Impact of Oral Intake of Glucosylceramide Extracted from Pineapple on Xerostomia: A Double-Blind Randomized Cross-Over Trial

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
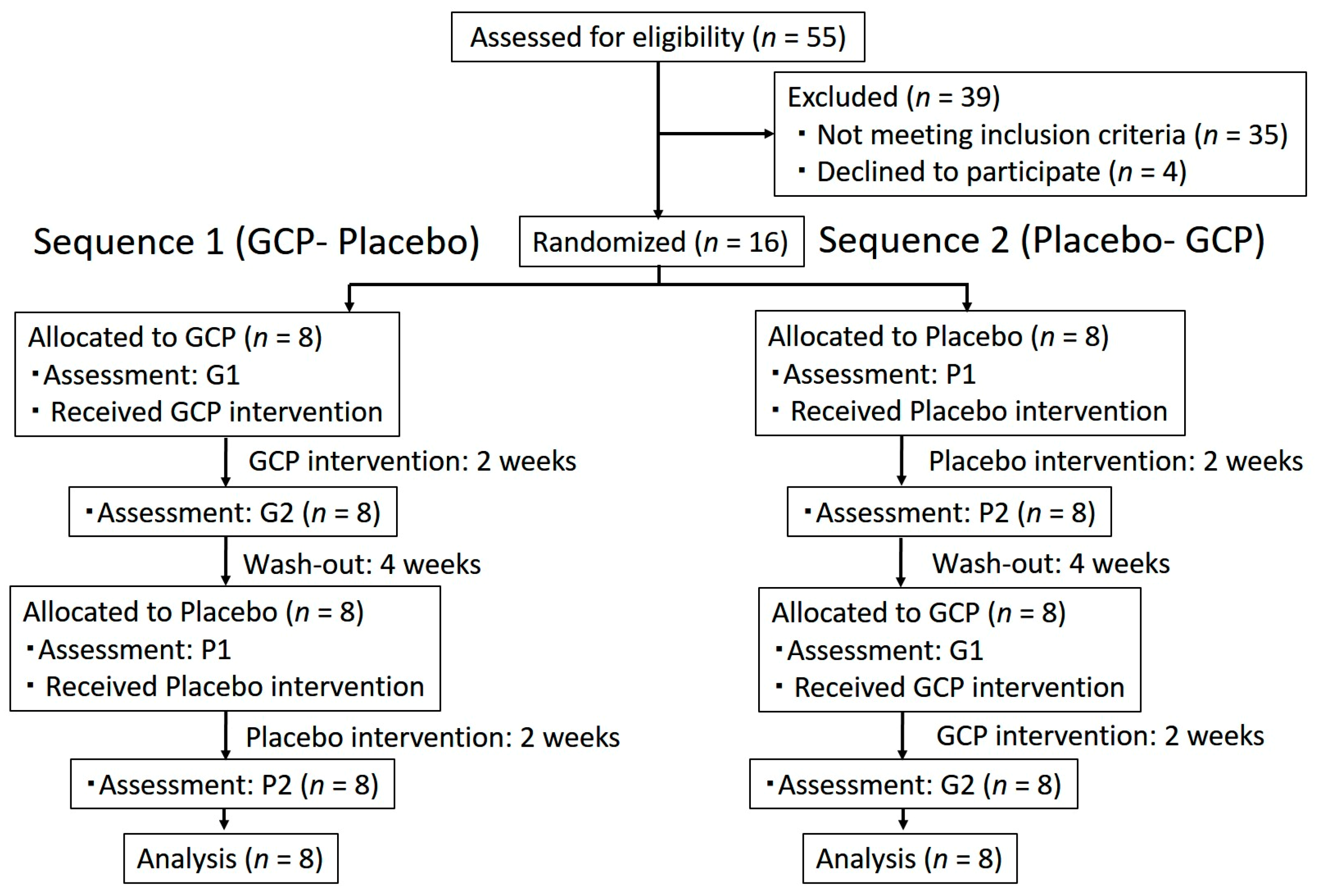
2.1. Study Design
2.2. Participants
2.3. Test Sample
2.4. Assessment
2.5. Oral Moisture Level
2.6. Number of Fungiform Papillae
2.7. Xerostomia Symptoms
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Diaz-Arnold, M.; Marek, C.A. The impact of saliva on patients: A literature review. J. Prosthet. Dent. 2002, 88, 337–343. [Google Scholar] [CrossRef]
- Han, P.; Suarez-Durall, P.; Mulligan, R. Dry mouth: A critical topic for older adult patients. J. Prosthodont. Res. 2015, 59, 6–19. [Google Scholar] [CrossRef] [PubMed]
- Gil-Montoya, J.A.; Guardia-L’opez, I.; Gonz’alez-Moles, M.A. Evaluation of the clinical efficacy of a mouthwash and oral gel containing the antimicrobial proteins lactoperoxidase, lysozyme and lactoferrin in elderly patients with dry mouth—a pilot study. Gerodontology 2008, 25, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Madison, K.C.; Wertz, P.W.; Strauss, J.S.; Downing, D.T. Lipid composition of cultured murine keratinocytes. J. Investig. Dermatol. 1986, 87, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Elias, P.M. Epidermal lipids, barrier function, and desquamation. J. Investig. Dermatol. 1983, 80, 44s–49s. [Google Scholar] [CrossRef] [PubMed]
- Imokawa, G.; Abe, A.; Jin, K.; Higaki, Y.; Kawashima, M.; Hidano, A. Decreased level of ceramides in stratum corneum of atopic dermatitis: An etiologic factor in atopic dry skin? J. Investig. Dermatol. 1991, 96, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Yamamura, T.; Tezuka, T. Change in sphingomyelinase activity in human epidermis during aging. J. Dermatol. Sci. 1990, 1, 79–83. [Google Scholar] [CrossRef]
- Egawa, M.; Tagami, H. Comparison of the depth profiles of water and water-binding substances in the stratum corneum determined in vivo by Raman spectroscopy between the cheek and volar forearm skin: Effects of age, seasonal changes and artificial forced hydration. Br. J. Dermatol. 2008, 158, 251–260. [Google Scholar] [CrossRef]
- Uchiyama, T.; Nakano, Y.; Ueda, O.; Mori, H.; Nakashima, M.; Noda, A.; Ishizaki, C.; Mizoguchi, M. Oral intake of glucosylceramide improves relatively higher level of transepidermal water loss in mice and healthy human subjects. J. Health Sci. 2008, 54, 559–566. [Google Scholar] [CrossRef]
- Sugawara, T.; Kinoshita, M.; Ohnishi, M.; Nagata, J.; Saito, M. Digestion of maize sphingolipids in rats and uptake of sphingadienine by Caco-2 cells. J. Nutr. 2003, 133, 2777–2782. [Google Scholar] [CrossRef]
- Duan, J.; Sugawara, T.; Hirose, M.; Aida, K.; Sakai, S.; Fujii, A.; Hirata, T. Dietary sphingolipids improve skin barrier functions via the upregulation of ceramide synthases in the epidermis. Exp. Dermatol. 2012, 21, 448–452. [Google Scholar] [CrossRef] [PubMed]
- Yoshino, S.; Nojima, J.; Ohto, N.; Kuwahara, H.; Miura, H. Long term intake of glucosylceramide extracted from pineapple -safety evaluation in healthy adults-. Jpn. Pharmacol. Ther. 2016, 44, 247–253. [Google Scholar]
- Yoshino, S.; Nojima, J.; Ohto, N.; Kuwahara, H.; Ito, K. Excessive intake of glucosylceramide extracted from pineapple -safety evaluation in healthy adults-. Jpn. Pharmacol. Ther. 2016, 44, 255–260. [Google Scholar]
- Tsuji, K.; Mitsutake, S.; Ishikawa, J.; Takagi, Y.; Akiyama, M.; Shimizu, H.; Tomiyama, T.; Igarashi, Y. Dietary glucosylceramide improves skin barrier function in hairless mice. J. Dermatol. Sci. 2006, 44, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Yoshino, S.; Iwasaki, D.; Nojima, J.; Ohto, N.; Kuwahara, H.; Nakata, S. Effects of glucosylceramide extracted from pineapple on healthy Japanese males and females with dullness and dry skin: Randomized, double blind, placebo controlled, parallel group study. Jpn. Pharmacol. Ther. 2015, 43, 1593–1600. [Google Scholar]
- Kimori, H.; Yamamoto, K.; Yamachika, S.; Tsurumoto, A.; Kamikawa, Y.; Sasao, M.; Morito, M.; Saito, I.; Ohshima, T.; Maeda, N.; et al. Factors associated with the presence of atrophic tongue in patients with dry mouth. Gerodontology 2015, 32, 13–17. [Google Scholar] [CrossRef] [PubMed]
- G*Power: Universität Düsseldorf. Available online: http://www.gpower.hhu.de (accessed on 7 March 2016).
- Murakami, M.; Nishi, Y.; Kamashita, Y.; Nagaoka, E. Relationship between symptoms of dryness and moisture levels in patients with maxillofacial prostheses. J. Prosthodont. Res. 2010, 54, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, Y.; Yoda, T.; Araki, R.; Sakai, T.; Toya, S.; Ito, K.; Funayama, S.; Enoki, Y.; Sato, T. Evaluation of oral wetness using an improved moisture-checking device for the diagnosis of dry mouth. Oral Sci. Int. 2017, 14, 33–36. [Google Scholar] [CrossRef]
- Negoro, A.; Umemoto, M.; Fukazawa, K.; Terada, T.; Sakagami, M. Observation of tongue papillae by video microscopy and contact endoscopy to investigate their correlation with taste function. Auris Nasus Larynx 2004, 31, 255–259. [Google Scholar] [CrossRef]
- Tanaka, T.; Komai, Y.; Tokuyama, Y.; Yanai, H.; Ohe, S.; Okazaki, K.; Ueno, H. Identification of stem cells that maintain and regenerate lingual keratinized epithelial cells. Nat. Cell Biol. 2013, 15, 511–518. [Google Scholar] [CrossRef]
- Cho, E.P.; Hwang, S.J.; Clovis, J.B.; Lee, T.Y.; Paik, D.I.; Hwang, Y.S. Enhancing the quality of life in elderly women through a programme to improve the condition of salivary hypofunction. Gerodontology 2012, 29, e972–e980. [Google Scholar] [CrossRef] [PubMed]
- Hakuta, C.; Mori, C.; Ueno, M.; Shinada, K.; Kawaguchi, Y. Evaluation of an oral function promotion programme for the independent elderly in Japan. Gerodontology 2009, 26, 250–258. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Sequence 1 (GCP-Placebo) | Sequence 2 (Placebo-GCP) | Total | p Value | |
|---|---|---|---|---|
| Patients; number | 8 | 8 | 16 | |
| Age; mean ± SD | 73.3 ± 9.9 | 75.3 ± 4.6 | 74.3 ± 7.6 | 0.06 # |
| Gender; Men/Women | 1/7 | 4/4 | 5/11 | 0.00 $ |
| No. of remaining teeth (Upper) | 6.3 ± 5.6 | 4.9 ± 4.3 | 5.6 ± 4.9 | 0.59 # |
| No. of remaining teeth (Lower) | 7.1 ± 4.8 | 6.7 ± 5.5 | 6.9 ± 5.0 | 0.89 # |
| Use of removable prostheses: None/Upper or lower/Upper and lower | 1/2/5 | 1/1/6 | 2/3/11 | 0.81 $ |
| Number of underlying diseases: None/One/More than two | 2/ 3/ 3 | 1/6/1 | 3/9/4 | 0.31 $ |
| Number of medications: None/One/More than two | 2/1/5 | 1/3/4 | 3/4/9 | 0.48 $ |
| Baseline oral moisture level: median (range) | G1: 31.55 (7.3) | P1: 31.55 (2.7) | 31.55 (7.3) | 0.48 % |
| Period | Median | Min | Max | 25% Tile | 75% Tile | 95% CI | p Value | |
|---|---|---|---|---|---|---|---|---|
| Sequence 1 | G1 | 31.55 | 26.00 | 33.30 | 28.65 | 32.55 | 28.63–32.82 | #p = 0.26 a |
| (GCP-Placebo) | G2 | 32.20 | 29.00 | 33.10 | 31.33 | 32.98 | 30.75–33.02 | |
| P1 | 32.15 | 30.30 | 33.50 | 31.38 | 32.93 | 31.24–32.94 | ||
| P2 | 32.60 | 30.50 | 33.90 | 31.38 | 33.70 | 31.47–33.56 | ||
| Sequence 2 | P1 | 31.55 | 30.40 | 33.10 | 31.03 | 32.58 | 30.94–32.51 | #p = 0.48 b |
| (Placebo-GCP) | P2 | 31.80 | 31.20 | 33.40 | 31.25 | 33.05 | 31.35–32.85 | |
| G1 | 31.70 | 30.70 | 33.20 | 31.13 | 32.25 | 31.12–32.43 | ||
| G2 | 32.40 | 28.80 | 33.40 | 31.20 | 33.18 | 30.68–33.24 | ||
| GCP | G1 | 31.70 | 26.00 | 33.30 | 30.78 | 32.38 | 30.23–32.25 | #p = 0.03 c |
| G2 | 32.35 | 28.80 | 33.40 | 31.23 | 33.08 | 31.18–32.67 | ||
| Placebo | P1 | 31.90 | 30.30 | 33.50 | 31.35 | 32.60 | 31.46–32.41 | #p = 0.12 d |
| P2 | 32.45 | 28.80 | 33.90 | 31.20 | 33.35 | 31.50–32.97 |
| Period | Median | Min | Max | 25% Tile | 75% Tile | 95% CI | p Value | |
|---|---|---|---|---|---|---|---|---|
| Sequence 1 | G1 | 8.5 | 6.0 | 14.0 | 7.3 | 10.5 | 6.9–11.1 | #p = 0.32 a |
| (GCP-Placebo) | G2 | 8.0 | 6.0 | 14.0 | 7.3 | 10.5 | 6.8–11.0 | |
| P1 | 8.0 | 6.0 | 15.0 | 6.5 | 9.8 | 6.4–11.1 | ||
| P2 | 8.0 | 6.0 | 15.0 | 7.3 | 9.8 | 6.6–11.2 | ||
| Sequence 2 | P1 | 12.5 | 5.0 | 25.0 | 8.3 | 14.5 | 7.5–17.5 | #p = 0.32 b |
| (Placebo-GCP) | P2 | 11.5 | 6.0 | 25.0 | 8.3 | 14.3 | 7.4–17.1 | |
| G1 | 12.0 | 5.0 | 25.0 | 8.3 | 14.5 | 7.4–17.4 | ||
| G2 | 12.5 | 4.0 | 26.0 | 8.3 | 14.8 | 7.2–18.1 | ||
| GCP | G1 | 9.0 | 5.0 | 25.0 | 8.0 | 12.8 | 8.1–13.2 | #p = 0.66 c |
| G2 | 9.0 | 4.0 | 26.0 | 8.0 | 13.8 | 8.0–13.5 | ||
| Placebo | P1 | 9.0 | 5.0 | 25.0 | 8.0 | 13.0 | 8.0–13.3 | #p = 0.71 d |
| P2 | 9.0 | 6.0 | 25.0 | 8.0 | 12.0 | 8.0–13.1 |
| Period | Median | Min | Max | 25% Tile | 75% Tile | 95% CI | p Value | |
|---|---|---|---|---|---|---|---|---|
| Sequence 1 | G1 | 42.86 | 9.54 | 78.99 | 12.55 | 61.54 | 18.82–62.03 | #p = 0.09 a |
| (GCP-Placebo) | G2 | 43.05 | 22.20 | 73.18 | 24.45 | 70.68 | 27.42–65.91 | |
| P1 | 54.67 | 3.43 | 87.57 | 46.04 | 71.13 | 33.38–74.64 | ||
| P2 | 60.31 | 8.44 | 86.99 | 24.05 | 74.96 | 27.75–74.64 | ||
| Sequence 2 | P1 | 52.99 | 8.48 | 88.95 | 35.06 | 62.29 | 30.57–69.92 | #p = 1.00 b |
| (Placebo-GCP) | P2 | 44.71 | 33.51 | 94.62 | 36.57 | 59.60 | 33.99–67.43 | |
| G1 | 50.45 | 19.28 | 90.94 | 29.89 | 62.96 | 30.56–69.41 | ||
| G2 | 49.81 | 34.38 | 92.26 | 37.97 | 68.66 | 37.46–70.50 | ||
| GCP | G1 | 46.02 | 9.54 | 90.94 | 22.23 | 62.91 | 32.29–58.13 | #p = 0.04 c |
| G2 | 49.81 | 22.20 | 92.26 | 30.23 | 70.68 | 39.10–61.55 | ||
| Placebo | P1 | 54.05 | 3.43 | 88.95 | 44.63 | 63.42 | 39.67–64.58 | #p = 0.96 d |
| P2 | 48.19 | 8.44 | 94.62 | 33.97 | 64.47 | 38.43–63.58 |
| Period | Median | Min | Max | 25% Tile | 75% Tile | 95% CI | p Value | |
|---|---|---|---|---|---|---|---|---|
| Sequence 1 | G1 | 37.97 | 9.16 | 79.40 | 10.03 | 62.73 | 15.37–60.95 | #p = 0.12 a |
| (GCP-Placebo) | G2 | 63.63 | 14.40 | 80.00 | 43.05 | 72.54 | 39.32–75.77 | |
| P1 | 55.34 | 3.44 | 86.77 | 46.84 | 68.58 | 33.33–73.72 | ||
| P2 | 61.97 | 8.80 | 87.94 | 47.56 | 78.04 | 38.96–80.30 | ||
| Sequence 2 | P1 | 51.19 | 10.68 | 89.66 | 20.60 | 66.10 | 25.48–69.98 | #p = 0.48 b |
| (Placebo-GCP) | P2 | 46.14 | 30.96 | 95.41 | 39.03 | 68.41 | 35.29–70.83 | |
| G1 | 52.33 | 21.71 | 91.36 | 37.94 | 70.28 | 36.11–72.66 | ||
| G2 | 45.93 | 39.01 | 90.97 | 41.15 | 76.54 | 38.11–72.55 | ||
| GCP | G1 | 46.73 | 9.16 | 91.36 | 24.51 | 64.62 | 32.79–59.75 | #p = 0.09 c |
| G2 | 54.62 | 14.40 | 90.97 | 41.15 | 72.54 | 45.50–67.37 | ||
| Placebo | P1 | 55.34 | 3.44 | 89.66 | 38.91 | 67.26 | 37.45–63.81 | #p = 0.31 d |
| P2 | 54.69 | 8.80 | 95.41 | 42.44 | 75.50 | 44.34–68.35 |
| Period | Median | Min | Max | 25% Tile | 75% Tile | 95% CI | p Value | |
|---|---|---|---|---|---|---|---|---|
| Sequence 1 | G1 | 74.62 | 45.05 | 98.27 | 50.45 | 91.61 | 55.72–90.01 | #p = 0.09 a |
| (GCP-Placebo) | G2 | 66.08 | 51.66 | 98.71 | 52.94 | 78.78 | 54.38–81.56 | |
| P1 | 63.28 | 20.49 | 95.98 | 53.59 | 74.11 | 44.50–80.76 | ||
| P2 | 71.35 | 26.49 | 97.64 | 63.37 | 89.93 | 52.92–90.47 | ||
| Sequence 2 | P1 | 78.54 | 47.69 | 98.63 | 74.21 | 89.26 | 66.04–91.13 | #p = 0.58 b |
| (Placebo-GCP) | P2 | 75.77 | 50.35 | 94.81 | 53.11 | 93.12 | 57.10–89.50 | |
| G1 | 78.03 | 49.22 | 97.34 | 56.46 | 87.93 | 60.47–88.97 | ||
| G2 | 72.56 | 43.54 | 91.17 | 51.68 | 89.57 | 56.00–87.43 | ||
| GCP | G1 | 76.73 | 45.05 | 98.27 | 53.17 | 91.13 | 64.07–83.52 | #p = 0.31 c |
| G2 | 70.57 | 43.54 | 98.71 | 52.94 | 86.33 | 60.74–78.95 | ||
| Placebo | P1 | 74.05 | 20.49 | 98.63 | 58.93 | 83.43 | 60.05–81.16 | #p = 0.68 d |
| P2 | 72.45 | 26.49 | 97.64 | 55.72 | 90.07 | 61.69–83.30 |
| Period | Median | Min | Max | 25% Tile | 75% Tile | 95% CI | p Value | |
|---|---|---|---|---|---|---|---|---|
| Sequence 1 | G1 | 48.82 | 7.25 | 90.48 | 15.64 | 70.66 | 22.12–72.36 | #p = 0.41 a |
| (GCP-Placebo) | G2 | 65.94 | 20.84 | 89.72 | 27.59 | 81.25 | 35.16–80.94 | |
| P1 | 60.41 | 3.16 | 85.98 | 34.41 | 78.92 | 32.41–79.03 | ||
| P2 | 60.28 | 8.20 | 91.11 | 41.97 | 74.87 | 35.74–77.99 | ||
| Sequence 2 | P1 | 40.39 | 10.05 | 91.56 | 18.31 | 85.61 | 20.44–76.84 | #p = 0.48 b |
| (Placebo-GCP) | P2 | 45.82 | 30.95 | 93.98 | 35.70 | 86.51 | 35.72–79.11 | |
| G1 | 51.98 | 25.97 | 89.05 | 29.51 | 77.09 | 33.47–73.70 | ||
| G2 | 52.13 | 27.40 | 90.07 | 38.61 | 80.93 | 37.17–75.08 | ||
| GCP | G1 | 51.98 | 7.25 | 90.48 | 29.21 | 70.66 | 36.29–64.53 | #p = 0.35 c |
| G2 | 55.47 | 20.84 | 90.07 | 36.60 | 81.25 | 44.14–70.04 | ||
| Placebo | P1 | 56.44 | 3.16 | 91.56 | 24.02 | 80.23 | 36.13–68.23 | #p = 0.23 d |
| P2 | 55.20 | 8.20 | 93.98 | 38.13 | 80.66 | 43.95–70.33 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murakami, M.; Nishi, Y.; Harada, K.; Masuzaki, T.; Minemoto, Y.; Yanagisawa, T.; Shimizu, T.; Tsuboi, A.; Hamada, T.; Nishimura, M. Impact of Oral Intake of Glucosylceramide Extracted from Pineapple on Xerostomia: A Double-Blind Randomized Cross-Over Trial. Nutrients 2019, 11, 2020. https://doi.org/10.3390/nu11092020
Murakami M, Nishi Y, Harada K, Masuzaki T, Minemoto Y, Yanagisawa T, Shimizu T, Tsuboi A, Hamada T, Nishimura M. Impact of Oral Intake of Glucosylceramide Extracted from Pineapple on Xerostomia: A Double-Blind Randomized Cross-Over Trial. Nutrients. 2019; 11(9):2020. https://doi.org/10.3390/nu11092020
Chicago/Turabian StyleMurakami, Mamoru, Yasuhiro Nishi, Kae Harada, Tomohiro Masuzaki, Yoko Minemoto, Takahiro Yanagisawa, Takaharu Shimizu, Akito Tsuboi, Taizo Hamada, and Masahiro Nishimura. 2019. "Impact of Oral Intake of Glucosylceramide Extracted from Pineapple on Xerostomia: A Double-Blind Randomized Cross-Over Trial" Nutrients 11, no. 9: 2020. https://doi.org/10.3390/nu11092020
APA StyleMurakami, M., Nishi, Y., Harada, K., Masuzaki, T., Minemoto, Y., Yanagisawa, T., Shimizu, T., Tsuboi, A., Hamada, T., & Nishimura, M. (2019). Impact of Oral Intake of Glucosylceramide Extracted from Pineapple on Xerostomia: A Double-Blind Randomized Cross-Over Trial. Nutrients, 11(9), 2020. https://doi.org/10.3390/nu11092020