Dairy Food Consumption is Inversely Associated with the Prevalence of Periodontal Disease in Korean Adults


Abstract
1. Introduction
2. Materials and Methods
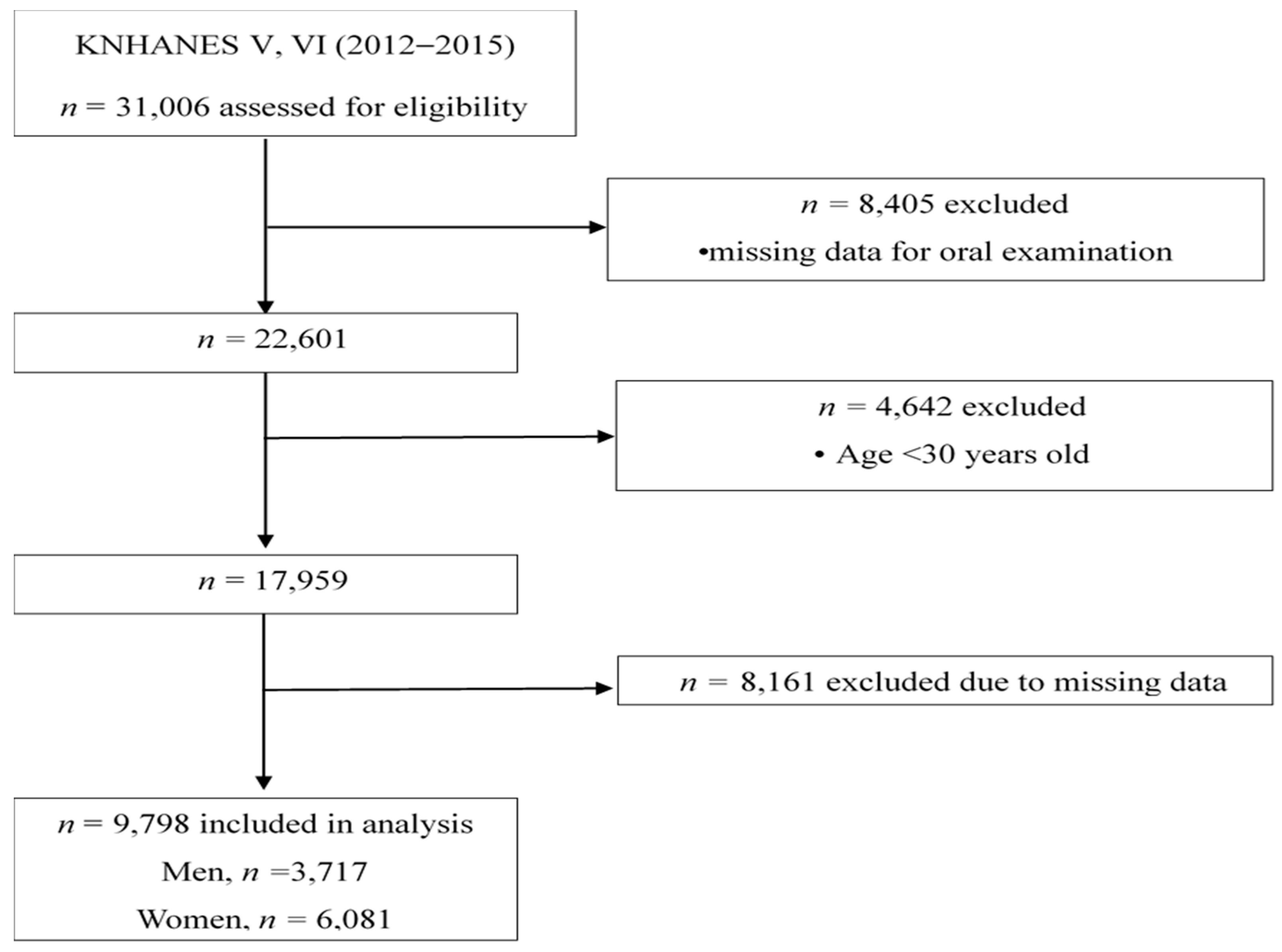
2.1. Study Population
2.2. Definition of Periodontal Disease
2.3. Dietary Assessment
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Subjects
3.2. Characteristics of Subjects According to Dairy Food Consumption
3.3. Association of Dairy Food Consumption with Periodontal Disease
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89, S159–S172. [Google Scholar] [CrossRef]
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef]
- Korea Centers for Disease Control and Prevention. Korea Health Statistics 2015: Korea National Health and Nutrition Examination Survey (KNHANES VI-3); Korea Centers for Disease Control and Prevention: Cheongwon, Korea, 2016.
- Al-Zahrani, M.S.; Bissada, N.F.; Borawski, E.A. Diet and periodontitis. J. Int. Acad. Periodontol. 2005, 7, 21–26. [Google Scholar]
- Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Zohaib, S.; Almas, K. The Role of Nutrition in Periodontal Health: An Update. Nutrients 2016, 8, 530. [Google Scholar] [CrossRef]
- Schifferle, R.E. Nutrition and Periodontal Disease. Dent. Clin. N. Am. 2005, 49, 595–610. [Google Scholar] [CrossRef]
- Park, Y.W. Bioactive Components in Milk and Dairy Products; John Wiley & Sons: Hoboken, NJ, USA, 2009. [Google Scholar]
- Al-Zahrani, M.S. Increased intake of dairy products is related to lower periodontitis prevalence. J. Periodontol. 2006, 77, 289–294. [Google Scholar] [CrossRef]
- Shimazaki, Y.; Shirota, T.; Uchida, K.; Yonemoto, K.; Kiyohara, Y.; Iida, M.; Saito, T.; Yamashita, Y. Intake of dairy products and periodontal disease: The Hisayama Study. J. Periodontol. 2008, 79, 131–137. [Google Scholar] [CrossRef]
- Adegboye, A.R.; Christensen, L.B.; Holm-Pedersen, P.; Avlund, K.; Boucher, B.J.; Heitmann, B.L. Intake of dairy products in relation to periodontitis in older Danish adults. Nutrients 2012, 4, 1219–1229. [Google Scholar] [CrossRef]
- Rizzoli, R. Dairy products, yogurts, and bone health. Am. J. Clin. Nutr. 2014, 99, 1256S–1262S. [Google Scholar] [CrossRef]
- Nishida, M. Calcium and the risk for periodontal disease. Clin. Calcium 2003, 13, 618–622. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare; Korea Centers for Disease Control and Prevention. The Fifth Korea National Health and Nutrition Examination Survey (KNHANES V-3), 2012; Korea Centers for Disease Control and Prevention: Cheongwon, Korea, 2013.
- Ministry of Health and Welfare; Korea Centers for Disease Control and Prevention. The Sixth Korea National Health and Nutrition Examination Survey (KNHANES Ⅵ), 2013-2015; Korea Centers for Disease Control and Prevention: Cheongwon, Korea, 2016.
- Ministry of Health and Welfare; Korea Centers for Disease Control and Prevention. The 5th National Health and Nutrition Examination Guidebook 2010–2012; Korea Centers for Disease Control and Prevention: Cheongwon, Korea, 2013.
- World Health Organization. Oral Health Surveys: Basic Methods, 4th ed.; World Health Organization (WHO): Geneva, Switzerland, 1997. [Google Scholar]
- Inagaki, K.; Kurosu, Y.; Yoshinari, N.; Noguchi, T.; Krall, E.A.; Garcia, R.I. Efficacy of Periodontal Disease and Tooth Loss to Screen for Low Bone Mineral Density in Japanese Women. Calcif. Tissue Int. 2005, 77, 9–14. [Google Scholar] [CrossRef]
- Shim, J.S.; Oh, K.W.; Suh, I.; Kim, M.Y.; Sohn, C.Y.; Lee, E.J.; Nam, C.M. A study on validity of a semi-quantitative food frequency questionnaire for Korean adults. Korean J. Community Nutr. 2002, 7, 484–494. [Google Scholar]
- The Korean Nutrition Society. Dietary Reference Intake for Korean 2015; The Korean Nutrition Society: Seoul, Korea, 2016. [Google Scholar]
- National Institute of Agricultural Sciences. Food Composition Table 8th Revision; Rural Development Administration: Suwon, Korea, 2011.
- Thomas, S.L.; Heck, R.H. Analysis of large-scale secondary data in higher education research: Potential perils associated with complex sampling designs. Res. High. Educ. 2001, 42, 517–540. [Google Scholar] [CrossRef]
- Lang, N.P.; Lindhe, J. Clinical Periodontology and Implant Dentistry, 2 Volume Set; John Wiley & Sons: Hoboken, NJ, USA, 2015. [Google Scholar]
- Intini, G.; Katsuragi, Y.; Kirkwood, K.L.; Yang, S. Alveolar Bone Loss: Mechanisms, Potential Therapeutic Targets, and Interventions. Adv. Dent. Res. 2014, 26, 38–46. [Google Scholar] [CrossRef]
- Zhu, K.; Prince, R.L. Calcium and bone. Clin. Biochem. 2012, 45, 936–942. [Google Scholar] [CrossRef]
- Perayil, J.; Menon, K.S.; Kurup, S.; Thomas, A.E.; Fenol, A.; Vyloppillil, R.; Bhaskar, A.; Megha, S. Influence of Vitamin D & Calcium Supplementation in the Management of Periodontitis. J. Clin. Diagn. Res. 2015, 9, ZC35–ZC38. [Google Scholar] [CrossRef]
- Kato, K.; Toba, Y.; Matsuyama, H.; Yamamura, J.I.; Matsuoka, Y.; Kawakami, H.; Itabashi, A.; Kumegawa, M.; Aoe, S.; Takada, Y. Milk basic protein enhances the bone strength in ovariectomized rats. J. Food Biochem. 2000, 24, 467–476. [Google Scholar] [CrossRef]
- Seto, H.; Toba, Y.; Takada, Y.; Kawakami, H.; Ohba, H.; Hama, H.; Horibe, M.; Nagata, T. Milk basic protein increases alveolar bone formation in rat experimental periodontitis. J. Periodontal Res. 2007, 42, 85–89. [Google Scholar] [CrossRef]
- Morita, Y.; Ishikawa, K.; Nakano, M.; Wakabayashi, H.; Yamauchi, K.; Abe, F.; Ooka, T.; Hironaka, S. Effects of lactoferrin and lactoperoxidase-containing food on the oral hygiene status of older individuals: A randomized, double blinded, placebo-controlled clinical trial. Geriatr. Gerontol. Int. 2017, 17, 714–721. [Google Scholar] [CrossRef]
- Sookkhee, S.; Chulasiri, M.; Prachyabrued, W. Lactic acid bacteria from healthy oral cavity of Thai volunteers: Inhibition of oral pathogens. J. Appl. Microbiol. 2001, 90, 172–179. [Google Scholar] [CrossRef]
- Haukioja, A. Probiotics and oral health. Eur. J. Dent. 2010, 4, 348. [Google Scholar]
- Fisberg, M.; Machado, R. History of yogurt and current patterns of consumption. Nutr. Rev. 2015, 73, 4–7. [Google Scholar] [CrossRef]
- Korea Centers for Disease Control and Prevention. Korea Health Statistics 2014: Korea National Health and Nutrition Examination Survey (KNHANES VI-2); Korea Centers for Disease Control and Prevention: Cheongwon, Korea, 2015.


{kind=link}
| Characteristics | Periodontal Disease (n = 2771) | Normal (n = 7027) | p Value |
|---|---|---|---|
| Age (years) | 49.4 ± 0.2 | 44.3 ± 0.2 | <0.001 |
| Sex | <0.001 | ||
| Men | 1397 (60.9) | 2320 (44.3) | |
| Women | 1374 (39.1) | 4707 (55.7) | |
| Education level (%) | <0.001 | ||
| ≤6 years | 549 (15.2) | 703 (7.6) | |
| 7–12 years | 1444 (53.7) | 3188 (45.3) | |
| >12 years | 778 (31.1) | 3136 (47.1) | |
| Income level (%) | <0.001 | ||
| Low | 749 (27.3) | 1517 (22.3) | |
| Middle | 1395 (50.4) | 3580 (50.8) | |
| High | 627 (22.3) | 1930 (26.8) | |
| Smoking status (%) | <0.001 | ||
| Non-smokers | 1397 (41.9) | 4798 (60.1) | |
| Former smokers | 606 (24.0) | 1162 (19.6) | |
| Current smokers | 768 (34.1) | 1067 (20.2) | |
| Alcohol consumption (%) | <0.001 | ||
| Never | 725 (22.2) | 1777 (22.0) | |
| <2 times/week | 1333 (48.2) | 3940 (55.8) | |
| ≥2 times/week | 713 (29.7) | 1310 (22.3) | |
| Body mass index (kg/m2) | 24.6 ± 0.1 | 23.8 ± 0.1 | <0.001 |
| Diabetes mellitus (%) | 409 (14.3) | 425 (5.5) | <0.001 |
| Tooth brushing frequency (%) | |||
| <3 times/day | 1445 (52.1) | 2903 (42.0) | |
| ≥3 times/day | 1326 (47.9) | 4124 (58.0) | |
| Use of dental floss (%) | 436 (9.8) | 1151 (17.9) | <0.001 |
| Total dairy intake 2 (servings/week) | 3.7 ± 0.1 | 4.7 ± 0.1 | <0.001 |
| Milk intake (servings/week) 2 | 2.0 ± 0.1 | 2.7 ± 0.1 | <0.001 |
| Yogurt intake (servings/week) | 1.7 ± 0.1 | 2.0 ± 0.1 | <0.001 |
| Calcium intake (mg/day) | 532.2 ± 7.4 | 528.7 ± 5.2 | 0.683 |
| Total Dairy Food Consumption (Servings/Week) | ||||||
|---|---|---|---|---|---|---|
| Characteristics | Never | 0–≤1 | 1<–≤3 | 3<–<7 | ≥7 | p Value |
| No. of subjects | 1439 | 1799 | 1930 | 2058 | 2572 | |
| Normal (%) | 901 (61.4) | 1238 (68.4) | 1404 (72.8) | 1522 (73.7) | 1962 (76.7) | <0.001 |
| Mild periodontal disease (%) | 522 (37.5) | 547 (30.6) | 513 (26.4) | 523 (25.5) | 596 (22.8) | |
| Severe periodontal disease (%) | 16 (1.1) | 14 (1.0) | 13 (0.9) | 13 (0.8) | 14 (0.5) | |
| Age (years) | 48.9 ± 0.3 | 46.6 ± 0.3 | 45.0 ± 0.2 | 44.5 ± 0.3 | 45.0 ± 0.2 | <0.001 |
| Sex (%) | <0.001 | |||||
| Men | 654 (55.4) | 736 (51.7) | 765 (51.5) | 762 (48.4) | 800 (41.9) | |
| Women | 785 (44.6) | 1063 (48.3) | 1165 (48.5) | 1296 (51.6) | 1772 (58.1) | |
| Education level (%) | <0.001 | |||||
| ≤6 years | 345 (18.6) | 284 (12.3) | 201 (8.3) | 186 (6.5) | 236 (6.8) | |
| 7–12 years | 703 (51.8) | 905 (50.8) | 880 (44.5) | 934 (45.7) | 1210 (47.2) | |
| >12 years | 391 (29.6) | 610 (36.9) | 849 (47.2) | 938 (47.9) | 1126 (46) | |
| Income level (%) | <0.001 | |||||
| Low | 417 (30.2) | 487 (27.9) | 439 (22.7) | 428 (21.2) | 495 (20) | |
| Middle | 718 (49.6) | 918 (50.8) | 1005 (51.6) | 1092 (53) | 1242 (48.7) | |
| High | 304 (20.3) | 394 (21.3) | 486 (25.7) | 538 (25.8) | 835 (31.3) | |
| Smoking status (%) | <0.001 | |||||
| Never | 783 (45.8) | 1090 (51.9) | 1201 (54.1) | 1341 (57) | 1780 (61.2) | |
| Former | 310 (24) | 357 (22.7) | 348 (20.9) | 339 (18.9) | 414 (19.4) | |
| Current | 346 (30.2) | 352 (25.3) | 381 (25) | 378 (24.1) | 378 (19.3) | |
| Alcohol consumption (%) | <0.001 | |||||
| Never | 401 (23.5) | 466 (22.3) | 444 (19.6) | 524 (22.6) | 667 (22.4) | |
| <2 times/week | 642 (45.4) | 931 (52) | 1081 (55.4) | 1122 (53.5) | 1497 (58) | |
| ≥2 times/week | 396 (31.2) | 402 (25.7) | 405 (24.9) | 412 (23.9) | 408 (19.6) | |
| Body mass index (kg/m2) | 24.3 ± 0.1 | 24.1 ± 0.1 | 23.9 ± 0.1 | 24.0 ± 0.1 | 23.8 ± 0.1 | 0.016 |
| Diabetes mellitus (%) | 188 (12.2) | 172 (8.6) | 160 (8.1) | 132 (6.1) | 182 (6.7) | <0.001 |
| Tooth brushing frequency (%) | <0.001 | |||||
| <3 times/day | 769 (51.6) | 897 (50.8) | 855 (45.4) | 881 (44.2) | 946 (36.8) | |
| ≥3 times/day | 670 (48.4) | 902 (49.2) | 1075 (54.6) | 1177 (55.8) | 1626 (63.2) | |
| Use of dental floss (%) | 227 (15.8) | 421 (23.3) | 541 (26.8) | 611 (29.1) | 771 (30.6) | <0.001 |
| Calcium intake (mg/day) | 460.8 ± 9.5 | 467.0 ± 9.7 | 498.2 ± 7.7 | 538.5 ± 7.7 | 632.2 ± 9.8 | <0.001 |
| Milk Consumption (Servings/Week) | ||||||
|---|---|---|---|---|---|---|
| Characteristics | Never | ≤1 | 1<–≤3 | 3<–< 7 | ≥7 | p Value |
| No. of subjects | 2949 | 2623 | 1885 | 793 | 1548 | |
| Normal (%) | 1953 (65.3) | 1863 (70.8) | 1421 (74.7) | 595 (75.5) | 1195 (78.4) | 0.001 |
| Mild periodontal disease (%) | 968 (33.5) | 743 (28.4) | 459 (25.0) | 189 (25.0) | 342 (22.8) | |
| Severe periodontal disease (%) | 28 (1.2) | 17 (0.8) | 5 (0.3) | 9 (1.3) | 11 (0.7) | |
| Age (years) | 48.4 ± 0.2 | 45.6 ± 0.2 | 44.7 ± 0.3 | 43.1 ± 0.4 | 43.8 ± 0.3 | <0.001 |
| Sex (%) | <0.001 | |||||
| Men | 1194 (50.5) | 1070 (52.5) | 643 (45.5) | 348 (55.5) | 462 (40.6) | |
| Women | 1755 (49.5) | 1553 (47.5) | 1242 (54.5) | 445 (44.5) | 1086 (59.4) | |
| Education level (%) | <0.001 | |||||
| ≤6 years | 592 (15.5) | 292 (8.8) | 159 (6.6) | 66 (5.9) | 143 (6.8) | |
| 7–12 years | 1446 (51) | 1283 (48.2) | 857 (45.4) | 359 (45) | 687 (44.6) | |
| >12 years | 911 (33.6) | 1048 (43) | 869 (48) | 368 (49.1) | 718 (48.6) | |
| Income level (%) | <0.001 | |||||
| Low | 790 (27.5) | 622 (24.4) | 382 (20.2) | 167 (22.2) | 305 (20.6) | |
| Middle | 1438 (48.5) | 1359 (51.5) | 1006 (53.8) | 419 (52.3) | 753 (48.9) | |
| High | 721 (24) | 642 (24.1) | 497 (26) | 207 (25.6) | 490 (30.4) | |
| Smoking status (%) | <0.001 | |||||
| Never | 1789 (52.3) | 1600 (52) | 1281 (60.6) | 475 (52) | 1050 (59.6) | |
| Former | 574 (21.9) | 494 (22) | 302 (19.4) | 147 (19.9) | 251 (19.5) | |
| Current | 586 (25.8) | 529 (26) | 302 (20) | 171 (28.1) | 247 (20.9) | |
| Alcohol consumption (%) | <0.001 | |||||
| Never | 850 (24.7) | 630 (20.5) | 428 (20.1) | 194 (21.1) | 400 (22.5) | |
| <2 times/week | 1403 (48.1) | 1436 (54.1) | 1095 (56.9) | 432 (54.7) | 907 (58.4) | |
| ≥2 times/week | 696 (27.2) | 557 (25.4) | 362 (23) | 167 (24.2) | 241 (19.1) | |
| Body mass index (kg/m2) | 24.0 ± 0.1 | 24.0 ± 0.1 | 24.1 ± 0.1 | 24.0 ± 0.1 | 23.8 ± 0.1 | 0.501 |
| Diabetes mellitus (%) | 305 (9.6) | 224 (8.5) | 138 (7.1) | 50 (4.9) | 117 (6.8) | 0.001 |
| Tooth brushing frequency (%) | <0.001 | |||||
| <3 times/day | 1454 (49) | 1243 (47.8) | 754 (41.6) | 332 (43) | 565 (36.9) | |
| ≥3 times/day | 1495 (51) | 1380 (52.2) | 1131 (58.4) | 461 (57) | 983 (63.1) | |
| Use of dental floss (%) | 628 (21.8) | 661 (23.7) | 598 (31.3) | 220 (28) | 464 (30.2) | <0.001 |
| Calcium intake (mg/day) | 474.0 ± 7.1 | 487.6 ± 7.4 | 536.1 ± 8.2 | 600.1 ± 12.9 | 661.7 ± 12.2 | <0.001 |
| Dairy Food Consumption (Servings/Week) | ||||||
|---|---|---|---|---|---|---|
| Total dairy | Never | ≤1 | 1<–≤3 | 3<–<7 | ≥7 | p for trend |
| No. of subjects (No. of cases) | 1439 (538) | 1799 (561) | 1930 (526) | 2058 (536) | 2572 (610) | |
| Model 1 | 1.00 | 0.73 (0.62–0.87) | 0.59 (0.50–0.70) | 0.57 (0.48–0.67) | 0.48 (0.41–0.57) | <0.001 |
| Model 2 | 1.00 | 0.85 (0.70–1.02) | 0.75 (0.63–0.89) | 0.75 (0.63–0.90) | 0.64 (0.54–0.77) | <0.001 |
| Model 3 | 1.00 | 0.91 (0.76–1.10) | 0.84 (0.70–1.01) | 0.87 (0.73–1.04) | 0.76 (0.63–0.91) | 0.052 |
| Milk | Never | ≤1 | 1<–≤3 | 3<–<7 | ≥7 | p for trend |
| No. of subjects (No. of cases) | 2949 (996) | 2623 (760) | 1885 (464) | 793 (198) | 1548 (353) | |
| Model 1 | 1.00 | 0.78 (0.68–0.88) | 0.64 (0.55–0.74) | 0.61 (0.50–0.74) | 0.52 (0.44–0.62) | <0.001 |
| Model 2 | 1.00 | 0.89 (0.77–1.02) | 0.80 (0.69–0.94) | 0.78 (0.64–0.96) | 0.71 (0.59–0.85) | <0.001 |
| Model 3 | 1.00 | 0.90 (0.78–1.04) | 0.88 (0.75–1.03) | 0.82 (0.67–1.02) | 0.74 (0.61–0.89) | 0.022 |
| Yogurt | Never | ≤1 | 1<–≤3 | 3<–<7 | ≥7 | p for trend |
| No. of subjects (No. of cases) | 3307 (1099) | 2617 (693) | 1871 (483) | 1155 (285) | 848 (211) | |
| Model 1 | 1.00 | 0.70 (0.61–0.81) | 0.65 (0.56–0.76) | 0.64 (0.53–0.77) | 0.65 (0.53–0.80) | <0.001 |
| Model 2 | 1.00 | 0.78 (0.68–0.91) | 0.80 (0.69–0.93) | 0.72 (0.59–0.88) | 0.68 (0.55–0.84) | <0.001 |
| Model 3 | 1.00 | 0.87 (0.74–1.01) | 0.92 (0.79–1.08) | 0.83 (0.67–1.01) | 0.83 (0.67–1.05) | 0.188 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.; Kim, J. Dairy Food Consumption is Inversely Associated with the Prevalence of Periodontal Disease in Korean Adults. Nutrients 2019, 11, 1035. https://doi.org/10.3390/nu11051035
Lee K, Kim J. Dairy Food Consumption is Inversely Associated with the Prevalence of Periodontal Disease in Korean Adults. Nutrients. 2019; 11(5):1035. https://doi.org/10.3390/nu11051035
Chicago/Turabian StyleLee, Kyueun, and Jihye Kim. 2019. "Dairy Food Consumption is Inversely Associated with the Prevalence of Periodontal Disease in Korean Adults" Nutrients 11, no. 5: 1035. https://doi.org/10.3390/nu11051035
APA StyleLee, K., & Kim, J. (2019). Dairy Food Consumption is Inversely Associated with the Prevalence of Periodontal Disease in Korean Adults. Nutrients, 11(5), 1035. https://doi.org/10.3390/nu11051035