Telephone-Delivered Dietary Intervention in Patients with Age-Related Macular Degeneration: 3-Month Post-Intervention Findings of a Randomised Controlled Trial

 ,
,  and
and
Abstract
1. Introduction
- present the 3-month post-intervention follow-up results of the RCT;
- report on the feasibility and acceptability of this telehealth programme for AMD patients.
2. Materials and Methods
2.1. Baseline Period
2.2. Intervention Period
2.3. Follow-Up Period
2.4. Outcome Measures
2.5. Analysis
3. Results
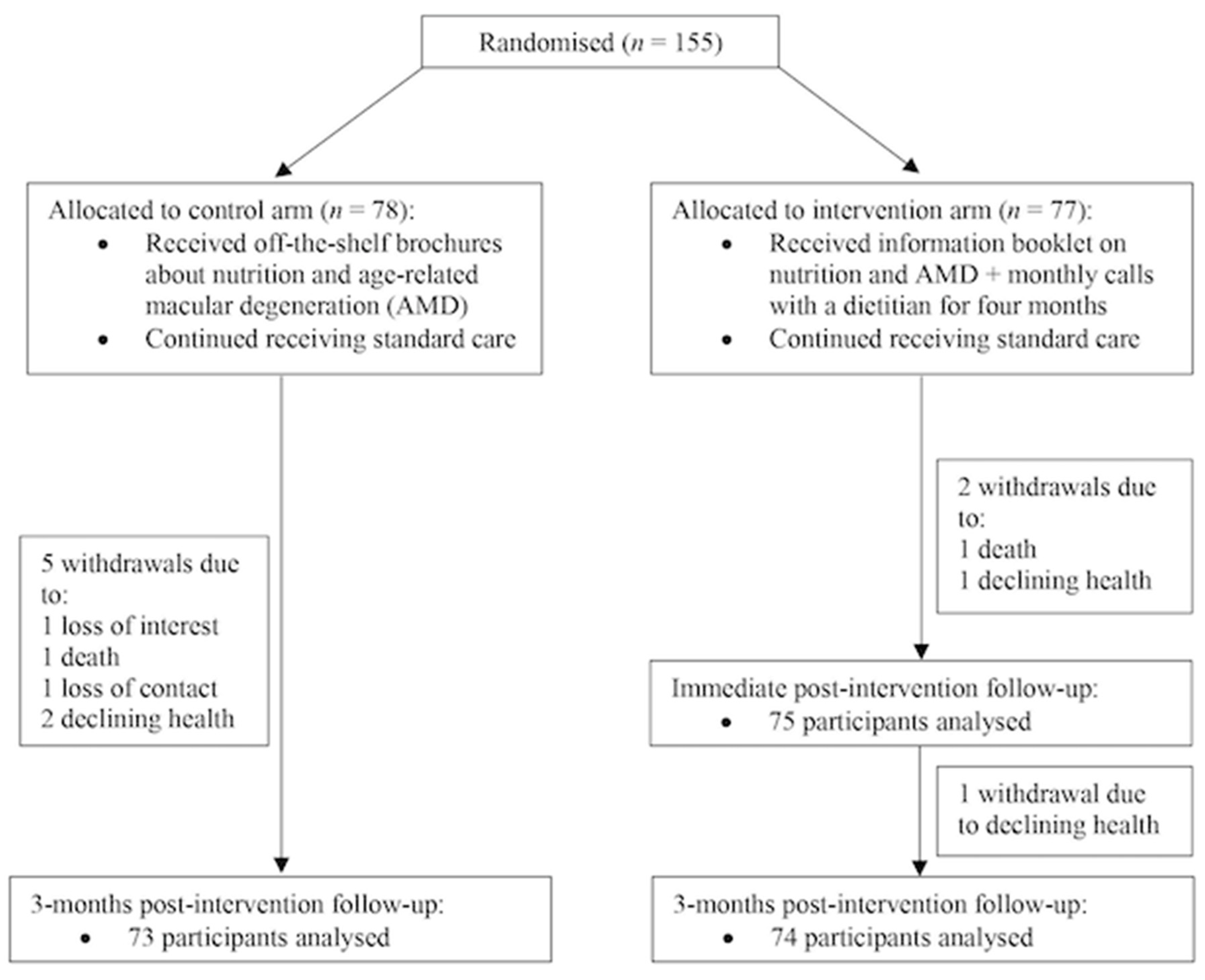
3.1. Participants
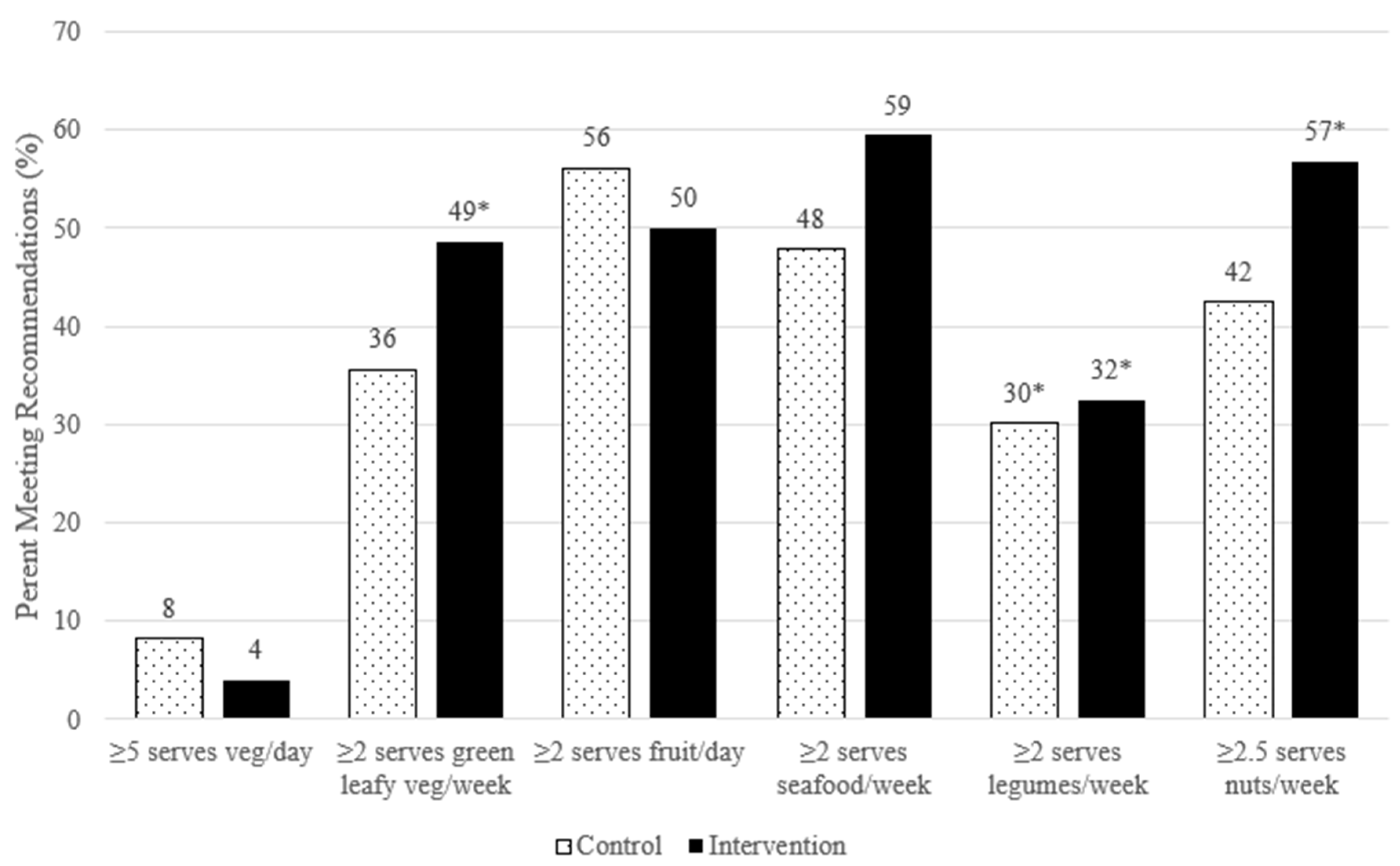
3.2. Dietary Intakes (Expressed as Mean Servings ± SE) between Study Arms
3.3. Dietary Intakes (Expressed as Mean Servings ± SE) within the RCT Arms
Immediately Post-Intervention
Three Months Post-Intervention
3.4. Intervention Adherence and Acceptability
Simple explanations and good suggestions about food substitutes if different foods are not liked or tolerated.(029)
Regular follow up which reinforced diet preference and benefits.(033)
Talking to [the dietitian] when I was getting lazy cooking for myself nightly, encouraged me to go back to a healthy eating practice.(142)
The phone calls review my previous month’s diet. It made me think about what I had eaten and encouraged me to eat better in the next month.(146)
I keep referring to the ‘Dietary Recommendations for AMD’ so that I’ll keep track.(082)
It was more the reminder to keep on the healthy foods and what are the best to have.(053)
I found the dietary sheets very helpful for planning the week meals and shopping.(054)
Confirmation of food choices. Recommendation of foods that were more beneficial.(015)
Although I have a good diet it was useful to get guidance and keep up to date.(108)
Helpful advice...found it reassuring as my diet has always included the foods recommended so now more focused on eating them regularly.(130)
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Mitchell, P.; Liew, G.; Gopinath, B.; Wong, T.Y. Age-related macular degeneration. Lancet 2018, 392, 1147–1159. [Google Scholar] [CrossRef]
- Cimarolli, V.R.; Casten, R.J.; Rovner, B.W.; Heyl, V.; Sörensen, S.; Horowitz, A. Anxiety and depression in patients with advanced macular degeneration: current perspectives. Clin. Ophthalmol. 2015, 10, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Broadhead, G.K.; Grigg, J.R.; Chang, A.A.; McCluskey, P.J. Dietary modification and supplementation for the treatment of age-related macular degeneration. Nutr. Rev. 2015, 73, 448–462. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.S.; Wang, J.J.; Flood, V.; Rochtchina, E.; Smith, W.; Mitchell, P. Dietary Antioxidants and the Long-term Incidence of Age-Related Macular Degeneration. Ophthalmology 2008, 115, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, B.; Natoli, S.; Liew, G.; Flood, V.M. Lutein and Zeaxanthin—Food Sources, Bioavailability and Dietary Variety in Age-Related Macular Degeneration Protection. Nutrients 2017, 9, 120. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.J.; Rochtchina, E.; Smith, W.; Klein, R.; Klein, B.E.K.; Joshi, T.; Sivakumaran, T.A.; Iyengar, S.K.; Mitchell, P. Combined Effects of Complement Factor H Genotypes, Fish Consumption, and Inflammatory Markers on Long-Term Risk for Age-related Macular Degeneration in a Cohort. Am. J. Epidemiol. 2008, 169, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Chew, E.Y.; Clemons, T.E.; SanGiovanni, J.P.; Danis, R.P.; Ferris, F.L.; Elman, M.J.; Antoszyk, A.N.; Ruby, A.J.; Orth, D.; Bressler, S.B.; et al. Secondary Analyses of the Effects of Lutein/Zeaxanthin on Age-Related Macular Degeneration Progression. JAMA Ophthalmol. 2014, 132, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Age-Related Eye Disease Study 2 Research Group Lutein + Zeaxanthin and Omega-3 Fatty Acids for Age-Related Macular Degeneration. JAMA 2013, 309, 2005–2015. [CrossRef]
- Shah, S.U.; Pilli, S.; Telander, D.G.; Morse, L.S.; Park, S.S. Survey of patients with age-related macular degeneration: knowledge and adherence to recommendations. Can. J. Ophthalmol. 2013, 48, 204–209. [Google Scholar] [CrossRef]
- Nunes, S.G.; Alves, D.; Figueira, J.; Santos, L.; Silva, R.; Barreto, P.; Raimundo, M.; Cachulo, M.d.L.; Farinha, C.; Laíns, I.; et al. Adherence to a Mediterranean diet and its association with age-related macular degeneration. The Coimbra Eye Study–Report 4. Nutrition 2018, 51, 6–12. [Google Scholar] [CrossRef]
- Kim, E.K.; Kim, H.; Kwon, O.; Chang, N. Associations between fruits, vegetables, vitamin A, β-carotene and flavonol dietary intake, and age-related macular degeneration in elderly women in Korea: the Fifth Korea National Health and Nutrition Examination Survey. Eur. J. Clin. Nutr. 2017, 72, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Cho, E.; Hung, S.; Willett, W.C.; Spiegelman, D.; Rimm, E.B.; Seddon, J.M.; A Colditz, G.; E Hankinson, S. Prospective study of dietary fat and the risk of age-related macular degeneration. Am. J. Clin. Nutr. 2001, 73, 209–218. [Google Scholar] [CrossRef] [PubMed]
- SanGiovanni, J.P.; Chew, E.Y.; Clemons, T.E.; Davis, M.D.; Ferris, F.L.; Gensler, G.R.; Kurinij, N.; Lindblad, A.S.; Milton, R.C.; Seddon, J.M.; et al. The Relationship of Dietary Lipid Intake and Age-Related Macular Degeneration in a Case-Control Study. Arch. Ophthalmol. 2007, 125, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Islam, F.M.A.; Chong, E.W.; Robman, L.D.; Hodge, A.M.; Guymer, R.H.; Aung, K.-Z.; Makeyeva, G.A.; Baird, P.N.; Hopper, J.L.; English, D.R.; et al. Dietary Patterns and Their Associations with Age-Related Macular Degeneration: The melbourne collaborative cohort study. Ophthalmology 2014, 121, 1428–1434.e2. [Google Scholar] [CrossRef]
- Merle, B.M.; E Silver, R.; Rosner, B.; Seddon, J.M. Adherence to a Mediterranean diet, genetic susceptibility, and progression to advanced macular degeneration: a prospective cohort study. Am. J. Clin. Nutr. 2015, 102, 1196–1206. [Google Scholar] [CrossRef]
- Hogg, R.E.; Woodside, J.V.; McGrath, A.; Young, I.S.; Vioque, J.L.; Chakravarthy, U.; De Jong, P.T.; Rahu, M.; Seland, J.; Soubrane, G.; et al. Mediterranean Diet Score and Its Association with Age-Related Macular Degeneration. Ophthalmology 2017, 124, 82–89. [Google Scholar] [CrossRef]
- Gopinath, B.; Flood, V.M.; Kifley, A.; Liew, G.; Mitchell, P. Smoking, Antioxidant Supplementation and Dietary Intakes among Older Adults with Age-Related Macular Degeneration over 10 Years. PLoS ONE 2015, 10, e0122548. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE). Age-Related Macular Degeneration: NICE Guideline 2018. Available online: https://www.nice.org.uk/guidance/ng82/chapter/Recommendations#information-and-support (accessed on 24 June 2020).
- Ng, W.T.; Goggin, M. Awareness of and compliance with recommended dietary supplement among age-related macular degeneration patients. Clin. Exp. Ophthalmol. 2006, 34, 9–14. [Google Scholar] [CrossRef]
- Lawrenson, J.G.; Evans, J.; Downie, L.E. A Critical Appraisal of National and International Clinical Practice Guidelines Reporting Nutritional Recommendations for Age-Related Macular Degeneration: Are Recommendations Evidence-Based? Nutrients 2019, 11, 823. [Google Scholar] [CrossRef]
- Stevens, R.; Cooke, R.; Bartlett, H. Testing the impact of an educational intervention designed to promote ocular health among people with age-related macular degeneration. Br. J. Vis. Impair. 2018, 36, 110–127. [Google Scholar] [CrossRef]
- Tang, D.; Mitchell, P.; Flood, V.; Kifley, A.; Hayes, A.; Liew, G.; Gopinath, B. Dietary intervention in patients with age-related macular degeneration: protocol for a randomised controlled trial. BMJ Open 2019, 9, e024774. [Google Scholar] [CrossRef] [PubMed]
- Goode, A.; Reeves, M.M.; Eakin, E. Telephone-Delivered Interventions for Physical Activity and Dietary Behavior Change. Am. J. Prev. Med. 2012, 42, 81–88. [Google Scholar] [CrossRef]
- Berg, N.V.D.; Schumann, M.; Kraft, K.; Hoffmann, W. Telemedicine and telecare for older patients—A systematic review. Maturitas 2012, 73, 94–114. [Google Scholar] [CrossRef]
- Kelly, J.T.; Reidlinger, D.P.; Hoffmann, T.C.; Campbell, K.L. Telehealth methods to deliver dietary interventions in adults with chronic disease: a systematic review and meta-analysis. Am. J. Clin. Nutr. 2016, 104, 1693–1702. [Google Scholar] [CrossRef] [PubMed]
- Desroches, S.; Lapointe, A.; Ratté, S.; Gravel, K.; Légaré, F.; Turcotte, S. Interventions to enhance adherence to dietary advice for preventing and managing chronic diseases in adults. Cochrane Database Syst. Rev. 2013, 2013, CD008722. [Google Scholar] [CrossRef]
- Tang, D.; Mitchell, P.; Liew, G.; Burlutsky, G.; Flood, V.M.; Gopinath, B. Evaluation of a Novel Tool for Screening Inadequate Food Intake in Age-Related Macular Degeneration Patients. Nutrients 2019, 11, 3031. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013. [Google Scholar]
- Goldstein, M.G.; Whitlock, E.P.; DePue, J. Multiple behavioral risk factor interventions in primary care. Am. J. Prev. Med. 2004, 27, 61–79. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.K.; DeVellis, B.M.; Strecher, V.J.; Ammerman, A.S.; DeVellis, R.F.; Sandler, R.S. Improving dietary behavior: the effectiveness of tailored messages in primary care settings. Am. J. Public Health 1994, 84, 783–787. [Google Scholar] [CrossRef]
- Pollard, C.M.; Miller, M.R.; Daly, A.M.; E Crouchley, K.; O’Donoghue, K.J.; Lang, A.J.; Binns, C.W. Increasing fruit and vegetable consumption: success of the Western Australian Go for 2&5®campaign. Public Health Nutr. 2008, 11, 314–320. [Google Scholar] [CrossRef]
- Chiu, C.-J.; Klein, R.; Milton, R.C.; Gensler, G.; Taylor, A. Does eating particular diets alter the risk of age-related macular degeneration in users of the Age-Related Eye Disease Study supplements? Br. J. Ophthalmol. 2009, 93, 1241–1246. [Google Scholar] [CrossRef]
- Kaushik, S.; Wang, J.J.; Flood, V.; Tan, J.S.L.; Barclay, A.W.; Wong, T.Y.; Brand-Miller, J.C.; Mitchell, P. Dietary glycemic index and the risk of age-related macular degeneration. Am. J. Clin. Nutr. 2008, 88, 1104–1110. [Google Scholar] [CrossRef] [PubMed]
- Chiu, C.-J.; Milton, R.C.; Klein, R.; Gensler, G.; Taylor, A. Dietary carbohydrate and the progression of age-related macular degeneration: a prospective study from the Age-Related Eye Disease Study. Am. J. Clin. Nutr. 2007, 86, 1210–1218. [Google Scholar] [CrossRef] [PubMed]
- Grains and Legumes Nutrition Council. Lifting the Lid on Legumes: The Benefits of Choosing Legumes 2013. Available online: https://www.glnc.org.au/wp-content/uploads/2011/04/GLN_LiftingtheLid_WEB.pdf (accessed on 29 October 2019).
- Australian Bureau of Statistics. Australian Health Survey: Nutrition First Results—Foods and Nutrients Table 5: Mean Daily Food Intake. 2014. Available online: https://www.abs.gov.au/statistics/health/health-conditions-and-risks/australian-health-survey-nutrition-first-results-foods-and-nutrients/latest-release#data-download (accessed on 24 September 2020).
- Tan, J.S.L.; Wang, J.J.; Flood, V.; Mitchell, P. Dietary Fatty Acids and the 10-Year Incidence of Age-Related Macular Degeneration. Arch. Ophthalmol. 2009, 127, 656–665. [Google Scholar] [CrossRef] [PubMed]
- Gopinath, B.; Liew, G.; Tang, D.; Burlutsky, G.; Flood, V.M.; Mitchell, P. Consumption of eggs and the 15-year incidence of age-related macular degeneration. Clin. Nutr. 2020, 39, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Darmadi-Blackberry, I.; Wahlqvist, M.L.; Kouris-Blazos, A.; Steen, B.; Lukito, W.; Horie, Y.; Horie, K. Legumes: The most important dietary predictor of survival in older people of different ethnicities—PubMed. Asia Pac. J. Clin. Nutr. 2004, 13, 217–220. [Google Scholar] [PubMed]
- Sahyoun, N.R.; Pratt, C.A.; Anderson, A. Evaluation of nutrition education interventions for older adults: a proposed framework. J. Am. Diet. Assoc. 2004, 104, 58–69. [Google Scholar] [CrossRef] [PubMed]
- Bandayrel, K.; Wong, S. Systematic Literature Review of Randomized Control Trials Assessing the Effectiveness of Nutrition Interventions in Community-Dwelling Older Adults. J. Nutr. Educ. Behav. 2011, 43, 251–262. [Google Scholar] [CrossRef]
- Wosik, J.; Fudim, M.; Cameron, B.; Gellad, Z.F.; Cho, A.; Phinney, D.; Curtis, S.; Roman, M.; Poon, E.G.; Ferranti, J.; et al. Telehealth transformation: COVID-19 and the rise of virtual care. J. Am. Med Informatics Assoc. 2020, 27, 957–962. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline Characteristics | Intervention (n = 77) | Control (n = 78) | p-Value |
|---|---|---|---|
| Age (years) | 78.1 ± 8.1 | 77.9 ± 8.5 | 0.88 |
| Sex (% female) | 50.7 | 64.1 | 0.09 |
| Weight (kg) | 75.0 ± 15.6 | 70.7 ± 14.0 | 0.08 |
| Height (cm) | 167.2 ± 11.5 | 161.5 ± 9.5 | 0.002 |
| BMI (kg/m2) | 26.8 ± 4.9 | 27.0 ± 5.4 | 0.82 |
| Type of age-related macular degeneration (AMD): | |||
| No. eyes with early AMD | 6 | 0 | |
| No. eyes with any late AMD | 94 | 104 | 0.01 |
| Cardiovascular disease (n, %) | 29.0 (37.7) | 26.0 (33.3) | 0.57 |
| Stroke (n, %) | 8.0 (10.4) | 7.0 (9.0) | 0.77 |
| High blood pressure (n, %) | 49.0 (63.6) | 49.0 (62.8) | 0.92 |
| High cholesterol (n, %) | 41.0 (53.3) | 38.0 (50.7) | 0.75 |
| Diabetes (n, %) | 15.0 (19.7) | 21.0 (26.9) | 0.29 |
| Kidney disease (n, %) | 6.0 (7.8) | 4.0 (5.2) | 0.51 |
| Physical activity (h/week) | 3.6 ± 4.0 | 4.4 ± 7.7 | 0.41 |
| No. smokers (%) | 34 (44.7) | 28 (35.9) | 0.35 |
| Intervention (n = 74) | Control (n = 73) | Mean Difference (Intervention–Control) at 3 Months Post-Intervention | ||||||
|---|---|---|---|---|---|---|---|---|
| Baseline Mean Servings ± SE* | 3 Months Post-Intervention Mean Servings ± SE | p-Value | Baseline Mean Servings ± SE | 3 Months Post-Intervention Mean Servings ± SE | p-Value | Mean Difference ± SE | p-Value | |
| Intake reported (per day): | ||||||||
| Total vegetables | 2.15 ± 0.16 | 2.01 ± 0.17 | 0.47 | 2.12 ± 0.13 | 2.28 ± 0.21 | 0.43 | −0.28 ± 0.27 | 0.31 |
| Fruit | 1.88 ± 0.13 | 1.84 ± 0.14 | 0.73 | 1.72 ± 0.12 | 1.85 ± 0.15 | 0.23 | −0.02 ± 0.20 | 0.93 |
| Water | 4.64 ± 0.26 | 4.73 ± 0.34 | 0.71 | 4.76 ± 0.27 | 4.47 ± 0.50 | 0.51 | 0.26 ± 0.67 | 0.67 |
| Intake reported (per week): | ||||||||
| Dark green leafy vegetables | 0.99 ± 0.17 | 1.71 ± 0.22 | 0.003 | 1.16 ± 0.25 | 1.32 ± 0.20 | 0.53 | 0.39 ± 0.29 | 0.19 |
| Cooked green vegetables | 3.92 ± 0.50 | 3.68 ± 0.30 | 0.65 | 4.16 ± 0.51 | 3.53 ± 0.29 | 0.23 | 0.15 ± 0.42 | 0.72 |
| Red meat | 2.06 ± 0.16 | 2.37 ± 0.20 | 0.11 | 2.29 ± 0.20 | 2.44 ± 0.26 | 0.58 | −0.07 ± 0.33 | 0.82 |
| Processed meat | 1.41 ± 0.20 | 1.39 ± 0.20 | 0.97 | 1.14 ± 0.16 | 1.35 ± 0.15 | 0.24 | 0.05 ± 0.25 | 0.86 |
| Fish/seafood | 1.75 ± 0.17 | 2.02 ± 0.18 | 0.17 | 1.73 ± 0.16 | 1.82 ± 0.22 | 0.68 | 0.20 ± 0.29 | 0.49 |
| Legumes | 0.69 ± 0.10 | 1.12 ± 0.16 | 0.02 | 0.84 ± 0.14 | 1.16 ± 0.17 | 0.08 | −0.04 ± 0.24 | 0.86 |
| Nuts | 3.29 ± 0.5 | 3.96 ± 0.51 | 0.15 | 3.27 ± 0.39 | 2.71 ± 0.32 | 0.06 | 1.25 ± 0.60 | 0.04 |
| Eggs | 3.34 ± 0.25 | 2.92 ± 0.24 | 0.14 | 2.72 ± 0.24 | 2.47 ± 0.25 | 0.25 | 0.46 ± 0.34 | 0.18 |
| Bread: | ||||||||
| Wholemeal, grain, rye, sourdough | 5.06 ± 0.50 | 4.71 ± 0.48 | 0.58 | 4.53 ± 0.53 | 4.26 ± 0.63 | 0.49 | 0.46 ± 0.63 | 0.47 |
| White | 1.41 ± 0.30 | 1.33 ± 0.30 | 0.85 | 1.63 ± 0.31 | 1.73 ± 0.31 | 0.72 | −0.41 ± 0.43 | 0.35 |
| Cakes, biscuits, ice cream, processed potato, takeaway, sugar-sweetened beverages | 8.31 ± 0.76 | 6.54 ± 0.58 | 0.01 | 8.82 ± 0.82 | 6.84 ± 0.62 | 0.0003 | −0.30 ± 0.85 | 0.73 |
| Alcohol | 3.72 ± 0.83 | 2.93 ± 0.53 | 0.30 | 2.18 ± 0.48 | 2.58 ± 0.51 | 0.40 | 0.35 ± 0.74 | 0.64 |
| Fats and oils: | ||||||||
| Olive oil | 2.14 ± 0.28 | 2.05 ± 0.28 | 0.71 | 2.58 ± 0.30 | 2.59 ± 0.31 | 0.98 | −0.54 ± 0.42 | 0.20 |
| Other | 5.72 ± 0.44 | 5.48 ± 0.39 | 0.59 | 6.57 ± 0.45 | 6.31 ± 0.50 | 0.57 | −0.83 ± 0.63 | 0.19 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tang, D.; Mitchell, P.; Liew, G.; Burlutsky, G.; Flood, V.M.; Gopinath, B. Telephone-Delivered Dietary Intervention in Patients with Age-Related Macular Degeneration: 3-Month Post-Intervention Findings of a Randomised Controlled Trial. Nutrients 2020, 12, 3083. https://doi.org/10.3390/nu12103083
Tang D, Mitchell P, Liew G, Burlutsky G, Flood VM, Gopinath B. Telephone-Delivered Dietary Intervention in Patients with Age-Related Macular Degeneration: 3-Month Post-Intervention Findings of a Randomised Controlled Trial. Nutrients. 2020; 12(10):3083. https://doi.org/10.3390/nu12103083
Chicago/Turabian StyleTang, Diana, Paul Mitchell, Gerald Liew, George Burlutsky, Victoria M. Flood, and Bamini Gopinath. 2020. "Telephone-Delivered Dietary Intervention in Patients with Age-Related Macular Degeneration: 3-Month Post-Intervention Findings of a Randomised Controlled Trial" Nutrients 12, no. 10: 3083. https://doi.org/10.3390/nu12103083
APA StyleTang, D., Mitchell, P., Liew, G., Burlutsky, G., Flood, V. M., & Gopinath, B. (2020). Telephone-Delivered Dietary Intervention in Patients with Age-Related Macular Degeneration: 3-Month Post-Intervention Findings of a Randomised Controlled Trial. Nutrients, 12(10), 3083. https://doi.org/10.3390/nu12103083