Dietary and Supplement-Based Complementary and Alternative Medicine Use in Pediatric Autism Spectrum Disorder

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Dietary Supplement Questionnaire
2.3. Measures
2.4. Procedures
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
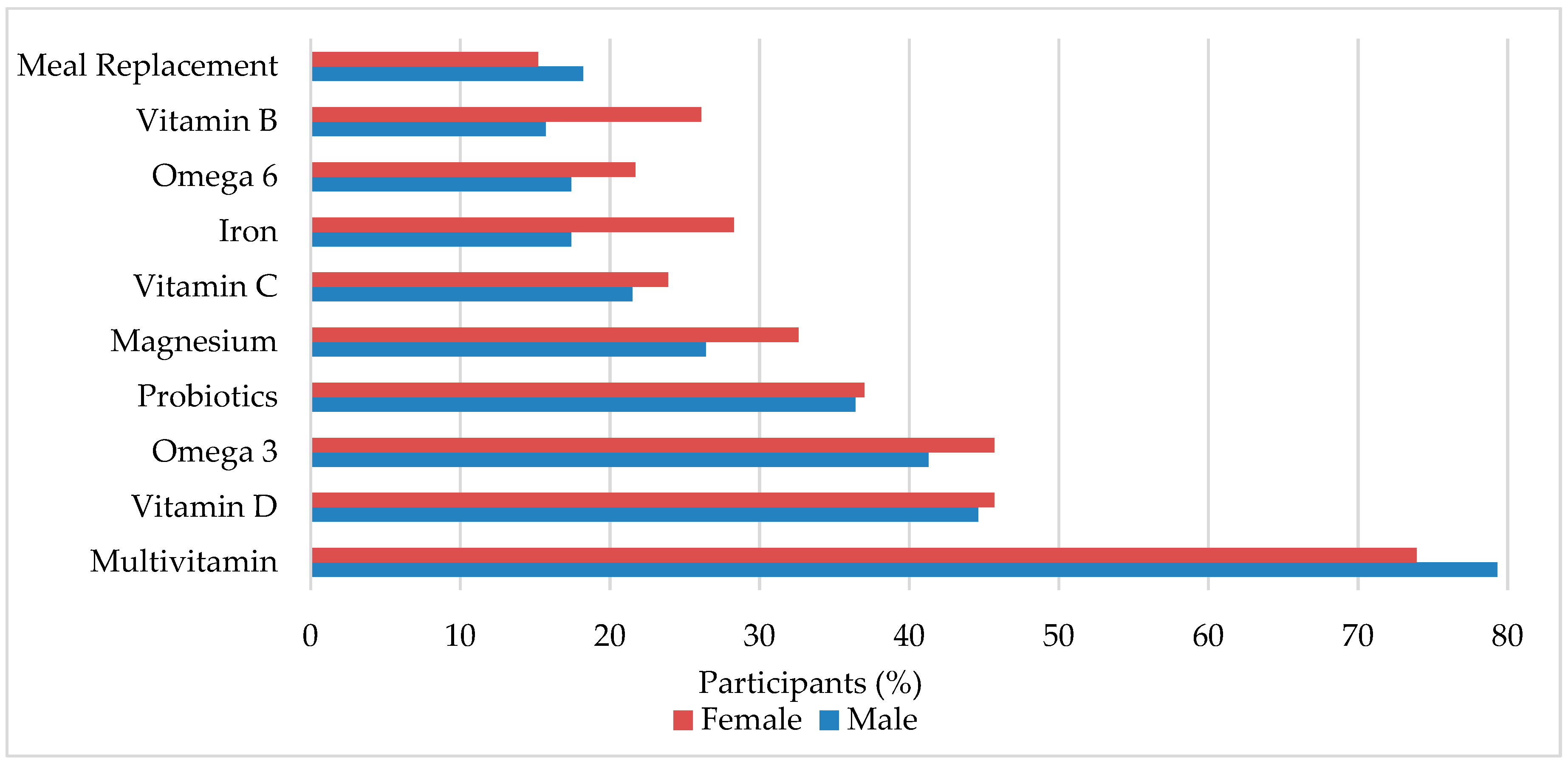
3.2. Dietary Supplement Use
3.3. Dietary Supplement Reasons for Use
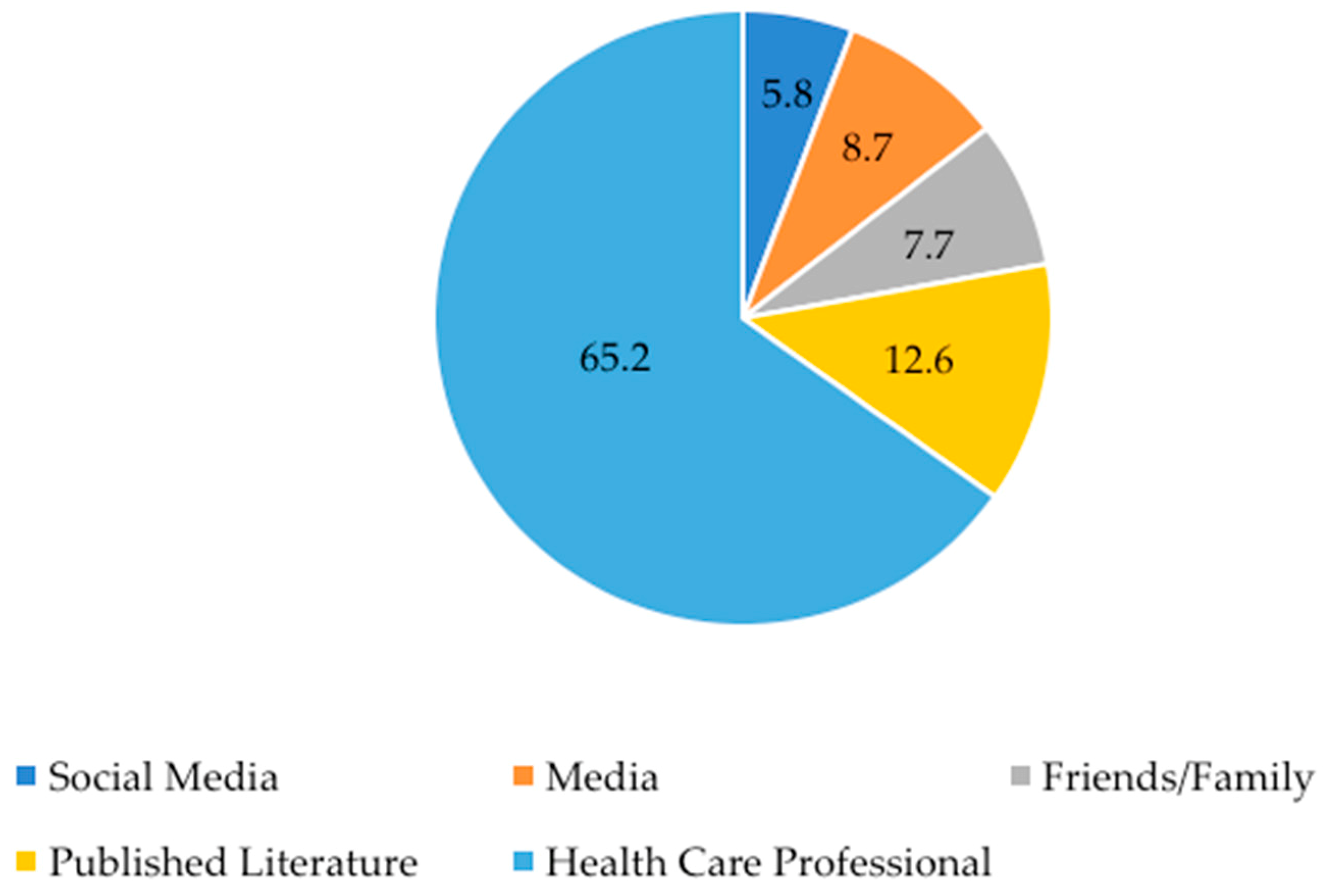
3.4. Special Diets and Information Sources
3.5. Physician Communication
4. Discussion
4.1. Dietary Supplement Patterns and Special Diet Use
4.2. Physician-Patient Communication
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Pub.: Philadelphia, PA, USA, 2013; Volume 21, ISBN 9780890425541. [Google Scholar]
- Lai, M.-C.; Lombardo, M.V.; Baron-Cohen, S. Autism. Lancet 2014, 383, 896–910. [Google Scholar] [CrossRef]
- Redfield, R.R.; Kent, C.K.; Leahy, M.A.; Martinroe, J.C.; Spriggs, S.R.; Yang, T.; Doan, Q.M.; King, P.H.; Maitland, P.D.; Starr, T.M.; et al. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years-Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2014 Surveillance Summaries Centers for Disease Control and Prevention MMWR Editorial and Production Staf. MMWR Surveill Summ. 2018, 67, 2. [Google Scholar]
- Klein, N.; Kemper, K.J. Integrative approaches to caring for children with autism. Curr. Probl. Pediatr. Adolesc. Health Care 2016, 46, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Bryson, S.E.; Rogers, S.J.; Fombonne, E. Autism spectrum disorders: Early detection, intervention, education, and psychopharmacological management. Can. J. Psychiatry 2003, 48, 506–516. [Google Scholar] [CrossRef] [PubMed]
- National Centre for Complementary and Integrative Health. The Use of Complementary and Alternative Medicine in the United States. Available online: https://nccih.nih.gov/research/statistics/2007/camsurvey_fs1.htm (accessed on 14 May 2019).
- National Centre for Complementary and Integrative Health. Complementary, Alternative, or Integrative Health: What’s In a Name? Available online: https://nccih.nih.gov/health/integrative-health (accessed on 14 June 2019).
- Sanders, H.; Davis, M.F.; Duncan, B.; Meaney, F.J.; Haynes, J.; Barton, L.L. Use of complementary and alternative medical therapies among children with special health care needs in southern Arizona. Pediatrics 2003, 111, 584–587. [Google Scholar] [CrossRef] [PubMed]
- Surette, S.; Vanderjagt, L.; Vohra, S. Surveys of complementary and alternative medicine usage: A scoping study of the paediatric literature. Complement. Ther. Med. 2013, 21, S48–S53. [Google Scholar] [CrossRef] [PubMed]
- Levy, S.E.; Mandell, D.S.; Merhar, S.; Ittenbach, R.F.; Pinto-Martin, J. A Use of complementary and alternative medicine among children recently diagnosed with autistic spectrum disorder. J. Dev. Behav. Pediatr. 2003, 24, 418–423. [Google Scholar] [CrossRef]
- Connett, D. Autism: Potentially lethal bleach “cure” feared to have spread to Britain. Available online: https://www.independent.co.uk/life-style/health-and-families/health-news/autism-potentially-lethal-bleach-cure-feared-to-have-spread-to-britain-a6744291.html (accessed on 1 May 2019).
- Anagnostou, E.; Hansen, R. Medical treatment overview: Traditional and novel psycho-pharmacological and complementary and alternative medications. Curr. Opin. Pediatr. 2011, 23, 621–627. [Google Scholar] [CrossRef]
- Huffman, L.C.; Sutcliffe, T.L.; Tanner, I.S.D.; Feldman, H.M. Management of symptoms in children with autism spectrum disorders: A comprehensive review of pharmacologic and complementary-alternative medicine treatments. J. Dev. Behav. Pediatr. 2011, 32, 56–68. [Google Scholar] [CrossRef]
- Hanson, E.; Kalish, L.A.; Bunce, E.; Curtis, C.; McDaniel, S.; Ware, J.; Petry, J. Use of complementary and alternative medicine among children diagnosed with autism spectrum disorder. J. Autism Dev. Disord. 2007, 37, 628–636. [Google Scholar] [CrossRef]
- Robinson, A.; McGrail, M.R. Disclosure of CAM use to medical practitioners: A review of qualitative and quantitative studies. Complement. Ther. Med. 2004, 12, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Izzo, A.; Ernst, E. Interactions Between Herbal Medicines and Prescribed Drugs. Drugs 2009, 69, 1777–1798. [Google Scholar] [CrossRef] [PubMed]
- Lenth, R. Java Applets for Power and Sample Size. Available online: https://homepage.divms.uiowa.edu/~rlenth/Power/ (accessed on 17 May 2019).
- Wiens, K.; Erdman, K.A.; Stadnyk, M.; Parnell, J.A. Dietary supplement usage, motivation, and education in young Canadian athletes. Int. J. Sport Nutr. Exerc. Metab. 2014, 24, 613–622. [Google Scholar] [CrossRef] [PubMed]
- Parnell, J.A.; Wiens, K.P.; Erdman, K.A. Dietary intakes and supplement use in pre-adolescent and adolescent Canadian athletes. Nutrients 2016, 8, 526. [Google Scholar] [CrossRef] [PubMed]
- The National Academies of Science and Medicine Dietary Reference Intakes Tables and Application. Available online: http://nationalacademies.org/hmd/Activities/Nutrition/SummaryDRIs/DRI-Tables.aspx (accessed on 13 June 2019).
- Brondino, N.; Fusar-Poli, L.; Rocchetti, M.; Provenzani, U.; Barale, F.; Politi, P. Complementary and alternative therapies for autism spectrum disorder. Evidence-Based Complement. Altern. Med. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Stewart, P.A.; Hyman, S.L.; Schmidt, B.L.; Macklin, E.A.; Reynolds, A.; Johnson, C.R.; James, S.J.; Manning-Courtney, P. Dietary Supplementation in Children with Autism Spectrum Disorders: Common, Insufficient, and Excessive. J. Acad. Nutr. Diet. 2015, 115, 1237–1248. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.B.; Audhya, T.; McDonough-Means, S.; Rubin, R.A.; Quig, D.; Geis, E.; Gehn, E.; Loresto, M.; Mitchell, J.; Atwood, S. Effect of a vitamin/mineral supplement on children and adults with autism. BMC Pediatr. 2011, 11, 111. [Google Scholar] [CrossRef]
- Cannell, J.J. Vitamin D and autism, what’s new? Rev. Endocr. Metab. Disord. 2017, 18, 183–193. [Google Scholar] [CrossRef]
- Saad, K.; Abdel-rahman, A.A.; Elserogy, Y.M.; Al-Atram, A.A.; Cannell, J.J.; Bjørklund, G.; Abdel-Reheim, M.K.; Othman, H.A.K.; El-Houfey, A.A.; Abd El-Aziz, N.H.R.; et al. Vitamin D status in autism spectrum disorders and the efficacy of vitamin D supplementation in autistic children. Nutr. Neurosci. 2015, 19, 346–351. [Google Scholar] [CrossRef]
- Sathe, N.; Andrews, J.C.; McPheeters, M.L.; Warren, Z.E. Nutritional and Dietary Interventions for Autism Spectrum Disorder: A Systematic Review. Pediatrics 2017, 139. [Google Scholar] [CrossRef]
- Food and Drug Administration. Report to the Honorable Barry M. Goldwater Jr. House of Representatives - Adrenal Cortex Extract Taken Off the Market. Available online: http://archive.gao.gov/f0102/115802.pdf (accessed on 25 July 2019).
- Hurt, R.T.; Mundi, M.S. Over-the-Counter Adrenal Supplements: More than Meets the Eye. Mayo Clin. Proc. 2018, 93, 276–277. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. Important Alert Adrenal Cortext Extract. Available online: https://www.accessdata.fda.gov/cms_ia/importalert_172.html (accessed on 14 September 2018).
- Piwowarczyk, A.; Horvath, A.; Łukasik, J.; Pisula, E.; Szajewska, H. Gluten- and casein-free diet and autism spectrum disorders in children: A systematic review. Eur. J. Nutr. 2018, 57, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Castro, K.; Faccioli, L.S.; Baronio, D.; Gottfried, C.; Perry, I.S.; Dos Santos Riesgo, R. Effect of a ketogenic diet on autism spectrum disorder: A systematic review. Res. Autism Spectr. Disord. 2015, 20, 31–38. [Google Scholar] [CrossRef]
- El-Rashidy, O.; El-Baz, F.; El-Gendy, Y.; Khalaf, R.; Reda, D.; Saad, K. Ketogenic diet versus gluten free casein free diet in autistic children: A case-control study. Metab. Brain Dis. 2017, 32, 1935–1941. [Google Scholar] [CrossRef] [PubMed]
- Newell, C.; Bomhof, M.R.; Reimer, R.A.; Hittel, D.S.; Rho, J.M.; Shearer, J. Ketogenic diet modifies the gut microbiota in a murine model of autism spectrum disorder. Mol. Autism 2016, 7, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kemper, K.J.; Vohra, S.; Walls, R. The Use of Complementary and Alternative Medicine in Pediatrics. Pediatrics 2008, 122, 1374–1386. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Descriptive Characteristics | All | Males | Females |
|---|---|---|---|
| Participants | 210 | 157 (74.8%) | 53 (25.2%) |
| Age, years | 9.2 (3.6) | 9.0 (3.6) | 9.5 (3.7) |
| Year of Diagnosis | |||
| 2003–2007 | 16 (7.8%) | 14 (6.8%) | 2 (1.0%) |
| 2008–2012 | 42 (20.5%) | 28 (13.7%) | 14 (6.8%) |
| 2013–2018 | 147 (71.7%) | 113 (55.1%) | 34 (16.6%) |
| Characteristic | All n (%) | Males n (%) | Females n (%) |
|---|---|---|---|
| Ethnicity | |||
| Caucasian | 170 (81.3) | 124 (59.3) | 46 (22.0) |
| Asian/Pacific Islander | 13 (6.2) | 11 (5.3) | 2 (1.0) |
| Hispanic or Latino | 2 (1.0) | 2 (1.0) | 0 (0.0) |
| Black or African American | 5 (2.4) | 2 (1.0) | 3 (1.4) |
| First Nations or Metis or Inuit | 6 (2.9) | 5 (2.4) | 1 (0.5) |
| Multiracial | 13 (6.2) | 12 (5.7) | 1 (0.5) |
| Household Income | |||
| >$20,000 | 10 (4.8) | 7 (3.3) | 3 (1.4) |
| $20,000–40,000 | 23 (11.0) | 18 (8.6) | 5 (2.4) |
| $40,000–60,000 | 23 (11.0) | 17 (8.1) | 6 (2.9) |
| $60,000–80,000 | 33 (15.7) | 25 (11.9) | 8 (3.8) |
| $80,000–$100,000 | 35 (16.7) | 23 (11.0) | 12 (5.7) |
| $100,000+ | 75 (35.7) | 60 (28.6) | 15 (7.1) |
| Not Applicable | 11 (5.2) | 7 (3.3) | 4 (1.9) |
| Parent Level of Education | |||
| High School Diploma | 17 (8.2) | 13 (6.3) | 4 (1.9) |
| Trade School Diploma | 4 (1.9) | 3 (1.4) | 1 (0.5) |
| Some College | 17 (8.2) | 13 (6.3) | 4 (1.9) |
| College Diploma | 51 (24.5) | 41 (19.7) | 10 (4.8) |
| Some University | 19 (9.1) | 17 (8.2) | 2 (1.0) |
| University Degree | 52 (25.0) | 40 (19.2) | 12 (5.8) |
| Master’s Degree | 30 (14.4) | 21 (10.1) | 9 (4.3) |
| Professional Degree | 11 (5.3) | 5 (2.4) | 6 (2.9) |
| Ph.D. | 7 (3.4) | 3 (1.4) | 4 (1.9) |
| All n (%) | Males n (%) | Females n (%) | p | |
|---|---|---|---|---|
| Reasons for Use | ||||
| Enhance diet | 127 (76.0) | 94 (56.3) | 33 (19.8) | 0.424 |
| Promote immune system function | 88 (52.7) | 66 (39.5) | 22 (13.2) | 0.490 |
| Increase quality/duration of sleep | 76 (45.5) | 53 (31.7) | 23 (13.8) | 0.602 |
| Improve cognitive ability | 54 (32.3) | 34 (20.4) | 20 (12.0) | 0.066 |
| Decrease repetitive or restrictive behavior | 21 (12.6) | 16 (9.6) | 5 (3.0) | 0.798 |
| Promote sociability | 18 (10.8) | 12 (7.2) | 6 (3.6) | 0.581 |
| Increase interactions with others | 13 (7.8) | 8 (4.8) | 5 (3.0) | 0.349 |
| Enhance motor skills | 12 (7.2) | 9 (5.4) | 3 (1.8) | 1.000 |
| Reasons Against Use | ||||
| Inadequate knowledge/information | 14 (32.6) | 12 (27.9) | 2 (4.7) | 1.000 |
| Too expensive | 8 (18.6) | 7 (16.3) | 1 (2.3) | 1.000 |
| May be considered harmful | 5 (11.6) | 5 (11.6) | 0 (0.0) | 0.574 |
| Based on suggestion from close family/friends | 4 (9.3) | 4 (9.3) | 0 (0.0) | 1.000 |
| Read in scholarly article | 4 (9.3) | 4 (9.3) | 0 (0.0) | 1.000 |
| All n (%) | Males n (%) | Females n (%) | p | |
|---|---|---|---|---|
| No restrictions | 142 (67.6) | 113 (72.0) | 29 (54.7) | 0.027 |
| Gluten free | 21 (10.0) | 8 (5.1) | 13 (24.5) | <0.001 |
| High carb | 17 (8.1) | 14 (8.9) | 3 (5.7) | 0.570 |
| Lactose free | 16 (7.6) | 7 (4.5) | 9 (17.0) | 0.006 |
| Casein free | 12 (5.7) | 8 (5.1) | 4 (7.5) | 0.734 |
| High protein | 8 (3.8) | 4 (2.5) | 4 (7.5) | 0.206 |
| Ketogenic diet (i.e., high fat, low card) | 7 (3.3) | 6 (3.8) | 1 (1.9) | 0.682 |
| Vegetarian | 4 (1.9) | 2 (1.3) | 2 (3.8) | 0.574 |
| Vegan | 0 (0.0) | 0 (0.0) | 0 (0.0) | n/a |
| Disclosure of Number of Supplements (%) | Frequency n (%) |
|---|---|
| None (0) | 11 (6.6) |
| Some (1–49) | 14 (8.4) |
| Half (50) | 8 (4.8) |
| Most (51–99) | 23 (13.8) |
| All (100) | 111 (66.5) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trudeau, M.S.; Madden, R.F.; Parnell, J.A.; Gibbard, W.B.; Shearer, J. Dietary and Supplement-Based Complementary and Alternative Medicine Use in Pediatric Autism Spectrum Disorder. Nutrients 2019, 11, 1783. https://doi.org/10.3390/nu11081783
Trudeau MS, Madden RF, Parnell JA, Gibbard WB, Shearer J. Dietary and Supplement-Based Complementary and Alternative Medicine Use in Pediatric Autism Spectrum Disorder. Nutrients. 2019; 11(8):1783. https://doi.org/10.3390/nu11081783
Chicago/Turabian StyleTrudeau, Melanie S., Robyn F. Madden, Jill A. Parnell, W. Ben Gibbard, and Jane Shearer. 2019. "Dietary and Supplement-Based Complementary and Alternative Medicine Use in Pediatric Autism Spectrum Disorder" Nutrients 11, no. 8: 1783. https://doi.org/10.3390/nu11081783
APA StyleTrudeau, M. S., Madden, R. F., Parnell, J. A., Gibbard, W. B., & Shearer, J. (2019). Dietary and Supplement-Based Complementary and Alternative Medicine Use in Pediatric Autism Spectrum Disorder. Nutrients, 11(8), 1783. https://doi.org/10.3390/nu11081783