Breastfeeding Status and Duration and Infections, Hospitalizations for Infections, and Antibiotic Use in the First Two Years of Life in the ELFE Cohort

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Breastfeeding
2.3. Parental Report of Infections
2.4. Other Variables
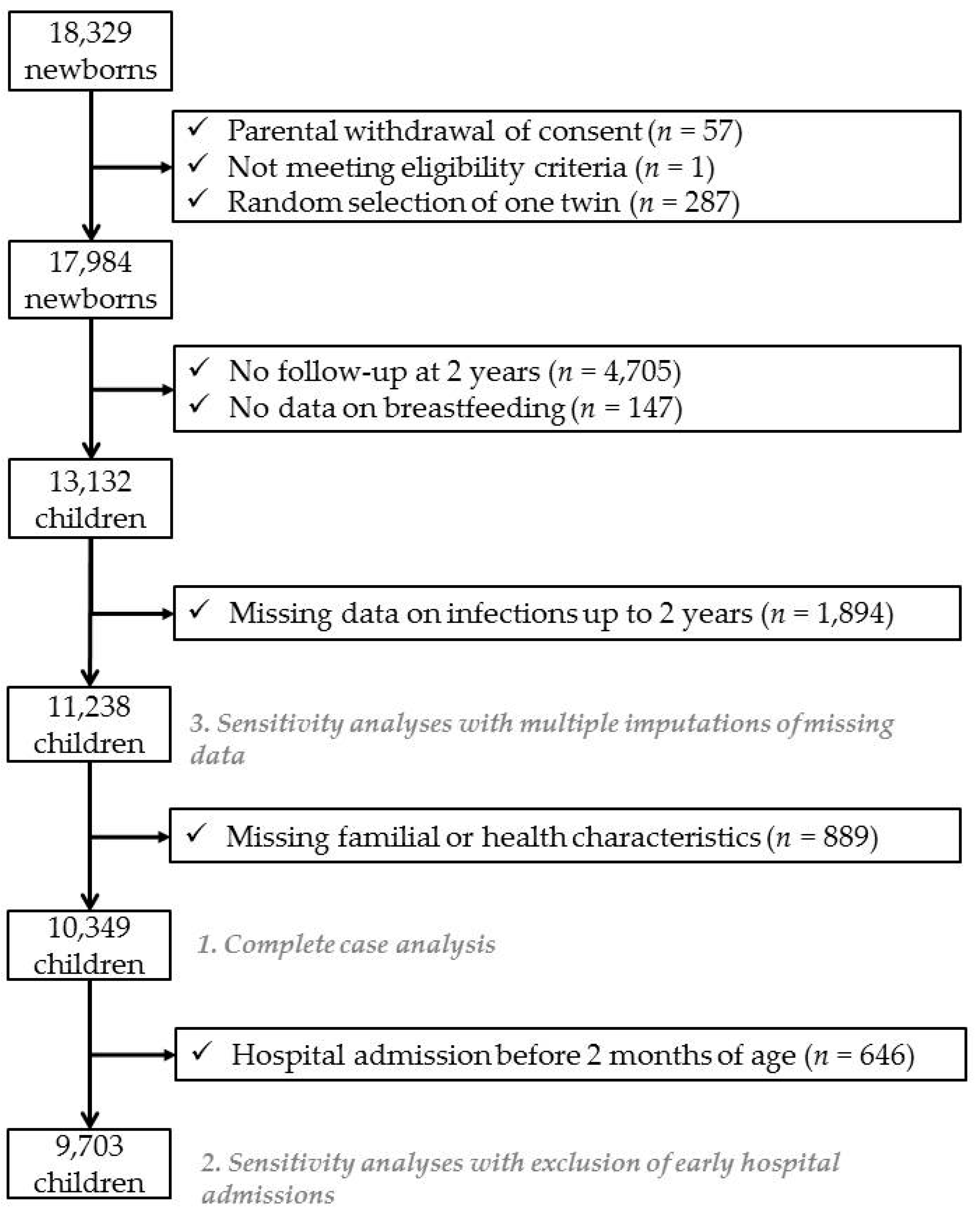
2.5. Sample Selection
2.6. Analyses
2.6.1. Main Analyses
2.6.2. Sensitivity Analyses
3. Results
3.1. Hospitalizations from Infectious Diseases
3.2. Bronchiolitis Events
3.3. Otitis Events
3.4. Antibiotic Use
3.5. Analyses after Multiple Imputations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kyu, H.H.; Pinho, C.; Wagner, J.A.; Brown, J.C.; Bertozzi-Villa, A.; Charlson, F.J.; Coffeng, L.E.; Dandona, L.; Erskine, H.E.; Ferrari, A.J.; et al. Global and National Burden of Diseases and Injuries Among Children and Adolescents Between 1990 and 2013: Findings From the Global Burden of Disease 2013 Study. JAMA Pediatr. 2016, 170, 267–287. [Google Scholar]
- World Health Organization. Feeding and Nutrition of Infants and Young Children, Guidelines for the WHO European Region, with Emphasis on the Former Soviet Countries; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Victora, C.G.; Bahl, R.; Barros, A.J.; Franca, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C.; et al. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef]
- Field, C.J. The immunological components of human milk and their effect on immune development in infants. J. Nutr. 2006, 135, 1–4. [Google Scholar] [CrossRef]
- Korvel-Hanquist, A.; Djurhuus, B.D.; Homoe, P. The Effect of Breastfeeding on Childhood Otitis Media. Curr. Allergy Asthma Rep. 2017, 17, 45. [Google Scholar] [CrossRef]
- Bowatte, G.; Tham, R.; Allen, K.J.; Tan, D.J.; Lau, M.; Dai, X.; Lodge, C.J. Breastfeeding and childhood acute otitis media: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 85–95. [Google Scholar] [CrossRef]
- Horta, B.L.; Victora, C.G. Short-Term Effects of Breastfeeding: A Systematic Review of the Benefits of Breastfeeding on Diarrhoea and Pneumonia Mortality; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Kramer, M.S.; Chalmers, B.; Hodnett, E.D.; Sevkovskaya, Z.; Dzikovich, I.; Shapiro, S.; Collet, J.P.; Vanilovich, I.; Mezen, I.; Ducruet, T.; et al. Promotion of Breastfeeding Intervention Trial (PROBIT). JAMA 2001, 285, 413–420. [Google Scholar] [CrossRef]
- Wagner, S.; Kersuzan, C.; Gojard, S.; Tichit, C.; Nicklaus, S.; Geay, B.; Humeau, P.; Thierry, X.; Charles, M.A.; Lioret, S.; et al. Breastfeeding duration in France according to parents and birth characteristics. Results from the ELFE longitudinal French Study, 2011. Bull. Epidemiol. Hebd. 2015, 29, 522–532. [Google Scholar]
- Vandentorren, S.; Bois, C.; Pirus, C.; Sarter, H.; Salines, G.; Leridon, H.; Elfe, T. Rationales, design and recruitment for the Elfe longitudinal study. BMC Pediatr. 2009, 9, 58. [Google Scholar] [CrossRef]
- Wagner, S.; Kersuzan, C.; Gojard, S.; Tichit, C.; Nicklaus, S.; Thierry, X.; Charles, M.A.; Lioret, S.; De Lauzon-Guillain, B. Breastfeeding initiation and duration in France: The importance of intergenerational and previous maternal breastfeeding experiences—results from the nationwide ELFE study. Midwifery 2019, 69, 67–75. [Google Scholar] [CrossRef]
- Lodge, C.J.; Bowatte, G.; Matheson, M.C.; Dharmage, S.C. The Role of Breastfeeding in Childhood Otitis Media. Curr. Allergy Asthma Rep. 2016, 16, 68. [Google Scholar] [CrossRef]
- Lanari, M.; Prinelli, F.; Adorni, F.; Di Santo, S.; Faldella, G.; Silvestri, M.; Musicco, M. Maternal milk protects infants against bronchiolitis during the first year of life. Results from an Italian cohort of newborns. Early Hum. Dev. 2013, 89, 51–57. [Google Scholar] [CrossRef]
- Tromp, I.; Kiefte-De Jong, J.; Raat, H.; Jaddoe, V.; Franco, O.; Hofman, A.; De Jongste, J.; Moll, H. Breastfeeding and the risk of respiratory tract infections after infancy: The Generation R Study. PLoS ONE 2017, 12, e0172763. [Google Scholar] [CrossRef]
- Stordal, K.; Lundeby, K.M.; Brantsaeter, A.L.; Haugen, M.; Nakstad, B.; Lund-Blix, N.A.; Stene, L.C. Breast-feeding and Infant Hospitalization for Infections: Large Cohort and Sibling Analysis. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 225–231. [Google Scholar] [CrossRef]
- Quigley, M.A.; Kelly, Y.J.; Sacker, A. Breastfeeding and hospitalization for diarrheal and respiratory infection in the United Kingdom Millennium Cohort Study. Pediatrics 2007, 119, e837–e842. [Google Scholar] [CrossRef]
- Kramer, M.S.; Guo, T.; Platt, R.W.; Sevkovskaya, Z.; Dzikovich, I.; Collet, J.P.; Shapiro, S.; Chalmers, B.; Hodnett, E.; Vanilovich, I.; et al. Infant growth and health outcomes associated with 3 compared with 6 mo of exclusive breastfeeding. Am. J. Clin. Nutr. 2003, 78, 291–295. [Google Scholar] [CrossRef]
- Pisacane, A.; Graziano, L.; Zona, G.; Granata, G.; Dolezalova, H.; Cafiero, M.; Coppola, A.; Scarpellino, B.; Ummarino, M.; Mazzarella, G. Breast feeding and acute lower respiratory infection. Acta Paediatr. 1994, 83, 714–718. [Google Scholar] [CrossRef]
- Howie, P.W.; Forsyth, J.S.; Ogston, S.A.; Clark, A.; Florey, C.D. Protective effect of breast feeding against infection. BMJ 1990, 300, 11–16. [Google Scholar] [CrossRef]
- Nenna, R.; Cutrera, R.; Frassanito, A.; Alessandroni, C.; Nicolai, A.; Cangiano, G.; Petrarca, L.; Arima, S.; Caggiano, S.; Ullmann, N.; et al. Modifiable risk factors associated with bronchiolitis. Ther. Adv. Respir. Dis. 2017, 11, 393–401. [Google Scholar] [CrossRef]
- Parizkova, P.; Dankova, N.; Fruhauf, P.; Jireckova, J.; Zeman, J.; Magner, M. Associations between breastfeeding rates and infant disease: A survey of 2338 Czech children. Nutr. Diet. J. Dietit. Assoc. Aust. 2019. [Google Scholar] [CrossRef]
- Korpela, K.; Salonen, A.; Virta, L.J.; Kekkonen, R.A.; De Vos, W.M. Association of Early-Life Antibiotic Use and Protective Effects of Breastfeeding: Role of the Intestinal Microbiota. JAMA Pediatr. 2016, 170, 750–757. [Google Scholar] [CrossRef]
- Krenz-Niedbala, M.; Koscinski, K.; Puch, E.A.; Zelent, A.; Breborowicz, A. Is the Relationship Between Breastfeeding and Childhood Risk of Asthma and Obesity Mediated by Infant Antibiotic Treatment? Breastfeed. Med. 2015, 10, 326–333. [Google Scholar] [CrossRef]


{kind=link}
| Family Characteristics | Breastfeeding Duration | |||||
|---|---|---|---|---|---|---|
| Never (n = 2489) | <1 Month (n = 1704) | 1 to <3 Months (n = 1629) | 3 to <6 Months (n = 1964) | ≥6 Months (n = 2563) | ||
| Maternal age at birth (years) | 30.4 (4.9) | 30.0 (5.0) | 30.4 (4.5) | 30.9 (4.3) | 31.6 (4.6) | |
| Maternal place of birth (France) | 96.6% (2405) | 94.5% (1611) | 92.4% (1505) | 90.3% (1774) | 82.7% (2120) | |
| Pre-pregnancy body mass index (kg/m²) | 23.9 (5.2) | 23.8 (4.9) | 23.4 (4.5) | 22.8 (4.1) | 23.0 (4.3) | |
| Education level | ||||||
| Below secondary school | 7.2% (178) | 5.4% (92) | 3.8% (62) | 3.6% (71) | 5.1% (131) | |
| Secondary school | 17.2% (428) | 15.8% (269) | 9.7% (158) | 7.3% (143) | 7.9% (202) | |
| High school | 21.6% (537) | 21.4% (365) | 18.4% (300) | 15.1% (297) | 13.7% (352) | |
| 2-year university degree | 24.5% (611) | 25.5% (434) | 26.2% (427) | 23.7% (465) | 21.2% (543) | |
| 3-year university degree | 15.8% (394) | 18.2% (310) | 19.6% (320) | 22.3% (437) | 22.8% (584) | |
| 5-year university degree or higher | 13.7% (341) | 13.7% (234) | 22.2% (362) | 28.1% (551) | 29.3% (751) | |
| Employed before pregnancy | 77.9% (1938) | 75% (1278) | 79.7% (1299) | 80.2% (1576) | 71.4% (1829) | |
| Traditional household composition | 87.9% (2188) | 87.9% (1498) | 91.3% (1487) | 91.6% (1799) | 90.2% (2311) | |
| Household monthly income (€) | 3379 (3171) | 3276 (2750) | 3665 (4608) | 3738 (3671) | 3506 (2663) | |
| Smoking status during pregnancy | ||||||
| Never smoker | 51.9% (1292) | 50.1% (853) | 57.5% (936) | 60.7% (1193) | 66.1% (1694) | |
| Only before pregnancy | 24% (598) | 27.4% (467) | 25.9% (422) | 25.1% (492) | 23.6% (604) | |
| Only in early pregnancy | 3.5% (88) | 4.7% (80) | 3.4% (56) | 3.8% (74) | 2.9% (75) | |
| Throughout pregnancy | 20.5% (511) | 17.8% (304) | 13.2% (215) | 10.4% (205) | 7.4% (190) | |
| Caesarean section | 19.2% (478) | 18% (307) | 18% (294) | 15.7% (309) | 15.2% (389) | |
| Gestational age (weeks) | 39.5 (1.5) | 39.7 (1.4) | 39.7 (1.4) | 39.7 (1.4) | 39.7 (1.4) | |
| Boys | 48.8% (1215) | 49.4% (841) | 51.6% (841) | 50.1% (984) | 48.7% (1249) | |
| First born | 42.9% (1069) | 50.5% (861) | 49.7% (809) | 45.7% (897) | 37.6% (963) | |
| Age at first attendance at a shared childcare facility | ||||||
| ≤2 months | 55.7% (1386) | 54.2% (924) | 48.4% (788) | 46.4% (912) | 61.6% (1580) | |
| >2 months to 4 months | 7.4% (183) | 5.8% (99) | 8% (130) | 3.6% (70) | 2.1% (53) | |
| >4 months to 6 months | 18.8% (469) | 20.4% (347) | 26.3% (429) | 24.3% (477) | 11.2% (286) | |
| >6 months to 12 months | 9.1% (227) | 9.2% (157) | 8.2% (133) | 13.7% (269) | 10.7% (273) | |
| Never attended in the first year | 9% (224) | 10.4% (177) | 9.1% (149) | 12% (236) | 14.5% (371) | |
| % (n) or mean (± SD) | ||||||
| Breastfeeding Status and Duration | Parental Report of Hospitalizations from Infection | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of Events (Ref = None) | Total Duration (Ref = Never) | Causes | |||||||||||
| 1 | ≥2 | p | 1–3 Nights | ≥4 Nights | p | Fever | p | Gastroint. Inf. | p | Bronchiolitis | p | ||
| Number of infants in each group | 842 | 413 | 470 | 429 | 282 | 397 | 475 | ||||||
| Any breastfeeding status | 0.52 | 0.33 | 0.11 | 0.40 | 0.98 | ||||||||
| Never | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | ||||||
| Ever | 1.10 (0.93; 1.31) | 1.04 (0.82; 1.32) | 1.16 (0.92; 1.46) | 0.92 (0.73; 1.16) | 1.28 (0.95; 1.74) | 1.11 (0.87; 1.42) | 1.00 (0.80; 1.24) | ||||||
| Any breastfeeding duration | 0.29 | 0.25 | 0.17 | 0.08 | 0.10 | ||||||||
| Never | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | ||||||
| <1 month | 1.13 (0.90; 1.42) | 1.20 (0.89; 1.62) | 1.21 (0.90; 1.63) | 1.02 (0.76; 1.38) | 1.38 (0.94; 2.02) | 1.42 (1.05; 1.91) | 0.92 (0.68; 1.24) | ||||||
| 1 to <3 months | 1.22 (0.97; 1.53) | 1.15 (0.84; 1.58) | 1.17 (0.86; 1.60) | 1.08 (0.79; 1.46) | 1.55 (1.06; 2.28) | 0.91 (0.64; 1.29) | 1.24 (0.93; 1.65) | ||||||
| 3 to <6 months | 1.13 (0.91; 1.42) | 0.94 (0.68; 1.29) | 1.28 (0.96; 1.71) | 0.85 (0.63; 1.17) | 1.13 (0.76; 1.68) | 1.03 (0.75; 1.43) | 1.07 (0.80; 1.42) | ||||||
| ≥6 months | 0.96 (0.77; 1.20) | 0.89 (0.65; 1.21) | 1.00 (0.74; 1.34) | 0.77 (0.57; 1.04) | 1.13 (0.78; 1.65) | 1.04 (0.76; 1.42) | 0.82 (0.62; 1.10) | ||||||
| Number of infants in each group | 839 | 413 | 468 | 428 | 281 | 395 | 474 | ||||||
| Predominant breastfeeding status | 0.42 | 0.27 | 0.65 | 0.73 | 0.59 | ||||||||
| Never | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | ||||||
| Ever | 1.10 (0.94; 1.29) | 0.96 (0.77; 1.19) | 1.12 (0.91; 1.39) | 0.88 (0.72; 1.09) | 1.06 (0.82; 1.39) | 1.04 (0.83; 1.30) | 1.06 (0.86; 1.30) | ||||||
| Predominant breastfeeding duration | 0.24 | 0.08 | 0.25 | 0.14 | 0.24 | ||||||||
| Never | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | ||||||
| <1 month | 1.24 (1.01; 1.52) | 1.09 (0.82; 1.44) | 1.27 (0.97; 1.65) | 1.07 (0.81; 1.40) | 1.13 (0.80; 1.59) | 1.28 (0.97; 1.68) | 1.25 (0.96; 1.62) | ||||||
| 1 to <3 months | 1.13 (0.92; 1.39) | 0.99 (0.74; 1.32) | 1.05 (0.79; 1.38) | 1.00 (0.76; 1.31) | 1.28 (0.92; 1.79) | 1.02 (0.76; 1.37) | 1.04 (0.79; 1.37) | ||||||
| 3 to <6 months | 1.02 (0.82; 1.27) | 0.79 (0.57; 1.08) | 1.08 (0.81; 1.44) | 0.67 (0.49; 0.93) | 0.85 (0.58; 1.24) | 0.84 (0.61; 1.17) | 1.00 (0.75; 1.32) | ||||||
| ≥6 months | 0.90 (0.68; 1.19) | 0.92 (0.63; 1.34) | 1.05 (0.74; 1.50) | 0.67 (0.45; 1.00) | 0.88 (0.56; 1.40) | 0.89 (0.60; 1.34) | 0.81 [0.56; 1.18) | ||||||
| Breastfeeding Status and Duration | Parental Report | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Bronchiolitis Events (Ref = None) | Otitis Events (Ref ≤ 3) | Antibiotic Use (Ref = Never) | ||||||||
| 1 or 2 | ≥3 | p | ≥3 | p | Once | 2 or 3 Times | >3 Times | p | ||
| Number of infants in each group | 6340 | 1264 | 2606 | 1944 | 1860 | 4411 | ||||
| Any breastfeeding status | 0.17 | 0.32 | 0.02 | |||||||
| Never | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | ||||
| Ever | 1.11 (0.99; 1.24) | 1.09 (0.92; 1.28) | 1.06 (0.95; 1.18) | 0.94 (0.80; 1.09) | 0.84 (0.72; 0.98) | 0.83 (0.73; 0.94) | ||||
| Any breastfeeding duration | 0.05 | 0.37 | 0.00 | |||||||
| Never | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | ||||
| <1 month | 1.07 (0.93; 1.24) | 1.19 (0.96; 1.48) | 1.08 (0.94; 1.25) | 0.99 (0.80; 1.22) | 1.02 (0.83; 1.26) | 1.09 (0.92; 1.30) | ||||
| 1 to <3 months | 1.09 (0.94; 1.26) | 1.08 (0.87; 1.35) | 1.12 (0.97; 1.29) | 1.04 (0.84; 1.28) | 0.95 (0.77; 1.18) | 0.98 (0.82; 1.17) | ||||
| 3 to <6 months | 1.15 (1.00; 1.33) | 1.20 (0.97; 1.48) | 1.06 (0.92; 1.22) | 1.00 (0.82; 1.22) | 0.78 (0.64; 0.95) | 0.79 (0.67; 0.94) | ||||
| ≥6 months | 1.12 (0.98; 1.29) | 0.90 (0.73; 1.12) | 0.98 (0.86; 1.13) | 0.79 (0.66; 0.95) | 0.71 (0.59; 0.85) | 0.61 (0.52; 0.71) | ||||
| Number of infants in each group | 6335 | 1263 | 2605 | 1940 | 1857 | 4410 | ||||
| Predominant breastfeeding status | 0.30 | 0.92 | 0.00 | |||||||
| Never | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | ||||
| Ever | 1.08 (0.98; 1.19) | 1.04 (0.90; 1.21) | 0.99 (0.90; 1.10) | 0.96 (0.83; 1.10) | 0.84 (0.73; 0.96) | 0.79 (0.71; 0.89) | ||||
| Predominant breastfeeding duration | 0.06 | 0.98 | 0.00 | |||||||
| Never | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | ||||
| <1 month | 1.09 (0.95; 1.24) | 1.19 (0.98; 1.45) | 1.02 (0.89; 1.16) | 1.11 (0.92; 1.33) | 1.05 (0.87; 1.26) | 0.97 (0.83; 1.14) | ||||
| 1 to <3 months | 1.13 (0.99; 1.30) | 1.08 (0.89; 1.32) | 1.01 (0.88; 1.15) | 0.95 (0.79; 1.14) | 0.82 (0.68; 0.99) | 0.87 (0.74; 1.01) | ||||
| 3 to <6 months | 1.10 (0.96; 1.270) | 0.99 (0.81; 1.22) | 0.97 (0.85; 1.11) | 0.88 (0.73; 1.06) | 0.71 (0.59; 0.85) | 0.65 (0.56; 0.76) | ||||
| ≥6 months | 0.94 (0.80; 1.110) | 0.77 (0.59; 1.00) | 0.97 (0.82; 1.15) | 0.89 (0.71; 1.10) | 0.75 (0.60; 0.93) | 0.62 (0.51; 0.75) | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davisse-Paturet, C.; Adel-Patient, K.; Divaret-Chauveau, A.; Pierson, J.; Lioret, S.; Cheminat, M.; Dufourg, M.-N.; Charles, M.-A.; de Lauzon-Guillain, B. Breastfeeding Status and Duration and Infections, Hospitalizations for Infections, and Antibiotic Use in the First Two Years of Life in the ELFE Cohort. Nutrients 2019, 11, 1607. https://doi.org/10.3390/nu11071607
Davisse-Paturet C, Adel-Patient K, Divaret-Chauveau A, Pierson J, Lioret S, Cheminat M, Dufourg M-N, Charles M-A, de Lauzon-Guillain B. Breastfeeding Status and Duration and Infections, Hospitalizations for Infections, and Antibiotic Use in the First Two Years of Life in the ELFE Cohort. Nutrients. 2019; 11(7):1607. https://doi.org/10.3390/nu11071607
Chicago/Turabian StyleDavisse-Paturet, Camille, Karine Adel-Patient, Amandine Divaret-Chauveau, Juliette Pierson, Sandrine Lioret, Marie Cheminat, Marie-Noëlle Dufourg, Marie-Aline Charles, and Blandine de Lauzon-Guillain. 2019. "Breastfeeding Status and Duration and Infections, Hospitalizations for Infections, and Antibiotic Use in the First Two Years of Life in the ELFE Cohort" Nutrients 11, no. 7: 1607. https://doi.org/10.3390/nu11071607
APA StyleDavisse-Paturet, C., Adel-Patient, K., Divaret-Chauveau, A., Pierson, J., Lioret, S., Cheminat, M., Dufourg, M.-N., Charles, M.-A., & de Lauzon-Guillain, B. (2019). Breastfeeding Status and Duration and Infections, Hospitalizations for Infections, and Antibiotic Use in the First Two Years of Life in the ELFE Cohort. Nutrients, 11(7), 1607. https://doi.org/10.3390/nu11071607