Tracking of Dietary Intake and Diet Quality from Late Pregnancy to the Postpartum Period

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
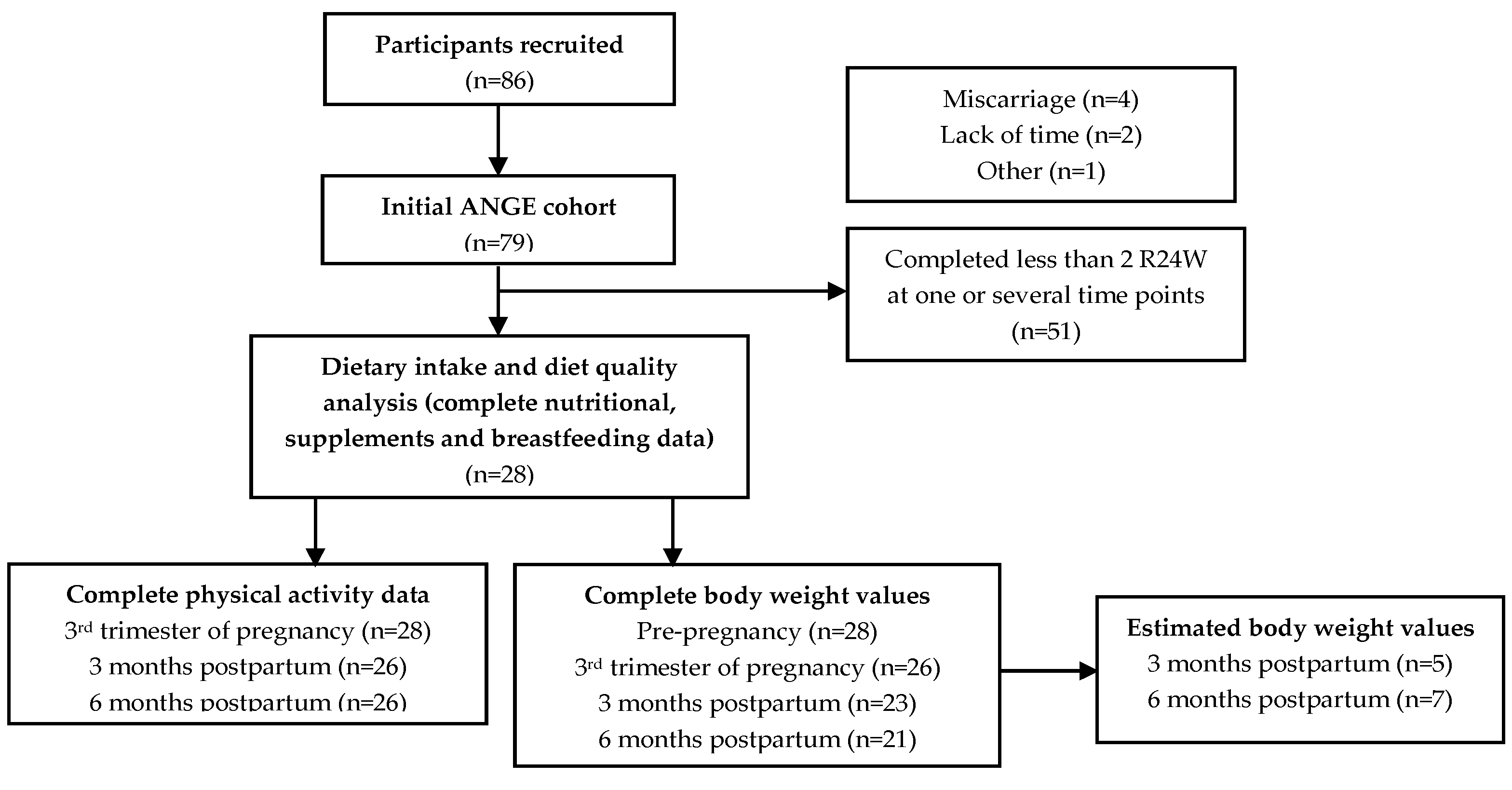
2.1. Study Population
2.2. The Automated Web-Based 24 h Recall (R24W)
2.3. Healthy Eating Index
2.4. Supplement Use
2.5. Other Web Questionnaires
2.6. Estimated Energy and Protein Requirements
2.7. Statistical Analyses
3. Results
3.1. Energy and Macronutrients
3.2. Vitamins and Minerals
3.3. Diet Quality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kaiser, L.; Allen, L.H. Position of the American Dietetic Association: Nutrition and lifestyle for a healthy pregnancy outcome. J. Am. Diet. Assoc. 2008, 108, 553–561. [Google Scholar] [PubMed]
- Symonds, M.E.R. Maternal-Fetal Nutrition during Pregnancy and Lactation; Cambridge University Press: Cambridge, UK, 2010. [Google Scholar]
- Rolfes, S.R.; Pinna, K.; Whitney, E. Understanding Normal and Clinical Nutrition; Wadsworth Publishing Company, Inc.: Belmont, CA, USA, 2002. [Google Scholar]
- Boghossian, N.S.; Yeung, E.H.; Lipsky, L.M.; Poon, A.K.; Albert, P.S. Dietary patterns in association with postpartum weight retention. Am. J. Clin. Nutr. 2013, 97, 1338–1345. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Graubard, B.I.; Williamson, D.F.; Gail, M.H. Cause-specific excess deaths associated with underweight, overweight, and obesity. JAMA 2007, 298, 2028–2037. [Google Scholar] [CrossRef] [PubMed]
- Rong, K.; Yu, K.; Han, X.; Szeto, I.M.; Qin, X.; Wang, J.; Ning, Y.; Wang, P.; Ma, D. Pre-pregnancy BMI, gestational weight gain and postpartum weight retention: A meta-analysis of observational studies. Public Health Nutr. 2015, 18, 2172–2182. [Google Scholar] [CrossRef] [PubMed]
- Tahir, M.J.; Haapala, J.L.; Foster, L.P.; Duncan, K.M.; Teague, A.M.; Kharbanda, E.O.; McGovern, P.M.; Whitaker, K.M.; Rasmussen, K.M.; Fields, D.A.; et al. Higher Maternal Diet Quality during Pregnancy and Lactation Is Associated with Lower Infant Weight-For-Length, Body Fat Percent, and Fat Mass in Early Postnatal Life. Nutrients 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Wennberg, A.L.; Isaksson, U.; Sandstrom, H.; Lundqvist, A.; Hornell, A.; Hamberg, K. Swedish women’s food habits during pregnancy up to six months post-partum: A longitudinal study. Sex. Reprod. Healthc. 2016, 8, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Olson, C.M. Tracking of food choices across the transition to motherhood. J. Nutr. Educ. Behav. 2005, 37, 129–136. [Google Scholar] [CrossRef]
- George, G.C.; Hanss-Nuss, H.; Milani, T.J.; Freeland-Graves, J.H. Food choices of low-income women during pregnancy and postpartum. J. Am. Diet. Assoc. 2005, 105, 899–907. [Google Scholar] [CrossRef]
- Wiltheiss, G.A.; Lovelady, C.A.; West, D.G.; Brouwer, R.J.; Krause, K.M.; Ostbye, T. Diet quality and weight change among overweight and obese postpartum women enrolled in a behavioral intervention program. J. Acad. Nutr. Diet. 2013, 113, 54–62. [Google Scholar] [CrossRef]
- George, G.C.; Milani, T.J.; Hanss-Nuss, H.; Freeland-Graves, J.H. Compliance with dietary guidelines and relationship to psychosocial factors in low-income women in late postpartum. J. Am. Diet. Assoc. 2005, 105, 916–926. [Google Scholar] [CrossRef]
- Savard, C.; Lemieux, S.; Carbonneau, E.; Provencher, V.; Gagnon, C.; Robitaille, J.; Morisset, A.S. Trimester-Specific Assessment of Diet Quality in a Sample of Canadian Pregnant Women. Int. J. Environ. Res. Public Health 2019, 16. [Google Scholar] [CrossRef] [PubMed]
- Savard, C.; Lemieux, S.; Weisnagel, S.J.; Fontaine-Bisson, B.; Gagnon, C.; Robitaille, J.; Morisset, A.S. Trimester-Specific Dietary Intakes in a Sample of French-Canadian Pregnant Women in Comparison with National Nutritional Guidelines. Nutrients 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Jacques, S.; Lemieux, S.; Lamarche, B.; Laramee, C.; Corneau, L.; Lapointe, A.; Tessier-Grenier, M.; Robitaille, J. Development of a Web-Based 24-h Dietary Recall for a French-Canadian Population. Nutrients 2016, 8. [Google Scholar] [CrossRef] [PubMed]
- Lafreniere, J.; Laramee, C.; Robitaille, J.; Lamarche, B.; Lemieux, S. Assessing the relative validity of a new, web-based, self-administered 24 h dietary recall in a French-Canadian population. Public Health Nutr. 2018, 21, 2744–2752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savard, C.; Lemieux, S.; Lafreniere, J.; Laramee, C.; Robitaille, J.; Morisset, A.S. Validation of a self-administered web-based 24-hour dietary recall among pregnant women. BMC Pregnancy Childbirth 2018, 18, 112. [Google Scholar] [CrossRef] [PubMed]
- Garriguet, D. Diet quality in Canada. Health Rep. 2009, 20, 41–52. [Google Scholar] [PubMed]
- Kennedy, E.T.; Ohls, J.; Carlson, S.; Fleming, K. The Healthy Eating Index: Design and applications. J. Am. Diet. Assoc. 1995, 95, 1103–1108. [Google Scholar] [CrossRef]
- Moran, L.J.; Sui, Z.; Cramp, C.S.; Dodd, J.M. A decrease in diet quality occurs during pregnancy in overweight and obese women which is maintained post-partum. Int. J. Obes. (Lond.) 2013, 37, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.; Bianchi, L.; Chung, H.; Weatherspoon, L.; Song, W.O. Is gestational weight gain associated with diet quality during pregnancy? Matern. Child Health J. 2014, 18, 1433–1443. [Google Scholar] [CrossRef] [PubMed]
- Tsigga, M.; Filis, V.; Hatzopoulou, K.; Kotzamanidis, C.; Grammatikopoulou, M.G. Healthy Eating Index during pregnancy according to pre-gravid and gravid weight status. Public Health Nutr. 2011, 14, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Eating Well with Canada’s Food Guide; Health Canada: Ottawa, ON, Canada, 2007.
- Health Canada. Licensed Natural Health Product Database. Available online: https://health-products.canada.ca/lnhpd-bdpsnh/index-eng.jsp (accessed on 1 May 2019).
- Chandonnet, N.; Saey, D.; Almeras, N.; Marc, I. French Pregnancy Physical Activity Questionnaire compared with an accelerometer cut point to classify physical activity among pregnant obese women. PLoS ONE 2012, 7, e38818. [Google Scholar] [CrossRef] [PubMed]
- Chasan-Taber, L.; Schmidt, M.D.; Roberts, D.E.; Hosmer, D.; Markenson, G.; Freedson, P.S. Development and validation of a Pregnancy Physical Activity Questionnaire. Med. Sci. Sports Exerc. 2004, 36, 1750–1760. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Otten, J.J.; Hellwig, J.P.; Meyers, L.D. (Eds.) Dietary Reference Intakes: The Essential Guide to Nutrient Requirements; National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Institute of Medicine (US) Subcommittee on Interpretation and Uses of Dietary Reference Intakes; Institute of Medicine (US) Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. Application of DRIs for Group Diet Assessment. In DRI Dietary Reference Intakes: Applications in Dietary Assessment; National Academies Press: Washington, DC, USA, 2000. [Google Scholar]
- Talai Rad, N.; Ritterath, C.; Siegmund, T.; Wascher, C.; Siebert, G.; Henrich, W.; Buhling, K.J. Longitudinal analysis of changes in energy intake and macronutrient composition during pregnancy and 6 weeks post-partum. Arch. Gynecol. Obstet. 2011, 283, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Derbyshire, E.; Davies, G.J.; Costarelli, V.; Dettmar, P.W. Habitual micronutrient intake during and after pregnancy in Caucasian Londoners. Matern. Child Nutr. 2009, 5, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Horan, M.K.; McGowan, C.A.; Gibney, E.R.; Byrne, J.; Donnelly, J.M.; McAuliffe, F.M. Maternal Nutrition and Glycaemic Index during Pregnancy Impacts on Offspring Adiposity at 6 Months of Age—Analysis from the ROLO Randomised Controlled Trial. Nutrients 2016, 8. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, K.L.; Heneghan, C.; McNulty, B.; Brennan, L.; McAuliffe, F.M. Lifestyle and dietary habits of an obese pregnant cohort. Matern. Child Health J. 2015, 19, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Moran, L.J.; McNaughton, S.A.; Sui, Z.; Cramp, C.; Deussen, A.R.; Grivell, R.M.; Dodd, J.M. The characterisation of overweight and obese women who are under reporting energy intake during pregnancy. BMC Pregnancy Childbirth 2018, 18, 204. [Google Scholar] [CrossRef] [PubMed]
- Brassard, D.; Laramee, C.; Corneau, L.; Begin, C.; Belanger, M.; Bouchard, L.; Couillard, C.; Desroches, S.; Houle, J.; Langlois, M.F.; et al. Poor Adherence to Dietary Guidelines among French-Speaking Adults in the Province of Quebec, Canada: The PREDISE Study. Can. J. Cardiol. 2018, 34, 1665–1673. [Google Scholar] [CrossRef]
- Wilson, R.D.; Wilson, R.D.; Audibert, F.; Brock, J.A.; Carroll, J.; Cartier, L.; Gagnon, A.; Johnson, J.A.; Langlois, S.; Murphy-Kaulbeck, L.; et al. Pre-Conception Folic Acid and Multivitamin Supplementation for the Primary and Secondary Prevention of Neural Tube Defects and Other Folic Acid-Sensitive Congenital Anomalies. J. Obstet. Gynaecol. Can. 2015, 37, 534–552. [Google Scholar] [CrossRef]
- Bassett-Gunter, R.L.; Levy-Milne, R.; Naylor, P.J.; Symons Downs, D.; Benoit, C.; Warburton, D.E.; Blanchard, C.M.; Rhodes, R.E. Oh baby! Motivation for healthy eating during parenthood transitions: A longitudinal examination with a theory of planned behavior perspective. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 88. [Google Scholar] [CrossRef] [PubMed]
- Hanson, M.A.; Bardsley, A.; De-Regil, L.M.; Moore, S.E.; Oken, E.; Poston, L.; Ma, R.C.; McAuliffe, F.M.; Maleta, K.; Purandare, C.N.; et al. The International Federation of Gynecology and Obstetrics (FIGO) recommendations on adolescent, preconception, and maternal nutrition: “Think Nutrition First”. Int. J. Gynaecol. Obstet. 2015, 131 (Suppl. 4), S213–S253. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Mean ± SD or n (%) |
|---|---|
| Age at study enrollment (years) | 32.7 ± 3.6 |
| Primiparous | 12 (43) |
| Pre-pregnancy BMI (kg/m2) | 24.9 ± 5.1 |
| Normal weight | 18 (64) |
| Overweight | 6 (21) |
| Obese | 4 (14) |
| Weight (kg) | |
| Pre-pregnancy | 69.3 ± 16.6 |
| 3rd trimester of pregnancy (difference with pre-pregnancy) a | 12.8 ± 4.5 |
| 3 months postpartum (difference with pre-pregnancy) b | 4.3 ± 6.3 |
| 6 months postpartum (difference with pre-pregnancy) c | 2.8 ± 5.7 |
| Ethnicity-Caucasian | 28 (100) |
| Education | |
| College | 2 (7) |
| University | 26 (93) |
| Household income | |
| <60,000$ | 4 (14) |
| 60,000–79,999$ | 5 (18) |
| 80,000–99,999$ | 10 (36) |
| >100,000$ | 9 (32) |
| Breastfeeding (exclusively or not) | |
| At 3 months postpartum | 27 (96) |
| At 6 months postpartum | 25 (89) |
| Duration of exclusive breastfeeding postpartum (months) c | 5.2 ± 1.0 |
| 3rd Trimester of Pregnancy | 3 Months Postpartum | 6 Months Postpartum | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | %Below AMDR, EER or UL | %Above AMDR, EER or UL | Mean ± SD | %Below AMDR, EER or UL | %Above AMDR, EER or UL | Mean ± SD | %Below AMDR, EER or UL | %Above AMDR, EER or UL | Overall p-Value b | |
| EER (kcal/day) a | 2497 ± 203 | - | - | 2578 ± 201 | - | - | 2678 ± 327 | - | - | - |
| Energy intake (kcal/day) | 2321 ± 429 | 61 | 39 | 2305 ± 506 | 78 | 22 | 2227 ± 474 | 74 | 26 | 0.48 |
| AMDR protein, E% | 10–35 | - | - | 10–35 | - | - | 10–35 | - | - | - |
| Protein, E% | 17.5 ± 2.8 | 0 | 0 | 17.1 ± 2.8 | 0 | 0 | 16.9 ± 3.2 | 0 | 0 | 0.70 |
| AMDR carbohydrate, E% | 45–65 | - | - | 45–65 | - | - | 45–65 | - | - | - |
| Carbohydrate, E% | 47.0 ± 5.9 | 29 | 0 | 44.8 ± 6.1 | 46 | 0 | 45.3 ± 5.9 | 50 | 0 | 0.08 |
| UL added sugar, E% | 25 | - | - | 25 | - | - | 25 | - | - | - |
| Added sugar, E% | 9.8 ± 3.8 | 100 | 0 | 9.4 ± 4.0 | 96 | 0 | 9.1 ± 3.2 | 100 | 0 | 0.71 |
| AMDR, total fat, E% | 20–35 | - | - | 20–35 | - | - | 20–35 | - | - | - |
| Total fat, E% | 35.5 ± 5.0 | 0 | 57 | 36.6 ± 4.6 | 0 | 64 | 36.3 ± 4.7 | 0 | 64 | 0.57 |
| SFA, E% | 13.6 ± 2.1 | - | - | 12.9 ± 1.6 | - | - | 13.0 ± 2.7 | - | - | 0.32 |
| MUFA% | 12.4 ± 2.2 | - | - | 13.0 ± 2.1 | - | - | 13.0 ± 2.1 | - | - | 0.30 |
| PUFA% | 6.7 ± 2.1 | - | - | 7.8 ± 2.8 | - | - | 7.4 ± 1.8 | - | - | 0.08 |
| 3rd Trimester of Pregnancy | 3 Months Postpartum | 6 Months Postpartum | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | %Below EAR | %Above UL | Mean ± SD | %Below EAR | %Above UL | Mean ± SD | %Below EAR | %Above UL | Overall p-Value a | |
| Vitamin D IU/day | 292 ± 128 | 75 | 0 | 252 ± 116 | 86 | 0 | 236 ± 105 | 93 | 0 | 0.06 |
| Iron, mg/day | 14.8 ± 3.7 | 96 | 0 | 14.9 ± 3.3 | 0 | 0 | 14.0 ± 3.5 | 0 | 0 | 0.09 |
| Folate, µg DFE/day | 518 ± 151 | 57 | - | 519 ± 130 | 36 | - | 474 ± 125 | 43 | - | 0.11 |
| Folic acid, µg/day | 136 ± 75 | - | 0 | 151 ± 67 | - | 0 | 134 ± 66 | - | 0 | 0.28 |
| Vitamin B6, mg/day | 1.8 ± 0.4 | 32 | 0 | 1.8 ± 0.1 | 36 | 0 | 1.7 ± 0.4 | 50 | 0 | 0.13 |
| Magnesium, mg/day | 424 ± 79 | 4 | - | 399 ± 99 | 7 | - | 400 ± 100 | 11 | - | 0.12 |
| Vitamin A, µg RAE/day | 975 ± 371 | 7 | 0 | 817 ± 317 | 68 | 0 | 752 ± 334 | 71 | 0 | 0.005 |
| Zinc, mg/day | 13.8 ± 3.9 | 7 | 0 | 12.2 ± 3.6 | 32 | 0 | 12.4 ± 3.9 | 36 | 0 | 0.06 |
| Calcium, mg/day | 1560 ± 453 | 0 | 0 | 1252 ± 386 | 18 | 0 | 1217 ± 377 | 18 | 0 | 0.002 |
| Vitamin C, mg/day | 148 ± 73 | 11 | 0 | 109 ± 58 | 25 | 0 | 108 ± 53 | 43 | 0 | 0.03 |
| Thiamin, mg/day | 1.8 ± 0.5 | 4 | - | 1.8 ± 0.6 | 7 | - | 1.7 ± 0.5 | 14 | - | 0.01 |
| Vitamin B12, µg/day | 5.8 ± 2.6 | 0 | - | 4.8 ± 1.7 | 7 | - | 4.7 ± 1.7 | 11 | - | 0.09 |
| Riboflavin, mg/day | 2.7 ± 0.7 | 0 | - | 2.4 ± 0.5 | 0 | - | 2.3 ± 0.6 | 7 | - | 0.004 |
| Niacin, mg NE/day | 46.1 ± 9.0 | 0 | - | 47.0 ± 9.4 | 0 | - | 45.9 ± 11.3 | 0 | - | 0.70 |
| Pantothenic acid, mg/day | 6.9 ± 1.6 | - | - | 6.4 ± 1.5 | - | - | 6.4 ± 1.6 | - | - | 0.18 |
| Phosphorus, mg/day | 1768 ± 362 | 0 | 0 | 1614 ± 346 | 0 | 0 | 1549 ± 354 | 0 | 0 | 0.01 |
| Sodium, mg/day | 3303 ± 893 | - | 86 | 3229 ± 921 | - | 86 | 3236 ± 1107 | - | 79 | 0.93 |
| Manganese, mg/day | 4.3 ± 1.3 | - | 0 | 4.1 ± 1.2 | - | 0 | 3.9 ± 1.2 | - | 0 | 0.17 |
| Selenium, µg/day | 136 ± 27 | 0 | 0 | 137 ± 34 | 0 | 0 | 136 ± 49 | 0 | 0 | 0.99 |
| Copper, mg/day | 1.6 ± 0.3 | 0 | 0 | 1.5 ± 0.3 | 4 | 0 | 1.5 ± 0.8 | 4 | 0 | 0.50 |
| n (%) | ||||
|---|---|---|---|---|
| 3rd Trimester of Pregnancy | 3 Months Postpartum | 6 Months Postpartum | Overall p-Value a | |
| ≥1 supplement (all types) | 25 (89) | 19 (68) | 13 (46) | 0.003 |
| Number of supplements (all types) taken during each period | ||||
| 0 | 3 (11) | 9 (32) | 15 (54) | 0.003 |
| 1 | 21 (75) | 14 (50) | 11 (39) | 0.03 |
| ≥2 | 4 (14) | 5 (18) | 2 (7) | 0.69 |
| Types of supplements most commonly taken | ||||
| Multivitamins | 23 (92) | 16 (84) | 12 (92) | 0.01 |
| Folic acid supplement | 2 (8) | 1 (5) | 1 (8) | 0.77 |
| Vitamin D supplement | 2 (8) | 2 (11) | 1 (8) | 0.81 |
| Iron supplement | 1 (4) | 1 (5) | 0 (0) | 0.60 |
| Omega-3 supplement (mostly EPA-DHA) | 1 (4) | 1 (5) | 1 (8) | 1.00 |
| 3rd Trimester of Pregnancy | 3 Months Postpartum | 6 Months Postpartum | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | %Below EAR | %Above UL | Mean ± SD | %Below EAR | %Above UL | Mean ± SD | %Below EAR | %Above UL | Overall p-Value a | |
| Vitamin D IU/day | 841 ± 776 | 11 | 4 | 684 ± 848 | 36 | 4 | 586 ± 846 | 57 | 4 | 0.001 |
| Iron, mg/day | 45.5 ± 32.7 | 18 | 39 | 33.8 ± 18.5 | 0 | 25 | 26.7 ± 15.7 | 0 | 14 | 0.03 |
| Folate, µg DFE/day | 1175 ± 993 | 18 | - | 1608 ± 2039 | 18 | - | 1095 ± 1045 | 21 | - | 0.30 |
| Folic acid, µg/day | 793 ± 999 | - | 46 | 1240 ± 1991 | - | 61 | 755 ± 1023 | - | 46 | 0.29 |
| Vitamin B6, mg/day | 6.1 ± 4.2 | 4 | 0 | 14.1 ± 46.9 | 14 | 4 | 3.8 ± 3.7 | 32 | 0 | 0.01 |
| Magnesium, mg/day | 474 ± 81 | 0 | 0 | 429 ± 106 | 7 | 0 | 420 ± 106 | 11 | 0 | 0.01 |
| Vitamin A, µg RAE/day | 1473 ± 607 | 4 | 0 | 924 ± 356 | 54 | 0 | 838 ± 360 | 54 | 0 | <0.0001 |
| Zinc, mg/day | 23.1 ± 7.3 | 0 | 0 | 19.1 ± 8.6 | 18 | 4 | 17.1 ± 8.1 | 25 | 0 | 0.001 |
| Calcium, mg/day | 1779 ± 471 | 0 | 4 | 1415 ± 387 | 11 | 0 | 1330 ± 433 | 14 | 0 | <0.0001 |
| Vitamin C, mg/day | 229 ± 70 | 4 | 0 | 171 ± 86 | 25 | 0 | 151 ± 78 | 25 | 0 | 0.001 |
| Thiamin, mg/day | 3.5 ± 1.1 | 0 | - | 3.2 ± 1.6 | 0 | - | 2.5 ± 1.2 | 7 | - | 0.001 |
| Vitamin B12, µg/day | 11.2 ± 5.7 | 0 | - | 8.8 ± 6.1 | 4 | - | 7.2 ± 4.6 | 7 | - | 0.002 |
| Riboflavin, mg/day | 4.5 ± 1.5 | 0 | - | 3.8 ± 1.6 | 0 | - | 3.2 ± 1.4 | 4 | - | 0.0002 |
| Niacin, mg NE/day | 61.7 ± 12.2 | 0 | 0 | 58.1 ± 15.2 | 0 | 4 | 53.4 ± 15.8 | 0 | 0 | 0.01 |
| Pantothenic acid, mg/day | 11.6 ± 2.9 | - | - | 9.9 ± 3.4 | - | - | 8.9 ± 3.6 | - | - | 0.001 |
| Phosphorus, mg/day | 1177 ± 349 | 0 | 0 | 1614 ± 346 | 0 | 0 | 1549 ± 354 | 0 | 0 | 0.01 |
| Sodium, mg/day | 3303 ± 893 | - | 86 | 3229 ± 921 | - | 86 | 3236 ± 1107 | - | 79 | 0.93 |
| Manganese, mg/day | 5.4 ± 1.2 | - | 0 | 4.8 ± 1.4 | - | 0 | 4.5 ± 1.1 | - | 0 | 0.002 |
| Selenium, µg/day | 150 ± 31 | 0 | 0 | 148 ± 38 | 0 | 0 | 145 ± 55 | 0 | 0 | 0.91 |
| Copper, mg/day | 2.8 ± 0.9 | 0 | 0 | 2.3 ± 1.1 | 4 | 0 | 2.1 ± 1.1 | 4 | 0 | 0.02 |
| HEI | Score Range | 3rd Trimester | 3 Months Postpartum | 6 Months Postpartum | Overall p-Value a |
|---|---|---|---|---|---|
| Total | 0–100 | 64.1 ± 12.2 | 61.2 ± 11.4 | 60.5 ± 8.3 | 0.13 |
| Adequacy | 0–60 | 46.4 ± 7.6 | 44.5 ± 8.3 | 43.3 ± 7.5 | 0.08 |
| Total vegetables and fruit | 0–10 | 8.2 ± 2.0 | 7.1 ± 2.2 | 6.9 ± 2.4 | 0.04 |
| Whole fruit | 0–5 | 4.4 ± 1.5 | 3.6 ± 1.9 | 3.4 ± 1.7 | 0.09 |
| Dark green and orange vegetables | 0–5 | 3.3 ± 1.6 | 3.4 ± 1.5 | 2.9 ± 1.6 | 0.25 |
| Total grains products | 0–5 | 4.4 ± 0.7 | 4.5 ± 0.8 | 4.2 ± 1.0 | 0.29 |
| Whole grains | 0–5 | 2.6 ± 1.8 | 2.7 ± 1.7 | 2.3 ± 1.9 | 0.62 |
| Milk and alternatives | 0–10 | 9.5 ± 1.4 | 8.8 ± 1.9 | 8.8 ± 2.4 | 0.08 |
| Meat and alternatives | 0–10 | 8.9 ± 1.6 | 8.6 ± 2.0 | 8.5 ± 1.9 | 0.16 |
| Unsaturated fat | 0–10 | 5.2 ± 3.7 | 5.8 ± 3.7 | 6.4 ± 3.3 | 0.29 |
| Moderation | 0–40 | 17.7 ± 7.2 | 16.7 ± 6.7 | 17.2 ± 7.6 | 0.65 |
| Saturated fats | 0–10 | 2.8 ± 2.6 | 3.5 ± 2.4 | 3.7 ± 3.1 | 0.33 |
| Sodium | 0–10 | 4.6 ± 2.8 | 4.8 ± 2.9 | 4.8 ± 3.2 | 0.93 |
| Other foods | 0–20 | 10.3 ± 5.1 | 8.4 ± 5.2 | 8.7 ± 4.8 | 0.16 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lebrun, A.; Plante, A.-S.; Savard, C.; Dugas, C.; Fontaine-Bisson, B.; Lemieux, S.; Robitaille, J.; Morisset, A.-S. Tracking of Dietary Intake and Diet Quality from Late Pregnancy to the Postpartum Period. Nutrients 2019, 11, 2080. https://doi.org/10.3390/nu11092080
Lebrun A, Plante A-S, Savard C, Dugas C, Fontaine-Bisson B, Lemieux S, Robitaille J, Morisset A-S. Tracking of Dietary Intake and Diet Quality from Late Pregnancy to the Postpartum Period. Nutrients. 2019; 11(9):2080. https://doi.org/10.3390/nu11092080
Chicago/Turabian StyleLebrun, Audrée, Anne-Sophie Plante, Claudia Savard, Camille Dugas, Bénédicte Fontaine-Bisson, Simone Lemieux, Julie Robitaille, and Anne-Sophie Morisset. 2019. "Tracking of Dietary Intake and Diet Quality from Late Pregnancy to the Postpartum Period" Nutrients 11, no. 9: 2080. https://doi.org/10.3390/nu11092080
APA StyleLebrun, A., Plante, A.-S., Savard, C., Dugas, C., Fontaine-Bisson, B., Lemieux, S., Robitaille, J., & Morisset, A.-S. (2019). Tracking of Dietary Intake and Diet Quality from Late Pregnancy to the Postpartum Period. Nutrients, 11(9), 2080. https://doi.org/10.3390/nu11092080