging: Older Adults’ Memory Fears. Educ. Gerontol. 2006, 32, 85–109. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- McCann, J.C.; Ames, B.N. Is there convincing biological or behavioral evidence linking vitamin D deficiency to brain dysfunction? FASEB J. 2007, 22, 982–1001. [Google Scholar] [CrossRef]
- Eyles, D.W.; Smith, S.; Kinobe, R.; Hewison, M.; McGrath, J.J. Distribution of the Vitamin D receptor and 1α-hydroxylase in human brain. J. Chem. Neuroanat. 2005, 29, 21–30. [Google Scholar] [CrossRef]
- Brouwer-Brolsma, E.M.; De Groot, L.C.P.G.M.; Van De Rest, O. Vitamin D and the Association with Cognitive Performance, Cognitive Decline, and Dementia. In Diet and Nutrition in Dementia and Cognitive Decline; Elsevier: Amsterdam, The Netherlands, 2015; pp. 679–700. [Google Scholar]
- A Nowson, C.; McGrath, J.J.; Ebeling, P.R.; Haikerwal, A.; Daly, R.M.; Sanders, K.M.; Seibel, M.J.; Mason, R.S. Vitamin D and health in adults in Australia and New Zealand: A position statement. Med. J. Aust. 2012, 196, 686–687. [Google Scholar] [CrossRef]
- Tripkovic, L.; Lambert, H.; Hart, K.; Smith, C.P.; Bucca, G.; Penson, S.; Chope, G.; Hyppönen, E.; Berry, J.; Vieth, R.; et al. Comparison of vitamin D2 and vitamin D3 supplementation in raising serum 25-hydroxyvitamin D status: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2012, 95, 1357–1364. [Google Scholar] [CrossRef] [Green Version]
- Bogusz, J.; Pagonis, G.; Holick, M.F. Evaluation of the bioavailability of vitamin D2 in mushrooms in healthy adults. FASEB J. 2013, 27, 794. [Google Scholar]
- Keegan, R.-J.H.; Lu, Z.; Bogusz, J.M.; Williams, J.E.; Holick, M.F. Photobiology of vitamin D in mushrooms and its bioavailability in humans. Dermato-Endocrinology 2013, 5, 165–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stepien, M.; O’Mahony, L.; O’Sullivan, A.; Collier, J.; Fraser, W.D.; Gibney, M.J.; Nugent, A.P.; Brennan, L. Effect of supplementation with vitamin D2-enhanced mushrooms on vitamin D status in healthy adults. J. Nutr. Sci. 2013, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urbain, P.; Singler, F.; Ihorst, G.; Biesalski, H.K.; Bertz, H. Bioavailability of vitamin D(2) from UV-B-irradiated button mushrooms in healthy adults deficient in serum 25-hydroxyvitamin D: A randomized controlled trial. Eur. J. Clin. Nutr. 2011, 65, 965–971. [Google Scholar] [CrossRef] [Green Version]
- Annweiler, C.; Llewellyn, D.J.; Beauchet, O. Low Serum Vitamin D Concentrations in Alzheimer’s Disease: A Systematic Review and Meta-Analysis. J. Alzheimer Dis. 2013, 33, 659–674. [Google Scholar] [CrossRef] [Green Version]
- Balion, C.; Griffith, L.E.; Strifler, L.; Henderson, M.; Patterson, C.; Heckman, G.; Llewellyn, D.J.; Raina, P. Vitamin D, cognition, and dementia: A systematic review and meta-analysis. Neurology 2012, 79, 1397–1405. [Google Scholar] [CrossRef] [Green Version]
- Etgen, T.; Sander, D.; Bickel, H.; Sander, K.; Förstl, H. Vitamin D Deficiency, Cognitive Impairment and Dementia: A Systematic Review and Meta-Analysis. Dement. Geriatr. Cogn. Disord. 2012, 33, 297–305. [Google Scholar] [CrossRef]
- Van Der Schaft, J.; Koek, H.; Dijkstra, E.; Verhaar, H.; Van Der Schouw, Y.; Emmelot-Vonk, M.; Van Der Schouw, Y.T. The association between vitamin D and cognition: A systematic review. Ageing Res. Rev. 2013, 12, 1013–1023. [Google Scholar] [CrossRef]
- Zhao, Y.; Sun, Y.; Ji, H.F.; Shen, L. Vitamin D levels in Alzheimer’s and Parkinson’s diseases: A meta-analysis. Nutrition 2013, 29, 828–832. [Google Scholar] [CrossRef]
- Annweiler, C.; Montero-Odasso, M.; Llewellyn, D.J.; Richard-Devantoy, S.; Duque, G.; Beauchet, O. Meta-Analysis of Memory and Executive Dysfunctions in Relation to Vitamin D. J. Alzheimer Dis. 2013, 37, 147–171. [Google Scholar] [CrossRef] [Green Version]
- Timpini, A.; Pini, L.; Tantucci, C.; Cossi, S.; Grassi, V. Vitamin D and health status in elderly. Intern. Emerg. Med. 2010, 6, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Rossom, R.C.; Espeland, M.A.; Manson, J.E.; Dysken, M.W.; Johnson, K.C.; Lane, R.S.; Leblanc, E.S.; Lederle, F.A.; Masaki, K.H.; Margolis, K.L. Calcium and vitamin D supplementation and cognitive impairment in the women’s health initiative. J. Am. Geriatr. Soc. 2012, 60, 2197–2205. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, J.A.; Edmondson, D.; Wasson, L.T.; Falzon, L.; Homma, K.; Ezeokoli, N.; Li, P.; Davidson, K.W. Vitamin D Supplementation for Depressive Symptoms: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Psychosom. Med. 2014, 76, 190–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zajac, I.; Cavuoto, P.; Danthiir, V.; Wittert, G.A.; Krause, D.; Lawson, L.; Noakes, M.; Weaver, J.; Bennett, L.E. A randomised, double blinded, placebo-controlled clinical trial testing the effects of a vitamin D-enriched mushroom supplement on cognitive performance and mood in healthy elderly adults: Study protocol. Healthy Aging Res. 2016, 5, 1–14. [Google Scholar] [CrossRef]
- Chai-Coetzer, C.L.; Antic, N.A.; Rowland, L.S.; Catcheside, P.G.; Esterman, A.; Reed, R.L.; Williams, H.; Dunn, S.V.; McEvoy, R.D. A simplified model of screening questionnaire and home monitoring for obstructive sleep apnoea in primary care. Thorax 2011, 66, 213–219. [Google Scholar] [CrossRef] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Bennett, L.; Kersaitis, C.; Macaulay, S.L.; Münch, G.; Niedermayer, G.; Nigro, J.; Payne, M.; Sheean, P.; Vallotton, P.; Zabaras, D.; et al. Vitamin D2-Enriched Button Mushroom (Agaricus bisporus) Improves Memory in Both Wild Type and APPswe/PS1dE9 Transgenic Mice. PLoS ONE 2013, 8, e76362. [Google Scholar] [CrossRef] [Green Version]
- Wesnes, K.A. Assessing cognitive function in clinical trials: Latest developments and future directions. Drug Discov. Today 2002, 7, 29–35. [Google Scholar] [CrossRef]
- Pipingas, A.; Harris, E.; Tournier, E.; King, R.; Kras, M.; Stough, C.K. Assessing the Efficacy of Nutraceutical Interventions on Cognitive Functioning in the Elderly. Curr. Top. Nutraceutical Res. 2010, 8, 79–87. [Google Scholar]
- Barnes, M.B.; Danthiir, V.; Noakes, M.; Macaulay, S.L.; Zajac, I.; Bennett, L.E. Cross-sectional relationships of serum 25-OH-D metabolite of vitamin D with cognition and mood in a cognitively-healthy older cohort. Curr. Psychopharmacol. 2016, 5, 47–60. [Google Scholar] [CrossRef]
- Danthiir, V.; Burns, N.; Nettelbeck, T.; Wilson, C.; Wittert, G. The older people, omega-3, and cognitive health (EPOCH) trial design and methodology: A randomised, double-blind, controlled trial investigating the effect of long-chain omega-3 fatty acids on cognitive ageing and wellbeing in cognitively healthy older adults. Nutr. J. 2011, 10, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crawford, J.R.; Henry, J.D. The Positive and Negative Affect Schedule (PANAS): Construct validity, measurement properties and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2004, 43, 245–265. [Google Scholar] [CrossRef] [PubMed]
- Antony, M.M.; Bieling, P.J.; Cox, B.J.; Enns, M.W.; Swinson, R.P. Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychol. Assess. 1998, 10, 176–181. [Google Scholar] [CrossRef]
- Lyubomirsky, S.; Lepper, H.S. A measure of subjective happiness: Preliminary reliability and construct validation. Soc. Indic. Res. 1999, 46, 137–155. [Google Scholar] [CrossRef]
- Fudge, A.N.; Galettis, P.; O’Loughlin, P.D. Measurement of 25-hydroxyvitamin D by high throughput liquid chromatography tandem mass spectroscopy. Clin. Biochem. Rev. 2012, 33, S34. [Google Scholar]
- Hanwell, H.; Vieth, R.; Cole, D.; Scillitani, A.; Modoni, S.; Frusciante, V.; Ritrovato, G.; Chiodini, I.; Minisola, S.; Carnevale, V. Sun exposure questionnaire predicts circulating 25-hydroxyvitamin D concentrations in Caucasian hospital workers in southern Italy. J. Steroid Biochem. Mol. Biol. 2010, 121, 334–337. [Google Scholar] [CrossRef]
- Battault, S.; Whiting, S.J.; Peltier, S.L.; Sadrin, S.; Gerber, G.; Maixent, J.M. Vitamin D metabolism, functions and needs: From science to health claims. Eur. J. Nutr. 2013, 52, 429–441. [Google Scholar] [CrossRef]
- Stephensen, C.B.; Zerofsky, M.; Burnett, D.J.; Lin, Y.-P.; Hammock, B.D.; Hall, L.M.; McHugh, T. Ergocalciferol from Mushrooms or Supplements Consumed with a Standard Meal Increases 25-Hydroxyergocalciferol but Decreases 25-Hydroxycholecalciferol in the Serum of Healthy Adults. J. Nutr. 2012, 142, 1246–1252. [Google Scholar] [CrossRef] [Green Version]
- Itkonen, S.T.; Skaffari, E.; Saaristo, P.; Saarnio, E.M.; Erkkola, M.; Jakobsen, J.; Cashman, K.D.; Lamberg-Allardt, C. Effects of vitamin D2-fortified bread v. supplementation with D2 or D3 on serum 25-hydroxyvitamin D metabolites: An 8-week randomised-controlled trial in young Finnish women. Br. J. Nutr. 2016, 115, 1232–1239. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, T.E.; Harvey, P.D.; Wesnes, K.A.; Snyder, P.J.; Schneider, L.S. Practice effects due to serial cognitive assessment: Implications for preclinical Alzheimer’s disease randomized controlled trials. Alzheimer Dement. Diagn. Assess. Dis. Monit. 2015, 1, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Jorde, R.; Sneve, M.; Figenschau, Y.; Svartberg, J.; Waterloo, K. Effects of vitamin D supplementation on symptoms of depression in overweight and obese subjects: Randomized double blind trial. J. Intern. Med. 2008, 264, 599–609. [Google Scholar] [CrossRef] [PubMed]
- Khoraminya, N.; Tehrani-Doost, M.; Jazayeri, S.; Hosseini, A.; Djazayery, A. Therapeutic effects of vitamin D as adjunctive therapy to fluoxetine in patients with major depressive disorder. Aust. N. Z. J. Psychiatry 2013, 47, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Ferry, M.; Coley, N.; Andrieu, S.; Bonhomme, C.; Caubère, J.P.; Cesari, M.; Gautry, J.; Sánchez, I.G.; Hugonot, L.; Mansuy, L.; et al. How to design nutritional intervention trials to slow cognitive decline in apparently healthy populations and apply for efficacy claims: A statement from the International Academy on Nutrition and Aging Task Force. J. Nutr. Health Aging 2013, 17, 619–623. [Google Scholar] [CrossRef] [Green Version]
- Lee, G.; Elashoff, D.; Di, L.; Teng, E.; Melchor, S.; Kim, J.; Lu, P.H. P3-238: Age-associated memory impairment increases risk of conversion to MCI and dementia. Alzheimer Dement. 2012, 8, P544. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| VARIABLE | Vitamin D Enhanced Mushroom (n = 93) | Vitamin D3 (n = 91) | Standard Mushroom (n = 94) | Placebo (n = 92) |
|---|---|---|---|---|
| Female, % | 51.6 | 53.8 | 51.1 | 51.1 |
| APOE-ε4 0/1/2, n | 72/21/0 | 72/17/2 | 76/18/0 | 72/18/2 |
| Smoking Behaviour, n | ||||
| Smoker | 0 | 1 | 0 | 0 |
| Ex-Smoker | 17 | 14 | 20 | 12 |
| Never-Smoker | 76 | 76 | 74 | 81 |
| Alcohol Behaviour, n | ||||
| Regular | 69 | 65 | 58 | 0 |
| Rarely | 7 | 2 | 2 | 67 |
| Never | 17 | 24 | 34 | 25 |
| Mean Alcohol Consumption, L/week | 1.5 (1.5) | 1.2 (1.1) | 1.1 (1.0) | 1.3 (1.4) |
| Age in years | 69.7 (6.6) | 70.8 (6.4) | 69.4 (6.7) | 70.1 (5.7) |
| BMI * | 27.5 (4.0) | 28.0 (4.0) | 26.6 (4.0) | 28.2 (4.1) |
| MMSE Score | 28.6 (1.3) | 28.5 (1.4) | 28.4 (1.5) | 28.6 (1.4) |
| Mean Sun Exposure Score | ||||
| Week 0 | 21.4 (10.3) | 21.6 (10.1) | 21.0 (8.6) | 21.5 (11.1) |
| +5 Weeks | 15.4 (8.6) | 16.4 (8.4) | 16.0 (7.3) | 17.8 (10.1) |
| +24 Weeks | 20.1 (10.1) | 22.9 (10.4) | 20.0 (9.1) | 22.8 (9.5) |
| Measure | Visit | D2M | D3 | SM | PL | Model p-Values | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| 25-OH-D | Baseline | 74.64 | ±2.08 | 77.80 | ±1.94 | 77.95 | ±1.92 | 74.13 | ±1.94 | T p < 0.001 Tr p = 0.052 T × Tr p < 0.001 |
| +24 Weeks | 66.76 | ±2.06 | 82.24 | ±1.90 | 64.91 | ±1.88 | 61.91 | ±1.89 | ||
| 25-OH-D3 | Baseline | 74.30 | ±2.09 | 77.57 | ±1.95 | 77.91 | ±1.92 | 74.09 | ±1.95 | T p < 0.001 Tr p < 0.01 T × Tr p < 0.001 |
| +24 Weeks | 47.02 | ±2.07 | 81.95 | ±1.92 | 64.71 | ±1.90 | 61.90 | ±1.90 | ||
| 25-OH-D2 > 5.0 nM | Baseline | 3 | (3.2%) | 3 | (3.3%) | 1 | (1.1%) | 1 | (1.1%) | T p < 0.001 Tr p < 0.001 T × Tr p < 0.001 |
| +24 Weeks | 88 | (94.6%) | 4 | (4.4%) | 3 | (3.2%) | 3 | (3.3%) | ||
| VARIABLE | D2M | D3 | SM | CONTROL | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Male, n | 48 | 42 | 46 | 45 | ||||||
| 25-OHD | Baseline | 75.92 | ±2.53 | 79.12 | ±2.87 | 79.11 | ±2.85 | 72.87 | ±2.49 | |
| +24 Weeks | 66.38 | ±1.92 | 84.67 | ±2.85 | 67.67 | ±3.7 | 60.47 | ±2.45 | ||
| 25-OHD3 | Baseline | 75.57 | ±2.55 | 78.73 | ±2.89 | 78.97 | ±2.88 | 72.7 | ±2.5 | |
| +24 Weeks | 48.95 | ±2.02 | 84.14 | ±2.81 | 67.46 | ±3.75 | 60.34 | ±2.47 | ||
| Female, n | 45 | 49 | 48 | 47 | ||||||
| 25-OHD | Baseline | 70.6 | ±2.97 | 76.8 | ±2.54 | 79.08 | ±2.71 | 75.3 | ±2.76 | |
| +24 Weeks | 64.39 | ±2.26 | 80.26 | ±2.67 | 65.2 | ±2.75 | 63.26 | ±2.76 | ||
| 25-OHD3 | Baseline | 70.42 | ±2.96 | 76.64 | ±2.55 | 79.1 | ±2.7 | 75.32 | ±2.76 | |
| +24 Weeks | 42.09 | ±2.31 | 80.11 | ±2.65 | 64.98 | ±2.76 | 63.28 | ±2.75 | ||
| Deficient, n | 54 | 44 | 40 | 47 | ||||||
| 25-OHD | Baseline | 60.55 | ±1.52 | 62.45 | ±1.57 | 61.65 | ±1.67 | 60.38 | ±1.65 | |
| +24 Weeks | 58.57 | ±1.69 | 72.02 | ±2.26 | 50.71 | ±2.39 | 52.02 | ±1.85 | ||
| 25-OHD3 | Baseline | 60.38 | ±1.54 | 62.27 | ±1.55 | 61.53 | ±1.67 | 60.2 | ±1.63 | |
| +24 Weeks | 38.36 | ±1.52 | 71.88 | ±2.23 | 50.28 | ±2.43 | 51.89 | ±1.83 | ||
| Sufficient, n | 39 | 47 | 54 | 45 | ||||||
| 25-OHD | Baseline | 90.69 | ±1.97 | 91.77 | ±1.7 | 92.02 | ±1.66 | 88.75 | ±1.59 | |
| +24 Weeks | 74.71 | ±1.65 | 91.55 | ±2.42 | 77.68 | ±2.61 | 72.66 | ±2.42 | ||
| 25-OHD3 | Baseline | 90.52 | ±1.95 | 91.42 | ±1.77 | 92 | ±1.67 | 88.79 | ±1.58 | |
| +24 Weeks | 55.77 | ±2.14 | 91.07 | ±2.39 | 77.62 | ±2.62 | 72.7 | ±2.41 | ||
| COGNITIVE MEASURE | D2M | D3 | SM | PL | Model p | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Reaction Time | Week 0 | 1.56 | ±0.03 | 1.55 | ±0.03 | 1.5 | ±0.03 | 1.55 | ±0.03 | T p < 0.001 |
| +5 Weeks | 1.58 | ±0.03 | 1.57 | ±0.04 | 1.57 | ±0.03 | 1.6 | ±0.03 | Tr p = 0.65 | |
| +24 Weeks | 1.61 | ±0.03 | 1.61 | ±0.04 | 1.57 | ±0.03 | 1.59 | ±0.03 | T × Tr p = 0.82 | |
| Speed of Processing | Week 0 | 0.49 | ±0.01 | 0.5 | ±0.01 | 0.47 | ±0.01 | 0.48 | ±0.01 | T p < 0.001 |
| +5 Weeks | 0.5 | ±0.01 | 0.51 | ±0.01 | 0.48 | ±0.01 | 0.5 | ±0.01 | Tr p = 0.10 | |
| +24 Weeks | 0.5 | ±0.01 | 0.51 | ±0.01 | 0.48 | ±0.01 | 0.5 | ±0.01 | T × Tr p = 0.51 | |
| Speed of Reasoning | Week 0 | 0.8 | ±0.02 | 0.79 | ±0.02 | 0.73 | ±0.02 | 0.79 | ±0.02 | T p < 0.001 |
| +5 Weeks | 0.85 | ±0.02 | 0.83 | ±0.03 | 0.77 | ±0.02 | 0.83 | ±0.02 | Tr p = 0.21 | |
| +24 Weeks | 0.86 | ±0.03 | 0.86 | ±0.02 | 0.8 | ±0.02 | 0.83 | ±0.02 | T × Tr p = 0.77 | |
| Speed of Memory Scanning | Week 0 | 0.75 | ±0.02 | 0.73 | ±0.02 | 0.7 | ±0.02 | 0.72 | ±0.02 | T p < 0.001 |
| +5 Weeks | 0.77 | ±0.02 | 0.75 | ±0.02 | 0.72 | ±0.02 | 0.75 | ±0.02 | Tr p = 0.39 | |
| +24 Weeks | 0.77 | ±0.02 | 0.74 | ±0.02 | 0.74 | ±0.02 | 0.74 | ±0.02 | T × Tr p = 0.47 | |
| Recognition Speed | Week 0 | 0.6 | ±0.02 | 0.61 | ±0.02 | 0.56 | ±0.01 | 0.59 | ±0.02 | T p < 0.001 |
| +5 Weeks | 0.6 | ±0.02 | 0.59 | ±0.02 | 0.56 | ±0.01 | 0.58 | ±0.02 | Tr p = 0.39 | |
| +24 Weeks | 0.65 | ±0.02 | 0.63 | ±0.02 | 0.59 | ±0.02 | 0.63 | ±0.01 | T × Tr p = 0.43 | |
| Verbal Working Memory | Week 0 | 0.79 | ±0.02 | 0.82 | ±0.02 | 0.74 | ±0.02 | 0.79 | ±0.02 | T p = 0.06 |
| +5 Weeks | 0.8 | ±0.02 | 0.83 | ±0.02 | 0.78 | ±0.02 | 0.83 | ±0.02 | Tr p = 0.05 | |
| +24 Weeks | 0.82 | ±0.02 | 0.8 | ±0.02 | 0.76 | ±0.02 | 0.82 | ±0.02 | T × Tr p = 0.04 | |
| Spatial Working Memory | Week 0 | 0.32 | ±0.02 | 0.29 | ±0.01 | 0.27 | ±0.01 | 0.3 | ±0.01 | T p < 0.001 |
| +5 Weeks | 0.29 | ±0.01 | 0.29 | ±0.01 | 0.28 | ±0.01 | 0.26 | ±0.01 | Tr p = 0.32 | |
| +24 Weeks | 0.36 | ±0.02 | 0.33 | ±0.01 | 0.33 | ±0.01 | 0.33 | ±0.01 | T × Tr p = 0.59 | |
| Overall Quality of Memory Performance | Week 0 | 0.79 | ±0.01 | 0.78 | ±0.01 | 0.76 | ±0.01 | 0.78 | ±0.01 | T p = 0.12 |
| +5 Weeks | 0.77 | ±0.01 | 0.76 | ±0.01 | 0.75 | ±0.01 | 0.75 | ±0.01 | Tr p = 0.13 | |
| +24 Weeks | 0.8 | ±0.01 | 0.78 | ±0.01 | 0.77 | ±0.01 | 0.78 | ±0.01 | T × Tr p = 0.58 | |
| D2M | D3 | SM | PL | Model p | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ANXIETY | Week 0 | 2.52 | ±0.26 | 3.1 | ±0.39 | 3.04 | ±0.34 | 3.13 | ±0.4 | T p = 0.46 |
| +5 Weeks | 2.77 | ±0.27 | 2.94 | ±0.4 | 2.57 | ±0.33 | 2.91 | ±0.4 | Tr p = 0.86 | |
| +24 Weeks | 2.63 | ±0.29 | 3.53 | ±0.47 | 3.08 | ±0.39 | 2.87 | ±0.44 | T × Tr p = 0.43 | |
| DEPRESSION | Week 0 | 4.31 | ±0.42 | 4.52 | ±0.59 | 4.44 | ±0.55 | 3.91 | ±0.47 | T p = 0.17 |
| +5 Weeks | 3.7 | ±0.39 | 4.18 | ±0.45 | 4.07 | ±0.41 | 3.54 | ±0.44 | Tr p = 0.95 | |
| +24 Weeks | 4.06 | ±0.48 | 4.29 | ±0.52 | 4.26 | ±0.51 | 3.39 | ±0.42 | T × Tr p = 0.97 | |
| STRESS | Week 0 | 7.46 | ±0.6 | 6.58 | ±0.55 | 7.93 | ±0.58 | 8.15 | ±0.61 | T p = 0.04 |
| +5 Weeks | 7.75 | ±0.59 | 7.21 | ±0.67 | 7.43 | ±0.54 | 7.7 | ±0.77 | Tr p = 0.61 | |
| +24 Weeks | 7.14 | ±0.62 | 6.25 | ±0.61 | 7.11 | ±0.56 | 7.52 | ±0.59 | T × Tr p = 0.92 | |
| POSITIVE AFFECT | Week 0 | 33.16 | ±0.91 | 34.53 | ±0.93 | 31.18 | ±0.84 | 34.57 | ±0.71 | T p = 0.37 |
| +5 Weeks | 32.7 | ±0.79 | 33.58 | ±1 | 31.66 | ±0.85 | 33.89 | ±0.74 | Tr p = 0.12 | |
| +24 Weeks | 33.56 | ±0.8 | 34.73 | ±0.92 | 31.8 | ±0.92 | 35.43 | ±0.73 | T × Tr p = 0.54 | |
| NEGATIVE AFFECT | Week 0 | 12.18 | ±0.49 | 11.1 | ±0.21 | 11.21 | ±0.28 | 11.68 | ±0.39 | T p = 0.004 |
| +5 Weeks | 11.89 | ±0.48 | 11.01 | ±0.17 | 10.92 | ±0.2 | 11.24 | ±0.29 | Tr p = 0.06 | |
| +24 Weeks | 10.82 | ±0.18 | 11.13 | ±0.31 | 10.65 | ±0.13 | 11.4 | ±0.31 | T × Tr p = 0.19 | |
| HAPPINESS | Week 0 | 5.66 | ±0.1 | 6.19 | ±0.52 | 6.14 | ±0.44 | 5.52 | ±0.1 | T p = 0.29 |
| +5 Weeks | 5.94 | ±0.16 | 5.57 | ±0.1 | 5.68 | ±0.11 | 5.61 | ±0.09 | Tr p = 0.45 | |
| +24 Weeks | 5.92 | ±0.18 | 5.7 | ±0.09 | 5.73 | ±0.1 | 5.7 | ±0.08 | T × Tr p = 0.45 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zajac, I.T.; Barnes, M.; Cavuoto, P.; Wittert, G.; Noakes, M. The Effects of Vitamin D-Enriched Mushrooms and Vitamin D3 on Cognitive Performance and Mood in Healthy Elderly Adults: A Randomised, Double-Blinded, Placebo-Controlled Trial. Nutrients 2020, 12, 3847. https://doi.org/10.3390/nu12123847
Zajac IT, Barnes M, Cavuoto P, Wittert G, Noakes M. The Effects of Vitamin D-Enriched Mushrooms and Vitamin D3 on Cognitive Performance and Mood in Healthy Elderly Adults: A Randomised, Double-Blinded, Placebo-Controlled Trial. Nutrients. 2020; 12(12):3847. https://doi.org/10.3390/nu12123847
Chicago/Turabian StyleZajac, Ian T., Mary Barnes, Paul Cavuoto, Gary Wittert, and Manny Noakes. 2020. "The Effects of Vitamin D-Enriched Mushrooms and Vitamin D3 on Cognitive Performance and Mood in Healthy Elderly Adults: A Randomised, Double-Blinded, Placebo-Controlled Trial" Nutrients 12, no. 12: 3847. https://doi.org/10.3390/nu12123847
APA StyleZajac, I. T., Barnes, M., Cavuoto, P., Wittert, G., & Noakes, M. (2020). The Effects of Vitamin D-Enriched Mushrooms and Vitamin D3 on Cognitive Performance and Mood in Healthy Elderly Adults: A Randomised, Double-Blinded, Placebo-Controlled Trial. Nutrients, 12(12), 3847. https://doi.org/10.3390/nu12123847