Nutritrauma: A Key Concept for Minimising the Harmful Effects of the Administration of Medical Nutrition Therapy

 , and
, and
Abstract
1. Introduction
2. Medical Nutrition Therapy as a Form of Life Support
3. Complications of Medical Nutrition Therapy that should be Included in the Definition of Nutritrauma
3.1. Miscalculation of Calorie and Protein Requirements
3.2. Fluid Overload
3.3. Metabolic Complications of Electrolyte and Acid-Base Imbalance
3.4. Hypertriglyceridaemia
3.5. Hepatobiliary Disorders Associated with Parenteral Nutrition
3.6. Metabolic Bone Disease
3.7. Hyperglycaemia
3.8. Hypersensitivity
3.9. Refeeding Syndrome
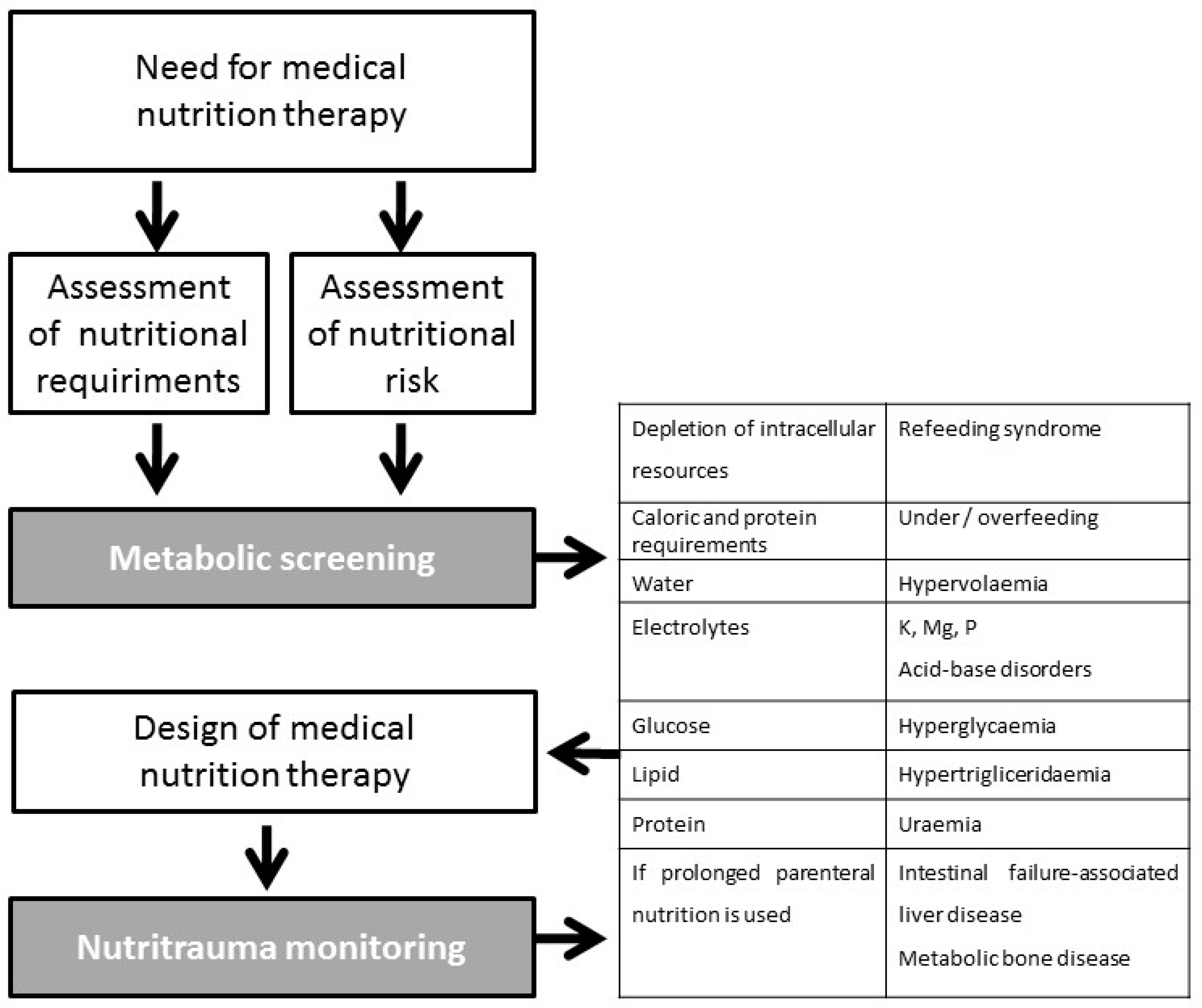
4. Monitoring Requirements
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gordo Vidal, F.; Delgado Arnaiz, C.; Calvo Herranz, E. Mechanical ventilation induced lung injury. Med. Intensiva 2007, 31, 18–26. [Google Scholar] [CrossRef]
- Akhoundi, A.; Singh, B.; Vela, M.; Chaudhary, S.; Monaghan, M.; Wilson, G.A.; Dillon, J.J.; Cartin-Ceba, R.; Lieske, J.C.; Gajic, O.; et al. Incidence of Adverse Events during Continuous Renal Replacement Therapy. Blood Purif. 2015, 39, 333–339. [Google Scholar] [CrossRef] [PubMed]
- International Consensus Conferences in Intensive Care Medicine. Ventilator-associated lung injury in ARDS. American Thoracic Society, European Society of Intensive Care Medicine, Societé de Réanimation Langue Française. Intensive Care Med. 1999, 25, 1444–1452. [Google Scholar] [CrossRef]
- Maynar Moliner, J.; Honore, P.M.; Sánchez-Izquierdo Riera, J.A.; Herrera Gutiérrez, M.; Spapen, H.D. Handling continuous renal replacement therapy-related adverse effects in intensive care unit patients: The dialytrauma concept. Blood Purif. 2012, 34, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Marini, J.J.; Collino, F.; Maiolo, G.; Rapetti, F.; Tonetti, T.; Vasques, F.; Quintel, M. The future of mechanical ventilation: Lessons from the present and the past. Crit. Care 2017, 21, 183. [Google Scholar] [CrossRef] [PubMed]
- Wischmeyer, P.E. Tailoring nutrition therapy to illness and recovery. Crit. Care 2017, 21 (Suppl. S3), 316. [Google Scholar] [CrossRef] [PubMed]
- Arabi, Y.M.; Casaer, M.P.; Chapman, M.; Heyland, D.K.; Ichai, C.; Marik, P.E.; Martindale, R.G.; McClave, S.A.; Preiser, J.-C.; Reignier, J.; et al. The intensive care medicine research agenda in nutrition and metabolism. Intensive Care Med. 2017, 43, 1239–1256. [Google Scholar] [CrossRef] [PubMed]
- Schindler, K.; Pichard, C.; Sulz, I.; Volkert, D.; Streicher, M.; Singer, P.; Ljungqvistf, O.; Van Gossumg, A.; Bauerc, P.; Hiesmayrh, H. NutritionDay: 10 years of growth. Clin. Nutr. 2017, 36, 1207–1214. [Google Scholar] [CrossRef]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Fuentes Padilla, P.; Martínez, G.; Vernooij, R.W.M.; Cosp, X.B.; Alonso-Coello, P. Nutrition in critically ill adults: A systematic quality assessment of clinical practice guidelines. Clin. Nutr. 2016, 35, 1219–1225. [Google Scholar] [CrossRef]
- Weijs, P.J.; Stapel, S.N.; de Groot, S.D.; Driessen, R.H.; de Jong, E.; Girbes, A.R.; Rob, J.M.; van Schijndel, S.; Beishuizen, A. Optimal protein and energy nutrition decreases mortality in mechanically ventilated, critically ill patients: A prospective observational cohort study. J. Parenter. Enter. Nutr. 2012, 36, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Zusman, O.; Theilla, M.; Cohen, J.; Kagan, I.; Bendavid, I.; Singer, P. Resting energy expenditure, calorie and protein consumption in critically ill patients: A retrospective cohort study. Crit. Care 2016, 20, 367. [Google Scholar] [CrossRef] [PubMed]
- Shaw, J.H.; Wolfe, R.R. An integrated analysis of glucose, fat, and protein metabolism in severely traumatized patients. Studies in the basal state and the response to total parenteral nutrition. Ann. Surg. 1989, 209, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Reintam Blaser, A.; Berger, M.M. Early or Late Feeding after ICU Admission? Nutrients 2017, 9, 1278. [Google Scholar] [CrossRef] [PubMed]
- Jebb, S.A.; Prentice, A.M.; Goldberg, G.R.; Murgatroyd, P.R.; Black, A.E.; Coward, W.A. Changes in macronutrient balance during over- and underfeeding assessed by 12-d continuous whole-body calorimetry. Am. J. Clin. Nutr. 1996, 64, 259–266. [Google Scholar] [CrossRef]
- Talpers, S.S.; Romberger, D.J.; Bunce, S.B.; Pingleton, S.K. Nutritionally associated increased carbon dioxide production. Excess total calories vs high proportion of carbohydrate calories. Chest 1992, 102, 551–555. [Google Scholar] [CrossRef]
- Bordeje, M.L. Nuestros grandes olvidados, los enfermos respiratorios crónicos. Nutr. Hosp. 2017, 34 (Suppl. S1), 38–45. [Google Scholar]
- Singer, P.; Anbar, R.; Cohen, J.; Shapiro, H.; Shalita-Chesner, M.; Shaul, L.; Grozovski, E.; Theilla, M.; Frishman, S.; Madar, Z. The Tight Calorie Control Study (TICACOS): A prospective, randomized, controlled pilot study of nutritional support in critically ill patients. Intensive Care Med. 2011, 37, 601–609. [Google Scholar] [CrossRef]
- Grau, T.; Bonet, A. Caloric intake and liver dysfunction in critically ill patients. Curr. Opin. Clin. Nutr. Metab. Care. 2009, 12, 175–179. [Google Scholar] [CrossRef]
- Grau, T.; Bonet, A.; Rubio, M.; Mateo, D.; Farré, M.; Acosta, J.A.; Blesa, A.; Montejo, J.C.; de Lorenzo, A.G.; Mesejo, A.; et al. Liver dysfunction associated with artificial nutrition in critically ill patients. Crit. Care 2007, 11, R10. [Google Scholar] [CrossRef]
- Singer, P.; Blaser, A.R.; Berger, M.M.; Alhazzani, W.; Calder, P.C.; Casaer, M.P.; Hiesmayr, M.; Mayer, K.; Montejo, J.C.; Pichard, C.; et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin. Nutr. 2019, 38, 48–79. [Google Scholar] [CrossRef]
- McClave, S.A.; Taylor, B.E.; Martindale, R.G.; Warren, M.M.; Johnson, D.R.; Braunschweig, C.; McCarthy, M.S.; Davanos, E.; Rice, T.W.; Cresci, G.A.; et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J. Parenter. Enter. Nutr. 2016, 40, 159–211, Erratum in: JPEN J. Parenter Enteral Nutr. 2016, 40, 1200. [Google Scholar] [CrossRef]
- Biesalski, H.K.; Bischoff, S.C.; Boehles, H.J.; Muehlhoefer, A.; Working group for developing the guidelines for parenteral nutrition of The German Association for Nutritional Medicine. Water, electrolytes, vitamins and trace elements—Guidelines on Parenteral Nutrition, Chapter 7. Ger. Med. Sci. 2009, 7, Doc21. [Google Scholar]
- Boyd, J.H.; Forbes, J.; Nakada, T.A.; Walley, K.R.; Russell, J.A. Fluid resuscitation in septic shock: A positive fluid balance and elevated central venous pressure are associated with increased mortality. Crit. Care Med. 2011, 39, 259–265. [Google Scholar] [CrossRef]
- Rhoda, K.M.; Porter, M.J.; Quintini, C. Fluid and electrolyte management: Putting aplan in motion. JPEN J. Parenter. Enter. Nutr. 2011, 35, 675–685. [Google Scholar] [CrossRef]
- Davila, J.; Konrad, D. Metabolic Complications of Home Parenteral Nutrition. Nutr. Clin. Pract. 2017, 32, 753–768. [Google Scholar] [CrossRef]
- Whang, R.; Whang, D.D.; Ryan, M.P. Refractory potassium repletion: A consequence of magnesium deficiency. Arch. Intern. Med. 1992, 152, 40–45. [Google Scholar] [CrossRef]
- Brown, R.O.; Hamrick, K.D.; Dickerson, R.N.; Lee, N.; Parnell, D.H., Jr.; Kudsk, K.A. Hyperkalemia secondary to concurrent pharmacotherapy in a patient receiving home parenteral nutrition. J. Parenter. Enter. Nutr. 1996, 20, 429–432. [Google Scholar] [CrossRef]
- Steele, T.; Kolamunnage-Dona, R.; Downey, C.; Toh, C.H.; Welters, I. Assessment and clinical course of hypocalcemia in critical illness. Crit. Care 2013, 3, R106. [Google Scholar] [CrossRef]
- Kelly, A.; Levine, M.A. Hypocalcemia in the critically ill patient. J. Intensive Care Med. 2013, 28, 166–177. [Google Scholar] [CrossRef]
- Mirtallo, J.M. Introduction to parenteral nutrition. In The Science and Practice of Nutrition Support. A Case-Based Core Curriculum. Part III: The Clinical Foundations of Nutrition Support; Gottschlich, M.M., Fuhrman, M.P., Hammond, K.A., Holcombe, B.J., Seidner, D.L., Eds.; Kendall Hunt Publishing: Dubuque, IA, USA, 2001; pp. 211–222. [Google Scholar]
- Mirtallo, J.; Canada, T.; Johnson, D.; Kumpf, V.; Petersen, C.; Sacks, G.; Seres, D.; Guenter, P. Task Force for the Revision of Safe Practices for Parenteral Nutrition. Safe practices for parenteral nutrition. J. Parenter. Enter. Nutr. 2004, 26, S39. [Google Scholar] [CrossRef]
- Btaiche, J.F.; Khalidi, N. Metabolic complications of parenteral nutrition in adults, Part 1. Am. J. Health Syst. Pharm. 2004, 61, 1938–1949. [Google Scholar] [CrossRef]
- Mirtallo, J.M.; Dasta, J.F.; Kleinschmidt, K.C.; Varon, J. State of the art review: Intravenous fat emulsions: Current applications, safety profile, and clinical implications. Ann. Pharmacother. 2010, 44, 688–700. [Google Scholar] [CrossRef]
- Llop, J.; Sabin, P.; Garau, M.; Burgos, R.; Pérez, M.; Massó, J.; Cardona, D.; Sánchez Segura, J.M.; Garriga, R.; Redondo, S.; et al. The importance of clinical factors in parenteral nutrition-associated hypertriglyceridemia. Clin. Nutr. 2003, 22, 577–583. [Google Scholar] [CrossRef]
- Mateu-de Antonio, J.; Grau, S.; Luque, S.; Marin-Casino, M.; Albert, I.; Ribes, E. Comparative effects of olive oil-based and soyabean oil-based emulsions on infection rate and leucocyte count in critically ill patients receiving parenteral nutrition. Br. J. Nutr. 2008, 99, 846–854. [Google Scholar] [CrossRef]
- Devaud, J.C.; Berger, M.M.; Pannatier, A.; Marques-Vidal, P.; Tappy, L.; Rodondi, N.; Voirol, C.P. Hypertriglyceridemia: A potential side effect of propofol sedation in critical illness. Intensive Care Med. 2012, 38, 1990–1998. [Google Scholar] [CrossRef]
- Devlin, J.W.; Lau, A.K.; Tanios, M.A. Propofol-associated hypertriglyceridemia and pancreatitis in the intensive care unit: An analysis of frequency and risk factors. Pharmacotherapy 2005, 25, 1348–1352. [Google Scholar] [CrossRef]
- Berger, M.M.; Reintam-Blaser, A.; Calder, P.C.; Casaer, M.; Hiesmayr, M.J.; Mayer, K.; Montejoj, J.C.; Pichardk, C.; Preiserl, J.-C.; van Zantenm, A.R.H.; et al. Monitoring nutrition in the, I.C.U. Clin. Nutr. 2019, 38, 584–593. [Google Scholar] [CrossRef]
- Braga, M.; Ljungqvist, O.; Soeters, P.; Fearon, K.; Weimann, A.; Bozzetti, F. ESPEN guidelines on parenteral nutrition: Surgery. Clin. Nutr. 2009, 28, 378–386. [Google Scholar] [CrossRef]
- Visschers, R.G.; Olde Damink, S.W.; Gehlen, J.M.; Winkens, B.; Soeters, P.B.; van Gemert, W.G. Treatment of hypertriglyceridemia in patients receiving parenteral nutrition. J. Parenter. Enter. Nutr. 2011, 35, 610–615. [Google Scholar] [CrossRef]
- Adolph, M.; Heller, A.R.; Koch, T.; Koletzko, B.; Kreymann, K.G.; Krohn, K.; Pscheidl, E.; Senkal, M.; Working group for developing the guidelines for parenteral nutrition of The German Association for Nutritional Medicine. Lipid emulsions—Guidelines on parenteral nutrition, Chapter 6. Ger. Med. Sci. 2009, 7, Doc22. [Google Scholar] [CrossRef]
- Kumpf, V.J.; Gervasio, J. Complications of parenteral nutrition. In The ASPEN Nutrition Support Core Curriculum, 2nd ed.; Mueller, C.M., Kovacevich, D.S., McClave, S.A., Stephen, A.M., Schwartrz, D.B., Miller, S.J., Eds.; ASPEN: Silver Spring, MD, USA, 2012; pp. 284–298. [Google Scholar]
- Cavicchi, M.; Beau, P.; Crenn, P.; Degott, C.; Messing, B. Prevalence of liver disease and contributing factors in patients receiving home parenteral nutrition for permanent intestinal failure. Ann. Intern. Med. 2000, 132, 525–532. [Google Scholar] [CrossRef]
- Kumpf, V. Parenteral nutrition-associated liver disease in adult and pediatric patients. Nutr. Clin. Pract. 2006, 21, 279–290. [Google Scholar] [CrossRef]
- Anez-Bustillos, L.; Dao, D.T. Intravenous fat emulsion formulations for the adult and pediatric patient: Understanding the differences. Nutr. Clin. Pract. 2016, 31, 596–609. [Google Scholar] [CrossRef]
- Lappas, B.M.; Patel, D.; Kumpf, V.; Adams, D.W.; Seidner, D.L. Parenteral Nutrition: Indications, Access, and Complications. Gastroenterol. Clin. N. Am. 2018, 47, 39–59. [Google Scholar] [CrossRef]
- Pironi, L.; Labate, A.M.; Pertkiewicz, M.; Przedlacki, J.; Tjellesen, L.; Staun, M.; De Francesco, A.; Gallenca, P.; Guglielmi, F.W.; Van Gossum, A.N.D.R.É; et al. Prevalence of bone disease in patients on home parenteral nutrition. Clin. Nutr. 2002, 21, 289–296. [Google Scholar] [CrossRef]
- Verhage, A.H.; Cheong, W.K.; Allard, J.P.; Jeejeebhoy, K.N.; Harry, M. Vars Research Award. Increase in lumbar spine bone mineral content in patients on long-term parenteral nutrition without vitamin D supplementation. J. Parenter. Enter. Nutr. 1995, 19, 431–436. [Google Scholar] [CrossRef]
- Pleva, M.; Mirtallo, J.M.; Steinberg, S.M. Hyperglycemic events in non-intensive care unit patients receiving parenteral nutrition. Nutr. Clin. Pract. 2009, 24, 626–634. [Google Scholar] [CrossRef]
- Gosmanov, A.R.; Umpierrez, G.E. Management of hyperglycemia during enteral and parenteral nutrition therapy. Curr. Diabetes Rep. 2013, 13, 155–162. [Google Scholar] [CrossRef]
- Ziegler, T.R. Parenteral nutrition in the critically ill patient. N. Engl. J. Med. 2009, 361, 1088–1097. [Google Scholar] [CrossRef]
- Kumar, P.R.; Crotty, P.; Raman, M. Hyperglycemia in hospitalized patients receiving parental nutrition is associated with increased morbidity and mortality: A review. Gastroenterol. Res. Pract. 2011, 10, 1155. [Google Scholar] [CrossRef]
- Finfer, S.; Chittock, D.R.; Su, S.Y.; Blair, D.; Foster, D.; Dhingra, V.; Bellomo, R.; Cook, D.; Dodek, P.; Henderson, W.R.; et al. Intensive versus conventional glucose control in critically ill patients. New Engl. J. Med. 2009, 360, 1283–1297. [Google Scholar] [CrossRef]
- Buchman, A.L.; Ament, M.E. Comparative hypersensitivity in intravenous lipid emulsions. J. Parenter. Enter. Nutr. 1991, 15, 345–346. [Google Scholar] [CrossRef]
- Market, A.D.; Lew, D.B.; Schropp, K.P.; Hak, E.B. Parenteral nutrition-associated anaphylaxis in a 4-year-old child. J. Pediatr. Gastroenterol. Nutr. 1998, 26, 229–231. [Google Scholar] [CrossRef]
- Christian, V.J.; Tallar, M.; Walia, C.L.S.; Sieracki, R.; Goday, P.S. Systematic Review of Hypersensitivity to Parenteral Nutrition. J. Parenter. Enter. Nutr. 2018, 42, 1222–1229. [Google Scholar] [CrossRef]
- Mehanna, H.M.; Moledina, J.; Travis, J. Refeeding syndrome: What it is, and how to prevent and treat it. BMJ 2008, 336, 1495–1498. [Google Scholar] [CrossRef]
- Boot, R.; Koekkoek, K.W.A.C.; van Zanten, A.R.H. Refeeding syndrome: Relevance for the critically ill patient. Curr. Opin. Crit. Care 2018, 24, 235–240. [Google Scholar] [CrossRef]
- Bonet Saris, A.; Márquez Vácaro, J.A.; Serón Arbeloa, C.; Metabolism and Nutrition Working Group of the Spanish Society of Intensive Care Medicine and Coronary units. Guidelines for specialized nutritional and metabolic support in the critically ill patient: Update. Consensus SEMICYUC-SENPE: Macronutrient and micronutrient requirements. Nutr. Hosp. 2011, 26 (Suppl. S2), 16–20. [Google Scholar] [CrossRef]
- Fernández-Ortega, J.F.; Herrero Meseguer, J.I.; Martínez García, P.; Metabolism and Nutrition Working Group of the Spanish Society of Intensive Care Medicine and Coronary units. Guidelines for specialized nutritional and metabolic support in the critically ill patient: Update. Consensus SEMICYUC-SENPE: Indications, timing and routes of nutrient delivery. Nutr. Hosp. 2011, 26 (Suppl. S2), 7–11. [Google Scholar] [CrossRef]


{kind=link}
| Item | INVASIVE MECHANICAL VENTILATION | CONTINUOUS HAEMODIALYSIS | MEDICAL NUTRITION THERAPY |
|---|---|---|---|
| Indication | Alteration of ventilation Alteration of oxygenation Airway permeability | Uraemia Dyselectrolytaemia Hypervolemia Removing toxins (endogenous and exogenous) Hypothermia | Inadequate nutritional intake |
| Access | Tracheal tube Tracheostomy | Central venous line | Central venous line Enteral tube |
| Adjuvant treatments | Sedation Neuromuscular block Artificial nutrition Physiotherapy | Systemic anticoagulation Circuit heater or thermal blanket | Insulin administration for glycaemic control Physiotherapy |
| AE related to access | Stenosis, Granulomas, Mucosal necrosis | Hemorrhage Thrombosis | Hemorrhage Thrombosis |
| AE related to infections | Ventilator-associated pneumonia | Catheter-related infections | Sinusitis Catheter-related infections |
| AE related to toxicity | Oxygen toxicity | Heparin-induced thrombocytopenia. Citrate-induced hypocalcemia | Chemical phlebitis |
| AE related to the technique | Barotrauma: Lung injury due to positive pressure, overdistention and alveolar break Volutrauma: Lung injury due to local overdistention as a result of using excessive tidal volumes Atelectrauma: Alveolar damage as a result of transient and repeated closure and reopening of alveoli during the respiratory cycle. Biotrauma: Mechanical stress in response to using high tidal volume and inadequate positive end-expiratory pressure (PEEP) leading to a systemic inflammatory response | Dialytrauma: Harmful effects of continuous renal replacement therapy Dyselectrolytaemia: hypokalaemia, hypophosphataemia, hyponatraemia, hypo/hypercalcaemia, alteration of lactate metabolism Loss of endogenous vital nutrients: water-soluble vitamins, antioxidants, carbohydrates, amino acids Incorrect adjustment of drugs Hypothermia Blood loss: secondary to circuit lifespan | Nutritrauma: Over- and underfeeding, Hypervolaemia Uraemia Hypercapnia Hypertriglyceridaemia Refeeding syndrome Dyselectrolytaemia Hyperglycaemia Hepatobiliary disorders: Cholestasis, cholecystitis, cholelithiasis, hepatic steatosis, non-alcoholic fatty liver disease, hepatic fibrosis and cirrhosis Metabolic bone disease Malabsorptive diarrhea |
| Component | Adverse Events | Therapeutic Approach |
|---|---|---|
| Inappropriate dosage | Overfeeding, underfeeding | Adjust calorie and protein administration to inflammatory status and clinical phase, Adjust non-nutritional calorie administration, Minimise interruptions and optimise enteral administration |
| Refeeding syndrome | Depletion of intracellular resources in previously malnourished or fasting patients | Assess nutritional risk and requirements, Restrict calorie intake during the first few days of transitioning back to a normal diet |
| Water | Fluid overload | Adjust prescription to liquid balances |
| Electrolytes | Electrolyte disturbances (K, Mg, P, acid-base disorders) | Periodic laboratory tests |
| Glucose | Hypoglycaemia, hyperglycaemia | Glycaemic control protocol |
| Calorie intake Lipid | Hypertriglyceridaemia, non-alcoholic fatty liver disease | Adjust lipid administration to calorie requirements, periodic laboratory test |
| Protein | Uraemia | Adjust protein prescription to requirements and stress |
| Prolonged use of Parenteral Nutrition | Intestinal failure-associated liver disease, metabolic bone disease | Test enteral tolerance if possible |
| Indicator Name | Nutritrauma Monitoring |
|---|---|
| Area | Safety |
| Justification | Inappropriate dosage of medical nutrition therapy is associated with greater morbidity and mortality in the critically ill patient. Monitoring the components of nutritional support can assist in recovery and improve prognosis |
| Formula | (No. of patients monitored) × 100 ÷ (No. of patients with medical nutritional support) |
| Explanation of terms | Monitoring of nutritrauma includes: An initial assessment of the nutritional status Assessment of calorie and protein requirements Monitoring of the administration of supplemental nutrition Monitoring water balance Monitoring of hypoglycaemia and hyperglycaemia Monitoring the incidence of uraemia not attributable to renal failure Monitoring the incidence of hypolipidaemia and hyperlipidaemia Monitoring the incidence of dyselectrolytaemia Monitoring the incidence of hepatopathy |
| Population | All critically ill patients who receive medical nutritional support |
| Type | Process |
| Data source | Medical records and clinical information systems |
| Standard | 100% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yébenes, J.C.; Campins, L.; Martínez de Lagran, I.; Bordeje, L.; Lorencio, C.; Grau, T.; Montejo, J.C.; Bodí, M.; Serra-Prat, M.; Working Group on Nutrition and Metabolism of the Spanish Society of Critical Care. Nutritrauma: A Key Concept for Minimising the Harmful Effects of the Administration of Medical Nutrition Therapy. Nutrients 2019, 11, 1775. https://doi.org/10.3390/nu11081775
Yébenes JC, Campins L, Martínez de Lagran I, Bordeje L, Lorencio C, Grau T, Montejo JC, Bodí M, Serra-Prat M, Working Group on Nutrition and Metabolism of the Spanish Society of Critical Care. Nutritrauma: A Key Concept for Minimising the Harmful Effects of the Administration of Medical Nutrition Therapy. Nutrients. 2019; 11(8):1775. https://doi.org/10.3390/nu11081775
Chicago/Turabian StyleYébenes, Juan Carlos, Lluis Campins, Itziar Martínez de Lagran, Lluisa Bordeje, Carol Lorencio, Teodoro Grau, Juan Carlos Montejo, Maria Bodí, Mateu Serra-Prat, and Working Group on Nutrition and Metabolism of the Spanish Society of Critical Care. 2019. "Nutritrauma: A Key Concept for Minimising the Harmful Effects of the Administration of Medical Nutrition Therapy" Nutrients 11, no. 8: 1775. https://doi.org/10.3390/nu11081775
APA StyleYébenes, J. C., Campins, L., Martínez de Lagran, I., Bordeje, L., Lorencio, C., Grau, T., Montejo, J. C., Bodí, M., Serra-Prat, M., & Working Group on Nutrition and Metabolism of the Spanish Society of Critical Care. (2019). Nutritrauma: A Key Concept for Minimising the Harmful Effects of the Administration of Medical Nutrition Therapy. Nutrients, 11(8), 1775. https://doi.org/10.3390/nu11081775