Availability of Donor Milk for Very Preterm Infants Decreased the Risk of Necrotizing Enterocolitis without Adversely Impacting Growth or Rates of Breastfeeding

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
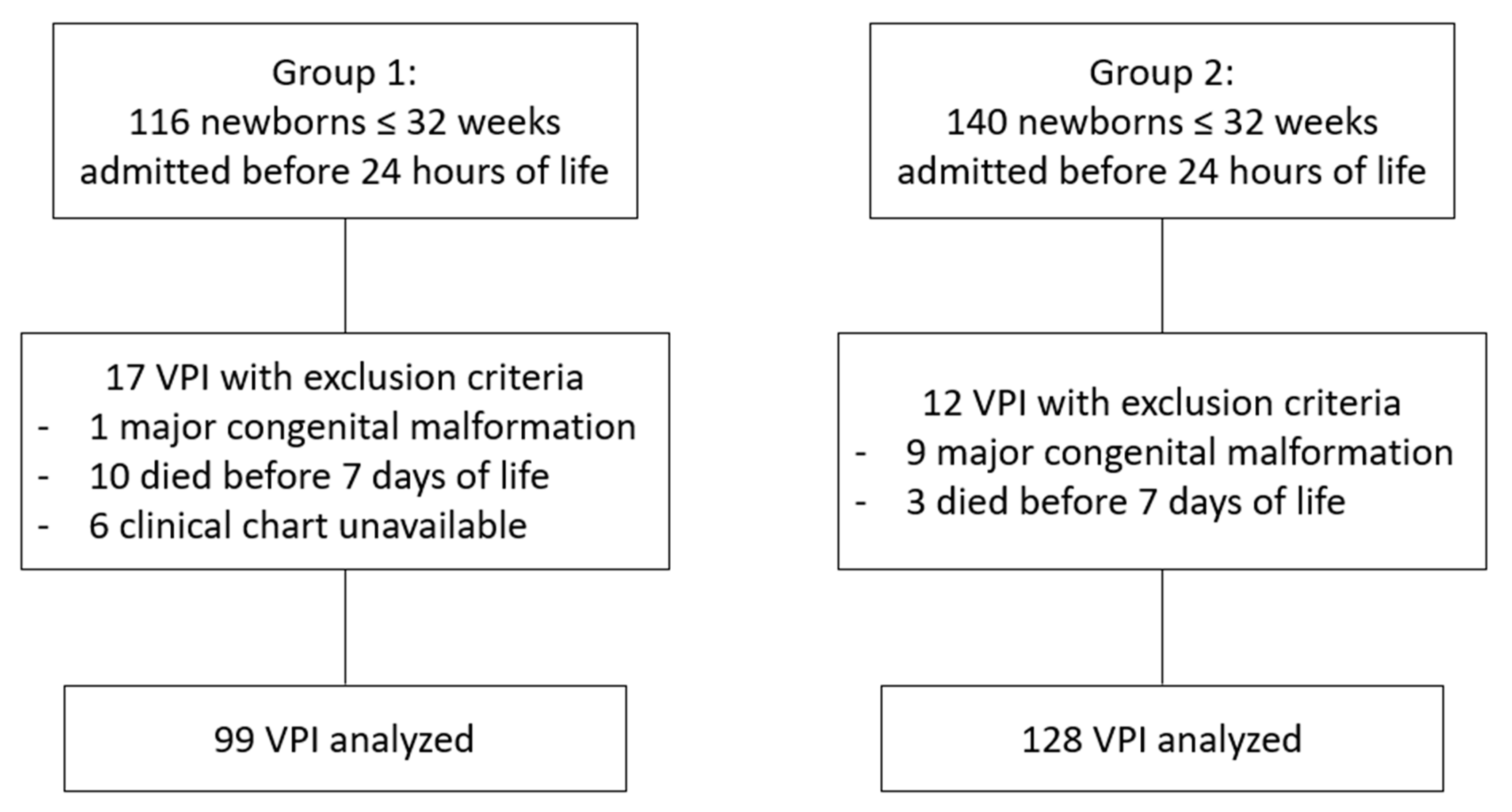
2.2. Patients
2.3. Clinical Protocols
2.4. Study Variables
2.5. Statistical Analysis
3. Results
3.1. Description of the Sample
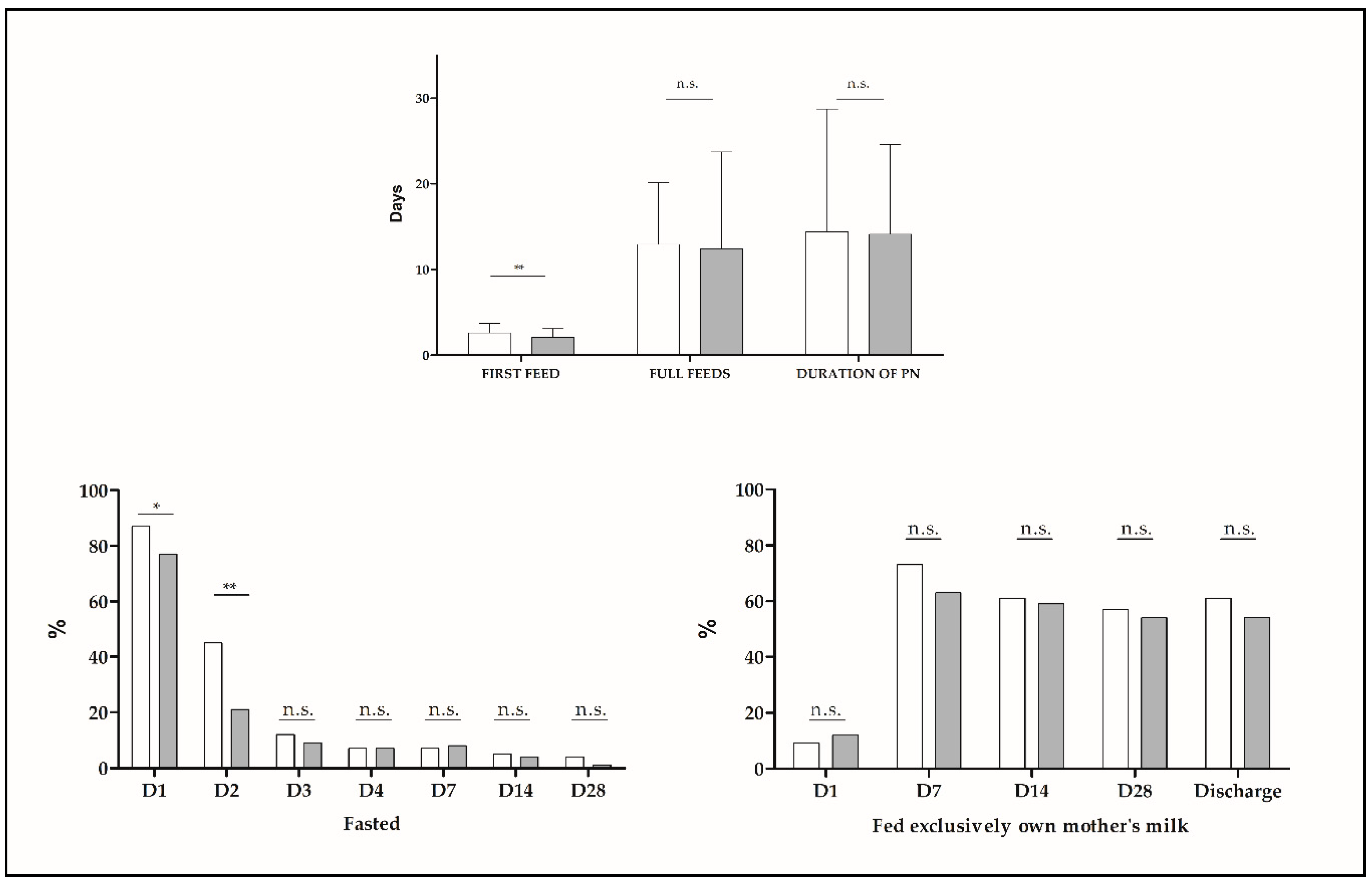
3.2. Enteral Nutrition Was Started Earlier after Availability of DM
3.3. Breastfeeding Rates Did Not Change with the Introduction of Donor Milk
3.4. Rates of Early Growth Were Better in Group 2
3.5. The Incidence of Necrotizing Enterocolitis Decreased after the Introduction of DM
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Morales, Y.; Schanler, R.J. Human Milk and Clinical Outcomes in VLBW Infants: How Compelling Is the Evidence of Benefit? Semin. Perinatol. 2007, 31, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Schanler, R.J.; Shulman, R.J.; Lau, C. Feeding Strategies for Premature Infants: Beneficial Outcomes of Feeding Fortified Human Milk Versus Preterm Formula. Pediatrics 1999, 103, 1150–1157. [Google Scholar] [CrossRef] [PubMed]
- Frost, B.L.; Modi, B.P.; Jaksic, T.; Caplan, M.S. New Medical and surgical insights into neonatal necrotizing enterocolitis a review. JAMA Pediatr. 2017, 171, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Shane, A.L.; Sánchez, P.J.; Stoll, B.J. Neonatal sepsis. Lancet 2017, 390, 1770–1780. [Google Scholar] [CrossRef]
- Cacho, N.T.; Parker, L.A.; Neu, J. Necrotizing Enterocolitis and Human Milk Feeding: A Systematic Review. Clin. Perinatol. 2017, 44, 49–67. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.; Tonkin, E.; Damarell, R.A.; McPhee, A.J.; Suganuma, M.; Suganuma, H.; Middleton, P.F.; Makrides, M.; Collins, C.T. A Systematic Review and Meta-Analysis of Human Milk Feeding and Morbidity in Very Low Birth Weight Infants. Nutrients 2018, 10, 707. [Google Scholar] [CrossRef]
- Quigley, M.; Mcguire, W. Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Libr. 2014, CD002971. [Google Scholar] [CrossRef]
- Aksu, T.; Atalay, Y.; Türkyilmaz, C.; Gülbahar, Ö.; Hirfanoğlu, I.M.; Demirel, N.; Önal, E.; Ergenekon, E.; Koç, E. The effects of breast milk storage and freezing procedure on interleukine-10 levels and total antioxidant activity. J. Matern. Neonatal Med. 2015, 28, 1799–1802. [Google Scholar] [CrossRef]
- Manti, S.; Lougaris, V.; Cuppari, C.; Tardino, L.; Dipasquale, V.; Arrigo, T.; Salpietro, C.; Leonardi, S. Breastfeeding and IL-10 levels in children affected by cow’s milk protein allergy: A restrospective study. Immunobiology 2017, 222, 358–362. [Google Scholar] [CrossRef]
- Arrigo, T.; Leonardi, S.; Cuppari, C.; Manti, S.; Lanzafame, A.; D’Angelo, G.; Gitto, E.; Marseglia, L.; Salpietro, C. Role of the diet as a link between oxidative stress and liver diseases. World J. Gastroenterol. 2015, 21, 384–395. [Google Scholar] [CrossRef]
- Aceti, A.; Beghetti, I.; Martini, S.; Faldella, G.; Corvaglia, L. Oxidative stress and necrotizing enterocolitis: Pathogenetic mechanisms, opportunities for intervention, and role of human milk. Oxid. Med. Cell. Longev. 2018, 2018, 7397659. [Google Scholar] [CrossRef]
- Asztalos, E.V. Supporting mothers of very preterm infants and breast milk production: A review of the role of galactogogues. Nutrients 2018, 10, 600. [Google Scholar] [CrossRef]
- Arslanoglu, S.; Corpeleijn, W.; Moro, G.; Braegger, C.; Campoy, C.; Colomb, V.; Decsi, T.; Domellöf, M.; Fewtrell, M.; Hojsak, I.; et al. Donor human milk for preterm infants: Current evidence and research directions. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 535–542. [Google Scholar] [CrossRef]
- Goelz, R.; Hihn, E.; Hamprecht, K.; Dietz, K.; Jahn, G.; Poets, C.; Elmlinger, M. Effects of different CMV-heat-inactivation-methods on growth factors in human breast milk. Pediatr. Res. 2009, 65, 458–461. [Google Scholar] [CrossRef]
- Daniels, B.; Schmidt, S.; King, T.; Israel-Ballard, K.; Mansen, K.A.; Coutsoudis, A. The effect of simulated flash-heat pasteurization on immune components of human milk. Nutrients 2017, 9, 178. [Google Scholar] [CrossRef]
- Untalan, P.B.; Keeney, S.E.; Palkowetz, K.H.; Rivera, A.; Goldman, A.S. Heat Susceptibility of Interleukin-10 and Other Cytokines in Donor Human Milk. Breastfeed. Med. 2009, 4, 137–144. [Google Scholar] [CrossRef]
- Cristofalo, E.A.; Schanler, R.J.; Blanco, C.L.; Sullivan, S.; Trawoeger, R.; Kiechl-Kohlendorfer, U.; Dudell, G.; Rechtman, D.J.; Lee, M.L.; Lucas, A.; et al. Randomized Trial of Exclusive Human Milk versus Preterm Formula Diets in Extremely Premature Infants. J. Pediatr. 2013, 163, 1592–1595. [Google Scholar] [CrossRef]
- Bertino, E.; Giuliani, F.; Baricco, M.; Di Nicola, P.; Peila, C.; Vassia, C.; Chiale, F.; Pirra, A.; Cresi, F.; Martano, C.; et al. Benefits of donor milk in the feeding of preterm infants. Early Hum. Dev. 2013, 89, S3–S6. [Google Scholar] [CrossRef]
- Villamor-Martínez, E.; Pierro, M.; Cavallaro, G.; Mosca, F.; Kramer, B.W.; Villamor, E. Donor human milk protects against bronchopulmonary dysplasia: A systematic review and meta-analysis. Nutrients 2018, 10, 238. [Google Scholar] [CrossRef]
- Unger, S.; Gibbins, S.; Zupancic, J.; O’Connor, D.L. DoMINO: Donor milk for improved neurodevelopmental outcomes. BMC Pediatr. 2014, 14, 1–12. [Google Scholar] [CrossRef]
- Zhou, J.; Shukla, V.V.; John, D.; Chen, C. Human Milk Feeding as a Protective Factor for Retinopathy of Prematurity: A Meta-analysis. Pediatrics 2015, 136, e1576–e1586. [Google Scholar] [CrossRef]
- Larena Fernández, I.; Vara Callau, M.; Royo Pérez, D.; López Bernués, R.; Cortés Sierra, J.; Samper Villagrasa, M.P. Estudio de los efectos de la implantación de un banco de leche donada en los recién nacidos pretérmino en Aragón. Enferm. Clin. 2015, 25, 57–63. [Google Scholar] [CrossRef]
- Izquierdo, M.; Martínez-Monseny, A.F.; Pociello, N.; Gonzalez, P.; Del Rio, R.; Iriondo, M.; Iglesias-Platas, I. Changes in Parenteral Nutrition during the First Week of Life Influence Early but Not Late Postnatal Growth in Very Low-Birth-Weight Infants. Nutr. Clin. Pract. 2016, 31, 666–672. [Google Scholar] [CrossRef]
- Tudehope, D. Human milk and the nutritional needs of preterm infants. J. Pediatr. 2013, 162, S17–S25. [Google Scholar] [CrossRef]
- Corbes de referència de pes, perímetre cranial i longitut en néixer de nounats d’embarassos únics, de bessons i de trigèmins a Catalunya.
- García Muñoz, F.; García-Alix, A.; Figueras, J.; Saavedra, P. Nuevas curvas poblacionales de crecimiento en recién nacidos extremadamente prematuros espanoles. An. Pediatr. 2013, 6, 1–8. [Google Scholar]
- Bell, M.; Ternberg, J.; Feigin, L. Neonatal necrotizing enterocolitis: Therapeutic decisions based upon clinical staging. Ann. Surg. 1978, 187, 1–7. [Google Scholar] [CrossRef]
- Papile, L.; Burstein, J.; Burstein, R.; Koffler, H. Incidence and evolution of subependimal and intraventricular hemorrhage: A study of infants with birth weight less than 1500 gm. J. Pediatr. 1978, 92, 529–534. [Google Scholar] [CrossRef]
- Patz, A. The new international classification of retinopathy of prematurity. Arch. Ophthalmol. 1984, 74, 160–161. [Google Scholar] [CrossRef]
- Quigley, M.; Embleton, N.D.; Mcguire, W. Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Database Syst. Rev. 2018, 6, CD002971. [Google Scholar] [CrossRef]
- Castellano Yáñez, C.; Castillo Barrio, B.; Muñoz Labián, M.D.C.; Ortiz Movilla, R.; García Lara, N.R.; Royuela Vicente, A.; Marín Gabriel, M.A. Providing very preterm infants with donor human milk led to faster breastfeeding rates but worse biometric gains. Acta Paediatr. Int. J. Paediatr. 2018, 12, 1–2. [Google Scholar] [CrossRef]
- Klingenberg, C.; Embleton, N.D.; Jacobs, S.E.; O’Connell, L.A.F.; Kuschel, C.A. Enteral feeding practices in very preterm infants: An international survey. Arch. Dis. Child. Fetal Neonatal Ed. 2012, 97, 1–3. [Google Scholar] [CrossRef]
- Corpeleijn, W.E.; De Waard, M.; Christmann, V.; Van Goudoever, J.B.; Jansen-Van Der Weide, M.C.; Kooi, E.M.W.; Koper, J.F.; Kouwenhoven, S.M.P.; Lafeber, H.N.; Mank, E.; et al. Effect of donor milk on severe infections and mortality in very low-birth-weight infants: The early nutrition study randomized clinical trial. JAMA Pediatr. 2016, 170, 654–661. [Google Scholar] [CrossRef]
- Assad, M.; Elliott, M.J.; Abraham, J.H. Decreased cost and improved feeding tolerance in VLBW infants fed an exclusive human milk diet. J. Perinatol. 2015, 36, 216–220. [Google Scholar] [CrossRef]
- De Silva, A.; Jones, P.W.; Spencer, S.A. Does human milk reduce infection rates in preterm infants? A systematic review. Arch. Dis. Child. Fetal Neonatal Ed. 2004, 89, 509–514. [Google Scholar] [CrossRef]
- Williams, T.; Nair, H.; Simpson, J.; Embleton, N. Use of Donor Human Milk and Maternal Breastfeeding Rates. J. Hum. Lact. 2016, 32, 212–220. [Google Scholar] [CrossRef]
- Kantorowska, A.; Gould, J.B.; Cohen, R.S.; Lee, H.C.; Wei, J.C.; Lawrence, R.A. Impact of Donor Milk Availability on Breast Milk Use and Necrotizing Enterocolitis Rates. Pediatrics 2016, 137, e20153123. [Google Scholar] [CrossRef]
- Underwood, M.A. Human milk for premature infants. Pediatr. Clin. N. Am. 2013, 60, 189–207. [Google Scholar] [CrossRef]
- Van Goudoever, J.B.; Vlaardingerbroek, H.; Van den Akker, C. Amino Acids and Proteins. World Rev. Nutr. Diet. 2014, 110, 49–63. [Google Scholar]
- Brownell, E.A.; Matson, A.P.; Smith, K.C.; Moore, J.E.; Esposito, P.A.; Lussier, M.M.; Lerer, T.J.; Hagadorn, J.I. Dose-response Relationship between Donor Human Milk, Mother’s Own Milk, Preterm Formula, and Neonatal Growth Outcomes. J. Pediatr. Gastroenterol. Nutr. 2018, 67, 90–96. [Google Scholar] [CrossRef]
- Sisk, P.M.; Lambeth, T.M.; Rojas, M.A.; Lightbourne, T.; Barahona, M.; Anthony, E.; Auringer, S.T. Necrotizing Enterocolitis and Growth in Preterm Infants Fed Predominantly Maternal Milk, Pasteurized Donor Milk, or Preterm Formula: A Retrospective Study. Am. J. Perinatol. 2017, 34, 676–683. [Google Scholar]
- Verd, S.; Porta, R.; Botet, F.; Gutiérrez, A.; Ginovart, G.; Barbero, A.H.; Ciurana, A.; Plata, I.I. Hospital Outcomes of Extremely Low Birth Weight Infants After Introduction of Donor Milk to Supplement Mother’s Milk. Breastfeed. Med. 2015, 10, 150–155. [Google Scholar] [CrossRef]
- Available online: https://www.amerihealthcaritaspa.com/pdf/provider/resources/clinical/policies/170401-donor-human-milk.pdf (accessed on 25 April 2019).
- Silano, M.; Milani, G.P.; Fattore, G.; Agostoni, C. Donor human milk and risk of surgical necrotizing enterocolitis: A meta-analysis. Clin. Nutr. 2019, 38, 1061–1066. [Google Scholar] [CrossRef]
- Binet, M.-E.; Bujold, E.; Lefebre, F.; Tremblay, Y.; Piedboeuf, B. Role of gender in morbidity and mortality of extremely premature neonates. Am. J. Perinatol. 2012, 29, 159–166. [Google Scholar] [CrossRef]
- Alur, P. Sex Differences in Nutrition, Growth, and Metabolism in Preterm Infants. Front. Pediatr. 2019, 7, 1–9. [Google Scholar] [CrossRef]
- Sáenz de Pipaón, M.; Closa, R.; Gormaz, M.; Lines, M.; Nabona, E.; Rodríguez-Martínez, G.; Uberos, J.; Zozaya, C.; Couce, M.L. Nutritional practices in very low birth weight infants: A national survey. Nutr. Hosp. 2017, 34, 1067–1072. [Google Scholar]
- Barone, G.; Maggio, L.; Saracino, A.; Perri, A.; Romagnoli, C.; Zecca, E. How to feed small for gestational age newborn. Ital. J. Pediatr. 2013, 39, 1–5. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Whole Sample | Gestational Age ≤ 28 Weeks | Gestational Age > 28 Weeks | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Group 1 (n = 99) | Group 2 (n = 128) | p | Group 1 (n = 26) | Group 2 (n = 43) | p | Group 1 (n = 73) | Group 2 (n = 85) | p | |
| Mean ± SD | Mean ± SD | Mean ± SD | |||||||
| Gestational age (weeks) | 29.5 ± 2.3 | 29.1 ± 2.3 | 0.227 | 26.2 ± 1.3 | 26.3 ± 1.3 | 0.853 | 30.7 ± 1.1 | 30.5 ± 1.2 | 0.180 |
| Birth weight (g) | 1283 ± 393 | 1197 ± 370 | 0.095 | 844 ± 183 | 854 ± 210 | 0.759 | 1439 ± 323 | 1371 ± 306 | 0.499 |
| Birth weight z score | 0.11 ± 0.87 | −0.14 ± 0.93 | 0.204 | 0.05 ± 0.98 | −0.12 ± 1.05 | 0.516 | −0.00 ± 0.83 | −0.16 ± 0.87 | 0.261 |
| CRIB (Clinical Ric Index for Babies) score | 2.2 ± 3.0 | 2.8 ± 3.1 | 0.188 | 5.5 ± 3.8 | 5.1 ± 3.3 | 0.622 | 1.0 ± 1.4 | 1.6 ± 2.1 | 0.062 |
| n (%) | n (%) | n (%) | |||||||
| Gender (boy) | 56 (56.6%) | 69 (53.9%) | 0.690 | 14 (53.8%) | 23 (53.5%) | 0.977 | 42 (57.5%) | 46 (54.1%) | 0.666 |
| Intrauterine growth restriction (IUGR) | 18 (18.2%) | 15 (11.7%) | 0.171 | 7 (26.9%) | 4 (9.3%) | 0.087 | 11 (15.2%) | 11 (12.9%) | 0.700 |
| Small for gestational age (SGA) | 7 (7.2%) | 10 (8.6%) | 0.706 | 3 (11.5%) | 4 (10.0%) | 1.000 | 4 (5.6%) | 6 (7.9%) | 0.747 |
| Multiple pregnancy | 39 (39.4%) | 47 (36.7%) | 0.771 | 8 (30.8%) | 12 (27.9%) | 0.800 | 31 (42.5%) | 35 (41.2%) | 0.870 |
| Cesarean section | 55 (55.6%) | 86 (67.2%) | 0.073 | 17 (65.4%) | 29 (67.4%) | 0.861 | 38 (52.1%) | 57 (67.1%) | 0.055 |
| Prenatal steroid course (2 doses) | 69 (69.7%) | 79 (61.7%) | 0.211 | 14 (53.8%) | 29 (67.4%) | 0.259 | 55 (75.3%) | 50 (58.8%) | 0.028 |
| Whole Sample | Gestational Age ≤ 28 Weeks | Gestational Age > 28 Weeks | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Group 1 (n = 99) | Group 2 (n = 128) | p | Group 1 (n = 26) | Group 2 (n = 42) | p | Group 1 (n = 73) | Group 2 (n = 85) | p |
| Age at minimum weight (days) | 3.8 ± 1.6 | 3.9 ± 1.5 | 0.612 | 3.9 ± 1.8 | 4.2 ± 1.7 | 0.517 | 3.8 ± 1.6 | 3.8 ± 1.4 | 0.982 |
| % weight loss | 11.4 ± 5.1 | 9.2 ± 8.6 | 0.026 | 13.8 ± 6.0 | 7.8 ± 5.5 | <0.001 | 10.6 ± 4.5 | 10.0 ± 9.8 | 0.617 |
| Age at recovery of birth weight (days) | 11.1 ± 4.1 | 1.4 ± 5.1 | 0.287 | 11.5 ± 5.6 | 10.8 ± 6.9 | 0.663 | 11.0 ± 3.4 | 10.3 ± 3.9 | 0.230 |
| Fall in weight z-score from | |||||||||
| birth to 28 dol | −1.18 ± 0.41 | −0.96 ± 0.66 | 0.003 | −1.33 ± 0.59 | −0.91 ± 0.94 | 0.055 | −1.13 ± 0.32 | −0.98 ± 0.46 | 0.023 |
| birth to 36 weeks PMA | −1.69 ± 0.79 | −1.64 ± 0.70 | 0.652 | −2.31 ± 0.95 | −2.04 ± 0.76 | 0.217 | −1.43 ± 0.53 | −1.38 ± 0.51 | 0.588 |
| birth to discharge | −1.42 ± 0.77 | −1.42 ± 0.79 | 0.951 | −1.96 ± 1.04 | −1.86 ± 0.99 | 0.692 | −1.23 ± 0.55 | −1.21 ± 0.56 | 0.793 |
| Clinical Outcomes During Admission | Whole Sample | Gestational Age ≤ 28 Weeks | Gestational Age > 28 Weeks | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Group 1 (n = 99) | Group 2 (n = 128) | p | Group 1 (n = 26) | Group 2 (n = 43) | p | Group 1 (n = 73) | Group 2 (n = 85) | p | |
| Days on mechanical ventilation | 6.4 ± 15.4 | 5.6 ± 10.8 | 0.651 | 21.2 ± 24.7 | 13.2 ± 13.8 | 0.141 | 1.1 ± 2.4 | 1.7 ±5.9 | 0.401 |
| Days on non-invasive respiratory support | 18.4 ± 21.6 | 21.3 ± 23.2 | 0.339 | 41.9 ± 26.3 | 42.3 ± 24.0 | 0.943 | 10.1 ± 11.1 | 10.7 ± 13.7 | 0.761 |
| Days on oxygen | 16.8 ± 33.0 | 16.3 ± 30.0 | 0.915 | 50.1 ± 49.0 | 42.6 ± 38.6 | 0.485 | 4.9 ± 10.4 | 3.0 ± 8.8 | 0.218 |
| Days on antibiotics | 10.8 ± 12.7 | 12.7 ± 12.9 | 0.267 | 24.4 ± 17.7 | 23.8 ± 14.4 | 0.884 | 6.0 ± 4.6 | 7.1 ± 7.2 | 0.253 |
| Days on central line | 14.4 ± 14.3 | 14.1 ± 10.5 | 0.864 | 25.0 ± 21.8 | 21.7 ± 12.2 | 0.420 | 9.4 ± 5.8 | 10.4 ± 5.0 | 0.247 |
| Days on parenteral nutrition | 13.5 ± 13.9 | 14.2 ± 9.7 | 0.658 | 25.8 ± 23.4 | 23.1 ± 12.8 | 0.542 | 10.3 ± 4.9 | 9.6 ± 4.7 | 0.308 |
| Patent ductus arteriosus | 44/99 (44.4%) | 57/128 (44.5%) | 0.990 | 21/26 (80.8%) | 31/43 (72.1%) | 0.418 | 23/73 (31.5%) | 26/59 (30.6%) | 0.901 |
| Surgical patent ductus arteriosus | 16/99 (16.2%) | 11/128 (8.6%) | 0.081 | 13/26 (50%) | 10/43 (23.3%) | 0.022 | 3/73 (4.1%) | 1/85 (1.2%) | 0.336 |
| Necrotizing enterocolitis | 9/99 (9.1%) | 4/128 (3.1%) | 0.055 | 5/26 (19.2%) | 4/43 (9.3%) | 0.282 | 4/73 (5.5%) | 0/85 (0%) | 0.044 |
| Surgical necrotizing enterocolitis | 5/9 (55.6%) | 1/4 (25%) | 0.308 | 1/26 (3.8%) | 1/43 (2.3%) | 1.000 | 0/73 | 0/85 | - |
| Late-onset sepsis | 18/99 (18.2%) | 27/128 (21.1%) | 0.585 | 14/26 (53.8%) | 22/43 (51.2%) | 0.829 | 4/73 (5.5%) | 5/73 (5.9%) | 0.913 |
| Bronchopulmonary dysplasia | 21/96 (21.9%) | 28/124 (22.6%) | 0.901 | 15/24 (62.5%) | 25/39 (64.1%) | 0.898 | 6/72 (8.3%) | 3/85 (3.5%) | 0.172 |
| Retinopathy of prematurity (any stage) | 27/87 (31%) | 43/113 (38.1%) | 0.302 | 19/23 (82.6%) | 26/40 (65.0%) | 0.136 | 8/64 (12.5%) | 17/56 (23.3%) | 0.103 |
| Severe retinopathy of prematurity | 5/81 (6.2%) | 6/112 (5.4%) | 0.809 | 5/23 (21.7%) | 6/39 (15.4%) | 0.732 | 0/58 (0%) | 0/73 (0%) | - |
| Severe intraventricular hemorrhage (grade III-IV) | 6/99 (6.1%) | 12/128 (9.4%) | 0.359 | 6/26 (23.1%) | 9/43 (20.9%) | 0.834 | 0/73 (0.0%) | 3/85 (3.5%) | 0.250 |
| Death | 4/99 (4%) | 7/128 (5.5%) | 0.619 | 3/26 (11.5%) | 6/43 (14.0%) | 1.000 | 1/73 (1.4%) | 1/85 (1.2%) | 1.000 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cañizo Vázquez, D.; Salas García, S.; Izquierdo Renau, M.; Iglesias-Platas, I. Availability of Donor Milk for Very Preterm Infants Decreased the Risk of Necrotizing Enterocolitis without Adversely Impacting Growth or Rates of Breastfeeding. Nutrients 2019, 11, 1895. https://doi.org/10.3390/nu11081895
Cañizo Vázquez D, Salas García S, Izquierdo Renau M, Iglesias-Platas I. Availability of Donor Milk for Very Preterm Infants Decreased the Risk of Necrotizing Enterocolitis without Adversely Impacting Growth or Rates of Breastfeeding. Nutrients. 2019; 11(8):1895. https://doi.org/10.3390/nu11081895
Chicago/Turabian StyleCañizo Vázquez, Débora, Sandra Salas García, Montserrat Izquierdo Renau, and Isabel Iglesias-Platas. 2019. "Availability of Donor Milk for Very Preterm Infants Decreased the Risk of Necrotizing Enterocolitis without Adversely Impacting Growth or Rates of Breastfeeding" Nutrients 11, no. 8: 1895. https://doi.org/10.3390/nu11081895
APA StyleCañizo Vázquez, D., Salas García, S., Izquierdo Renau, M., & Iglesias-Platas, I. (2019). Availability of Donor Milk for Very Preterm Infants Decreased the Risk of Necrotizing Enterocolitis without Adversely Impacting Growth or Rates of Breastfeeding. Nutrients, 11(8), 1895. https://doi.org/10.3390/nu11081895