Effect of Overeating Dietary Protein at Different Levels on Circulating Lipids and Liver Lipid: The PROOF Study



Abstract
:1. Introduction
2. Methods and Materials
2.1. Participants
2.2. Protocol
2.3. Diets
2.4. Body Composition
2.5. Measurement of Adipose Tissue Volumes and Liver Fat
2.6. Adipose Tissue Biopsy for Fat Cell Size
2.7. Laboratory Measurements
3. Statistical Analysis
4. Results
4.1. Associations with Dietary Protein Assignment
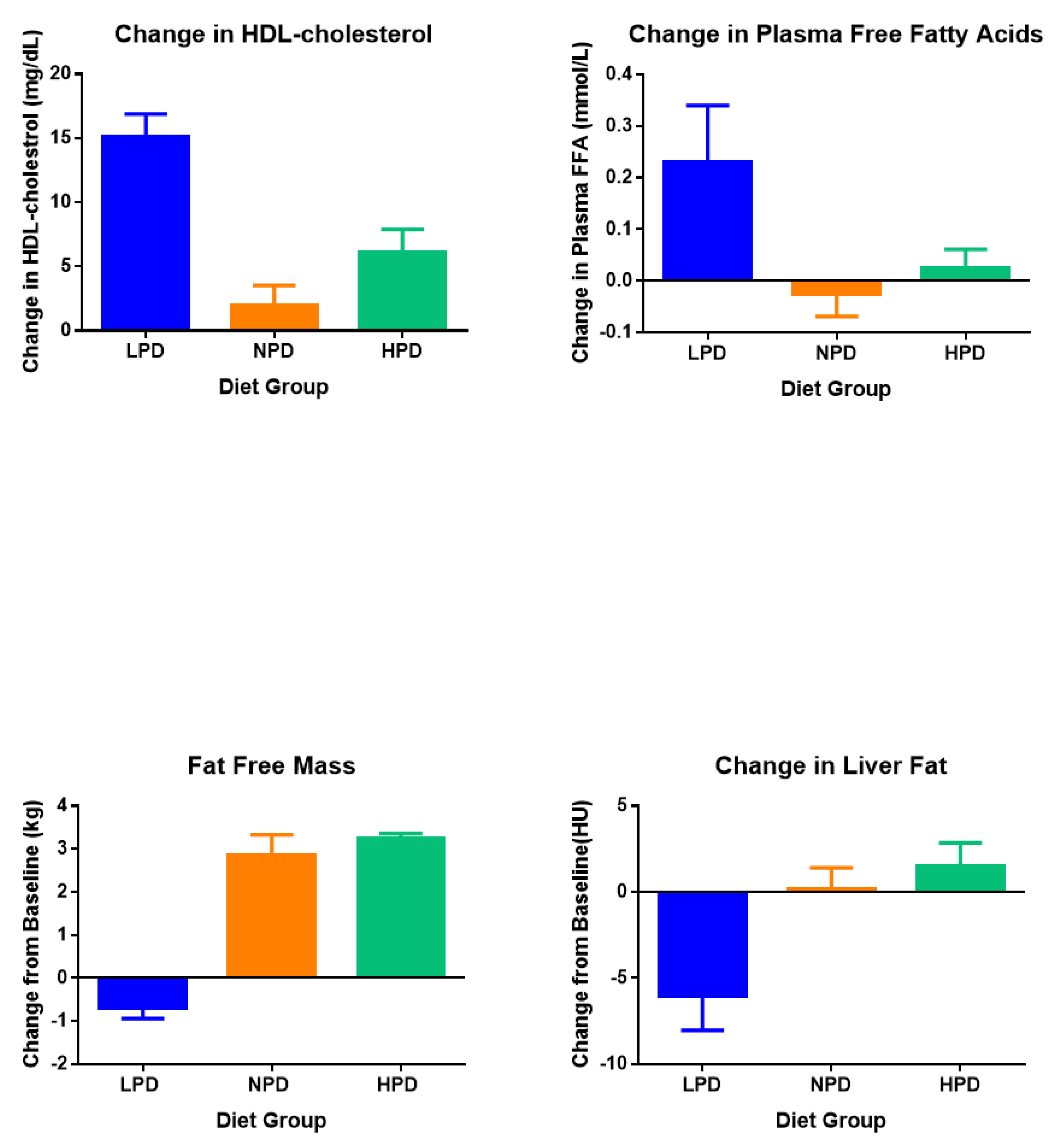
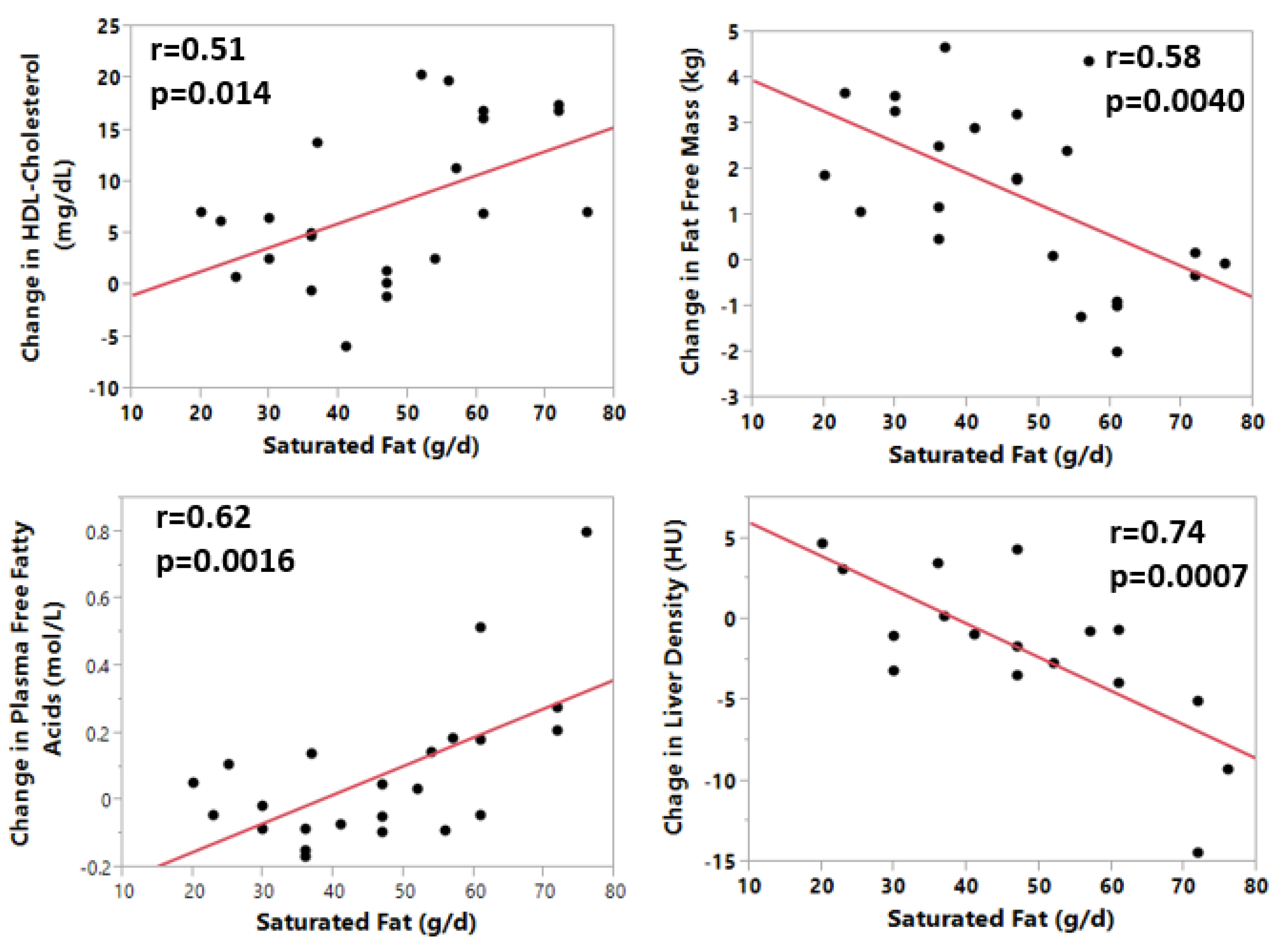
4.2. Effects of Dietary Fat on HDL-Cholesterol, Total Cholesterol, Free Fatty Acids, and Liver Fat
5. Discussion
5.1. Overall Effects of Overfeeding
5.2. Overfed Protein
5.3. Overfed Fat
Author Contributions
Funding
Conflicts of Interest
References
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Berrington de Gonzalez, A.; Hartge, P.; Cerhan, J.R.; Flint, A.J.; Hannan, L.; Maclnnis, R.J.; Moore, S.C.; Tobias, G.S.; Anton-Culver, H.; Freeman, L.B.; et al. Body-mass index andmortality among 1.46 million white adults. N. Eng. J. Med. 2010, 363, 2211–2219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, G.A.; Heisel, W.E.; Afshin, A.; Jensen, M.D.; Dietz, W.H.; Long, M.; Kushner, R.F.; Daniels, S.R.; Wadden, T.A.; Tsai, A.G.; et al. The science of obesity management: An endocrine society scientific statement. Endocr. Rev. 2018, 39, 79–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sims, E.A.; Goldman, R.F.; Gluck, C.M.; Horton, E.S.; Kelleher, P.C.; Rowe, D.W. Experimental obesity in man. Trans. Assoc. Am. Phys. 1968, 81, 153–170. [Google Scholar] [PubMed]
- Bray, G.A.; Bouchard, C. The biology of human overfeeding: A systematic analysis. Obes. Rev. 2020, 9, e13040. [Google Scholar]
- Stock, M.J. Gluttony and thermogenesis revisited. Int. J. Obes. Relat. Metab. Disord. 1999, 23, 1105–1117. [Google Scholar] [CrossRef] [Green Version]
- Dulloo, A.G.; Jacquet, J. Low-protein overfeeding: A tool to unmask susceptibility to obesity in humans. Int. Obes. Relat. Metab. Disord. 1999, 23, 1118–1121. [Google Scholar] [CrossRef] [Green Version]
- Bray, G.A.; Smith, S.R.; de Jonge, L. Effect of dietary protein content on weight gain, energy expenditure, and body composition during overeating: A randomized controlled trial. JAMA 2012, 307, 47–55. [Google Scholar] [CrossRef] [Green Version]
- Bray, G.A.; Redman, L.M.; de Jonge, L.; Rood, J.; Sutton, E.F.; Smith, S.R. Plasma amino acids during 8 weeks of overfeeding: Relation to diet body composition and fat cell size in the PROOF Study. Obesity (Silver Spring) 2018, 26, 324–331. [Google Scholar] [CrossRef] [Green Version]
- Bray, G.A.; Redman, L.M.; de Jonge, L.; Rood, J.; Sutton, E.F.; Smith, S.R. Plasma fatty acyl-carnitines during 8 Weeks of overfeeding: Relation to diet energy expenditure and body composition: The PROOF study. Metabolism 2018, 83, 1–10. [Google Scholar] [CrossRef]
- Joosen, A.M.; Bakker, A.H.; Westerterp, K.R. Metabolic efficiency and energy expenditure during short-term overfeeding. Physiol. Behav. 2005, 85, 593–597. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.S.; Mumford, P. Gluttony. 1. An experimental study of overeating low- or high-protein diets. Am. J. Clin. Nutr. 1967, 20, 1212–1222. [Google Scholar] [CrossRef] [PubMed]
- Apolzan, J.W.; Bray, G.A.; Smith, S.R.; de Jonge, L.; Rood, J.; Han, H.; Redman, L.M.; Martin, C.K. Effects of weight gain induced by controlled overfeeding on physical activity. Am. J. Physiol. Endocrinol. Metab. 2014, 307, E1030–E1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, G.A.; Redman, L.M.; de Jonge, L.; Covington, J.; Rood, J.; Brock, C.; Mancuso, S.; Martin, C.K.; Smiths, S.R. Effect of protein overfeeding on energy expenditure measured in a metabolic chamber. Am. J. Clin. Nutr. 2015, 101, 496–505. [Google Scholar] [CrossRef] [Green Version]
- Bray, G.A.; Redman, L.M.; de Jonge, L.; Rood, J.; Smith, S.R. Effect of three levels of dietary protein on metabolic phenotype of healthy individuals with 8 weeks of overfeeding. J. Clin. Endocrinol. Metab. 2016, 101, 2836–2843. [Google Scholar] [CrossRef] [PubMed]
- Sutton, E.F.; Bray, G.A.; Burton, J.H.; Smith, S.R.; Redman, L.M. No evidence for metabolic adaptation in thermic effect of food by dietary protein. Obesity (Silver Spring) 2016, 24, 1639–1642. [Google Scholar] [CrossRef] [Green Version]
- Kelley, D.E.; Thaete, F.L.; Troost, F.; Huwe, T.; Goodpaster, B.H. Subdivision of subcutaneous abdominal adipose tissue and insulin resistance. Am. J. Physiol. Endocrinol. Metab. 2000, 278, E941–E948. [Google Scholar] [CrossRef]
- Smith, S.R.; Lovejoy, J.C.; Greenway, F.; Ryan, D.; de Jonge, L.; de la Bretonne, J.; Volafova, J.; Bray, G.A. Contributions of total body fat, abdominal subcutaneous adipose tissue compartments, and visceral adipose tissue to the metabolic complications of obesity. Metabolism 2001, 50, 425–435. [Google Scholar] [CrossRef]
- Sims, E.A.; Horton, E.S. Endocrine and metabolic adaptation to obesity and starvation. Am. J. Clin. Nutr. 1968, 21, 1455–1470. [Google Scholar] [CrossRef]
- Teran-Garcia, M.; Despres, J.P.; Couillard, C.; Tremblay, A.; Bouchard, C. Effects of long-term overfeeding on plasma lipoprotein levels in identical twins. Atherosclerosis 2004, 173, 277–283. [Google Scholar] [CrossRef]
- Magkos, F.; Smith, G.I.; Reeds, D.N.; Okunade, A.; Patterson, B.W.; Mittendorfer, B. One day of overfeeding impairs nocturnal glucose but not fatty acid homeostasis in overweight men. Obesity (Silver Spring) 2014, 22, 435–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, N.; Jensen, M.D. Clinical effects of high-fat meals and weight gain due to high-fat feeding. Int. J. Obes. Suppl. 2012, 2 (Suppl. 2), S51–S55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orr, J.S.; Gentile, C.L.; Davy, B.M.; Davy, K.P. Large artery stiffening with weight gain in humans: Role of visceral fat accumulation. Hypertension 2008, 51, 1519–1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iggman, D.; Rosqvist, F.; Larsson, A.; Arnlow, J.; Beckman, L.; Rudling, M.; Riserus, U. Role of dietary fats in modulating cardiometabolic risk during moderate weight gain: A randomized double-blind overfeeding trial (LIPOGAIN study). J. Am. Heart Assoc. 2014, 3, e001095. [Google Scholar] [CrossRef] [Green Version]
- Johannsen, D.L.; Tchoukalova, Y.; Tam, C.S.; Covington, J.D.; Xie, W.; Schwarz, J.-M.; Bajpeyi, S.; Ravussin, E. Effect of 8 weeks of overfeeding on ectopic fat deposition and insulin sensitivity: Testing the adipose tissue expandability hypothesis. Diabetes Care 2014, 37, 2789–2797. [Google Scholar] [CrossRef] [Green Version]
- Gentile, C.L.; Orr, J.S.; Davy, B.M.; Davy, K.P. Cardiorespiratory fitness influences the blood pressure response to experimental weight gain. Obesity (Silver Spring) 2007, 15, 3005–3012. [Google Scholar] [CrossRef] [Green Version]
- Fabbrini, E.; Yoshino, J.; Yoshino, M.; Magkos, F.; Luecking, C.T.; Samovski, D.; Fratterigo, G.; Okunade, L.A.; Patterson, B.W.; Klein, S. Metabolically normal obese people are protected from adverse effects following weight gain. J. Clin. Investig. 2015, 125, 787–795. [Google Scholar] [CrossRef] [Green Version]
- National Academy of Sciences. Dietary Reference Intakes: The Essential Guide to Nutrient Requirements; National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Rosqvist, F.; Iggman, D.; Kullberg, J.; Cedernaes, J.; Johansson, H.-E.; Larsson, A.; Johansson, L.; Ahlstrom, H.; Arner, P.; Dahlman, I. Overfeeding polyunsaturated and saturated fat causes distinct effects on liver and visceral fat accumulation in humans. Diabetes 2014, 63, 2356–2368. [Google Scholar] [CrossRef] [Green Version]
- Seyssel, K.; Alligier, M.; Meugnier, E.; Chanseaume, E.; Loizon, E.; Canto, C.; Disse, E.; Lambert-Porcheron, S.; Brozek, J.; Blond, E. Regulation of energy metabolism and mitochondrial function in skeletal muscle during lipid overfeeding in healthy men. J. Clin. Endocrinol. Metab. 2014, 99, E1254–E1262. [Google Scholar] [CrossRef] [Green Version]
- Fabbrini, E.; Magkos, F.; Mohammed, B.S.; Pietka, T.; Abumrad, N.A.; Patterson, B.W.; Okunade, A.; Klein, S. Intrahepatic fat, not visceral fat, is linked with metabolic complications of obesity. Proc. Natl. Acad. Sci. USA 2009, 106, 15430–15435. [Google Scholar] [CrossRef] [Green Version]
- Bortolotti, M.; Kreis, R.; Debard, C.; Cariou, B.; Faeh, D.; Chetiveaux, M.; Ith, M.; Stefanoni, N.; Le, K.-A.; Schneiter, P. High protein intake reduced intrahepatoceular lipid deposition in humans. Am. J. Clin. Nutr. 2009, 90, 1002–1010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theytaz, F.; Noguchi, Y.; Egli, L.; Campos, V.; Buehler, T.; Hodson, L.; Patterson, B.W.; Nishikata, N.; Kreis, R. Effects of supplementation with essential amino acids on intraheatic lipid concentrations during fructose overfeeding in humans. Am. J. Clin. Nutr. 2012, 96, 1008–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Variable | LPD | NPD | HPD | p by ANOVA |
|---|---|---|---|---|
| Number of Participants (M/F) | 8 (5M/3F) | 9 (6M/3F) | 6 (3M/3F) | |
| Age (years) | 22.9 + 0.97 | 22.9 + 1.83 | 27.2 + 0.87 | 0.043 |
| Weight (kg) | 68.6 + 4.73 | 79.2 + 5.47 | 75.8 + 6.28 | 0.39 |
| Calories fed (kcal/d) | 3130 ± 129 * | 3508 ± 228 | 3501 ± 309 | 0.14 |
| Percent overfed | 38 ± 3% | 42 ± 3% | 39 ± 5% | 0.15 |
| Carbohydrate Intake (g/d)(%) | 341 ± 13 (39%) | 369 ± 24 (46%) | 378 ± 38 (45%) | 0.57 |
| Protein Intake (g/d)(%) | 46.6 ± 1.66 (5%) | 140.0 ± 9.62 (14%) | 231.5 ± 23.0 (25%) | <0.0001 |
| Total Fat (g/d)(%) | 186 ± 7.1 (56%) | 170.9 ± 10.8 (39%) | 132 ± 11.1 (29%) | 0.0054 |
| Saturated Fat (g/d) | 63.9 ± 3.0 | 44.6 ± 2.62 | 27.5 ± 2.49 | <0.0001 |
| Monounsaturated fat (g/d) | 48.9 ± 2.1 | 45.8 ± 3.13 | 27.8 ± 2.56 | <0.0001 |
| Polyunsaturated fat (g/d) | 30.4 ± 0.80 | 30.0 ± 1.76 | 15.3 ± 1.52 | <0.0001 |
| Variable | LPD | NPD | HPD | p for ANOVA | Overall p Value | |||
|---|---|---|---|---|---|---|---|---|
| Baseline | Change | Baseline | Change | Baseline | Change | |||
| Weight (kg) | 68.6 ± 4.7 | 3.17 ± 0.46c | 79.2 ± 5.95 | 6.26 ± 0.46c | 75.8 ± 6.3 | 7.0 ± 0.49d | =0.0028 | <0.0001 |
| Body Fat (kg) | 16.6 ± 1.8 | 3.65 ± 0.32d | 18.3 ± 2.5 | 3.45 ± 0.50b | 21.2 ± 2.7 | 3.62 ± 0.34d | =0.86 | <0.0001 |
| FFM (kg) | 53.2 ± 3.65 | −0.70 ± 0.24 | 59.9 ± 4.2 | 2.86 ± 0.47b | 56.2 ± 64 | 3.24 ± 0.12c | <0.0001 | 0.0011 |
| VAT (kg) | 1.56 ± 0.31 | 0.51 ± 0.088b | 1.58 ± 0.32 | 0.39 ± 0.11a | 2.6 ± 0.63 | 0.47 ± 0.11c | =0.63 | 0.0091 |
| DSAT (kg) | 1.31 ± 0.49 | 0.63 ± 0.21a | 1.31 ± 0.56 | 0.59 ± 0.21a | 1.8 ± 0.61 | 0.72 ± 0.16b | =0.90 | <0.0001 |
| SSAT (kg) | 4.21 ± 0.75 | 1.31 ± 0.21c | 4.21 ± 0.90 | 1.14 ± 0.095d | 5.0 ± 0.85 | 1.3 ± 0.06d | =0.63 | <0.0001 |
| Fat Cell Size (µL) | 0.59 ± 0.068 | 0.20 ± 0.10 | 0.61 ± 0.10 | 0.11 ± 0.073 | 0.64 ± 0.10 | 0.13 ± 0.06 | =0.92 | 0.0041 |
| Liver Density (HU) | 68.2 ± 4.65 | −6.02 ± 2.05c | 66.4 ± 2.78 | 0.17 ± 1.24 | 64.7 ± 5.4 | 1.49 ± 1.37 | =0.010 | 0.23 |
| Chol (mg/dL) | 161 ± 8.6 | 31.2 ± 6.5b | 163 ± 10.7 | 1.28 ± 1.3 | 182 ± 7.8 | 13.1 ± 6.0 | =0.015 | 0.0047 |
| Chol:HDL | 3.83 ± 0.30 | 2.42 ± 2.29a | 3.87 ± 0.28 | 7.54 ± 2.16a | 3.71 ± 0.35 | 2.95 ± 2.65 | =0.23 | 0.0034 |
| HDL (mg/dL) | 42.3 ± 2.2 | 15.1 ± 1.80d | 43.7 ± 2.1 | 1.96 ± 1.56 | 50.4 ± 3.8 | 6.1 ± 1.8a | <0.0001 | <0.0001 |
| LDL (mg/dL) | 94.6 ± 6.5 | 21.8 ± 6.3b | 97.7 ± 8.6 | 1.83 ± 6.3 | 110.1 ± 6.5 | 13.6 ± 6.2 | =0.088 | 0.0068 |
| LDL:HDL | 2.26 ± 0.21 | 1.77 ± 2.18 | 2.31 ± 0.20 | 2.28 ± 2.05 | 2.25 ± 0.24 | 3.55 ± 2.52 | =0.86 | 0.16 |
| TG (mg/dL) | 118 ± 11.1 | −28.9 ± 8.0 | 112 ± 25.7 | −13.2 ± 6.8 | 106 ± 15.3 | −33.5 ± 5.66b | =0.13 | <0.0001 |
| FFA (mmol/L) | 0.29 ± 0.038 | 0.23 ± 0.11 | 0.32 ± 0.027 | −0.027 ± 0.042 | 0.29 ± 0.06 | 0.025 ± 0.036 | =0.035 | 0.13 |
| Glucose (mg/dL) | 85.2 ± 2.91 | 4.0 ± 1.1b | 84.5 ± 2.64 | 4.44 ± 2.66 | 84.5 ± 1.2 | 4.8 ± 3.1 | =0.97 | 0.0030 |
| Insulin (µU/mL) | 11.6 ± 1.7 | 1.6 ± 1.35 | 13.0 ± 3.02 | 1.24 ± 1.02 | 12.7 ± 2.43 | 1.15 ± 2.04 | =0.59 | 0.014 |
| Leptin (ng/dL) | 11.6 ± 3.4 | 8.7 ± 2.3b | 14.1 ± 4.7 | 5.9 ± 1.30b | 20.1 ± 5.1 | 8.25 ± 1.65b | =0.50 | <0.0001 |
| SBP (mmHg) | 103 ± 3.1 | 8.7 ± 2.3 | 106 ± 2.1 | 8.88 ± 3.5a | 107 ± 2.3 | 12.1 ± 4.3a | =0.80 | =0.0002 |
| DBP (mmHg) | 67 ± 2.6 | 4.25 ± 2.61 | 7.0 ± 2.1 | 2.48 ± 2.8 | 70 ± 3.5 | 4.0 ± 3.0 | =0.88 | =0.036 |
| Variable | Total Fat | SFA | MUFA | PUFA | ||||
|---|---|---|---|---|---|---|---|---|
| r | p | r | p | r | p | r | p | |
| Weight (kg) | 0.11 | 0.65 | −0.11 | 0.13 | 0.00 | 0.97 | −0.044 | 0.76 |
| Body Fat (kg) | 0.49 | 0.033 | 0.29 | 0.23 | 0.39 | 0.095 | 0.35 | 0.19 |
| FFM (kg) | −0.39 | 0.61 | −0.58 | 0.0093 | −0.21 | 0.23 | −0.24 | 0.18 |
| VAT (kg) | 0.49 | 0.038 | 0.34 | 0.17 | 0.38 | 0.12 | 0.24 | 0.31 |
| DSAT (kg) | −0.024 | 0.93 | −0.12 | 0.64 | −0.086 | 0.75 | 0.11 | 0.67 |
| SSAT (kg) | −0.058 | 0.79 | −0.070 | 0.77 | −0.13 | 0.61 | −0.14 | 0.58 |
| Fat Cell Size µL | 0.096 | 0.84 | 0.14 | 0.65 | 0.050 | 0.92 | −0.030 | 0.82 |
| Liver Density (HU) | −0.64 | 0.0046 | −0.74 | 0.0008 | −0.59 | 0.013 | −0.49 | 0.045 |
| Cholesterol (mg/dL) | 0.25 | 0.25 | 0.36 | 0.090 | 0.18 | 0.40 | 0.14 | 0.52 |
| HDL:LDL | −0.091 | 0.68 | −0.02 | 0.93 | −0.045 | 0.84 | 0.014 | 0.95 |
| HDL (mg/dL) | 0.31 | 0.16 | 0.51 | 0.014 | 0.24 | 0.28 | 0.18 | 0.40 |
| LDL (mg/dL) | 0.11 | 0.60 | 0.20 | 0.36 | 0.054 | 0.80 | 0.020 | 0.92 |
| TG (mg/dL) | 0.27 | 0.21 | 0.20 | 0.53 | 0.34 | 0.12 | 0.34 | 0.11 |
| FFA (mmol/L) | 0.56 | 0.0056 | 0.62 | 0.0016 | 0.48 | 0.0184 | 0.37 | 0.083 |
| Glucose (mg/dL) | 0.22 | 0.31 | 0.08 | 0.71 | 0.18 | 0.42 | 0.12 | 0.59 |
| Insulin (µU/mL) | 0.10 | 0.65 | 0.069 | 0.75 | 0.14 | 0.54 | 0.94 | 0.67 |
| Leptin (ng/mL) | −0.37 | 0.078 | −0.16 | 0.46 | −0.34 | 0.11 | −0.28 | 0.18 |
| SBP (mmHg) | 0.016 | 0.81 | −0.026 | 0.90 | 0.006 | 0.99 | −0.05 | 0.82 |
| DBP (mmHg) | 0.35 | 0.10 | 0.20 | 0.35 | 0.27 | 0.22 | 0.23 | 0.29 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bray, G.A.; Redman, L.M.; Rood, J.; de Jonge, L.; Smith, S.R. Effect of Overeating Dietary Protein at Different Levels on Circulating Lipids and Liver Lipid: The PROOF Study. Nutrients 2020, 12, 3801. https://doi.org/10.3390/nu12123801
Bray GA, Redman LM, Rood J, de Jonge L, Smith SR. Effect of Overeating Dietary Protein at Different Levels on Circulating Lipids and Liver Lipid: The PROOF Study. Nutrients. 2020; 12(12):3801. https://doi.org/10.3390/nu12123801
Chicago/Turabian StyleBray, George A., Leanne M. Redman, Jennifer Rood, Lilian de Jonge, and Steven R. Smith. 2020. "Effect of Overeating Dietary Protein at Different Levels on Circulating Lipids and Liver Lipid: The PROOF Study" Nutrients 12, no. 12: 3801. https://doi.org/10.3390/nu12123801
APA StyleBray, G. A., Redman, L. M., Rood, J., de Jonge, L., & Smith, S. R. (2020). Effect of Overeating Dietary Protein at Different Levels on Circulating Lipids and Liver Lipid: The PROOF Study. Nutrients, 12(12), 3801. https://doi.org/10.3390/nu12123801