The Efficacy of an Energy-Restricted Anti-Inflammatory Diet for the Management of Obesity in Younger Adults

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Design
2.3. Intervention
2.4. Anthropometry and Body Composition
2.5. Cardiometabolic Parameters
2.6. Inflammatory Parameters
2.7. The Inflammatory Potential of the Diet
2.8. The Outcomes
2.9. Statistical Analysis
3. Results
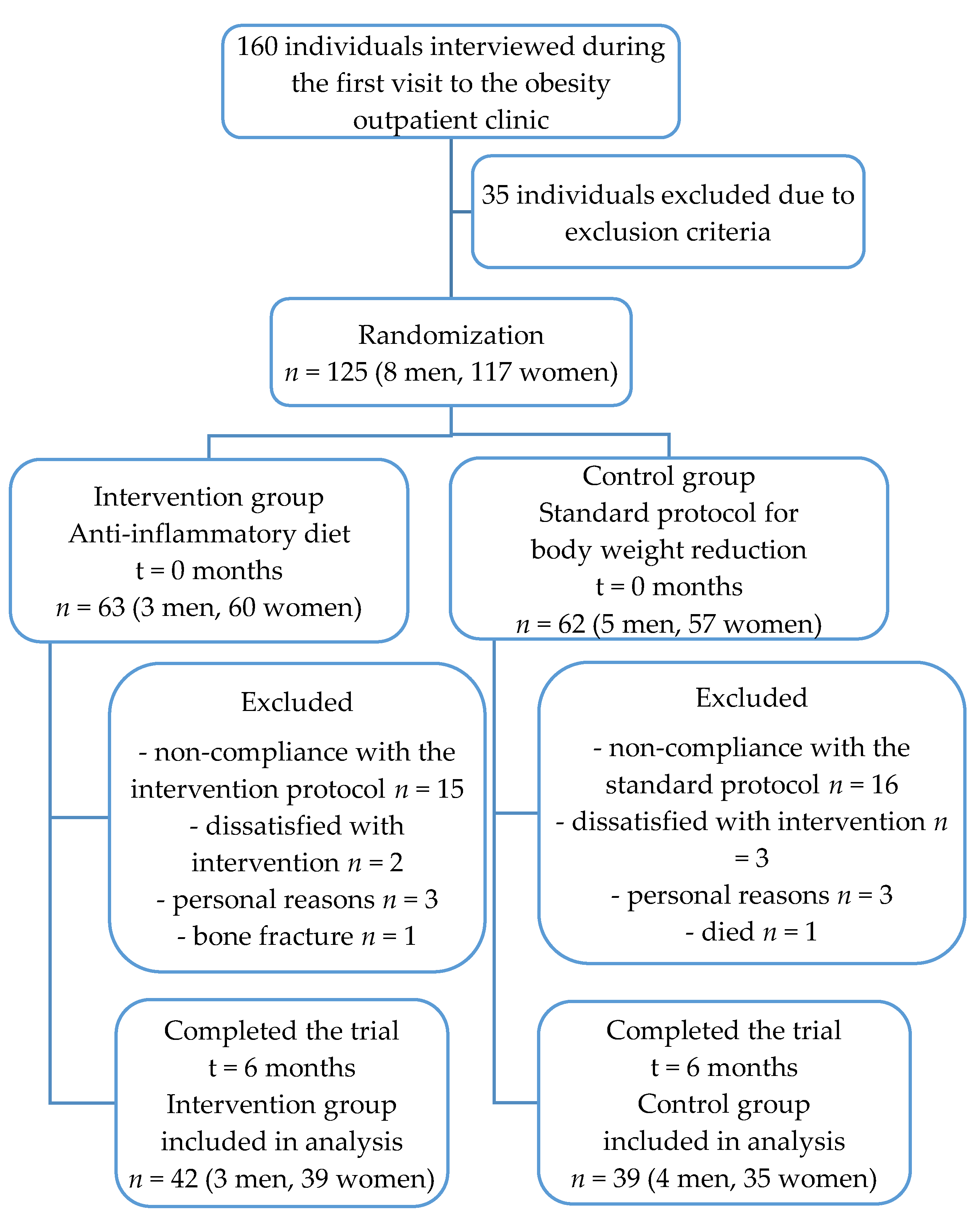
3.1. Study Participants
3.2. Effect of Dietary Intervention on Diet Quality
3.3. Effects of the Dietary Intervention on Anthropometric and Body Composition Parameters
3.4. Effect of the Dietary Interventions on the Cardiometabolic and Inflammatory Statuses
3.5. Associations Between the Inflammatory Potential of the Diet and the Anthropometric, Cardiometabolic, and Inflammatory Parameters
4. Discussion
4.1. The Effect of the Dietary Interventions on Diet Quality Changes
4.2. The Effect of the Dietary Interventions on the Anthropometric and Body Composition Parameters
4.3. Effect of the Dietary Interventions on the Cardiometabolic and Inflammatory Statuses
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Frühbeck, G.; Toplak, H.; Woodward, E.; Yumuk, V.; Maislos, M.; Oppert, J.M. Executive Committee of the European Association for the Study of Obesity. Obesity: The gateway to ill health—An EASO position statement on a rising public health, clinical and scientific challenge in Europe. Obes. Facts 2013, 6, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H. Obesity Management Task Force of the European Association for the Study of Obesity. European Guidelines for Obesity Management in Adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.; Peralta, M.; Naia, A.; Loureiro, N.; de Matos, M.G. Prevalence of adult overweight and obesity in 20 European countries, 2014. Eur. J. Public Health 2018, 28, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Saltiel, A.R.; Olefsky, J.M. Inflammatory mechanisms linking obesity and metabolic disease. J. Clin. Investig. 2017, 127, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Hotamisligil, G.S. Inflammation, metaflammation and immunometabolic disorders. Nature 2017, 542, 177–185. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, T.; Ackerman, S.E.; Shen, L.; Engleman, E. Role of innate and adaptive immunity in obesity-associated metabolic disease. J. Clin. Investig. 2017, 127, 5–13. [Google Scholar] [CrossRef]
- Wu, H.; Ballantyne, C.M. Metabolic Inflammation and Insulin Resistance in Obesity. Circ. Res. 2020, 126, 1549–1564. [Google Scholar] [CrossRef]
- Forsythe, L.K.; Wallace, J.M.; Livingstone, M.B. Obesity and inflammation: The effects of weight loss. Nutr. Res. Rev. 2008, 21, 117–133. [Google Scholar] [CrossRef]
- Chait, A.; den Hartigh, L.J. Adipose Tissue Distribution, Inflammation and Its Metabolic Consequences, Including Diabetes and Cardiovascular Disease. Front. Cardiovasc. Med. 2020, 7, 22. [Google Scholar] [CrossRef]
- Calder, P.C.; Ahluwalia, N.; Brouns, F.; Buetler, T.; Clement, K.; Cunningham, K.; Esposito, K.; Jönsson, L.S.; Kolb, H.; Lansink, M.; et al. Dietary factors and low-grade inflammation in relation to overweight and obesity. Br. J. Nutr. 2011, 106, S5–S78. [Google Scholar] [CrossRef]
- Giugliano, D.; Ceriello, A.; Esposito, K. The effects of diet on inflammation: Emphasis on the metabolic syndrome. J. Am. Coll. Cardiol. 2006, 48, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Casas, R.; Estruch, R. Dietary Patterns, Foods, Nutrients and Chronic Inflammatory Disorders. Immunome Res. 2016, 12, 122. [Google Scholar] [CrossRef]
- Alkhatib, A.; Tsang, C.; Tiss, A.; Bahorun, T.; Arefanian, H.; Barake, R.; Khadir, A.; Tuomilehto, J. Functional Foods and Lifestyle Approaches for Diabetes Prevention and Management. Nutrients 2017, 9, 1310. [Google Scholar] [CrossRef] [PubMed]
- Razquin, C.; Martinez-Gonzalez, M.A. A Traditional Mediterranean Diet Effectively Reduces Inflammation and Improves Cardiovascular Health. Nutrients 2019, 11, 1842. [Google Scholar] [CrossRef]
- Netea, M.G.; Balkwill, F.; Chonchol, M.; Cominelli, F.; Donath, M.Y.; Giamarellos-Bourboulis, E.J.; Golenbock, D.; Gresnigt, M.S.; Heneka, M.T.; Hoffman, H.M.; et al. A guiding map for inflammation. Nat. Immunol. 2017, 18, 826–831. [Google Scholar] [CrossRef]
- Mancini, J.G.; Filion, K.B.; Atallah, R.; Eisenberg, M.J. Systematic Review of the Mediterranean Diet for Long-Term Weight Loss. Am. J. Med. 2016, 129, 407–415. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Gea, A.; Ruiz-Canela, M. The Mediterranean Diet and Cardiovascular Health. Circ. Res. 2019, 124, 779–798. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Mediterranean dietary pattern, inflammation and endothelial function: A systematic review and meta-analysis of intervention trials. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 929–939. [Google Scholar] [CrossRef]
- Medina-Remón, A.; Casas, R.; Tressserra-Rimbau, A.; Ros, E.; Martínez-González, M.A.; Fitó, M.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventos, R.M.; Estruch, R.; et al. Polyphenol intake from a Mediterranean diet decreases inflammatory biomarkers related to atherosclerosis: A substudy of the PREDIMED trial. Br. J. Clin. Pharmacol. 2017, 83, 114–128. [Google Scholar]
- Casas, R.; Sacanella, E.; Urpí-Sardà, M.; Corella, D.; Castaner, O.; Lamuela-Raventos, R.M.; Salas-Salvadó, J.; Martínez-González, M.A.; Ros, E.; Estruch, R. Long-Term Immunomodulatory Effects of a Mediterranean Diet in Adults at High Risk of Cardiovascular Disease in the PREvención con DIetaMEDiterránea (PREDIMED) Randomized Controlled Trial. J. Nutr. 2016, 146, 1684–1693. [Google Scholar] [CrossRef]
- Dinu, M.; Pagliai, G.; Angelino, D.; Rosi, A.; Dall’Asta, M.; Bresciani, L.; Ferraris, C.; Guglielmetti, M.; Godos, J.; Del Bo, C.; et al. Effects of Popular Diets on Anthropometric and Cardiometabolic Parameters: An Umbrella Review of Meta-Analyses of Randomized Controlled Trials. Adv. Nutr. 2020, 11, 815–833. [Google Scholar] [CrossRef] [PubMed]
- Jovanović, G.K.; Mrakovcic-Sutic, I.; Udović, I.Š.; Majanović, S.K. Evaluating the Effect of an Energy-Restricted Anti-Inflammatory Diet on Weight Loss, Body Composition, Cardiometabolic Risk Factors and Immune System Response in Younger Adults with Obesity: Study Protocol for a Randomized Controlled Trial. Eur. J. Integr. Med. 2020, 37, 101165. [Google Scholar] [CrossRef]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [PubMed]
- Ministarstvo Zdravlja. Odluka o Standardu Prehrane Bolesnika u Bolnicama. Narodne Novine, 59 (on Croatian). 2015. Available online: https://narodne-novine.nn.hr/clanci/sluzbeni/2007_11_121_3528.html (accessed on 15 February 2019).
- Mifflin, M.D.; St Jeor, S.T.; Hill, L.A.; Scott, B.J.; Daugherty, S.A.; Koh, Y.O. A new predictive equation for resting energy expenditure in healthy individuals. Am. J. Clin. Nutr. 1990, 51, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef]
- Kenđel Jovanović, G.; Pavičić Žeželj, S.; Klobučar Majanović, S.; Mrakovcic-Sutic, I.; Šutić, I. Metabolic syndrome and its association with the Dietary Inflammatory Index (DII)® in a Croatian working population. J. Hum. Nutr. Diet. 2020, 33, 128–137. [Google Scholar] [CrossRef]
- Kaić-Rak, A.; Antonić, K. Tablice o Sastavu Namirnica I Pića; Zavod za zaštitu zdravlja Hrvatske: Zagreb, Croatia, 1990; (On Croatian). [Google Scholar]
- Frida Food Data; Version 1; National Food Institute, Technical University of Denmark: Kongens Lyngby, Denmark, 2015; Available online: http://frida.fooddata.dk (accessed on 11 March 2019).
- U.S. Department of Agriculture, Agricultural Research Service, USDA Nutrient Data Laboratory. USDA National Nutrient Database for Standard Reference. Available online: https://ndb.nal.usda.gov/ndb/ (accessed on 11 March 2019).
- Rothwell, J.A.; Perez-Jimenez, J.; Neveu, V.; Medina-Remon, A.; M’Hiri, N.; García-Lobato, P.; Manach, C.; Knox, C.; Eisner, R.; Wishart, D.S.; et al. Phenol-Explorer 3.0: A major update of the Phenol-Explorer database to incorporate data on the effects of food processing on polyphenol content. Database 2013, 2013, bat070. [Google Scholar] [CrossRef]
- Haytowitz, D.B.; Wu, X.; Bhagwat, S. USDA Database for the Flavonoid Content of Selected Foods, Release 3.3. U.S. Department of Agriculture, Agricultural Research Service. Nutrient Data Lab. 2018. Available online: http://www.ars.usda.gov/nutrientdata/flav (accessed on 18 March 2019).
- Gunathile, K.D.P.P.; Ranaweera, K.K.D.S.; Rupasinghe, H.P.V. Influence of boiling, steaming and frying of selected leafy vegetables on the in vitro anti-inflammation associated biological activities. Plants 2018, 7, 22. [Google Scholar] [CrossRef]
- Rothwell, J.A.; Medina-Remón, A.; Pérez-Jiménez, J.; Neveu, V.; Knaze, V.; Slimani, N.; Scalbert, A. Effects of food processing on polyphenol contents: A systematic analysis using phenol-explorer data. Nutrition 2019, 58, 140–148. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, I.; Daimon, T. The “cardiometabolic index” as a new marker determined by adiposity and blood lipids for discrimination of diabetes mellitus. Clin. Chim. Acta 2015, 438, 274–478. [Google Scholar] [CrossRef] [PubMed]
- Salama, A.A.; Amine, E.K.; Salem, H.A.; Abd El Fattah, N.K. Anti-Inflammatory Dietary Combo in Overweight and Obese Women with Polycystic Ovary Syndrome. N. Am. J. Med. Sci. 2015, 7, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Cavallari, J.F.; Denou, E.; Foley, K.P.; Khan, W.I.; Schertzer, J.D. Different Th17 immunity in gut, liver, and adipose tissues during obesity: The role of diet, genetics, and microbes. Gut Microbes 2016, 7, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Gotsis, E.; Anagnostis, P.; Mariolis, A.; Vlachou, A.; Katsiki, N.; Karagiannis, A. Health benefts of the Mediterranean Diet: An Update of Research Over the Last 5 Years. Angiology 2015, 66, 304–318. [Google Scholar] [CrossRef] [PubMed]
- Romagnolo, D.F.; Selmin, O.I. Mediterranean Diet and Prevention of Chronic Diseases. Nutr. Today 2017, 52, 208–222. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvado, J.; Becerra-Tomas, N.; García-Gavilán, J.F.; Bullo, M.; Barrubes, L. Mediterranean Diet and Cardiovascular Disease Prevention: What Do We Know? Prog. Cardiovasc. Dis. 2018, 61, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Andreoli, A.; Lauro, S.; Di Daniele, N.; Sorge, R.; Celi, M.; Volpe, S.L. Effect of a moderately hypoenergetic Mediterranean diet and exercise program on body cell mass and cardiovascular risk factors in obese women. Eur. J. Clin. Nutr. 2008, 62, 892–897. [Google Scholar] [CrossRef]
- Franquesa, M.; Pujol-Busquets, G.; García-Fernández, E.; Rico, L.; Shamirian-Pulido, L.; Aguilar-Martínez, A.; Medina, F.X.; Serra-Majem, L.; Bach-Faig, A. Mediterranean Diet and Cardiodiabesity: A Systematic Review through Evidence-Based Answers to Key Clinical Questions. Nutrients 2019, 11, 655. [Google Scholar] [CrossRef]
- Ortner Hadžiabdić, M.; Vitali Čepo, D.; Rahelić, D.; Božikov, V. The Effect of the Mediterranean Diet on Serum Total Antioxidant Capacity in Obese Patients: A Randomized Controlled Trial. J. Am. Coll. Nutr. 2015, 35, 224–351. [Google Scholar] [CrossRef]
- Estruch, R. Anti-inflammatory effects of the Mediterranean diet: The experience of the PREDIMED study. Proc. Nutr. Soc. 2010, 69, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-style diet for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2019, 3, CD009825. [Google Scholar] [CrossRef] [PubMed]
- Doko Jelinić, J.; Pucarin-Cvetković, J.; Nola, I.A.; Senta, A.; Milošević, M.; Kern, J. Regional differences in dietary habits of adult Croatian population. Coll. Antropol. 2009, 33, 31–34. [Google Scholar]
- Kenđel Jovanović, G.; Pavičić Žeželj, S.; Malatestinić, Đ.; Mrakovčić Šutić, I.; Nadarević Štefanac, V.; Dorčić, F. Diet quality of middle age and older women from Primorsko-Goranska County evaluated by healthy eating index and association with body mass index. Coll. Antropol. 2010, 34, 155–160. [Google Scholar]
- Pavičić Žeželj, S.; Kenđel Jovanović, G.; Dragaš Zubalj, N.; Mićović, V.; Sesar, Ž. Associations between Adherence to the Mediterranean Diet and Lifestyle Assessed with the MEDLIFE Index among the Working Population. Int. J. Environ. Res. Public Health 2018, 15, 2126. [Google Scholar] [CrossRef]
- Sahay, R.D.; Couch, S.C.; Missoni, S.; Sujoldžić, A.; Novokmet, N.; Duraković, Z.; Rao, M.B.; Musić Milanović, S.; Vuletić, S.; Deka, R.; et al. Dietary patterns in adults from an Adriatic Island of Croatia and their associations with metabolic syndrome and its components. Coll. Antropol. 2013, 37, 335–342. [Google Scholar]
- Tomas, Ž.; Škarić-Jurić, T.; Zajc Petranović, M.; Jalšovec, M.; Rajić Šikanjić, P.; Smolej Narančić, N. Waist to height ratio is the anthropometric index that most appropriately mirrors the lifestyle and psychological risk factors of obesity. Nutr. Diet. 2019, 76, 539–545. [Google Scholar] [CrossRef]
- Willoughby, D.; Hewlings, S.; Kalman, D. Body Composition Changes in Weight Loss: Strategies and Supplementation for Maintaining Lean Body Mass, a Brief Review. Nutrients 2018, 10, 1876. [Google Scholar] [CrossRef]
- Connaughton, R.M.; McMorrow, A.M.; McGillicuddy, F.C.; Lithander, F.E.; Roche, H.M. Impact of anti-inflammatory nutrients on obesity-associated metabolic-inflammation from childhood through to adulthood. Proc. Nutr. Soc. 2016, 75, 115–124. [Google Scholar] [CrossRef]
- Perez-Jimenez, J.; Fezeu, L.; Touvier, M.; Arnault, N.; Manach, C.; Hercberg, S.; Galan, P.; Scalbert, A. Dietary intake of 337 polyphenols in French adults 1–3. Am. J. Clin. Nutr. 2011, 93, 1220–1228. [Google Scholar] [CrossRef]
- Hostetler, G.L.; Ralston, R.A.; Schwartz, S.J. Flavones: Food Sources, Bioavailability, Metabolism, and Bioactivity. Adv. Nutr. 2017, 8, 423–435. [Google Scholar] [CrossRef] [PubMed]
- The EFSA Comprehensive European Food Consumption Database. Available online: http://data.europa.eu/euodp/data/dataset/the-efsa-comprehensive-european-food-consumption-database (accessed on 15 June 2019).
- WHO: GEMS/Food Consumption Database. Available online: https://www.who.int/nutrition/landscape_analysis/nlis_gem_food/en/ (accessed on 17 June 2019).
- Tapsell, L.C.; Hemphill, I.; Cobiac, L.; Sullivan, D.R.; Fenech, M.; Patch, C.S.; Roodenrys, S.; Keogh, J.B.; Clifton, P.M.; Williams, P.G.; et al. Health benefits of herbs and spices: The past, the present, the future. Med. J. Aust. 2006, 1854, S4–S24. [Google Scholar] [CrossRef]
- Jiang, T.A. Health Benefits of Culinary Herbs and Spices. J. AOAC Int. 2019, 102, 395–411. [Google Scholar] [CrossRef] [PubMed]
- Shoba, G.; Joy, D.; Joseph, T.; Rajendran, M.M.; Srinivas, P.S. Influence of piperine on the pharmacokinetics of curcumin in animals and human volunteers. Planta Med. 1998, 64, 353–356. [Google Scholar] [CrossRef] [PubMed]
- Babatunde, O.A.; Arp Adams, S.; Truman, S.; Sercy, E.; Murphy, A.E.; Khan, S.; Hurley, T.G.; Wirth, M.D.; Choi, S.K.; Johnson, H.; et al. The impact of a randomized dietary and physical activity intervention on chronic inflammation among obese African-American women. Women Health 2020, 1–14. [Google Scholar] [CrossRef]
- Mayr, H.L.; Itsiopoulos, C.; Tierney, A.C.; Ruiz-Canela, M.; Hebert, J.R.; Shivappa, N.; Thomas, C.J. Improvement in dietary inflammatory index score after 6-month dietary intervention is associated with reduction in interleukin-6 in patients with coronary heart disease: The AUSMED heart trial. Nutr. Res. 2018, 55, 108–121. [Google Scholar] [CrossRef]
- Turner-McGrievy, G.M.; Wirth, M.D.; Shivappa, N.; Dunn, C.G.; Crimarco, A.; Hurley, T.G.; West, D.S.; Hussey, J.R.; Hébert, J.R. Impact of a 12-month Inflammation Management Intervention on the Dietary Inflammatory Index, inflammation, and lipids. Clin. Nutr. ESPEN 2019, 30, 42–51. [Google Scholar] [CrossRef]
- Wirth, M.D.; Shivappa, N.; Khan, S.; Vyas, S.; Beresford, L.; Sofge, J.; Hébert, J.R. Impact of a 3-Month Anti-inflammatory Dietary Intervention Focusing on Watermelon on Body Habitus, Inflammation, and Metabolic Markers: A Pilot Study. Nutr. Metab. Insights 2020, 13, 1178638819899398. [Google Scholar] [CrossRef]
- Jovanović, Ž.; Crnčević-Orlić, Ž.; Štimac, D.; Kokić, S.; Peršić, V.; Ružić, T.; Goll-Barić, S. Effects of obesity reduction on cardiovascular risk factors: Comparison of individual and group treatment--substudy of the Croatian Healthy Weight Loss Programme. Coll. Antropol. 2009, 33, 751–757. [Google Scholar]
- Hoyas, I.; Leon-Sanz, M. Nutritional Challenges in Metabolic Syndrome. J. Clin. Med. 2019, 8, 1301. [Google Scholar] [CrossRef]
- Tay, J.; Thompson, C.H.; Brinkworth, G.D. Glycemic Variability: Assessing Glycemia Differently and the Implications for Dietary Management of Diabetes. Ann. Rev. Nutr. 2015, 35, 389–424. [Google Scholar] [CrossRef] [PubMed]
- Boucher, J.L. Mediterranean Eating Pattern. Diabetes Spectr. 2017, 30, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Hallberg, S.J.; Dockter, N.E.; Kushner, J.A.; Athinarayanan, S.J. Improving the scientific rigour of nutritional recommendations for adults with type 2 diabetes: A comprehensive review of the American Diabetes Association guideline-recommended eating patterns. Diabetes Obes. Metab. 2019, 21, 1769–1779. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, M.L.; Dunbar, S.A.; Jaacks, L.M.; Karmally, W.; Mayer-Davis, E.J.; Wylie-Rosett, J.; Yancy, W.S. Macronutrients, food groups, and eating patterns in the management of diabetes: A systematic review of the literature, 2010. Diabetes Care 2012, 35, 434–445. [Google Scholar] [CrossRef] [PubMed]
- Huo, R.; Du, T.; Xu, Y.; Xu, W.; Chen, X.; Sun, K.; Yu, X. Effects of Mediterranean-style diet on glycemic control, weight loss and cardiovascular risk factors among type 2 diabetes individuals: A meta-analysis. Eur. J. Clin. Nutr. 2015, 69, 1200–1208. [Google Scholar] [CrossRef] [PubMed]
- Vessby, B.; Uusitupa, M.; Hermansen, K.; Riccardi, G.; Rivellese, A.A.; Tapsell, L.C.; Nälsén, C.; Berglund, L.; Louheranta, A.; Rasmussen, B.M.; et al. Substituting dietary saturated for monounsaturated fat impairs insulin sensitivity in healthy men and women: The KANWU Study. Diabetologia 2001, 44, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Julibert, A.; Bibiloni, M.D.; Bouzas, C.; Martínez-González, M.Á.; Salas-Salvadó, J.; Corella, D.; Zomeño, M.D.; Romaguera, D.; Vioque, J.; Alonso-Gómez, Á.M.; et al. Total and Subtypes of Dietary Fat Intake and Its Association with Components of the Metabolic Syndrome in a Mediterranean Population at High Cardiovascular Risk. Nutrients 2019, 11, 1493. [Google Scholar] [CrossRef]
- Savva, S.C.; Lamnisos, D.; Kafatos, A.G. Predicting cardiometabolic risk: Waist-to-height ratio or BMI. A meta-analysis. Diabetes Metab. Syndr. Obes. 2013, 6, 403–419. [Google Scholar] [CrossRef]
- Wu, J.H.Y.; Micha, R.; Mozaffarian, D. Dietary fats and cardiometabolic disease: Mechanisms and effects on risk factors and outcomes. Nat. Rev. Cardiol. 2019, 16, 581–601. [Google Scholar] [CrossRef]
- Després, J.P. Is visceral obesity the cause of the metabolic syndrome? Ann. Med. 2006, 38, 52–63. [Google Scholar] [CrossRef]
- Perticone, M.; Maio, R.; Sciacqua, A.; Suraci, E.; Pinto, A.; Pujia, R.; Zito, R.; Gigliotti, S.; Sesti, G.; Perticone, F. Ketogenic Diet-Induced Weight Loss is Associated with an Increase in Vitamin D Levels in Obese Adults. Molecules 2019, 24, 2499. [Google Scholar] [CrossRef] [PubMed]
- Cowan, S.F.; Leeming, E.R.; Sinclair, A.; Dordevic, A.L.; Truby, H.; Gibson, S.J. Effect of whole foods and dietary patterns on markers of subclinical inflammation in weight-stable overweight and obese adults: A systematic review. Nutr. Rev. 2020, 78, 19–38. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, V.E. Weight loss is a critical factor to reduce inflammation. Clin. Nutr. ESPEN 2018, 28, 21–35. [Google Scholar] [CrossRef] [PubMed]
- Magkos, F.; Fraterrigo, G.; Yoshino, J.; Luecking, C.; Kirbach, K.; Kelly, S.C.; De Las Fuentes, L.; He, S.; Okunade, A.L.; Patterson, B.W.; et al. Effects of Moderate and Subsequent Progressive Weight Loss on Metabolic Function and Adipose Tissue Biology in Humans with Obesity. Cell Metab. 2016, 23, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Headland, M.; Clifton, P.M.; Carter, S.; Keogh, J.B. Weight-Loss Outcomes: A Systematic Review and Meta-Analysis of Intermittent Energy Restriction Trials Lasting a Minimum of 6 Months. Nutrients 2016, 8, 354. [Google Scholar] [CrossRef]
- Woodside, J.V.; Welch, R.W.; Patterson, C.C.; McKinley, M.C. Study Design: Intervention Studies. In Nutrition Research Methodologies; Lovegrove, J.A., Hodson, L., Sharma, S., Lanham-New, S.A., Eds.; The Nutrition Society Textbook Series; Wiley-Blackwell: West Sussex, UK, 2015; pp. 28–47. [Google Scholar]


{kind=link}
| Variable | Anti-inflammatory Diet (AID) Group (42 (51.9)) | Control Diet (CD) Group (39 (48.1)) | p-Value |
|---|---|---|---|
| Gender, Men | 3 (7.1) | 4 (10.3) | 0.619 a |
| Women | 39 (92.9) | 35 (89.7) | |
| Age (years) (Mean± SD) | 43.60 ± 5.75 | 41.72 ± 6.70 | 0.178 b |
| Marriage Status, Single | 3 (7.1) | 3 (7.7) | 0.537 a |
| Married | 38 (90.5) | 33 (84.6) | |
| Divorced | 1 (2.4) | 3 (7.7) | |
| Widowed | 0 (0) | 0 (0) | |
| Education Degree, Elementary school | 0 (0) | 2 (5.1) | 0.00 a |
| High School | 12 (28.6) | 22 (56.4) | |
| University | 29 (69.0) | 15 (38.5) | |
| Postgraduate | 1 (2.4) | 0 (0) | |
| Professional Status, Unemployed | 1 (2.4) | 9 (23.1) | 0.033 a |
| Employed | 40 (95.2) | 30 (76.9) | |
| Student | 1 (2.4) | 0 (0) | |
| Physical Activity, Inactive | 15 (35.7) | 18 (46.2) | 0.315 a |
| Moderately Inactive | 9 (21.4) | 3 (7.7) | |
| Moderately Active | 14 (33.3) | 15 (38.5) | |
| Active | 4 (9.5) | 3 (7.7) | |
| Obesity, First Degree | 26 (61.9) | 21 (53.8) | 0.584 a |
| Second Degree | 10 (23.8) | 9 (23.1) | |
| Third Degree | 6 (14.3) | 9 (23.1) | |
| Metabolic Syndrome, Yes | 20 (47.6) | 13 (33.3) | 0.191 a |
| Autoimmune Thyroid Disease | 10 (23.8) | 3 (7.7) | 0.048 a |
| Variable | Anti-inflammatory Diet Group | Control Diet Group | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Trial End | Change (%) | p-Value c | Baseline | Trial End | Change (%) | p-Value c | Baseline p-Value d | Trial End p-Value e | |
| Energy (MJ) | 10.03 (2.64) | 6.92 (0.47) | −31.01 | <0.001 | 11.21 (2.59) | 7.63(0.40) | −31.94 | <0.001 | 0.129 | <0.001 |
| Protein (g) | 103.03 (31.08) | 85.60 (14.42) | −16.92 | 0.009 a | 113.70 (26.49) | 97.13 (8.72) | −14.57 | 0.001 a | 0.211 a | 0.002 a |
| Carbohydrate (g) | 233.91 (77.56) | 145.35 (31.43) | −37.86 | <0.001 a | 280.21 (79.75) | 172.96 (17.32) | −38.27 | <0.001 a | 0.049 a | <0.001 a |
| Fat (g) | 111.94 (27.14) | 81.05 (13.91) | −27.60 | <0.001 a | 120.07 (30.28) | 80.69 (9.58) | −32.80 | <0.001 a | 0.338 a | 0.918 a |
| MUFA (g) | 44.93 (11.90) | 39.30 (8.69) | −12.53 | 0.110 a | 43.93 (10.30) | 32.39 (3.68) | −26.27 | <0.001 a | 0.759 a | <0.001 a |
| PUFA (g) | 19.02 (5.39) | 15.40 (3.63) | −19.03 | 0.010 a | 21.10 (4.92) | 13.26 (1.24) | −37.16 | <0.001 a | 0.174 a | 0.009 a |
| Omega-3 (g) | 1.16 (0.68) | 1.27 (0.54) | 9.48 | 0.049 a | 0.79 (0.21) | 0.54 (0.15) | −31.65 | <0.001 a | 0.015 a | <0.001 b |
| Omega-6 (g) | 0.73 (0.21) | 0.47 (0.19) | −35.62 | <0.001 a | 0.91 (0.30) | 0.60 (0.12) | −3.23 | 0.159 a | 0.023 a | <0.001 a |
| Saturated fat (g) | 41.50 (14.69) | 20.20 (3.10) | −51.33 | <0.001 a | 49.35 (14.67) | 28.63 (3.56) | −41.99 | <0.001 a | 0.074 a | <0.001 a |
| Trans fat (g) | 1.67 (0.41) | 1.32 (0.62) | −20.96 | <0.001 a | 2.13 (0.67) | 1.31 (0.30) | −38.50 | <0.001 a | 0.007 a | 0.941 a |
| Cholesterol (mg) | 380.81 (160.38) | 318.51 (175.61) | −16.36 | 0.030 a | 477.55 (463.01) | 463.01 (125.57) | −3.04 | 0.643 | 0.004 a | <0.001 a |
| Fiber (g) | 27.44 (11.30) | 33.90 (5.22) | 23.54 | 0.002 a | 25.46 (6.69) | 28.69 (3.95) | 12.69 | 0.146 | 0.467 a | <0.001 a |
| Alcohol (g) | 6.10 (12.29) | 0.21 (1.02) | −96.56 | <0.001 b | 3.34 (3.87) | 2.44 (3.33) | −26.95 | 0.605 b | 0.991 b | 0.005 b |
| Caffeine (g) | 315.41 (162.30) | 239.48 (112.49) | −24.07 | 0.675 a | 218.35 (221.56) | 202.07 (79.48) | −7.46 | 0.864 b | 0.095 a | 0.193 a |
| Folate (μg) | 433.81 (243.26) | 539.07 (158.45) | 47.86 | <0.001 a | 330.28 (82.88) | 373.58 (53.67) | 11.27 | 0.042 a | 0.055 a | <0.001 a |
| Beta carotene (μg) | 4.20 (2.16) | 5.72 (1.95) | 36.19 | <0.001 b | 3.75 (1.57) | 3.32 (0.71) | −11.47 | <0.001 a | 0.002 b | 0.193 a |
| Vitamin A (RE) | 700.87 (334.55) | 919.41 (570.63) | 31.18 | 0.020 a | 969.03 (530.92) | 1083.97 (540.80) | 11.86 | 0.190 b | 0.008 a | 0.187 a |
| Vitamin B6 (mg) | 2.24 (0.90) | 2.42 (1.16) | 0.00 | 0.480 a | 2.81 (1.31) | 2.00 (0.70) | −28.83 | 0.022 b | 0.024 a | 0.250 b |
| Vitamin B12 (μg) | 3.14 (1.33) | 2.46 (1.44) | −21.66 | 0.012 a | 3.18 (1.07) | 2.30 (0.47) | −27.67 | <0.001 a | 0.884 a | 0.139 a |
| Vitamin C (mg) | 204.13 (153.16) | 287.64 (106.32) | 40.91 | 0.002 a | 166.32 (76.80) | 133.05 (33.06) | −20.00 | 0.007 a | 0.287 a | <0.001 a |
| Vitamin D (μg) | 14.54 (22.06) | 6.24 (17.41) | −57.08 | 0.012 b | 10.10 (11.68) | 2.18 (0.96) | −78.42 | <0.001 a | 0.966 b | 0.261 a |
| Vitamin E (mg) | 22.51 (12.98) | 26.81 (8.19) | 19.10 | 0.015 a | 16.12 (2.97) | 12.35 (2.44) | −23.39 | <0.0001 a | 0.113 b | <0.001 a |
| Iron (mg) | 8.22 (2.05) | 8.55 (2.12) | 4.01 | 0.487 a | 9.03 (2.81) | 9.37 (1.85) | 3.77 | 0.571 a | 0.143 a | 0.017 a |
| Magnesium (mg) | 412.51 (132.81) | 440.18 (80.88) | 6.71 | 0.213 a | 393.11 (88.66) | 371.74 (36.78) | −5.44 | 0.080 a | 0.557 a | <0.001 a |
| Niacin (mg) | 19.40 (6.37) | 17.38 (3.91) | −10.41 | 0.077 a | 24.82 (8.20) | 17.29 (1.68) | −30.34 | <0.001 a | 0.001 a | 0.881 a |
| Riboflavin (mg) | 1.60 (0.65) | 2.01 (0.71) | 25.63 | 0.089 a | 2.07 (0.70) | 2.24 (0.31) | 8.21 | 0.189 a | 0.002 a | 0.056 a |
| Selenium (μg) | 37.42 (17.60) | 31.76 (10.95) | −15.13 | 0.467 a | 35.86 (7.79) | 39.61 (10.99) | 10.46 | 0.309 a | 0.696 a | 0.018 a |
| Thiamine (mg) | 1.54 (0.51) | 1.73 (0.39) | 12.34 | 0.057 a | 1.93 (0.58) | 1.56 (0.25) | −19.17 | 0.001 a | 0.002 a | 0.023 a |
| Zinc (mg) | 15.42 (4.59) | 13.91 (3.17) | −9.79 | 0.084 a | 18.12 (4.85) | 13.70 (1.30) | −24.39 | <0.001 a | 0.025 a | 0.772 a |
| Flavan-3-ol (mg) | 28.81 (26.79) | 15.83 (10.41) | −45.05 | 0.056 b | 23.37 12.83 | 8.34 (2.39) | −64.31 | <0.001 a | 0.807 b | <0.001 b |
| Flavones (mg) | 2.90 (2.03) | 5.58 (3.40) | 92.41 | <0.001 a | 2.27 (1.40) | 3.14 (1.46) | 38.33 | 0.037 b | 0.366 b | 0.002 a |
| Flavonols (mg) | 147.41 (78.61) | 149.40 (6.79) | 1.35 | 0.856 a | 107.57 (34.82) | 74.19 (39.99) | −31.03 | <0.001 a | 0.029 a | <0.001 a |
| Flavonones (mg) | 46.08 (37.87) | 22.96 (22.86) | −50.17 | <0.001 a | 65.59 (74.68) | 3.64 (3.98) | -94.45 | <0.001 a | 0.856 b | <0.001 b |
| Anthocyanidins (mg) | 24.25 (34.64) | 29.97 (28.37) | 23.59 | 0.406 a | 15.54 (9.33) | 24.30 (19.43) | 56.37 | 0.606 a | 0.873 b | 0.426 a |
| Isoflavones (mg) | 0.36 (0.22) | 0.56 (0.28) | 55.55 | 0.864 a | 0.27 (0.36) | 0.62 (0.49) | 129.63 | 0.787 a | 0.816 a | 0.374 a |
| Eugenol (mg) | 0.03 (0.06) | 0.04 (0.12) | 33.33 | 0.499 b | 0.02 (0.02) | 0.00 (0.01) | −100.00 | 0.004 b | 0.062 b | 0.262 b |
| Green/black tea (g) | 1.07 (0.91) | 2.86 (1.66) | 167.29 | 0.011 a | 0.96 (0.24) | 2.08 (1.84) | 116.67 | 0.009 a | 0.358 a | 0.686 a |
| Garlic (g) | 2.10 (1.49) | 6.60 (2.28) | 86.57 | 0.006 b | 0.75 (1.19) | 4.32 (1.44) | 476.00 | <0.001 b | <0.001 a | <0.001 a |
| Ginger (g) | 0.15 (0.38) | 0.19 (0.26) | 26.67 | 0.098 b | 0.06 (0.07) | 0.00 (0.00) | −100.00 | <0.001 b | 0.481 b | <0.001 b |
| Onion (g) | 14.61 (7.03) | 13.11 (10.63) | −10.27 | 0.074 a | 17.97 (9.01) | 10.89 (7.89) | −39.40 | 0.009 b | 0.163 a | 0.418 a |
| Pepper (g) | 0.67 (0.68) | 1.25 (0.56) | 86.57 | 0.006 b | 0.55 (0.54) | 0.70 (0.23) | 27.27 | 0.033 a | 0.621 b | <0.001 a |
| Rosemary (mg) | 0.11 (0.17) | 0.17 (0.29) | 54.55 | 0.909 a | 0.02 (0.03) | 0.01 (0.01) | −50.00 | <0.001 b | 0.139 b | <0.001 b |
| Saffron (g) | 0.01 (0.01) | 0.01 (0.02) | 0.00 | 0.939 b | 0.00 (0.00) | 0.01 (0.01) | 0.00 | 0.999 b | 0.917 b | 0.884 b |
| Turmeric (mg) | 0.38 (0.94) | 1.05 (0.69) | 176.32 | 0.002 b | 0.08 (0.18) | 0.01 (0.03) | −87.50 | 0.002 b | 0.220 b | <0.001 b |
| Thyme/oregano (mg) | 0.09 (0.11) | 0.29 (0.16) | 222.22 | <0.001 a | 0.04 (0.08) | 0.13 (0.06) | 225.00 | 0.002 b | 0.009 b | 0.001 b |
| DII® | −0.53 (2.29) | −2.03 (0.97) | 283.02 | 0.002 a | −0.23 (1.28) | −0.31 (1.01) | 30.43 | 0.725 a | 0.579 a | <0.001 a |
| Variable | Anti-inflammatory Diet Group | Control Diet Group | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Trial End | Change (%) | p-Value c | Baseline | Trial End | Change (%) | p-Value c | Baseline p-Value d | Trial End p-Value e | |
| Body weight (kg) | 102.94 (14.19) | 95.67 (11.72) | −7.06 | <0.001 a | 101.35 (21.93) | 95.06 (21.36) | −6.21 | <0.001 a | 0.770 a | 0.903 a |
| Body mass index (kg/m2) | 35.36 (4.27) | 32.90 (3.90) | −6.96 | <0.001 a | 33.40 (5.48) | 30.99 (4.32) | −7.22 | <0.001 a | 0.179 a | 0.119 a |
| Waist circumference (cm) | 108.43 (8.37) | 102.91 (7.77) | −5.09 | <0.001 a | 107.86 (10.11) | 100.88 (10.04) | −6.47 | <0.001 a | 0.482 b | 0.442 a |
| Fat tissue (kg) | 46.49 (10.17) | 40.84 (7.87) | −12.15 | <0.001 a | 45.89 (7.71) | 39.42 (8.82) | −14.10 | <0.001 a | 0.807 b | 0.328 b |
| Fat tissue (%) | 44.87 (4.38) | 42.34 (4.80) | −5.64 | <0.001 a | 45.57 (2.57) | 42.20 (2.98) | −7.40 | 0.001 a | 0.505 a | 0.755 a |
| Visceral adipose tissue (l) | 3.14 (1.32) | 2.44 (1.05) | −22.29 | <0.001 a | 3.46 (1.63) | 2.58 (1.37) | −25.43 | <0.001 a | 0.376 b | 0.798 b |
| Non-fat tissue (kg) | 56.45 (6.50) | 55.28 (6.09) | −2.07 | 0.139 a | 54.88 (11.50) | 53.81 (12.97) | −1.95 | 0.019 b | 0.569 b | 0.625 a |
| Non-fat tissue (%) | 55.13 (4.38) | 57.80 (4.66) | 4.84 | <0.001 a | 54.40 (2.61) | 57.21 (2.40) | 5.17 | <0.001 a | 0.484 a | 0.587 a |
| Skeletal muscle tissue (kg) | 27.41 (3.86) | 26.22 (3.29) | −4.34 | 0.022 a | 26.96 (6.21) | 25.78 (7.34) | −4.38 | 0.005 b | 0.449 b | 0.085 b |
| Total water (L) | 42.40 (4.95) | 41.33 (4.40) | −2.52 | 0.009 a | 41.16 (8.26) | 40.04 (9.50) | −2.72 | 0.091 a | 0.537 a | 0.053 b |
| Total water (%) | 41.13 (8.37) | 43.17 (4.08) | 4.96 | <0.001 a | 40.34 (1.70) | 42.66 (1.81) | 5.73 | 0.009 a | 0.407 a | 0.582 a |
| Variable | Anti-inflammatory Diet Group | Control Diet Group | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Trial End | Change (%) | p-Value c | Baseline | Trial End | Change (%) | p-Value c | Baseline p-Value d | Trial End p-Value e | |
| Glucose (mmol/L) | 5.69 (1.41) | 5.48 (0.62) | −3.69 | 0.284 b | 5.58 (0.45) | 4.85 (0.59) | −13.08 | <0.001 a | 0.107 b | <0.001 a |
| HbA1c (mmol/mol) | 35.26 (6.45) | 34.66 (7.62) | −1.70 | 0.855 a | 38.34 (4.87) | 38.37 (4.74) | 0.08 | 0.121 a | 0.071 a | 0.050 a |
| HbA1c (%) | 5.40 (0.63) | 5.52 (0.55) | 2.22 | 0.049 a | 5.64 (0.45) | 5.65 (0.45) | 0.18 | 0.127 a | 0.128 a | 0.371 a |
| Insulin (mU/L) | 18.22 (11.69) | 16.19 (9.98) | −11.14 | 0.946 a | 16.10 (4.91) | 11.73 (3.88) | −27.14 | 0.008 b | 0.419 b | 0.048 a |
| HOMA - IR (pmol/L) | 4.84 (3.89) | 4.09 (3.00) | −15.50 | 0.307 b | 3.99 (1.26) | 2.54 (0.86) | −36.34 | 0.002 a | 0.572 b | 0.040 b |
| Total cholesterol (mmol/L) | 5.25 (1.10) | 4.97 (1.34) | −5.33 | 0.594 a | 5.84 (0.65) | 5.39 (0.80) | −7.71 | 0.002 a | 0.028 a | 0.193 a |
| HDL-C (mmol/L) | 1.37 (0.21) | 1.51 (0.53) | 10.22 | 0.058 a | 1.34 (0.20) | 1.33 (0.13) | −0.75 | 0.073 a | 0.642 a | 0.127 b |
| LDL-C (mmol/L) | 3.30 (1.02) | 3.15 (0.99) | −4.55 | 0.357 a | 3.84 (0.61) | 3.38 (0.63) | −11.98 | <0.001 a | 0.031 a | 0.343 a |
| Triglycerides (mmol/L) | 1.31 (0.94) | 1.15 (0.56) | −12.21 | 0.446 b | 1.50 (0.40) | 1.33 (0.47) | −11.33 | 0.393 a | 0.008 b | 0.144 b |
| CMI index | 0.66 (0.60) | 0.51 (0.39) | −22.73 | 0.153 b | 0.71 (0.21) | 0.59 (0.22) | −16.90 | 0.622 a | 0.016 b | 0.145 b |
| Vitamin D (nmol/L) | 48.13 (21.36) | 66.59 (24.72) | 38.35 | <0.001 a | 54.09 (11.47) | 48.35 (18.46) | −10.61 | 0.135 b | 0.237 a | 0.006 a |
| hs-CRP (mg/L) | 6.28 (5.48) | 4.43 (4.29) | −29.46 | 0.003 a | 6.78 (4.09) | 3.92 (0.92) | −42.18 | 0.010 b | 0.311 b | 0.662 b |
| IL-6 (pg/mL) | 0.77 (0.63) | 0.63 (0.36) | −18.18 | 0.013 a | 1.34 (0.85) | 0.98 (0.81) | −26.86 | 0.002 a | <0.001 a | 0.001 a |
| TNF-α (pg/mL) | 0.38 (0.19) | 0.25 (0.09) | −34.21 | 0.002 a | 1.72 (0.33) | 1.54 (0.36) | −10.47 | <0.001 a | 0.001 b | <0.001 b |
| Variable | Anti-inflammatory Diet Group | Control Diet Group | ||||||
|---|---|---|---|---|---|---|---|---|
| β | 95% CI | p-Value | β | 95% CI | p-Value | |||
| Body weight (kg) | −0.13 | −0.31 | 0.58 | 0.540 | −0.21 | −0.64 | 0.22 | 0.328 |
| Body mass index (kg/m2) | −0.19 | −0.25 | 0.69 | 0.247 | −0.33 | −0.75 | 0.09 | 0.114 |
| Waist circumference (cm) | −0.06 | −0.16 | 0.79 | 0.087 | −0.12 | −0.56 | 0.32 | 0.582 |
| Fat mass (kg) | −0.18 | −0.26 | 0.70 | 0.234 | −0.26 | −0.69 | 0.16 | 0.214 |
| Fat free mass (kg) | −0.03 | −0.48 | 0.42 | 0.897 | −0.03 | −0.47 | 0.41 | 0.899 |
| Skeletal muscle tissue (kg) | 0.05 | −0.41 | 0.50 | 0.831 | −0.03 | −0.48 | 0.41 | 0.875 |
| Visceral adipose tissue (L) | −0.21 | −0.23 | 0.65 | 0.339 | −0.11 | −0.33 | 0.55 | 0.608 |
| Total water (L) | −0.00 | −0.46 | 0.45 | 0.990 | −0.04 | −0.48 | 0.40 | 0.853 |
| Glucose (mmol/L) | −0.14 | −0.59 | 0.31 | 0.525 | −0.02 | −0.42 | 0.46 | 0.932 |
| HbA1c (mmol/mol) | −0.17 | −0.28 | 0.61 | 0.446 | −0.04 | −0.34 | 0.49 | 0.835 |
| HbA1c (%) | −0.02 | −0.44 | 0.47 | 0.943 | −0.03 | −0.44 | 0.47 | 0.878 |
| Insulin (mU/L) | −0.04 | −0.49 | 0.42 | 0.865 | −0.55 | −0.92 | −0.18 | 0.005 |
| HOMA-IR (pmol/L) | −0.06 | −0.52 | 0.39 | 0.778 | −0.49 | −0.88 | −0.11 | 0.015 |
| Total cholesterol (mmol/L) | −0.01 | −0.44 | 0.46 | 0.961 | −0.38 | −0.79 | 0.03 | 0.071 |
| HDL-C (mmol/L) | −0.05 | −0.51 | 0.40 | 0.814 | 0.17 | −0.27 | 0.61 | 0.428 |
| LDL-C (mmol/L) | −0.10 | −0.55 | 0.35 | 0.659 | −0.22 | −0.65 | 0.21 | 0.300 |
| Triglycerides (mmol/L) | −0.13 | −0.58 | 0.32 | 0.565 | −0.56 | −0.93 | −0.20 | 0.004 |
| CMI index | −0.05 | −0.51 | 0.40 | 0.804 | −0.59 | −0.94 | −0.23 | 0.003 |
| Vitamin D (nmol/L) | −0.07 | −0.39 | 0.52 | 0.766 | −0.23 | −0.66 | 0.20 | 0.277 |
| hs-CRP (mg/L) | −0.06 | −0.40 | 0.51 | 0.798 | −0.21 | −0.64 | 0.22 | 0.319 |
| IL-6 (pg/mL) | −0.46 | −0.56 | 0.46 | 0.026 | −0.14 | −0.58 | 0.30 | 0.520 |
| TNF-α (pg/mL) | −0.17 | −0.62 | 0.28 | 0.440 | −0.05 | −0.50 | 0.39 | 0.804 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kenđel Jovanović, G.; Mrakovcic-Sutic, I.; Pavičić Žeželj, S.; Šuša, B.; Rahelić, D.; Klobučar Majanović, S. The Efficacy of an Energy-Restricted Anti-Inflammatory Diet for the Management of Obesity in Younger Adults. Nutrients 2020, 12, 3583. https://doi.org/10.3390/nu12113583
Kenđel Jovanović G, Mrakovcic-Sutic I, Pavičić Žeželj S, Šuša B, Rahelić D, Klobučar Majanović S. The Efficacy of an Energy-Restricted Anti-Inflammatory Diet for the Management of Obesity in Younger Adults. Nutrients. 2020; 12(11):3583. https://doi.org/10.3390/nu12113583
Chicago/Turabian StyleKenđel Jovanović, Gordana, Ines Mrakovcic-Sutic, Sandra Pavičić Žeželj, Branislav Šuša, Dario Rahelić, and Sanja Klobučar Majanović. 2020. "The Efficacy of an Energy-Restricted Anti-Inflammatory Diet for the Management of Obesity in Younger Adults" Nutrients 12, no. 11: 3583. https://doi.org/10.3390/nu12113583
APA StyleKenđel Jovanović, G., Mrakovcic-Sutic, I., Pavičić Žeželj, S., Šuša, B., Rahelić, D., & Klobučar Majanović, S. (2020). The Efficacy of an Energy-Restricted Anti-Inflammatory Diet for the Management of Obesity in Younger Adults. Nutrients, 12(11), 3583. https://doi.org/10.3390/nu12113583