Assessing Validity of Self-Reported Dietary Intake within a Mediterranean Diet Cluster Randomized Controlled Trial among US Firefighters

 , , ,
, , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
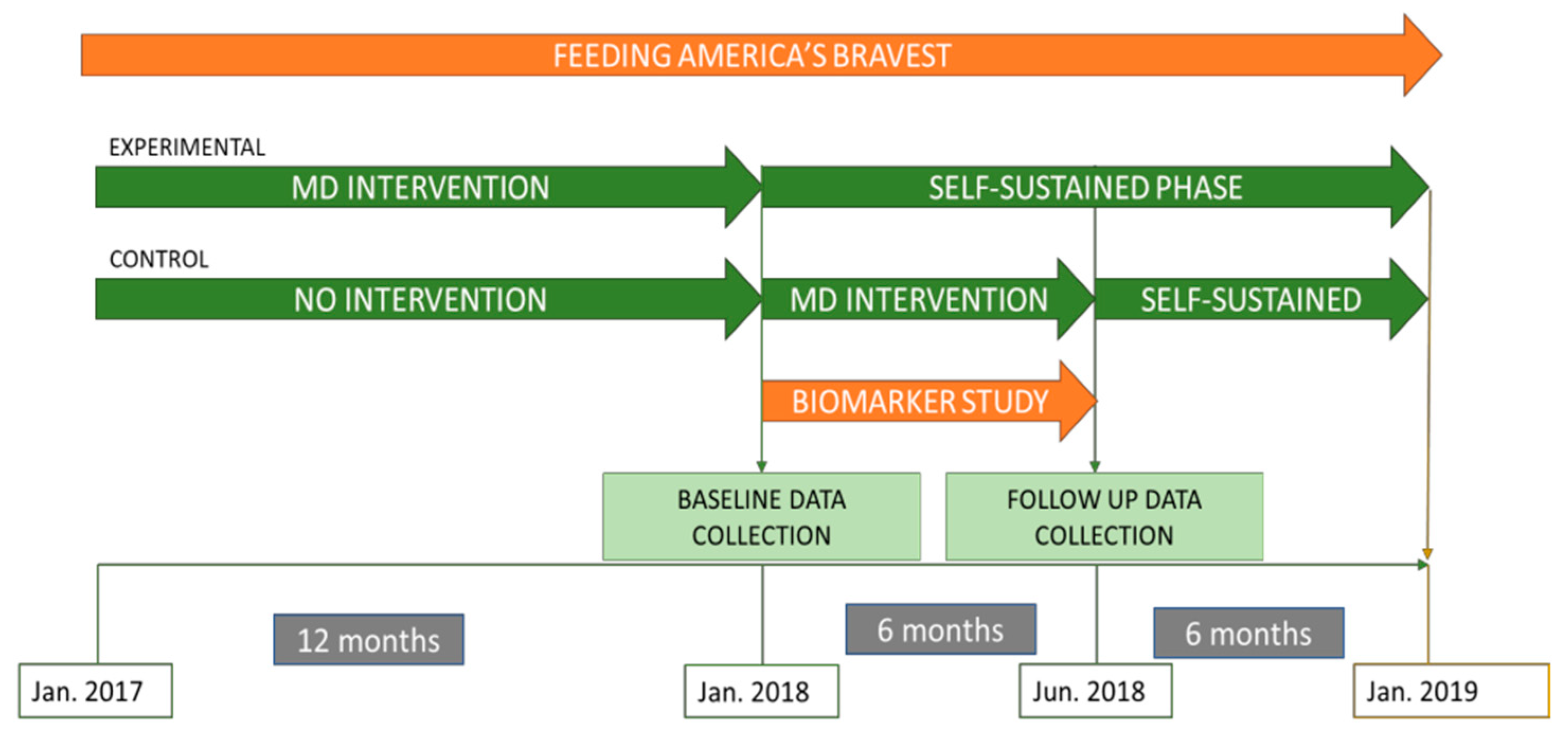
2.1. Study Design
2.2. Study Population
2.3. Diet Assessment
2.4. Biomarker Assessment
2.5. Statistical Analysis
3. Results
3.1. Participants Characteristics
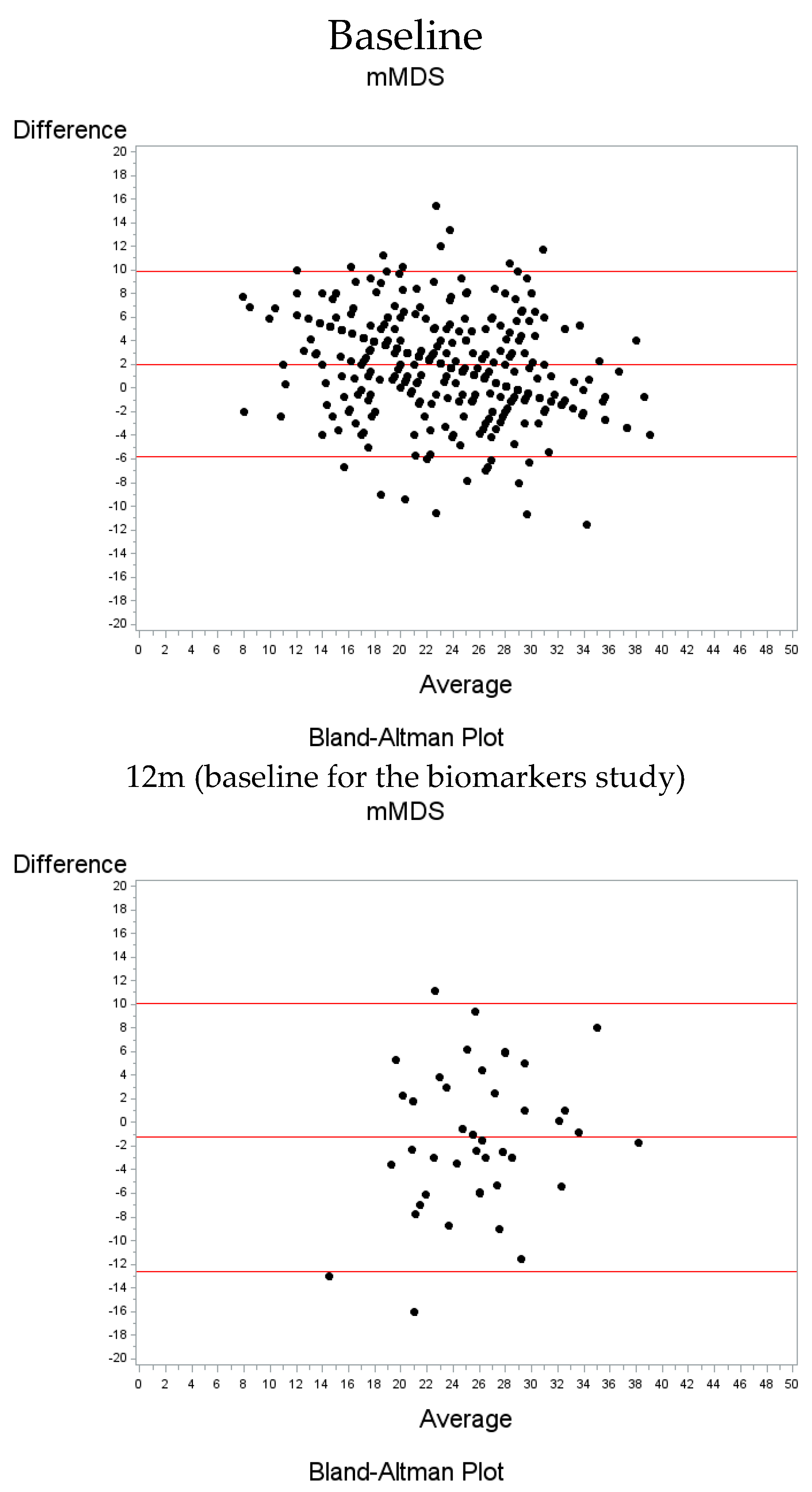
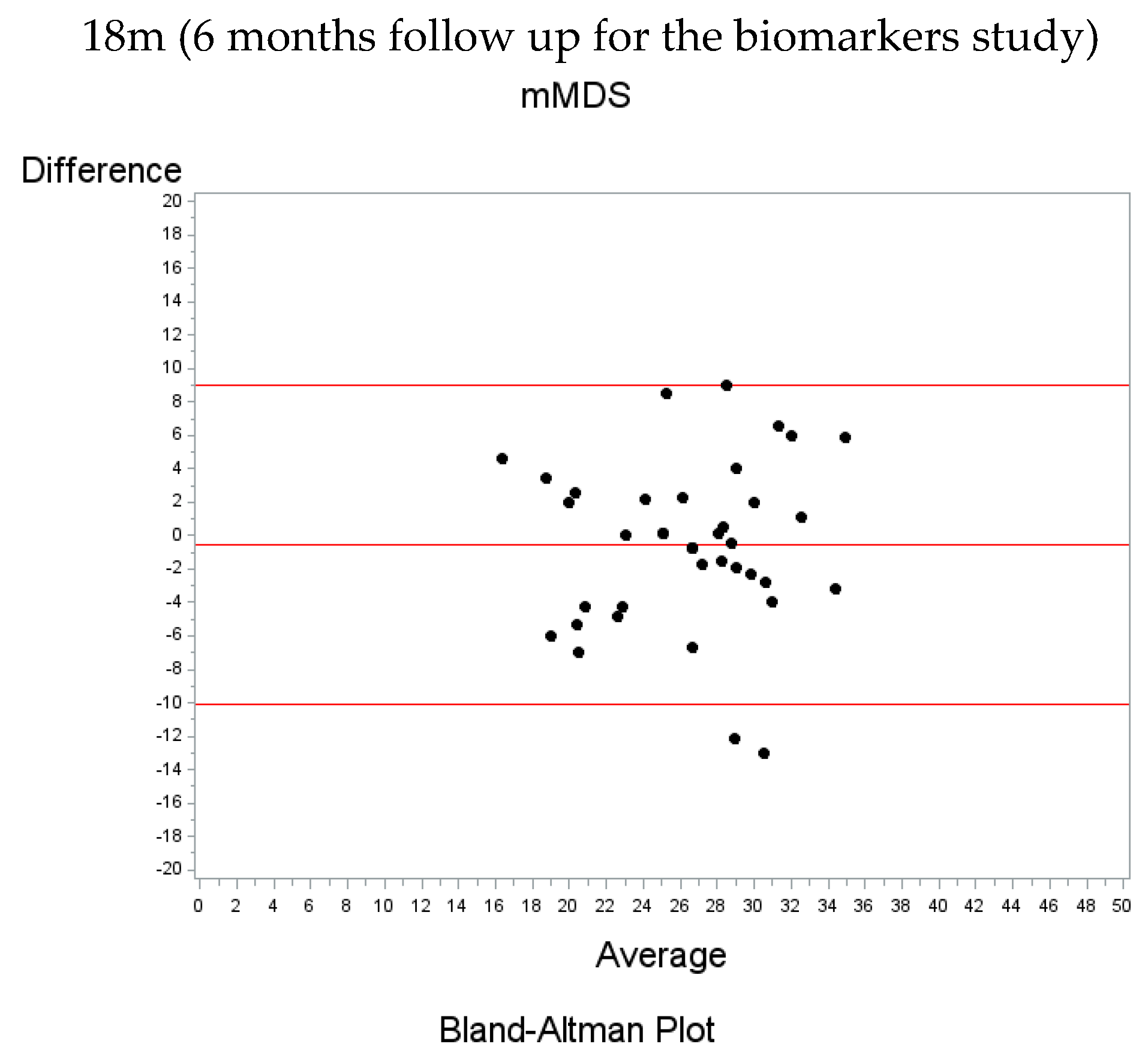
3.2. Modified Mediterranean Diet Score Agreement
3.3. Plasma and Urine Biomarkers Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Freedman, L.S.; Commins, J.M.; Moler, J.E.; Arab, L.; Baer, D.J.; Kipnis, V.; Midthune, D.; Moshfegh, A.J.; Neuhouser, M.L.; Prentice, R.L.; et al. Pooled Results From 5 Validation Studies of Dietary Self-Report Instruments Using Recovery Biomarkers for Energy and Protein Intake. Am. J. Epidemiol. 2014, 180, 172–188. [Google Scholar] [CrossRef] [PubMed]
- Ortega, R.M. Dietary assessment methods: Dietary records. Nutr. Hosp. 2015, 31, 38–45. [Google Scholar] [PubMed]
- Dragsted, L.O.; Gao, Q.; Praticò, G.; Manach, C.; Wishart, D.S.; Scalbert, A.; Feskens, E.J.M. Dietary and health biomarkers—Time for an update. Genes Nutr. 2017, 12, 24. [Google Scholar] [CrossRef] [PubMed]
- Freedman, L.S.; Commins, J.M.; Willett, W.; Tinker, L.F.; Spiegelman, D.; Rhodes, D.; Potischman, N.; Neuhouser, M.L.; Moshfegh, A.J.; Kipnis, V.; et al. Evaluation of the 24-Hour Recall as a Reference Instrument for Calibrating Other Self-Report Instruments in Nutritional Cohort Studies: Evidence From the Validation Studies Pooling Projec. Am. J. Epidemiol. 2017, 186, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Kuhnle, G.G.C. Biomarkers of Intake. In Nutrition Research Methodologies; Wiley-Blackwell: Hoboken, NJ, USA, 2015; pp. 90–107. ISBN 978-1-119-18042-5. [Google Scholar]
- Yang, J.; Farioli, A.; Korre, M.; Kales, S.N. Modified Mediterranean Diet Score and Cardiovascular Risk in a North American Working Population. PLoS ONE 2014, 9, e87539. [Google Scholar] [CrossRef]
- Sotos-Prieto, M.; Cash, S.B.; Christophi, C.A.; Folta, S.; Moffatt, S.; Muegge, C.; Korre, M.; Mozaffarian, D.; Kales, S.N. Rationale and design of feeding America’s bravest: Mediterranean diet-based intervention to change firefighters’ eating habits and improve cardiovascular risk profiles. Contemp. Clin. Trials 2017, 61, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Sotos-Prieto, M.; Jin, Q.; Rainey, D.; Coyle, M.; Kales, S.N. Barriers and solutions to improving nutrition among fire academy recruits: A qualitative assessment. Int. J. Food Sci. Nutr. 2019, 70, 771–779. [Google Scholar] [CrossRef]
- Baylin, A.; Kim, M.K.; Donovan-Palmer, A.; Siles, X.; Dougherty, L.; Tocco, P.; Campos, H. Fasting Whole Blood as a Biomarker of Essential Fatty Acid Intake in Epidemiologic Studies: Comparison with Adipose Tissue and Plasma. Am. J. Epidemiol. 2005, 162, 373–381. [Google Scholar] [CrossRef]
- Chang, N.W.; Huang, P.C. Effects of dietary monounsaturated fatty acids on plasma lipids in humans. J. Lipid Res. 1990, 31, 2141–2147. [Google Scholar]
- Hodge, A.M.; Simpson, J.A.; Gibson, R.A.; Sinclair, A.J.; Makrides, M.; O’Dea, K.; English, D.R.; Giles, G.G. Plasma phospholipid fatty acid composition as a biomarker ofhabitual dietary fat intake in an ethnically diverse cohort. Nutr. Metab. Cardiovasc. Dis. 2007, 17, 415–426. [Google Scholar] [CrossRef]
- Hodson, L.; Skeaff, C.M.; Fielding, B.A. Fatty acid composition of adipose tissue and blood in humans and its use as a biomarker of dietary intake. Prog. Lipid Res. 2008, 47, 348–380. [Google Scholar] [CrossRef] [PubMed]
- Poppitt, S.D.; Kilmartin, P.; Butler, P.; Keogh, G.F. Assessment of erythrocyte phospholipid fatty acid composition as a biomarker for dietary MUFA, PUFA orsaturated fatty acid intake in a controlled cross-over intervention trial. Lipids Health Dis. 2005, 4, 30. [Google Scholar] [CrossRef] [PubMed]
- Skeaff, C.M.; Hodson, L.; McKenzie, J.E. Dietary-Induced Changes in Fatty Acid Composition of Human Plasma, Platelet, and Erythrocyte Lipids Follow a Similar Time 461 Course. J. Nutr. 2006, 136, 565–569. [Google Scholar] [CrossRef] [PubMed]
- Warensjö Lemming, E.; Nälsén, C.; Bec ker, W.; Ridefelt, P.; Mattisson, I.; Lindroos, A.K. Relative validation of the dietary intake of fatty acids among adults in the SwedishNational Dietary Survey using plasma phospholipid fatty acid composition. J. Nutr. Sci. 2015, 4, e25. [Google Scholar] [CrossRef] [PubMed]
- Miró-Casas, E.; Covas, M.-I.; Fitó, M.; Farré-Albadalejo, M.; Marrugat, J.; de la Torre, R. Tyrosol and hydroxytyrosol are absorbed from moderate and sustained doses of virginolive oil in humans. Eur. J. Clin. Nutr. 2003, 57, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Zazpe, I.; Sanchez-Tainta, A.; Estruch, R.; Lamuela-Raventos, R.M.; Schröder, H.; Salas-Salvado, J.; Corella, D.; Fiol, M.; Gomez-Gracia, E.; Aros, F.; et al. A LargeRandomized Individual and Group Intervention Conducted by Registered DietitiansIncreased Adherence to Mediterranean-Type Diets: The PREDIMED Study. J. Am. Diet. Assoc. 2008, 108, 1134–1144. [Google Scholar] [CrossRef]
- Estruch, R. Anti-inflammatory effects of the Mediterranean diet: The experience of the PREDIMED study. Proc. Nutr. Soc. 2010, 69, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Hermsdorff, H.H.M.; Zulet, M.Á.; Abete, I.; Martníez, J.A. Discriminated benefits of aMediterranean dietary pattern within a hypocaloric diet program on plasma RBP4 concentrations and other inflammatory markers in obese subjects. Endocrine 2009, 36, 445–479. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: Aystematic review and meta-analysis of observational studies. Int. J. Cancer 2014, 135, 1884–1897. [Google Scholar] [CrossRef]
- Durand, G.; Tsismenakis, A.J.; Jahnke, S.A.; Baur, D.M.; Christophi, C.A.; Kales, S.N. Firefighters’ Physical Activity: Relation to Fitness and Cardiovascular Disease Risk. Med. Sci. Sports Exerc. 2011, 43, 1752–1759. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.S.; Blair, S.N.; Mahar, M.T.; Wier, L.T.; Ross, R.; Stuteville, J.E. Prediction of functional aerobic capacity without exercise testing. Med. Sci. Sports Exerc. 1990, 22, 863–870. [Google Scholar] [CrossRef]
- Willett, W.C.; Sampson, L.; Stampfer, M.J.; Rosner, B.; Bain, C.; Witschi, J.; Hennekens, C.H.; Speizer, F.E. Reproducibility and validity of a semiquantitative food frequency questionnaire. Am. J. Epidemiol. 1985, 122, 51–65. [Google Scholar] [CrossRef] [PubMed]
- Chiuve, S.E.; Fung, T.T.; Rimm, E.B.; Hu, F.B.; McCullough, M.L.; Wang, M.; Stampfer, M.J.; Willett, W.C. Alternative dietary indices both strongly predict risk of chronic disease. J. Nutr. 2012, 142, 1009–1018. [Google Scholar] [CrossRef]
- Salvini, S.; Hunter, D.J.; Sampson, L.; Stampfer, M.J.; Colditz, G.A.; Rosner, B.; Willett, W.C. Food-based validation of a dietary questionnaire: The effects of week-to-week variation in food consumption. Int. J. Epidemiol. 1989, 18, 858–867. [Google Scholar] [CrossRef] [PubMed]
- Zock, P.L.; Gerritsen, J.; Katan, M.B. Partial conservation of the sn-2 position of dietary triglycerides in fasting plasma lipids in humans. Eur. J. Clin. Investig. 1996, 26, 141–150. [Google Scholar] [CrossRef]
- Zock, P.L.; Mensink, R.P.; Harryvan, J.; de Vries, J.H.; Katan, M.B. Fatty acids in serum cholesteryl esters as quantitative biomarkers of dietary intake in humans. Am. J. Epidemiol. 1997, 145, 1114–1122. [Google Scholar] [CrossRef]
- Miró-Casas, E.; Farré Albaladejo, M.; Covas, M.-I.; Rodriguez, J.O.; Menoyo Colomer, E.; Lamuela Raventós, R.M.; de la Torre, R. Capillary Gas Chromatography–Mass Spectrometry Quantitative Determination of Hydroxytyrosol and Tyrosol in Human Urine after Olive Oil Intake. Anal. Biochem. 2001, 294, 63–72. [Google Scholar] [CrossRef]
- Lu, L.; Shara, N. Reliability Analysis: Calculate and Compare Intraclass Correlation Coefficients (ICC) in SAS. 2007. Available online: https://pdfs.semanticscholar.org/26e8/939dbe0fa9c9ba8257b4996b840a87e6b455.pdf (accessed on 6 November 2018).
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A Short Screener Is Valid for Assessing Mediterranean Diet Adherence among Older Spanish Men and Women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef]
- Toutenburg, H.; Fleiss, J.L. Statistical Methods for Rates and Proportions. John Wiley & Sons, New York-London-Sydney-Toronto 1973. XIII, 233 S. Biom. Z. 1974, 16, 539. [Google Scholar]
- Ashby, D. Practical statistics for medical research. Douglas, G.; Altman, Chapman and Hall, London, 1991. No. of pages: 611. Price: £32.00. Stat. Med. 1991, 10, 1635–1636. [Google Scholar] [CrossRef]
- Miura, K.; Entwistle, T.R.; Fildes, J.E.; Green, A.C. Relative validity of short questionnaires to assess Mediterranean diet or low-fat diet adherence. J. Aging Res. Clin. Pract. 2017, 6, 23–27. [Google Scholar]
- Sotos-Prieto, M. Validation of a questionnaire to measure overall mediterranean lifestyle habits for research application: The mediterranean lifestyle index (MEDLIFE). Nutr. Hosp. 2015, 32, 1153–1163. [Google Scholar] [PubMed]
- Hebestreit, K.; Yahiaoui-Doktor, M.; Engel, C.; Vetter, W.; Siniatchkin, M.; Erickson, N.; Halle, M.; Kiechle, M.; Bischoff, S.C. Validation of the German version of the Mediterranean Diet Adherence Screener (MEDAS) questionnaire. BMC Cancer 2017, 17, 341. [Google Scholar] [CrossRef] [PubMed]
- Sotos-Prieto, M.; Moreno-Franco, B.; Ordovás, J.M.; León, M.; Casasnovas, J.A.; Peñalvo, J.L. Design and development of an instrument to measure overall lifestyle habits for epidemiological research: The Mediterranean Lifestyle (MEDLIFE) index. Public Health Nutr. 2015, 18, 959–967. [Google Scholar] [CrossRef] [PubMed]
- Thompson, F.E.; Subar, A.F.; Brown, C.C.; Smith, A.F.; Sharbaugh, C.O.; Jobe, J.B.; Mittl, B.; Gibson, J.T.; Ziegler, R.G. Cognitive research enhances accuracy of food frequency questionnaire reports: Results of an experimental validation study. J. Am. Diet. Assoc. 2002, 102, 212–225. [Google Scholar] [CrossRef]
- Barceló, F.; Perona, J.S.; Prades, J.; Funari, S.S.; Gomez-Gracia, E.; Conde, M.; Estruch, R.; Ruiz-Gutiérrez, V. Mediterranean-Style Diet Effect on the Structural Properties of the Erythrocyte Cell Membrane of Hypertensive Patients: The Prevencion con Dieta Mediterranea Study. Hypertension 2009, 54, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Santangelo, C.; Filesi, C.; Varì, R.; Scazzocchio, B.; Filardi, T.; Fogliano, V.; D’Archivio, M.; Giovannini, C.; Lenzi, A.; Morano, S.; et al. Consumption of extra-virgin olive oil rich in phenolic compounds improves metabolic control in patients with type 2 diabetes mellitus: A possible involvement of reduced levels of circulating visfatin. J. Endocrinol. Investig. 2016, 39, 1295–1301. [Google Scholar] [CrossRef]
- Rozati, M.; Barnett, J.; Wu, D.; Handelman, G.; Saltzman, E.; Wilson, T.; Li, L.; Wang, J.; Marcos, A.; Ordovás, J.M.; et al. Cardio-metabolic and immunological impacts of extra virgin olive oil consumption in overweight and obese older adults: A randomized controlled trial. Nutr. Metab. 2015, 12, 28. [Google Scholar] [CrossRef]
- Yarla, N.S.; Polito, A.; Peluso, I. Effects of Olive Oil on TNF-α and IL-6 in Humans: Implication in Obesity and Frailty. Available online: http://www.eurekaselect.com/157385/article (accessed on 6 November 2018).
- De la Torre, R.; Covas, M.I.; Pujadas, M.A.; Fitó, M.; Farré, M. Is dopamine behind the health benefits of red wine? Eur. J. Nutr. 2006, 45, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Seah, J.Y.H.; Gay, G.M.W.; Su, J.; Tai, E.-S.; Yuan, J.-M.; Koh, W.-P.; Ong, C.N.; Van Dam, R.M. Consumption of Red Meat, but Not Cooking Oils High in Polyunsaturated Fat, Is Associated with Higher Arachidonic Acid Status in Singapore Chinese Adults. Nutrients 2017, 9, 101. [Google Scholar] [CrossRef] [PubMed]
- King, I.B.; Lemaitre, R.N.; Kestin, M. Effect of a low-fat diet on fatty acid composition in red cells, plasma phospholipids, and cholesterol esters: Investigation of a biomarker of total fat intake. Am. J. Clin. Nutr. 2006, 83, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Simopoulos, A.P. An Increase in the Omega-6/Omega-3 Fatty Acid Ratio Increases the Risk for Obesity. Nutrients 2016, 8, 128. [Google Scholar] [CrossRef] [PubMed]
- Fretts, A.M.; Mozaffarian, D.; Siscovick, D.S.; Djousse, L.; Heckbert, S.R.; King, I.B.; McKnight, B.; Sitlani, C.; Sacks, F.M.; Song, X.; et al. Plasma Phospholipid Saturated Fatty Acids and Incident Atrial Fibrillation: The Cardiovascular Health Study. J. Am. Heart Assoc. 2014, 3, e000889. [Google Scholar] [CrossRef] [PubMed]
- Forsythe, C.E.; Phinney, S.D.; Feinman, R.D.; Volk, B.M.; Freidenreich, D.; Quann, E.; Ballard, K.; Puglisi, M.J.; Maresh, C.M.; Kraemer, W.J.; et al. Limited effect of dietary saturated fat on plasma saturated fat in the context of a low carbohydrate diet. Lipids 2010, 45, 947–962. [Google Scholar] [CrossRef] [PubMed]
- Takkunen, M.; Agren, J.; Kuusisto, J.; Laakso, M.; Uusitupa, M.; Schwab, U. Dietary fat in relation to erythrocyte fatty acid composition in men. Lipids 2013, 48, 1093–1102. [Google Scholar] [CrossRef] [PubMed]
- Mena, M.-P.; Sacanella, E.; Vazquez-Agell, M.; Morales, M.; Fitó, M.; Escoda, R.; Serrano-Martínez, M.; Salas-Salvadó, J.; Benages, N.; Casas, R.; et al. Inhibition of circulating immune cell activation: A molecular antiinflammatory effect of the Mediterranean diet. Am. J. Clin. Nutr. 2009, 89, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Van Bussel, B.C.T.; Henry, R.M.A.; Schalkwijk, C.G.; Ferreira, I.; Feskens, E.J.M.; Streppel, M.T.; Smulders, Y.M.; Twisk, J.W.R.; Stehouwer, C.D.A. Fish Consumption in Healthy Adults Is Associated with Decreased Circulating Biomarkers of Endothelial Dysfunction and Inflammation during a 6-Year Follow-Up. J. Nutr. 2011, 141, 1719–1725. [Google Scholar] [CrossRef] [PubMed]
- Akbaraly, T.; Würtz, P.; Singh-Manoux, A.; Shipley, M.J.; Haapakoski, R.; Lehto, M.; Desrumaux, C.; Kähönen, M.; Lehtimäki, T.; Mikkilä, V.; et al. Association of circulating metabolites with healthy diet and risk of cardiovascular disease: Analysis of two cohort studies. Sci. Rep. 2018, 8, 8620. [Google Scholar] [CrossRef]
- Lenighan, Y.M.; Nugent, A.P.; Li, K.F.; Brennan, L.; Walton, J.; Flynn, A.; Roche, H.M.; McNulty, B.A. Processed red meat contribution to dietary patterns and the associated cardio-metabolic outcomes. Br. J. Nutr. 2017, 118, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Toffano, R.B.D.; Hillesheim, E.; Mathias, M.G.; Coelho-Landell, C.A.; Salomão, R.G.; Almada, M.O.R.V.; Camarneiro, J.M.; Barros, T.T.; Camelo-Junior, J.S.; Rezzi, S.; et al. Validation of the Brazilian Healthy Eating Index-Revised Using Biomarkers in Children and Adolescents. Nutrients 2018, 10, 154. [Google Scholar] [CrossRef] [PubMed]
- Vyncke, K.; Cruz Fernandez, E.; Fajó-Pascual, M.; Cuenca-García, M.; De Keyzer, W.; Gonzalez-Gross, M.; Moreno, L.A.; Beghin, L.; Breidenassel, C.; Kersting, M.; et al. Validation of the Diet Quality Index for Adolescents by comparison with biomarkers, nutrient and food intakes: The HELENA study. Br. J. Nutr. 2013, 109, 2067–2078. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Overall Feeding America’s Bravest | Pilot –Biomarkers Study (Baseline) | |||||||
|---|---|---|---|---|---|---|---|---|
| All (n = 420) | Control (n = 214) | Intervention (n = 206) | p-Value | All (n = 48) | Control (n = 24) | Intervention (n = 24) | p-Value | |
| Age (years) | 48.36 ± 8.29 | 49.02 ± 7.86 | 47.67 ± 8.68 | 0.096 | 47.52 ± 7.63 | 47.58 ± 8.63 | 47.46 ± 6.67 | 0.955 |
| Gender | 0.140 | 0.520 | ||||||
| Males | 250 (94.7%) | 122 (96.8%) | 128 (92.8%) | 38 (92.7%) | 20 (95.2%) | 18 (90.0%) | ||
| Females | 14 (5.3%) | 4 (3.2%) | 10 (7.2%) | 3 (7.3%) | 1 (4.8%) | 2 (10.0%) | ||
| Race | 0.003 | 0.563 | ||||||
| Caucasian | 217 (82.8%) | 112 (89.6%) | 105 (76.6%) | 31 (79.5%) | 16 (80.0%) | 15 (78.9%) | ||
| African American | 39 (14.9%) | 9 (7.2%) | 30 (21.9%) | 7 (17.9%) | 3 (15.0%) | 4 (21.1%) | ||
| Other | 6 (2.3%) | 4 (3.2%) | 2 (1.5%) | 1 (2.6%) | 1 (5.0%) | 0 (0.0%) | ||
| BMI (kg/m2) | 29.97 ± 4.48 | 30.13 ± 4.47 | 29.80 ± 4.50 | 0.447 | 29.68 ± 3.50 | 31.13 ± 3.07 | 28.24 ± 3.35 | 0.003 |
| BMI group | 0.785 | 0.094 | ||||||
| 18.5–25 | 49 (11.9%) | 24 (11.4%) | 25 (12.4%) | 5 (10.4%) | 1 (4.2%) | 4 (16.7%) | ||
| 25–30 | 185 (44.8%) | 98 (46.4%) | 87 (43.1%) | 20 (41.7%) | 8 (33.3%) | 12 (50.0%) | ||
| 30+ | 179 (43.3%) | 89 (42.2%) | 90 (44.6%) | 23 (47.9%) | 15 (62.5%) | 8 (33.3%) | ||
| Smoking | 0.433 | 0.520 | ||||||
| Yes | 11 (4.2%) | 4 (3.1%) | 7 (5.1%) | 3 (7.3%) | 1 (4.8%) | 2 (10.0%) | ||
| No | 254 (95.8%) | 123 (96.9%) | 131 (94.9%) | 38 (92.7%) | 20 (95.2%) | 18 (90.0%) | ||
| Overall mMDS (0–51 points) | 24.08 ± 5.73 | 24.38 ± 5.61 | 23.78 ± 5.85 | 0.284 | 25.02 ± 5.79 | 26.00 ± 5.00 | 24.04 ± 6.44 | 0.245 |
| FFQ-derived mMDS | 22.05 ± 6.89 | 21.95 ± 6.97 | 22.16 ± 6.82 | 0.753 | 26.42 ± 4.79 | 27.88 ± 4.78 | 24.96 ± 4.44 | 0.034 |
| CRP (ngmL) | N/A | N/A | N/A | 1733 ± 2041 | 1640 ± 1936 | 1827 ± 2179 | 0.754 | |
| TNF-α (pgmL) | N/A | N/A | N/A | 1.09 ± 0.35 | 1.14 ± 0.39 | 1.04 ± 0.31 | 0.308 | |
| IL-6 (pgmL) | N/A | N/A | N/A | 1.92 ± 2.15 | 1.69 ± 1.14 | 2.15 ± 2.84 | 0.489 | |
| MUFA (%) | N/A | N/A | N/A | 22.33 ± 3.16 | 22.98 ± 3.16 | 21.69 ± 3.08 | 0.157 | |
| PUFA (%) | N/A | N/A | N/A | 47.14 ± 4.15 | 46.89 ± 4.00 | 47.39 ± 4.37 | 0.682 | |
| mMDS FFQ Derived | |||||||
|---|---|---|---|---|---|---|---|
| mMDS Questionnaire | Agree (Low-Low) | Agree (High-High) | Disagree (Low-High) | Disagree (High-Low) | r | k (95%CI) | ICC |
| Overall (parent trial baseline) | 183 (43%) | 192 (45%) | 27 (6%) | 24 (6%) | 0.76 (p < 0.001) | 0.76 (95% CI: 0.70, 0.82) | 0.76 (95% CI: 0.72, 0.80) |
| Pilot study baseline | 15 (31%) | 15 (31%) | 8 (17%) | 10 (21%) | 0.25 (p = 0.08) | 0.25 (95% CI: −0.02, 0.52) | 0.11 (95% CI: −0.21, 0.41) |
| Pilot study 6 m follow-up | 15 (37%) | 19 (46%) | 4 (10%) | 3 (7%) | 0.66 (p < 0.001) | 0.66 (95% CI: 0.42, 0.89) | 0.65 (95% CI: 0.44, 0.79) |
| Variable | Control Active Intervention | Intervention Self Sustained-Continuation Phase | p ^ | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 6-Months Follow-Up | Changes | p # | Baseline | 6-Months Follow-Up | Changes | p # | ||||||||||||||
| N | Mean | SD | N | Mean | SD | N | Mean | SD | N | Mean | SD | N | Mean | SD | N | Mean | SD | ||||
| TNF-α (pgmL) | 24 | 1.14 | 0.39 | 20 | 1.22 | 0.44 | 20 | 0.053 | 0.228 | 0.315 | 24 | 1.04 | 0.31 | 21 | 1.21 | 0.35 | 21 | 0.181 | 0.289 | 0.009 | 0.123 |
| IL6 (pgmL) | 22 | 1.69 | 1.14 | 20 | 1.88 | 2.48 | 18 | 0.209 | 2.668 | 0.744 | 22 | 2.15 | 2.84 | 21 | 2.51 | 4.29 | 20 | 0.363 | 5.279 | 0.762 | 0.909 |
| CRP (ngmL) | 24 | 1640 | 1936 | 20 | 1084 | 1232 | 20 | −619 | 1656 | 0.111 | 24 | 1827 | 2179 | 21 | 1584 | 1783 | 21 | −19 | 2185 | 0.969 | 0.330 |
| Tyrosol (ppm) | 18 | 0.019 | 0.026 | 14 | 0.024 | 0.015 | 9 | 0.013 | 0.019 | 0.072 | 19 | 0.020 | 0.033 | 16 | 0.016 | 0.006 | 13 | 0.002 | 0.014 | 0.569 | 0.149 |
| Hydroxytyrosol (ppm) | 23 | 0.105 | 0.094 | 17 | 0.090 | 0.082 | 16 | −0.018 | 0.082 | 0.400 | 24 | 0.137 | 0.105 | 17 | 0.095 | 0.073 | 17 | −0.033 | 0.120 | 0.275 | 0.681 |
| SFA (%) | 24 | 29.01 | 1.42 | 20 | 27.64 | 1.46 | 20 | −1.347 | 1.679 | 0.002 | 24 | 29.74 | 1.66 | 21 | 28.49 | 1.80 | 21 | −1.118 | 1.897 | 0.014 | 0.686 |
| Oleic Acid (%) | 24 | 19.45 | 3.06 | 20 | 19.64 | 2.08 | 20 | −0.042 | 2.897 | 0.949 | 24 | 18.02 | 2.83 | 21 | 19.06 | 2.81 | 21 | 1.052 | 1.766 | 0.013 | 0.157 |
| Alpha-linolenic Acid (%) | 24 | 31.36 | 3.37 | 20 | 32.69 | 3.33 | 20 | 1.461 | 3.682 | 0.092 | 24 | 31.60 | 3.83 | 21 | 31.10 | 3.88 | 21 | −0.756 | 3.917 | 0.387 | 0.070 |
| Linoleic Acid (%) | 24 | 0.63 | 0.23 | 20 | 0.68 | 0.26 | 20 | 0.023 | 0.219 | 0.645 | 24 | 0.64 | 0.16 | 21 | 0.67 | 0.17 | 21 | 0.004 | 0.210 | 0.938 | 0.775 |
| Omega 3 fatty acid (%) | 24 | 3.35 | 0.91 | 20 | 3.54 | 0.96 | 20 | 0.056 | 0.553 | 0.654 | 24 | 3.91 | 1.25 | 21 | 3.82 | 1.08 | 21 | −0.082 | 0.978 | 0.704 | 0.579 |
| mMDS (0–51 points) | 24 | 26.00 | 5.00 | 22 | 26.93 | 4.74 | 22 | 1.063 | 4.613 | 0.292 | 24 | 24.04 | 6.44 | 22 | 25.05 | 5.47 | 22 | 1.231 | 5.140 | 0.274 | 0.909 |
| Baseline (n = 48) | 6 Months Follow-Up (n = 41) | |||||||
|---|---|---|---|---|---|---|---|---|
| β | SE | p | R2 | β | SE | p | R2 | |
| Olive oil with | ||||||||
| CRP (ngmL) | −582.06 | 402.82 | 0.157 | 0.10 | 676.12 | 365.72 | 0.077 | 0.13 |
| TNF-α (pgmL) | −0.257 | 0.066 | <0.001 | 0.31 | −0.012 | 0.114 | 0.919 | 0.002 |
| IL-6 (pgmL) | −0.156 | 0.543 | 0.776 | 0.03 | 0.653 | 0.611 | 0.296 | 0.069 |
| MUFA (%) | −0.518 | 0.623 | 0.412 | 0.08 | 0.123 | 0.648 | 0.852 | 0.004 |
| Oleic acid (%) | −0.437 | 0.586 | 0.460 | 0.08 | 0.124 | 0.545 | 0.822 | 0.009 |
| Omega 3 (%) | 0.663 | 0.218 | 0.004 | 0.24 | 0.491 | 0.272 | 0.083 | 0.120 |
| Omega 6 (%) | −0.162 | 0.850 | 0.850 | 0.00 | −0.396 | 0.918 | 0.670 | 0.026 |
| Omega 9 (%) | −0.556 | 0.635 | 0.387 | 0.06 | 0.090 | 0.650 | 0.891 | 0.002 |
| Hydroxytyrosol (ppm) | 0.038 | 0.019 | 0.058 | 0.11 | 0.005 | 0.020 | 0.790 | 0.014 |
| Tyrosol (ppm) | 0.003 | 0.007 | 0.721 | 0.01 | −0.007 | 0.004 | 0.081 | 0.221 |
| Olive oil as oil most frequently used with | ||||||||
| CRP (ngmL) | −504.39 | 660.75 | 0.450 | 0.06 | 131.02 | 582.42 | 0.824 | 0.003 |
| TNF-α (pgmL) | −0.13320 | 0.12563 | 0.296 | 0.048 | −0.37219 | 0.15281 | 0.023 | 0.199 |
| IL-6 (pgmL) | 0.61535 | 0.83815 | 0.468 | 0.039 | 0.70396 | 0.92189 | 0.453 | 0.048 |
| MUFA (%) | 0.131 | 1.011 | 0.898 | 0.06 | 0.696 | 0.957 | 0.475 | 0.024 |
| Oleic acid (%) | 0.036 | 0.948 | 0.970 | 0.06 | 0.463 | 0.808 | 0.572 | 0.020 |
| Omega 3 (%) | 0.89628 | 0.36287 | 0.019 | 0.183 | 0.20528 | 0.42999 | 0.637 | 0.010 |
| Omega 6 (%) | −1.33274 | 1.34777 | 0.330 | 0.027 | −0.42694 | 1.37174 | 0.758 | 0.022 |
| Omega 9 (%) | 0.10684 | 1.03085 | 0.918 | 0.047 | 0.56453 | 0.96316 | 0.563 | 0.016 |
| Hydroxytyrosol (ppm) | 0.02982 | 0.03239 | 0.364 | 0.031 | −0.05012 | 0.02876 | 0.097 | 0.141 |
| Tyrosol (ppm) | −0.01744 | 0.01281 | 0.185 | 0.067 | −0.00006872 | 0.00715 | 0.992 | 0.063 |
| Fast Food with | ||||||||
| TNF-α (pgmL) | 0.02919 | 0.05935 | 0.626 | 0.024 | 0.11427 | 0.08914 | 0.212 | 0.066 |
| IL-6 (pgmL) | −0.16980 | 0.38495 | 0.662 | 0.028 | −0.03013 | 0.50372 | 0.953 | 0.025 |
| SFA (%) | 0.25249 | 0.23367 | 0.287 | 0.124 | −0.40098 | 0.38530 | 0.308 | 0.076 |
| Trans fat (%) | 0.02804 | 0.02014 | 0.173 | 0.069 | −0.07291 | 0.11761 | 0.541 | 0.107 |
| Red and processed meats with | ||||||||
| TNF-α (pgmL) | −0.01099 | 0.03673 | 0.766 | 0.020 | 0.06130 | 0.03965 | 0.135 | 0.092 |
| IL-6 (pgmL) | 0.10635 | 0.23932 | 0.660 | 0.028 | −0.05615 | 0.22705 | 0.807 | 0.027 |
| SFA (%) | 0.16769 | 0.14391 | 0.252 | 0.129 | −0.04400 | 0.17753 | 0.806 | 0.036 |
| Omega 3 (%) | −0.22092 | 0.10696 | 0.046 | 0.145 | −0.17799 | 0.09880 | 0.084 | 0.119 |
| Omega 6 (%) | 0.17853 | 0.39255 | 0.652 | 0.006 | 0.15885 | 0.33333 | 0.638 | 0.027 |
| Nuts with | ||||||||
| TNF-α (pgmL) | 0.00314 | 0.05098 | 0.951 | 0.018 | 0.05098 | 0.05688 | 0.379 | 0.034 |
| IL-6 (pgmL) | −0.41093 | 0.31558 | 0.202 | 0.072 | −0.13178 | 0.31502 | 0.679 | 0.031 |
| Omega 3 (%) | 0.16628 | 0.15453 | 0.289 | 0.071 | 0.03149 | 0.14626 | 0.831 | 0.002 |
| Omega 6 (%) | −0.15244 | 0.54522 | 0.781 | 0.002 | 0.76669 | 0.43868 | 0.093 | 0.129 |
| Linoleic acid (%) | 0.02443 | 0.49517 | 0.961 | 0.004 | 0.97259 | 0.49793 | 0.063 | 0.172 |
| n-6 Linolenic acid (%) | −0.03366 | 0.02793 | 0.236 | 0.041 | −0.01286 | 0.03494 | 0.716 | 0.006 |
| Fish with | ||||||||
| TNF-α (pgmL) | 0.02446 | 0.04830 | 0.616 | 0.025 | −0.07476 | 0.07311 | 0.317 | 0.043 |
| IL-6 (pgmL) | −0.70823 | 0.29396 | 0.022 | 0.172 | −0.00409 | 0.40835 | 0.992 | 0.024 |
| Omega 3 (%) | 0.27259 | 0.14209 | 0.063 | 0.132 | 0.17512 | 0.18567 | 0.355 | 0.036 |
| Omega 6 | −0.20296 | 0.51794 | 0.698 | 0.004 | 1.01657 | 0.56466 | 0.084 | 0.135 |
| Alcoholic beverages with | ||||||||
| TNF-α (pgmL) | 0.03047 | 0.15146 | 0.842 | 0.019 | −0.09094 | 0.17645 | 0.611 | 0.012 |
| IL-6 (pgmL) | −0.99832 | 0.98883 | 0.320 | 0.053 | 0.03948 | 0.97002 | 0.968 | 0.024 |
| Hydroxytyrosol (ppm) | −0.02219 | 0.03874 | 0.571 | 0.017 | −0.08268 | 0.02863 | 0.009 | 0.302 |
| Tyrosol (ppm) | 0.00420 | 0.01449 | 0.774 | 0.004 | −0.00624 | 0.00872 | 0.484 | 0.090 |
| Baseline Corresponding Plasma Biomarker | 6-Months Follow up Corresponding Plasma Biomarker | |||||||
|---|---|---|---|---|---|---|---|---|
| Control | Intervention | Control Intervention | Intervention Self-Sustained Phase | |||||
| Nutrients (from FFQ) | p-Value | p-Value | p-Value | p-Value | ||||
| SFA | 0.137 | 0.524 | 0.178 | 0.406 | −0.038 | 0.874 | 0.295 | 0.194 |
| Lauric fatty acid | −0.094 | 0.662 | 0.227 | 0.286 | −0.191 | 0.420 | −0.054 | 0.818 |
| Myristic fatty acid | −0.123 | 0.566 | 0.166 | 0.439 | −0.315 | 0.177 | 0.184 | 0.425 |
| Palmitic fatty acid | −0.096 | 0.654 | 0.133 | 0.537 | 0.177 | 0.455 | 0.570 | 0.007 |
| Stearic fatty acid | 0.020 | 0.925 | −0.072 | 0.738 | 0.387 | 0.092 | −0.128 | 0.581 |
| Palmitoleic acid | −0.039 | 0.857 | 0.018 | 0.935 | −0.614 | 0.004 | 0.226 | 0.324 |
| MUFA | 0.079 | 0.715 | 0.152 | 0.477 | −0.295 | 0.206 | 0.262 | 0.251 |
| Oleic acid | −0.165 | 0.441 | −0.357 | 0.087 | 0.062 | 0.795 | 0.021 | 0.928 |
| PUFA | −0.260 | 0.220 | −0.059 | 0.785 | 0.134 | 0.573 | −0.316 | 0.163 |
| Linoleic acid | −0.191 | 0.373 | 0.210 | 0.324 | 0.127 | 0.593 | −0.090 | 0.699 |
| Alfa-Linolenic acid | 0.217 | 0.307 | 0.302 | 0.152 | 0.073 | 0.760 | −0.083 | 0.722 |
| Omega-3 fatty acids | 0.624 | 0.001 | 0.381 | 0.066 | 0.741 | <0.001 | 0.396 | 0.075 |
| Eicosapentaenoic fatty acid (EPA) | 0.466 | 0.022 | 0.441 | 0.031 | 0.688 | <0.001 | 0.621 | 0.003 |
| Docosahexahenoico (DHA) | 0.673 | <0.001 | 0.347 | 0.097 | 0.775 | <0.001 | 0.292 | 0.198 |
| Total Trans fatty acid | 0.080 | 0.711 | −0.033 | 0.878 | −0.081 | 0.733 | −0.059 | 0.800 |
| Conjugated linoleic acid | −0.148 | 0.490 | 0.122 | 0.570 | −0.066 | 0.783 | 0.726 | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sotos-Prieto, M.; Christophi, C.; Black, A.; Furtado, J.D.; Song, Y.; Magiatis, P.; Papakonstantinou, A.; Melliou, E.; Moffatt, S.; Kales, S.N. Assessing Validity of Self-Reported Dietary Intake within a Mediterranean Diet Cluster Randomized Controlled Trial among US Firefighters. Nutrients 2019, 11, 2250. https://doi.org/10.3390/nu11092250
Sotos-Prieto M, Christophi C, Black A, Furtado JD, Song Y, Magiatis P, Papakonstantinou A, Melliou E, Moffatt S, Kales SN. Assessing Validity of Self-Reported Dietary Intake within a Mediterranean Diet Cluster Randomized Controlled Trial among US Firefighters. Nutrients. 2019; 11(9):2250. https://doi.org/10.3390/nu11092250
Chicago/Turabian StyleSotos-Prieto, Mercedes, Costas Christophi, Alicen Black, Jeremy D Furtado, Yiqing Song, Prokopios Magiatis, Aikaterini Papakonstantinou, Eleni Melliou, Steven Moffatt, and Stefanos N. Kales. 2019. "Assessing Validity of Self-Reported Dietary Intake within a Mediterranean Diet Cluster Randomized Controlled Trial among US Firefighters" Nutrients 11, no. 9: 2250. https://doi.org/10.3390/nu11092250
APA StyleSotos-Prieto, M., Christophi, C., Black, A., Furtado, J. D., Song, Y., Magiatis, P., Papakonstantinou, A., Melliou, E., Moffatt, S., & Kales, S. N. (2019). Assessing Validity of Self-Reported Dietary Intake within a Mediterranean Diet Cluster Randomized Controlled Trial among US Firefighters. Nutrients, 11(9), 2250. https://doi.org/10.3390/nu11092250